CASE REPORT
Nonsurgical Treatment of an Adult Skeletal Class III Patient with Compensated Dentition
Phase I intervention in a skeletal Class III case can involve maxillary traction with a facemask, often combined with rapid maxillary expansion, followed by orthodontic correction using Class III mechanics.1 After cessation of growth, however, treatment options may be limited to surgical-orthodontic therapy.2,3 Although surgical treatment might produce the best results, many patients reject this option due to apprehension, cost, or esthetic concerns.4-6 Orthodontic camouflage treatment is possible in borderline cases, but it is difficult to decompensate the dentition and correct the occlusion without jeopardizing the dental-periodontal equilibrium.
This case report describes a nonsurgical intervention in a postpubertal orthodontic patient with a moderate skeletal Class III malocclusion and compensated dentition.
Diagnosis and Treatment Plan
An 18-year-old female presented for correction of her protrusive lower jaw (Fig. 1). Clinical examination showed a symmetrical face with a tendency toward a dolichofacial pattern. The patient had a straight profile with a moderately prognathic mandible and a well-defined chin-throat angle. She displayed severe Class III anteroposterior relationships, a reverse anterior overjet, maxillary transverse constriction, and wide buccal corridors, with moderate crowding in the maxillary arch and minimal crowding in the mandibular arch. The upper midline was shifted 3mm to the left.
Similar articles from the archive:
- CASE REPORT Nonsurgical Treatment of a Surgically Prepared Skeletal Class III Patient Using Skeletal Anchorage September 2021
- CASE REPORT Nonsurgical Correction of Class III Malocclusion and Anterior Open Bite with Mini-Implant Anchorage November 2018
- Nonsurgical Orthodontic Treatment of Adolescent Patients with Severe Jaw Deformities September 2018
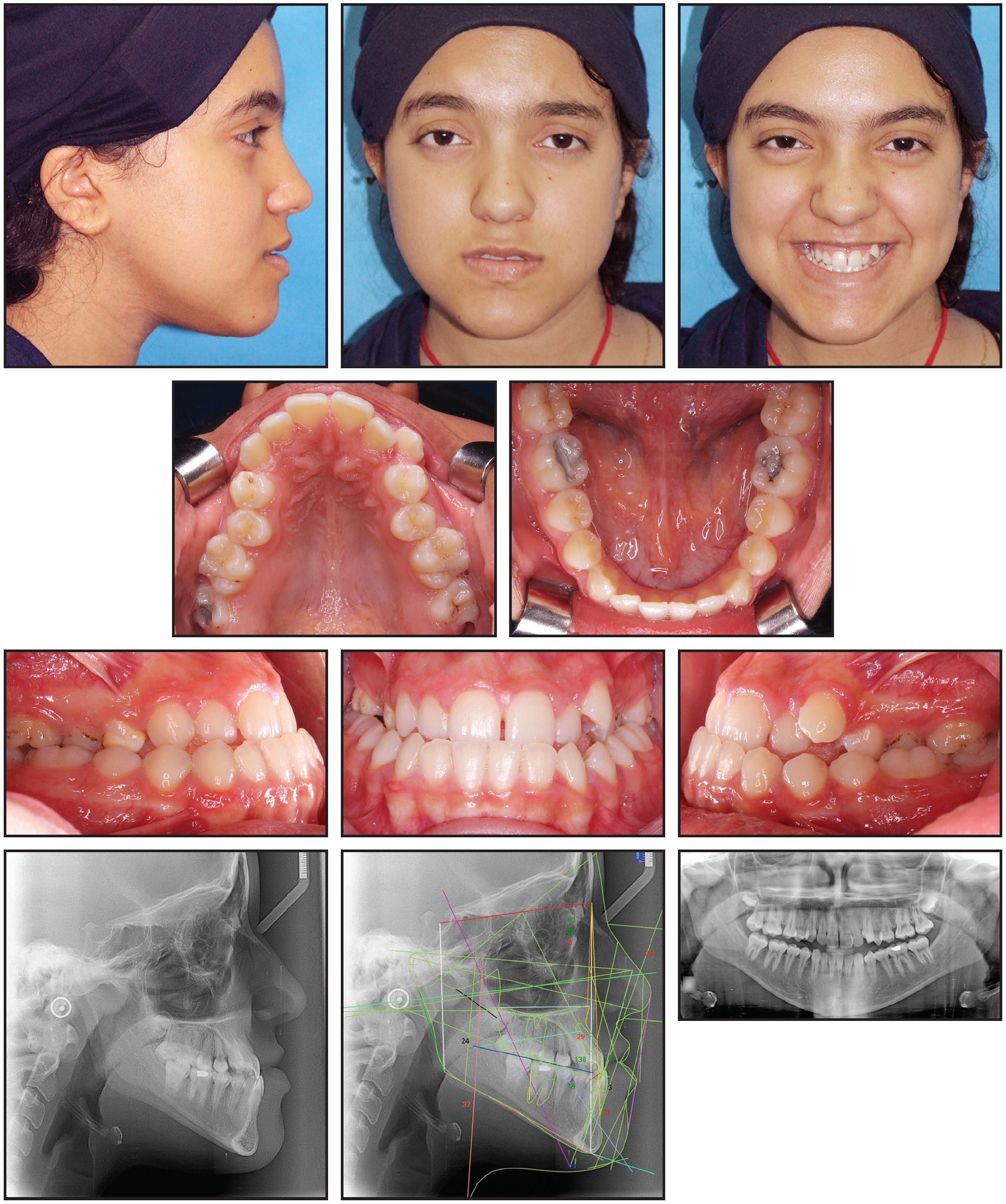
Fig. 1 18-year-old female patient with skeletal Class III relationship, reverse anterior overjet, maxillary transverse constriction, and wide buccal corridors before treatment.
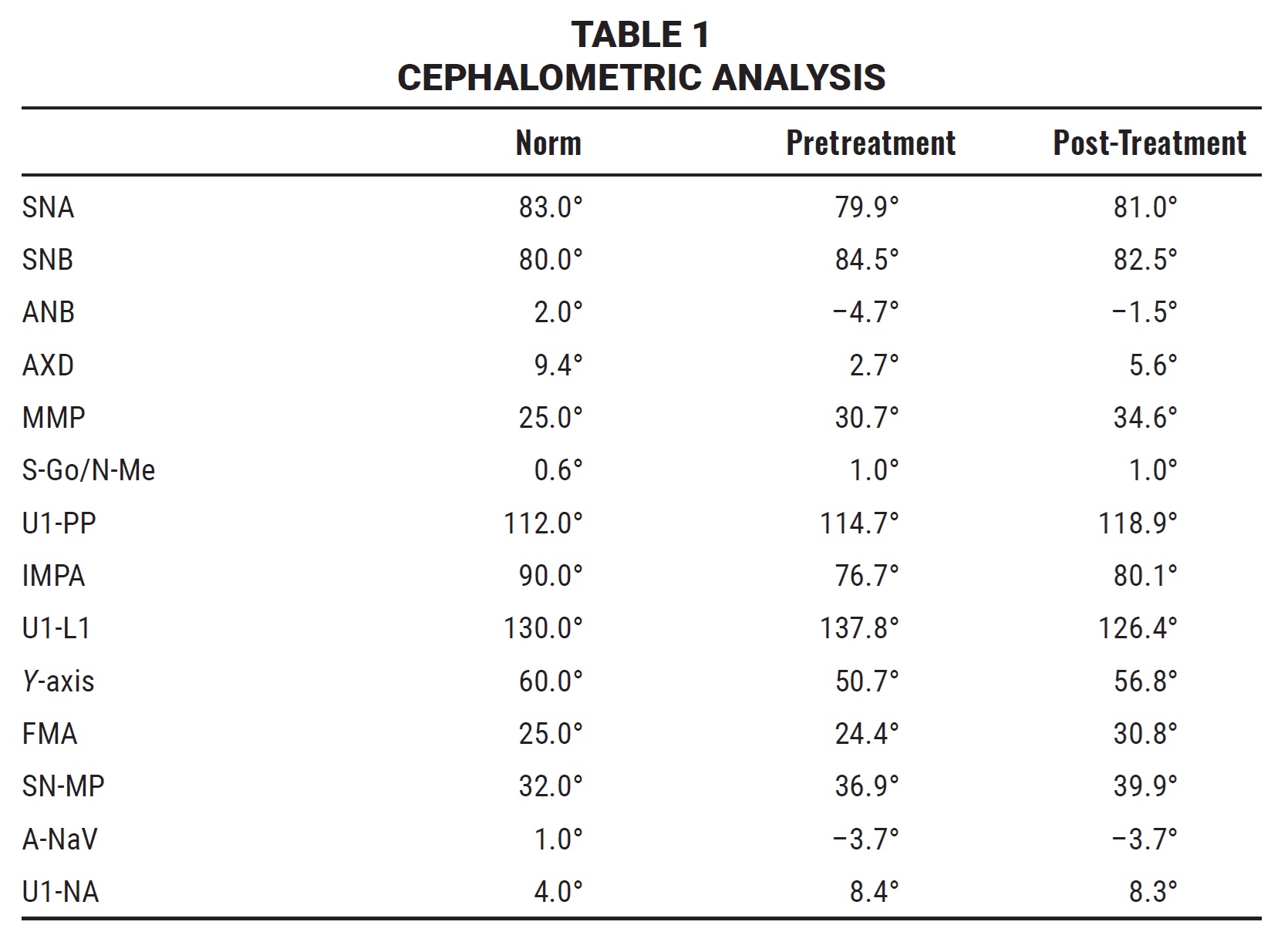
Cephalometric analysis found a skeletal Class III pattern, with an ANB angle of –4.7° caused by a combination of maxillary retrusion and mandibular protrusion (Table 1). A vertical facial pattern was evident, with dental compensation indicated by proclination of the maxillary anterior teeth (U1-PP = 114.7°) and lingual inclination of the mandibular anterior teeth (IMPA = 76.7°).
Treatment goals included correction of the maxillary transverse constriction, reverse anterior overjet, Class III relationships, and prognathic profile. Two treatment plans were presented to the patient: surgically assisted rapid palatal expansion to rectify the maxillary constriction, with orthognathic surgery to set back the mandible; or orthodontic maxillary expansion and camouflage treatment. Although the second option would resolve the anterior crossbite, the mandibular incisors would be tipped back even more, which could jeopardize the dental-periodontal relationship in the lower incisor region. After being informed of these potential consequences, the patient chose the second option.
Treatment Progress
The patient’s proclined upper incisors and retroclined lower incisors demonstrated natural compensation mechanisms that had resulted in a functional occlusion. In the maxillary arch, leveling and alignment would cause additional proclination of the upper incisors, supporting a camouflage correction of the anterior crossbite. On the other hand, leveling and alignment of the lower incisors would result in decompensation and proclination, which would complicate the camouflage treatment and overload the proclination forces on the upper incisors. The challenge was to apply short Class III elastics from the first day of treatment without leveling and aligning the lower arch, until a heavy stabilizing archwire could be ligated. If the elastics were applied after leveling and alignment, the result would be roundtripping of the lower incisors.5,7 Our solution was to use a transparent thermoformed retainer in the mandibular arch to maintain the lingual inclination of the compensated lower incisors while the Class III elastics were applied (Fig. 2). The thermoformed retainer would act as a bite raiser to help correct the transverse and sagittal discrepancies.

Fig. 2 Upper leveling and alignment, with short Class III elastics attached to brackets on lower canines and first premolars; lower thermoformed retainer worn to maintain lingual inclination of compensated lower incisors.
At the first visit, a Quad Helix* appliance was cemented to the upper first molars, the upper arch was bonded with preadjusted MBT** .018" × .025" brackets, and a 2mm thermoformed clear retainer was fabricated for the lower arch, with cutouts in the canine and first premolar areas to allow attachment of the elastics. Maxillary leveling and alignment started with .014" nickel titanium archwires. Short ³⁄16", 3.5oz Class III elastics were attached bilaterally from the upper second premolars to the lower first premolars and from the upper first premolars to the lower canines. After one month of treatment, the upper archwire was changed to .018" nickel titanium; four weeks later, an .016" × .022" nickel titanium archwire was placed.
The Quad Helix was expanded about 8mm at each monthly activation appointment, which yielded an expansion of about 2mm per month because of the resiliency of the Quad Helix and the length of the wire. About 10mm of expansion was achieved in four months, but activation was continued for another two months until overexpansion was achieved. The Quad Helix was then left in a passive state for three months to allow stabilization and interdigitation with the mandibular arch after leveling and alignment. The maxillary expansion provided space for leveling and alignment of the upper left canine and space between the upper central incisors to help correct the maxillary midline and the anterior crossbite.
After four months of leveling and alignment, an .016" stainless steel protraction arch with 4mm × 5mm gingival omega loops mesial to the first molars was ligated to the upper brackets (Fig. 3). The anterior overjet and overbite were corrected, and Class I canine relationships were achieved with 3mm of space mesial to the upper first molars. Class III elastics were worn for two months from the upper second premolars to the lower first premolars and from the upper first premolars to the lower canines to correct the reverse overjet, primarily by mesial movement of the upper premolars and anterior teeth.

Fig. 3 After six months of leveling and alignment, maxillary protraction arch inserted with gingival omega loops mesial to first molars.
The mandibular arch was then bonded using an indirect technique. Leveling and alignment began on an .014" nickel titanium wire, followed by .018" and .016" × .022" nickel titanium wires, with Class III elastics restricted to nighttime wear. After nine months of treatment, full expression of the lower bracket prescriptions was accomplished with the insertion of an .017" × .025" stainless steel archwire (Fig. 4). Positive torque was applied to the lower second premolars and molars to correct the lingual inclination of the posterior teeth. Light intermaxillary elastics were used for finishing and detailing of the occlusion and correction of the maxillary midline shift. Occlusal settling was carried out on a lower .014" stainless steel archwire.
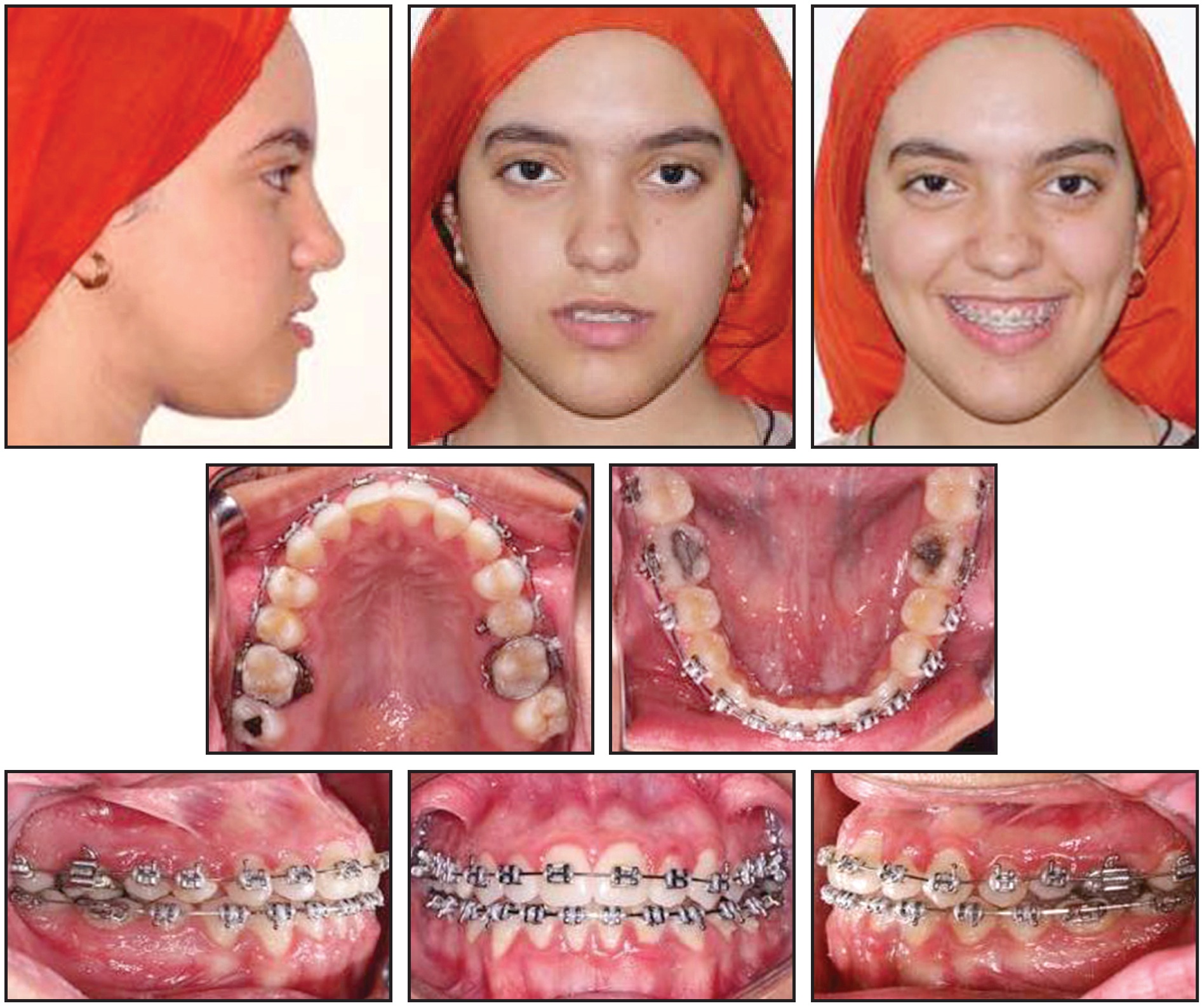
Fig. 4 After nine months of treatment.
After 12 months of orthodontic treatment, fixed lingual 3-3 retainers were bonded in both arches (Fig. 5A and 5B).
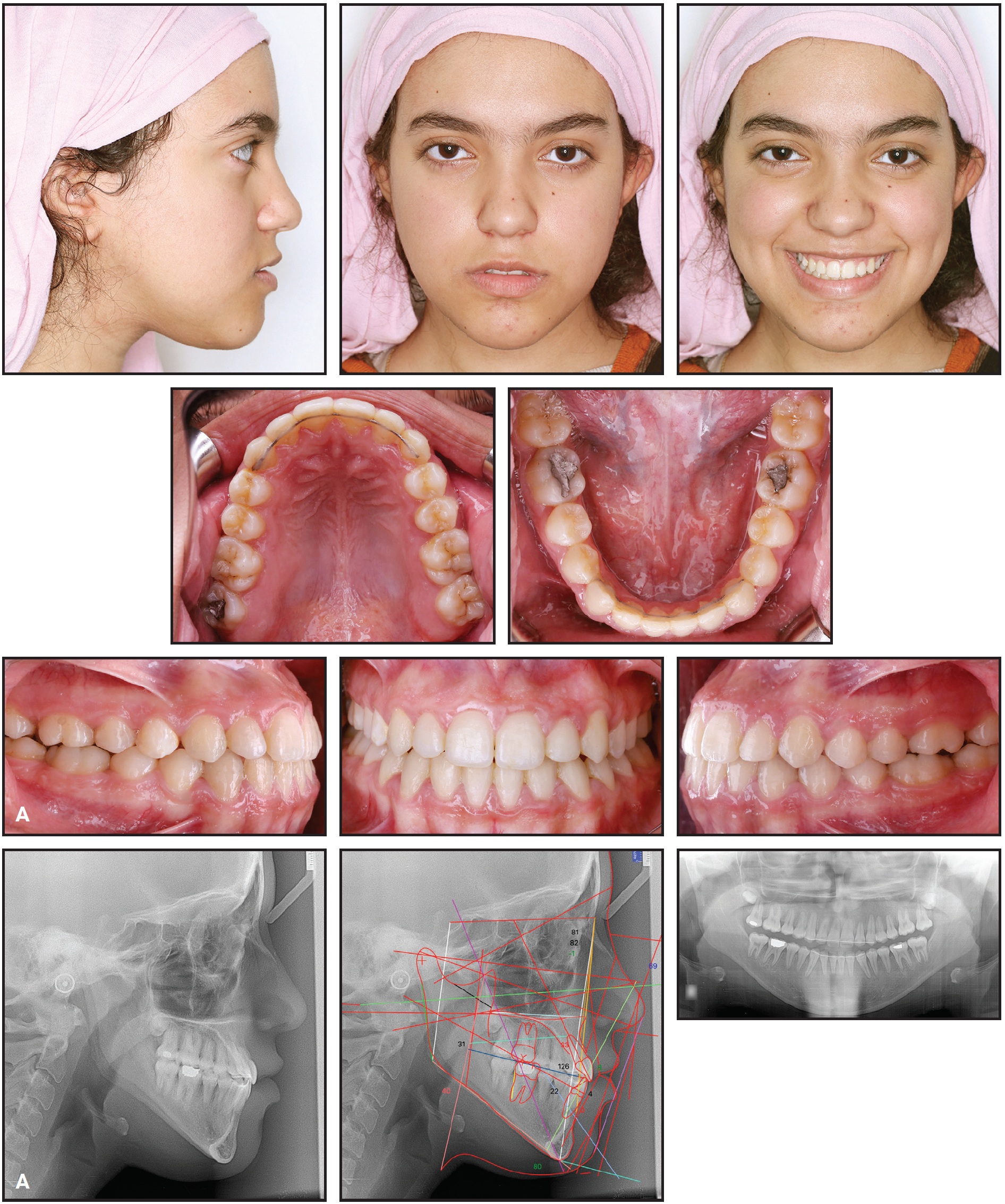
Fig. 5 A. Patient after 12 months of treatment (continued in next image).
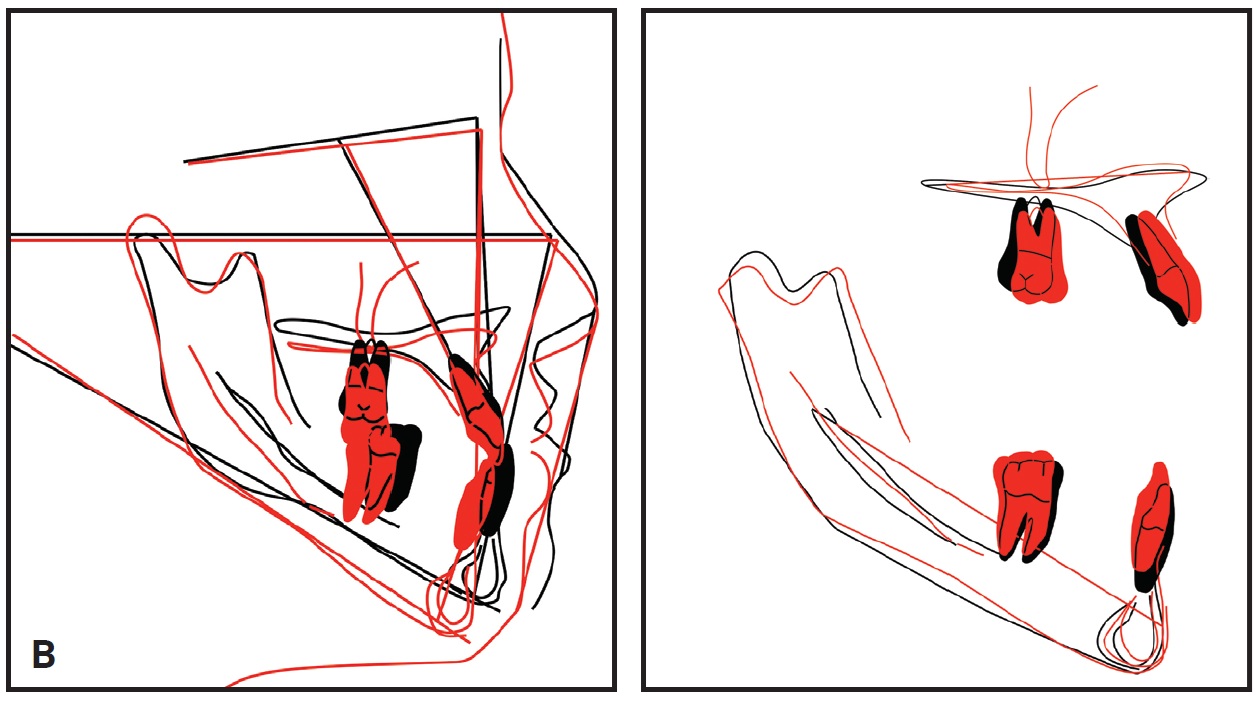
Fig. 5 (cont.) B. Superimposition of pre- and post-treatment cephalometric tracings.
Treatment Results
Post-treatment records demonstrated an improvement in the facial profile. The transverse constriction and posterior crossbite were corrected by the maxillary expansion, which resulted in narrower buccal corridors and improved smile esthetics. The maxillary midline and anterior crossbite were also corrected, and a normal overjet and overbite and bilateral Class I molar and canine relationships were achieved.
Post-treatment cephalometric analysis confirmed a 2° improvement in the SNB angle, with consequent correction of the ANB angle (Table 1). The maxillary incisors were protracted with some palatal root torque, whereas the mandibular incisors exhibited minimal proclination. The post-treatment panoramic radiograph showed no significant root resorption or other pathology.
Extrusion and mesial tipping of the maxillary molars were achieved by palatal expansion and associated hinging of the molars’ palatal cusps, while the Class III elastics simultaneously tipped the mandibular molars distally with some extrusion. In addition, the lingual root torque probably enhanced the extrusion of the lower posterior teeth. As a result, the mandible hinged open, with downward and backward mandibular rotation and clockwise rotation of the occlusal plane, which corrected the dental and skeletal Class III malocclusion and improved the straight profile and facial convexity. The use of short Class III elastics minimized the downward and backward mandibular rotation, however, as compared with a typical application of long Class III elastics.
Results remained stable one year after treatment (Fig. 6).

Fig. 6 Patient one year after treatment.
Discussion
Borderline Class III cases are challenging in terms of rectifying or camouflaging the dental and skeletal problems and achieving stable results in the short and long term, without disrupting the neutral zone or violating the dental-periodontal equilibrium. In this case, after the patient rejected a surgical-orthodontic treatment plan, our orthodontic approach permitted the correction of fundamental problems in a sequence that minimized complications.8
While a toothborne expander such as the Quad Helix can significantly increase maxillary width at the palatal level,9-11 it produces dental side effects such as tipping of the molars and premolars12 and extrusion of the palatal cusps of the maxillary posterior teeth. This extrusion tends to hinge the mandible open,13 but that was a beneficial effect in the present case because it resulted in a reduction of the ANB angle and correction of the straight profile.
If intermaxillary elastics are applied to a flexible archwire, they may cause bending of the archwire and consequent extrusion of the upper molars, counterclockwise rotation of the occlusal plane, and clockwise rotation of the mandible.14 Such complications can be minimized by the use of short Class III elastics, which can be attached to a short span of rigid wire.15 This allows for early correction of an anteroposterior discrepancy from the initial stages of treatment, and thus shortens treatment time.
In our patient, the Class III elastics were supplemented by a maxillary protraction arch, which helped correct the anterior crossbite and provided 3mm of space for mesialization of the upper first molars into a Class I relationship. A protraction arch exerts force in an anteroposterior direction; when used concurrently with Class III elastics, it directs the force of the elastics anteriorly. Finally, our treatment plan was successful in changing the spatial position of the mandible to correct the profile while reducing the force load after decompensation of the dentition.
FOOTNOTES
- *Rocky Mountain Orthodontics, Denver, CO; www.rmortho.com.
- **Trademark of 3M, Monrovia, CA; www.3M.com.
REFERENCES
- 1. Franchi, L.; Baccetti, T.; and McNamara, J.A.: Postpubertal assessment of treatment timing for maxillary expansion and protraction therapy followed by fixed appliances, Am. J. Orthod. 126:555-568, 2004.
- 2. Haryani, J.; Nagar, A.; Mehrotra, D.; and Ranabhatt, R.: Management of severe skeletal Class III malocclusion with bimaxillary orthognathic surgery, Contemp. Clin. Dent. 7:574-578, 2016.
- 3. Wilson Machado, A.; Rabelo Caldas, S.G.; and Martins Maia, L.G.: Early correction of a developing Class III malocclusion with a removable appliance, Dent. Oral Craniofac. Res. 2:359-361, 2016.
- 4. Carrière, L.: Nonsurgical correction of severe skeletal Class III malocclusion, J. Clin. Orthod. 50:216-230, 2016.
- 5. Kumari, L. and Nayan, K.: Non-surgical management of skeletal class III malocclusion with bilateral posterior crossbite: A case report, J. Clin. Diag. Res. 10:4-6, 2016.
- 6. Farret, M.M.; Farret, M.M.B.; and Farret, A.M.: Orthodontic camouflage of skeletal Class III malocclusion with miniplate: A case report, Dent. Press J. Orthod. 21:89-98, 2016.
- 7. Seo, Y.J.; Chung, K.R.; Kim, S.H.; and Nelson, G.: Camouflage treatment of skeletal class III malocclusion with asymmetry using a bone-borne rapid maxillary expander, Angle Orthod. 85:322-334, 2015.
- 8. Mostafa, Y.A.: Before we continue: Une pause, World J. Orthod. suppl:27-30, 2005.
- 9. McNally, M.R.; Spary, D.J.; and Rock, W.P.: A randomized controlled trial comparing the quadhelix and the expansion arch for the correction of crossbite, J. Orthod. 32:29-35, 2005.
- 10. Algharbi, M.; Bazargani, F.; and Dimberg, L.: Do different maxillary expansion appliances influence the outcomes of the treatment? Eur. J. Orthod. 40:97-106, 2018.
- 11. Zhou, Y.; Long, H.; Ye, N.; Xue, J.; Yang, X.; Liao, L.; and Lai, W.: The effectiveness of non-surgical maxillary expansion: A meta-analysis, Eur. J. Orthod. 36:233-242, 2014.
- 12. Conroy-Piskai, C.; Galang-Boquiren, M.T.S.; Obrez, A.; Costa Viana, M.G.; Opperman, N.; Sanchez, F.; Edgren, B.; and Kusnoto, B.: Assessment of vertical changes during maxillary expansion using quad helix or bonded rapid maxillary expander, Angle Orthod. 86:925-933, 2016.
- 13. Donohue, V.E.; Marshman, L.A.G.; and Winchester, L.J.: A clinical comparison of the quadhelix appliance and the nickel titanium (tandem loop) palatal expander: A preliminary, prospective investigation, Eur. J. Orthod. 26:411-420, 2004.
- 14. Hu, H.; Chen, J.; Guo, J.; Li, F.; Liu, Z.; He, S.; and Zou, S.: Distalization of the mandibular dentition of an adult with a skeletal Class III malocclusion, Am. J. Orthod. 142:854-862, 2012.
- 15. He, S.; Gao, J.; Wamalwa, P.; Wang, Y.; Zou, S.; and Chen, S.: Camouflage treatment of skeletal Class III malocclusion with multiloop edgewise arch wire and modified Class III elastics by maxillary mini-implant anchorage, Angle Orthod. 83:630-640, 2013.
-
 DR. RAHIMA
DR. RAHIMA -
 DR. EL-BEIALY
DR. EL-BEIALY -
 DR. MOSTAFA
DR. MOSTAFA
Dr. Rahima is a Lecturer, Department of Orthodontics and Dentofacial Orthopedics, Faculty of Dentistry, Gharyan University, Libya. Dr. El-Beialy is an Associate Professor, Department of Orthodontics and Dentofacial Orthopedics, Faculty of Dentistry, Cairo University, 11 El-Saraya St., 11553 Manial, Cairo, Egypt; e-mail: amr.elbeialy@dentistry.cu.edu.eg. Dr. Mostafa is Head, Department of Orthodontics and Dentofacial Orthopedics, Faculty of Dentistry, Future University in Egypt, New Cairo, and Professor Emeritus, Department of Orthodontics and Dentofacial Orthopedics, Faculty of Dentistry, Cairo University, Egypt.