ORTHODONTICS IN THE COVID-19 ERA
The Way Forward Part 1: Office Environmental and Infection Control
The material contained in this communication is subject to change based upon federal, state, and local regulations; guidance from agencies; and additional knowledge that will come to light throughout the COVID-19 crisis. This information was organized to provide assistance and not specific direction; further due diligence is still required. Decisions for any specific orthodontic practice should be based on your own considerations and requirements, after consulting with professional advisers who are involved in all aspects of your practice.
The current pandemic, known as COVID-19, could not have been more predictable. It marks the return of a familiar enemy. Throughout human history, nothing has killed more people than the viruses and bacteria that cause disease.
As COVID-19 is painfully demonstrating, our interconnected global economy helps spread new infectious diseases and, with its long supply chains, is uniquely vulnerable to the disruption that the virus has caused. The ability to get to nearly any spot in the world within 20 hours, especially since we may be packing a virus along with our carry-on luggage, permits new diseases to emerge and grow when they might have died out within smaller regions in the past. For all the advances we’ve made against infectious disease, it seems civilization’s progress has also made us more vulnerable to microbes that evolve 40 million times faster than humans.1
Similar articles from the archive:
Coronavirus disease (COVID-19) is a highly infectious disease caused by the newly discovered coronavirus, SARS-CoV-2. On Jan. 8, this novel coronavirus was officially regarded as the causative pathogen of COVID-19 by the Chinese Center for Disease Control and Prevention.2 The epidemic of COVID-19 started in the region of Wuhan, China, last December and has since become a major public-health challenge, not only for China, but for virtually all countries around the world.3 On Jan. 30, the World Health Organization (WHO) announced that this outbreak constituted a global public health emergency4 and declared it a pandemic.
Results from the study of Lauer and colleagues estimated the median incubation period of COVID-19 to be 5.1 days; 97% of their respondents who were infected and developed symptoms did so within 11.5 days.5 Backer and colleagues assessed the mean incubation period to be 6.4 days, ranging from 2.1 to 11.1 days.6 According to the WHO COVID-19 Situation Report-73, this incubation period is also known as the “pre-symptomatic period” in which infected patients become contagious, suggesting that transmission can occur before symptom onset.7
A study by Santarpia and colleagues on the transmission potential of COVID-19 in viral shedding observed at the University of Nebraska Medical Center indicated that COVID-19 is spread to the environment as expired particles, found during toileting and through contact with fomites as well as spread through direct contact.8 Such contacts include person-to-person and droplet transmission, along with indirect contact from contaminated objects and airborne transmission, thereby supporting a focus on airborne isolation precautions.
Keep in mind that the key to Infection = Exposure to Virus × Time. For instance, following a recent two-and-a-half-hour choir practice attended by 61 members (unfortunately including one undiagnosed symptomatic index patient), the Centers for Disease Control and Prevention (CDC) reported that 87% developed COVID-19.9 How many hours in a clinic day might you find yourself in an environment where you could, in close proximity, encounter multiple possible “vectors”? This has led the Occupational Safety and Health Administration (OSHA) to release recommendations for dentistry beyond “standard precautions,” now including both “contact” and “droplet” precautions.
Consequently, all dental professionals, including orthodontists, are at a high risk of acquiring COVID-19 through multiple transmission routes, including7:
- Respiratory droplets from coughing and sneezing that may occur during a dental or orthodontic procedure. A single cough can release 3,000 droplets at 50mph and a sneeze, 30,000 at 200mph, with perhaps 200 million virus particles expelled. This increases the possibility of inhaling at least 1,000 virus particles, apparently required to establish an infection.
- Indirect contact, in which viral droplets fall onto a surface that the dental professional or orthodontist later contacts.
- Aerosols created during dental or orthodontic procedures.
- Treatment of patients who may have experienced indirect contact transmission themselves from removing and replacing aligners, appliances, or elastics.
- Contact or exposure time with multiple such persons, including those who accompany the patients. Asymptomatic vectors or carriers who might unintentionally spread the virus by breathing, speaking (with perhaps 20 virus copies released per minute10), or singing,9 even in the absence of physical contact.
As SARS-CoV-2 has also been identified in the saliva of infected individuals, it poses a significant risk for dental professionals and their patients.2
As of this writing, there are 210 countries or territories affected by the virus. Many of these countries have established quarantines or lockdowns according to the alarming epidemiological risks involving the highly infectious state of the virus and the general susceptibility of the population.
Thanh Le and colleagues pointed out that vaccines have been in development since the release of the genetic sequence of SARS-CoV-2 on Jan. 11.11 This has led to the start of at least one clinical trial of unprecedented speed since March 16. Given the imperative for speed, there is an indication that vaccines should be available by early 2021 or, with luck, even earlier. This would represent a fundamental change from the traditional vaccine development, which takes an average 10 years, with five years representing one of the fastest.
Most orthodontic treatments are not life-threatening or part of a high-priority triage; a procedure could be considered an “emergency,” however, when an orthodontic appliance loses its integrity. Situations like swelling, soft-tissue damage, difficulty in opening the jaws, longstanding ulcers,
and inadvertent tooth movements may merit a high-priority need for dental attention. Even when scientists have found suitable treatments and vaccines, however, the handling of orthodontic patients may continue to be a challenge.
Due to economic constraints, governments are expected to gradually lift the lockdown restrictions and, in turn, permit the resumption of routine dental and orthodontic operations. This is when the serious potential for a “second wave” of COVID-19 is likely to occur.12
Feeling Conflicted?
In lieu of the upcoming relaxation of the lockdown restrictions in various countries, a thorough knowledge and understanding of sterilization and disinfection protocols is required, along with good scientific and clinical reasoning.13,14 The dichotomy of attitudes and responses to this pandemic has been extreme, ranging from, “We already use standard precautions in our practice, so you won’t even see any ‘sneeze guards’ at our reception desk,” all the way to quitting dentistry or dental hygiene due to the risks. Public perception will also be at work, especially considering that on the way to your practice, patients may encounter various protective measures such as those found at fast-food restaurants and chain stores. Decisions about changes in how we practice will likely be dictated by regulatory agencies (and it is most important to review their proclamations regularly) but, presumably, also supported by individual professional judgment. It’s a bit like investing—how risk-averse are you?
Although unlikely, the advent of contact tracing could result in quite a marketing challenge for any practice “traced and targeted” as even an asymptomatic “Typhoid Mary” source of an outbreak in its area. Consider, too, the recent incidence of multisystem inflammatory syndrome in children15-18 (while children do have a lower mortality rate, even one loss is too many), along with the reported potential for 25% of asymptomatic carriers to slip through the cracks into our practices. In fact, recent OSHA guidance (not mandates) could create legal liability risks for reopened practices if the virus is transmitted in the dental environment.19 A recent communication from the ADA stated, “This guidance is intended to help dental practices lower (but not eliminate) the risk of coronavirus transmission . . . not presume that following the guidelines will insulate them from liability in case of infection.”20 Seeking professional advice on how to handle a patient or staff member who develops COVID-19 sometime after a visit to your practice is certainly warranted. All this signals that there is an inevitable “new normal” ahead of us, although some may negotiate changes with heels dug deep along the way.
It was 35 years ago that one of the authors remembers first donning gloves and stating that, “There is no way I’ll ever be able to bend wires with these on.” A bit later, the practice of dipping orthodontic pliers in a solution for disinfection (at least until the next patient presented) evolved into autoclaves and, now, even the hiring of infection-control specialists for advice and training.
This article was not composed as an exercise in alarmism or “virtue signaling,” but rather is intended to provide orthodontic practitioners some guidance—or at least food for thought—on precautions to be taken for the treatment of orthodontic patients in a post-lockdown era, until at-home or in-office testing, vaccines, or successful treatments for COVID-19 are developed. Please consider the following touchstone when evaluating any decision made during this crisis: “What’s the downside of a bad decision?”
Sterilization Protocols
Dental professionals should be familiar with how SARS-CoV-2 is potentially spread, how to identify patients with SARS-CoV-2 infection, and what extra-protective measures should be adopted during practice to prevent the transmission of SARS-CoV-2. Here, we reinforce the standard infection-control measures that should be followed by dental professionals, though these may be subject to alteration and addenda, considering that aerosols and the droplets they arise from are presently considered the main spreading routes of SARS-CoV-2. In contrast, it appears that experts cannot agree about the significance of aerosol transmission, at least in terms of virus-laden “micro” aerosols smaller than 5μm in diameter. We might apply the aphorism, “Absence of evidence is not evidence of absence,” or argumentum ad ignorantiam: a common fallacy of logic. Advance knowledge certainly allows for advance preparation: forewarned is forearmed.21
Many of our suggestions are based on Guidance on Preparing Workplaces for COVID-19 established by the Occupational Safety and Health Act of 1970.22 The ADA recommends that all surfaces of the clinic, especially those frequently touched, be wiped with Environmental Protection Agency (EPA)-registered surface disinfectants and that instruments be autoclaved along with dental handpieces. It is important to review the manufacturer’s instructions for use of any product mentioned in this article.
Medical waste, including disposable personal protective equipment (PPE) after use, should be transported to the temporary storage area of the dental facility in a timely manner. Reusable instruments and other clinical items should be cleaned, sterilized, and properly stored in accordance with the CDC Guidelines for COVID-19 Medical Waste Disposal.23,24 The CDC notes that “medical waste (trash) coming from healthcare facilities treating COVID-19 patients is no different than waste coming from facilities without COVID-19 patients.” CDC’s guidance states that management of laundry, food-service utensils, and medical waste should be performed in accordance with routine procedures. There is no current evidence to suggest that facility waste needs any additional disinfection.
Pre-Appointment Screening and Triage
Triage includes establishing an office hotline for tele-consultation that can be used to determine the need for a patient to visit a health-care facility or provide support in following social-distancing protocols. Our teams should also inform patients on preventive measures to undertake before they come to our offices. Screening or self-assessment tools as published by CDC and the Mayo Clinic include the following questions25,26:
1. Have you recently participated in large gatherings and/or gatherings of people unrelated to you?
2. Have you traveled to or reside in a country/area reporting local transmission of COVID-19?
3. Have you been within six feet of a person with a lab-confirmed case of COVID-19 for at least five minutes, or had direct contact with their mucous or saliva, in the past 14 days?
4. Have you had any of the following symptoms within the last 48 hours?
- Fever of 100.4°F or above, or potential fever symptoms such as alternating shivering and sweating
- Cough
- Trouble breathing, shortness of breath, or severe wheezing
- Chills
- Muscle aches
- Sore throat
- Diarrhea
- Loss of smell or taste or change in taste
5. Were you a patient who has recovered from COVID-19?
If all answers are NO: Appointment can be scheduled to manage orthodontic emergency.
If any or all of questions 1, 2, or 3 were answered YES: Recommend self-quarantine procedure first, secure clearance, and screen again.
If any or all of questions 1, 2, 3, or 4 were answered YES: Refer the patient to a hospital for management.
If question 5 was answered YES: Patient should secure clearance first
Separation of Powers: New In-Office Roles
In this new environment, there may be new roles and job descriptions for staff with considerations for social distancing. The clinical staff should be segregated from reception and administrative staff using a virtual or physical “redline” on the floor or even an actual door, with the intent that, as Kipling wrote: “Never the twain shall meet.”
As patients present to our offices, they can inform us of their presence by phone, text, or a video option such as doxy.me or Zoom. The role of a greeter (or patient screener) includes asking screening questions, providing information about what to expect during the appointment, and noting specific concerns or questions the patient would like answered. The greeter (wearing appropriate PPE) instructs the patient to come to the practice entrance alone, wearing his or her own mask or scarf, and records a screening temperature. Other persons accompanying a patient will remain in their “waiting room”: their own vehicle in the parking lot.
After patients are directed to wash their hands or use provided hand sanitizer, the greeter directs them to the clinic area. They will be met by the scribe (or communications assistant) wearing appropriate clinical PPE. The role of the scribe is to welcome and dismiss patients from the clinic area without any actual treatment contact. The scribe also charts any information for the appointment, generates orders or prescriptions, takes clinical photographs, and obtains needed supplies. Although wireless and “washable” keyboards and mice are available from companies such as Seal Shield, only the scribe will use the computer, thus avoiding cross-contamination and PPE waste.
Arranging orthodontic chairs in an open bay to create a minimum of social distancing may necessitate halving capacity by working in pairs of chairs, or possibly separating units with room dividers. A second orthodontic assistant works in tandem with the scribe for each set of chairs. While one chair is occupied by a patient, the other is disinfected and left vacant. Upon completion of the appointment, the scribe directs the patient back to the reception area for egress out to the vehicle. The scribe then communicates with the parent by phone, text, e-mail, or better yet, video chat, reporting on progress, procedures accomplished, concerns, and recommendations. If video connection software is being used, the orthodontist can also be brought in on the conversation without physically meeting the parent. This saves the doctor’s time and avoids the waste of doffing and donning PPE for a trip to chat with each parent.
Feeling the Heat
It appears that the taking and recording of temperatures for staff members, patients, and even service personnel may be de rigueur going forward. Employee and patient screening forms (hard-copy, digital, or a combined temp-time clock) can be used to log the required daily health questions and temperatures.
Numerous options for “no-touch” thermometers have flooded the market in response. It is critical, however, to evaluate the instructions and specifications of any device before purchasing—some may have an accuracy of ±2°F. For instance, here are some instructions for the Braun No Touch (Fig. 1) that might be considered disconcerting27:
“1. It is important to know each individual’s normal temperature when they are well [requires taking multiple readings] . . . the only way to accurately diagnose a fever.
“2. Patient must be inside for 30 minutes before taking a measurement. Device and patient should be in same ambient temperature for 10 minutes and also remove hats [hoodies, headbands, head scarves, etc.?] 10 minutes before taking a reading. [Significantly, there may be dramatically different readings depending on the outside temperature.]
“3. Patients should not drink, eat, or physically be active before/while taking the measurement. [Does that mean they should not be chased around the reception area to get the reading?]”
Also quickly entering the marketplace are infrared temperature sensors, mounted on tripods or kiosks much like the identification kiosks found in airports (Fig. 2). These devices maintain social distancing and free up a staff member. The time-cost benefit may in the long term be worth the substantial up-front investment, depending again upon their accuracy.
Aerosol Mitigation
It seems obvious that the primary sources of aerosol production in dentistry are the same vectors: contact and proximity among patients and the treatment team. The purpose of six-foot social distancing has been to separate potential vectors from physical contact and human-generated aerosols. Unfortunately, in dentistry, that distance constricts to a mere six inches, necessitating further mitigation with gloves, goggles, and gowns, among other protective measures.

Fig. 1 Braun No Touch thermometer. Read directions and specifications before purchasing any such device.

Fig. 2 Digital Touch Systems touchless temperature monitor.
There is still some confusion about the difference in properties between the scarce, fit-tested N95 and ASTM Level 3 masks, with conflicting reports arguing both sides of “equivalent effectiveness.”28-30 Both types have high fluid resistance and are recommended when heavy amounts of fluid, spray, or aerosols are produced.28-31 It is important to note, however, that Level 3 masks filter particles of >.1μm and 98% of bacteria, but may be relatively ineffective against viruses in aerosols (coronavirus particles are .06-.14μm in size).28-30,32,33 On the other hand, N95s are FDA-regulated respirators that block at least 95% of small (.3μm) test particles and are recommended when treating patients with airborne diseases such as tuberculosis, influenza, and potentially COVID-19.34
There has also been a recent movement toward interjecting clear plastic between the parties, driven by the observation that the human eye is susceptible to coronavirus infection. Plastic barriers include not only sneeze guards and face shields, but also improvised plastic screens that can be moved over the patient’s head and even devices like the plastic “boxes” used as isolation for anesthesiology intubation.35 Although some aerosols will be blocked from directly in front of the clinician, others may slip around these types of clear barriers, as can occur with plastic face shields. And one can only imagine the distortion created by looking through a combination of loupes, face shield, and plastic box. Another possibility is to alter the clinic schedule to establish different times during the day or even separate days when aerosol-generating procedures (AGP) will be performed.
Beyond the typical sneezes and coughs, the other specific offenders in dentistry are splashes and sprays emanating from the oral environment. This is especially crucial when using such devices as dental handpieces, air-water syringes, prophy devices, ultrasonic scalers, prophy jets, and even soft-tissue lasers. It is also important to consider toothbrushing and patient rinsing in common sinks. Perhaps the demise of the “environmentally friendly” hand dryer is also at hand.
One of the most important investigations that should be performed immediately is to determine where the high-volume evacuation (HVE) and low-volume evacuation (LVE) dental units exhaust all the “contaminated” air that they suction from patients’ oral cavities. Remember, typical HVEs evacuate a substantial amount of air at about 100 cubic feet per minute, with an ideal suction pressure of 11-12 bars. Trace the connections back to the dry or wet vacuum pump in your facility’s utility room or basement to determine where the exhaust from those units terminates. After the effluent is separated, the liquids will probably empty into the sewer (note that methods to trace SARSCoV-2 through sewage are being developed to track existing or prevent future occurrences). But it may come as a shock to find that the aerosol-containing air terminates right back into a utility room or basement—as may well occur if there were no building regulations during construction that required the exhaust to be directed out of the building. This means the contaminated air that we are so diligently suctioning from our patient’s mouth using HVE is simply being pumped right back into our environment, negating any of our carefully planned filtration efforts (Fig. 3).
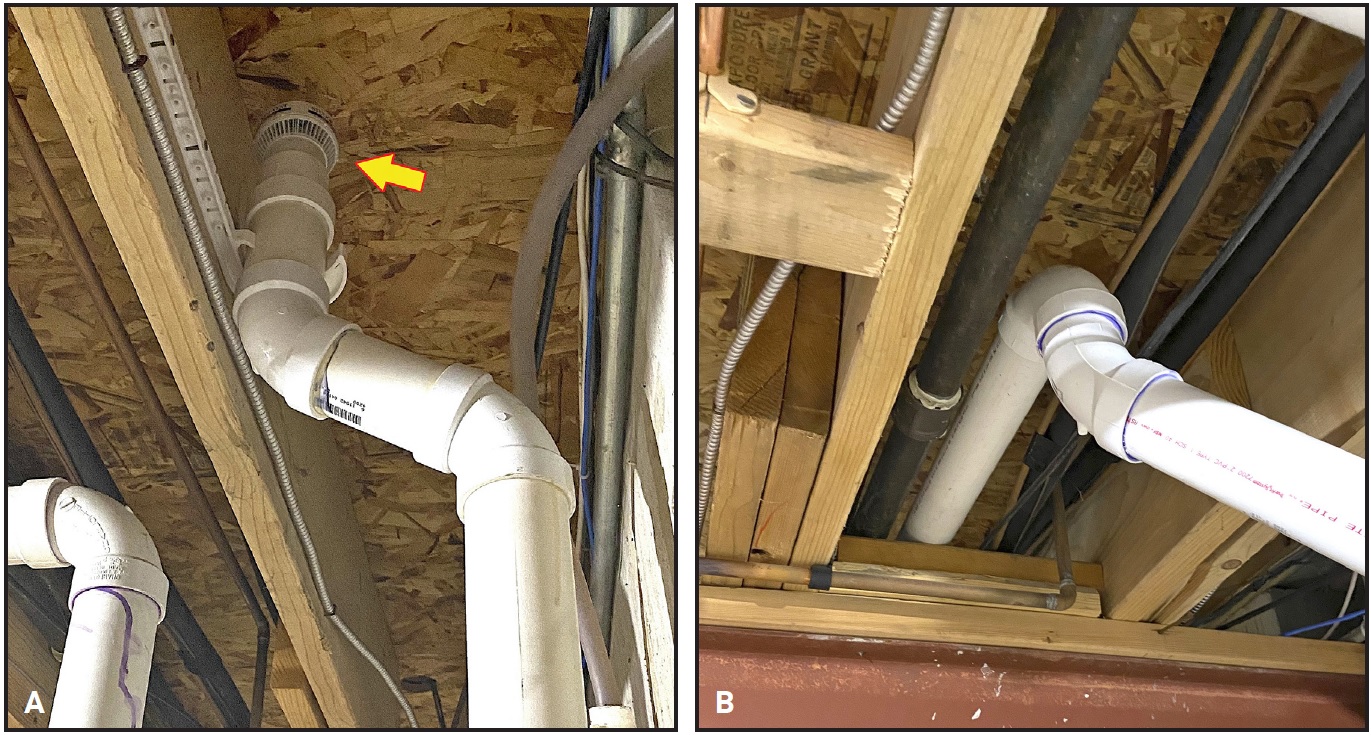
Fig. 3 Similar to leaky automobile exhaust system under floorboards, air from high-volume evacuation system may have been inappropriately exiting into utility room or basement instead of being directed outside. A. “Diffuser” exhaust for vacuum unit (arrow) was unfortunately positioned right below floor of clinic. B. Solution routes exhaust outside office.
A number of hands-free intraoral LVE attachments, including ReLeaf, Isolite, PushBackVac, Mr. Thirsty, DryShield, and NOLA, are familiar to dentists. Other intriguing options include the HVE Dental Mirror—a single instrument that incorporates suction through a modified dental mirror, which could obviate the need for an assistant to hold the evacuation instead of a mirror when using a handpiece. Other products include the Purevac system of mirror tips with HVE hose adapter and the Nu-Bird Silver Raven Evacuation Mirror (]Fig. 4).
Many simple “funnels” or “dry cup” HVE attachments have been introduced for next ad labra (next-to-the-lips) evacuation, but this kind of device must be held steady by the patient near the lower lip. Also interesting are HVE devices that are attached to standard cheek retractors, providing aerosol “scavenging” immediately adjacent to the lower lip (Fig. 5).
A variety of external mobile aerosol suction units have entered the professional marketplace for prope os (close-to-the mouth) evacuation. These devices may have started life in the nail salon market or as dental mercury vapor scavengers. Their adjustable suction arms can be positioned close to the mouth, and they not only serve as aerosol scavengers, but often feature self-contained high-efficiency particulate air (HEPA) or ultraviolet (UV) air-purification filters (Fig. 6).
Taking all these options ad absurdum, you could combine intraoral LVE isolation, an HVE mirror, a next-to-the-lips HVE attachment, a mobile close-to-the-mouth scavenger (possibly with a separate portable filtration unit), and plastic shielding between vectors. That might be thought to eliminate almost any transmission.
HVAC Office Engineering
There are innumerable HEPA and UV air-filtration units of all shapes and sizes (Fig. 7), featuring various claims of efficacy, all the way up to serious “air scrubber” portable filtration systems. In the current pandemic atmosphere, buying extra equipment should warrant a caveat emptor attitude rather than a knee-jerk panic purchase. Before investing in a chorus of portable air filters to line the walls of an open-bay clinic, you should take the time to request an office environmental evaluation from a heating, ventilation, and air conditioning (HVAC) expert or engineer, not just an inexperienced “heating and cooling” tech. This may save money, time, disappointment, and distress in the long run.
Proceed with caution if you’re thinking only “air purifiers,” and pay serious attention to the location of the exhaust from any of these units.40 Moreover, you might not save money and effort in the long run with a series of portable devices—especially considering the costs of replacing filters and UV lamps, maintenance, and electricity if you are employing several of these. It is critical to compare the cubic footage of the space you’re attempting to filter to the capabilities of the units you may be purchasing. How many air changes per hour (ACH) will be generated, what is the filtration effectiveness level, and where will it exhaust? Many units offer the option to exhaust air back into the environment whence it came, or perhaps it could be engineered to exit out of the office. Imagine connecting a series of these units in an open bay, perhaps to a common exterior exhaust, as a kind of “negative pressure.” An argument can be made that these individual or portable filters can’t hurt, might help, and, if visible to the public, might make parents or patients more confident that preventive actions have been taken in the practice.
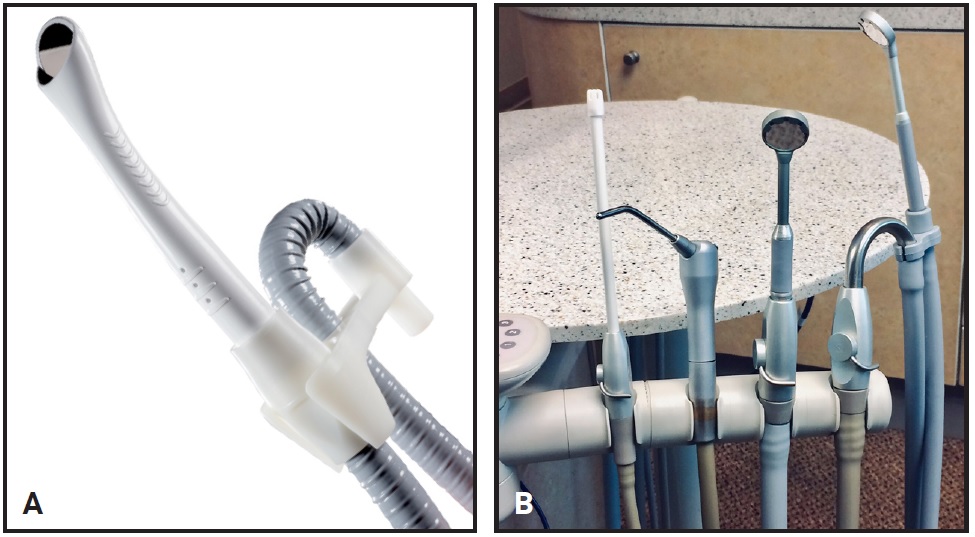
Fig. 4 Purevac (A) and Nu-Bird (B) intraoral evacuation systems. Added versatility is offered by combining high-volume evacuation suction with modified dental mirror.
Fig. 5 Astadentium Oral BioFilter (A) and Xuction Dental Aerosol Reduction Device (B) attach to cheek retractors for next-to-lips evacuation.
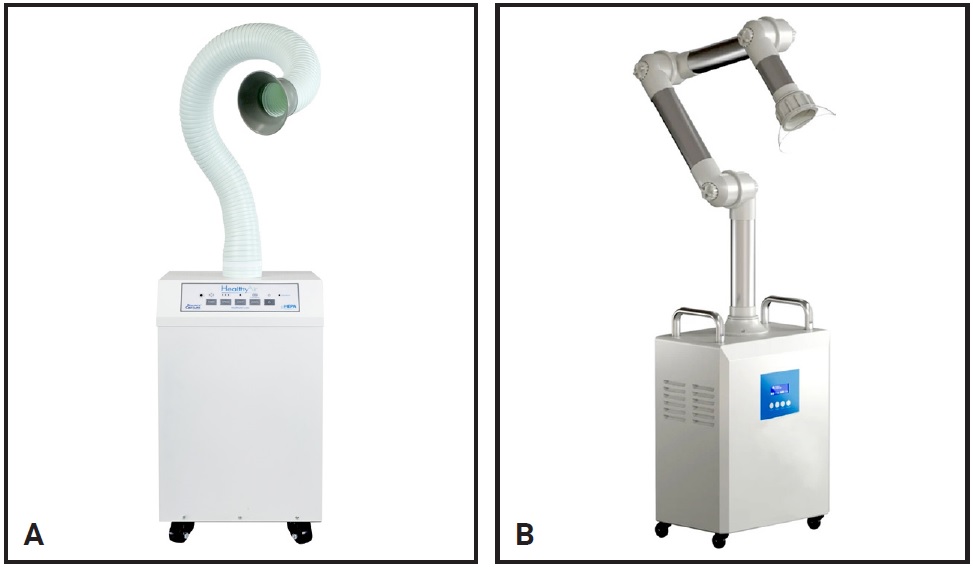
Fig. 6 HealthyAir Oral Aerosol Vacuum and Air Purification Filter (A) and OCTOdent Aerosol Scavenging Suction Unit (B) for close-to-mouth evacuation.

Fig. 7 Jade Model SCA50000C HEPA-RX and ultraviolet (UV) stand-alone filtration units.
True negative pressure is produced by a ventilation system that removes more air from a room than is permitted to enter (often through a gap under the door).41,42 We must keep in mind that the recommendation for a simple ceiling fan in a typical family bathroom is 8 ACH; therefore, we may already have a primitive negative pressure room in our own home. In theory, a collection of bathroom fans in an open bay could constitute a loud, inefficient, unfiltered, and ultimately unacceptable method of aerosol clearance. But more important, where would the exhaust from those fans go?
What do the alphabet agencies (CDC, OSHA, ADA, AAO) regulating our future say about air quality in regard to AGP? Although “regs” will likely continue to change, the direction thus far encompasses emergency care in an isolated environment, with “engineering controls” such as high-efficiency air filters, increased ventilation rates (6-12 ACH for new construction or renovation areas), and negative pressure ventilation to minimize hazard exposure.22,43-45 These words strike fear into the heart of the dental profession.
Interviewing an HVAC engineer with experience in health-care settings (perhaps with certification from an organization like ACCA, NCI, BPI, or ASHRAE) may provide invaluable advice on endeavors to improve safety in the current and post-COVID environment. Remember, any enhancement to mitigate aerosols will also provide a potential reduction in transmission of all other types of airborne infectious diseases, from rare to common (SARS, tuberculosis, H1N1, meningitis, noroviruses, chickenpox/shingles, DTP, pneumonia, strep, measles, colds, and influenza) in our practice environment. Office humidity is another concern; the recommendation is to maintain 40-60% humidity, since it appears that the current virus is more vulnerable in that range. Consulting with an engineer who is familiar with your location is critical, because HVAC filtration needs differ considerably in arid, humid, arctic, and rainforest climates.
Unless it is mandated in the future, the addition of medical-grade filtration seems to be a personal decision that must be weighed in terms of cost-benefit ratio for the orthodontist. Perhaps adding HEPA (capture and kill) filtration with ultraviolet germicidal irradiation (UVGI) light units to existing air conditioning/heating units could be considered a substantial first step toward improving overall office air quality (Fig. 8). Finally, don’t forget that you may need to leave the HVAC system fan switched on during the clinic day to ensure that the air-filtration circulation is constant; otherwise, when the air or heat is off, no filtration will occur.
Segregation of Aerosol-Generating Procedures
If you are considering the segregation of typical AGP such as bonding and debonding within your practice, then the concern is whether your facility can accommodate construction or conversion of a separate, private room. What if you, your staff, your patients, or regulatory authorities determine that your HVE, room dividers, and “temporary containment solutions” (walls or room kits, such as those from STARC Systems), combined with general office filtration systems, are insufficient?
Fig. 8 “In-duct” REME Halo UV air-purification system can be installed into heating, ventilation, and air conditioning system.
If you have the luxury of a private room that can accommodate a dental unit and can be isolated with a door, you may be able to add a Food and Drug Administration (FDA)-approved, self-contained, in-ceiling-mounted HEPA filter module (Fig. 9), reinforced with optional UV-C lamps for viral irradiation. Damper-regulated intake ducts connected to a blower system modulate the filtered air, exhausting either back into the same room or outside the facility. The amount of air directed externally regulates the “negative pressure” from 0 to 100%, as desired or required (Fig. 10). Remember, though, the air you’re pushing outdoors is the same air you paid to “condition” or heat; in other words, your dollars may literally be flying outside.
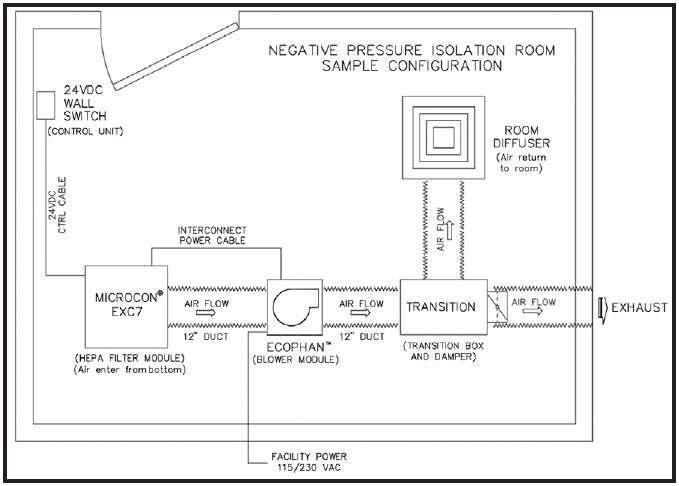
Fig. 9 Sample isolation room configuration with optional, regulated negative pressure. Clinic air >>> Private room >>> Filtration module >>> UV unit >>> Blower >>> Duct-filtered air back to room or exhaust outside office (negative pressure). (Image courtesy of RGF-BioControls.)
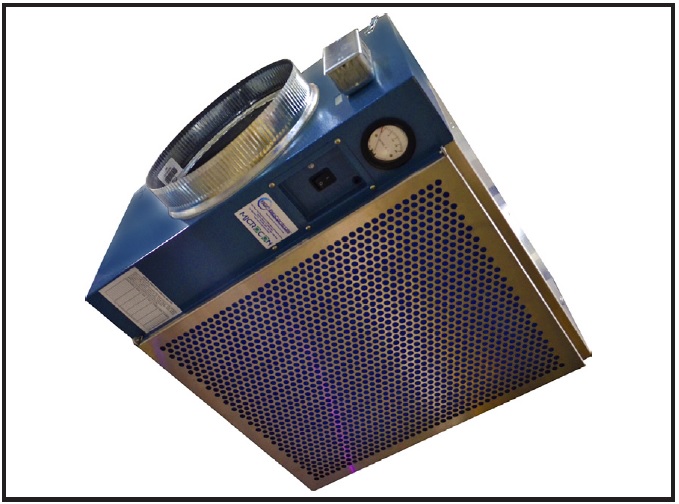
Fig. 10 HEPA air-filtration module such as MICROCON EXCY7UV with Ecophan blower can be combined with ducting and dampers to create separate system for aerosol isolation room.
Depending on the dimensions of the room, the ACH can be regulated from the recommended 6 to more than 12. These units can provide 850 cubic feet per minute of filtration at 1.35 static pressure level (in comparison, the resistance for ducting in a typical office system is about .5 static pressure level). The cost of installation is a serious consideration for this more permanent and versatile solution. But keep in mind the possible long-term benefits in the event of a recurrence of COVID-19, along with the reduced risk of other airborne diseases throughout the year.
Liquid and Spray Disinfection
As part of annually required OSHA team training, we are already familiar with the proper ties, instructions, and safety requirements for typical
disinfecting sprays and liquids. Some additional diligence may be needed to determine the coronavirus effectiveness and contact times of the products we use. The following advice should be considered an adjunct to Dorst’s article on “Back-to- Work Coronavirus Infection Control.”46
Alternative disinfection options may be worth investigation, including materials that are said to be nontoxic and produce little or no residue, but it is important to check them against the EPA’s List N of disinfectants approved for use against SARS-CoV-2.47 Some of these options are gaining popularity in hospitals, airlines, and grocery stores (some are safe on foods) for “spray and wipe” surfaces or for use in portable or stand-alone sprayers or foggers.
Hypochlorous acid (HOCl) is a weak acid created when chlorine dissolves in water to form a hypochlorite (electrolysis of saltwater is a common application). It is a naturally occurring material, even produced by your white blood cells, but it has a limited shelf life—mix it and use it—because 90 minutes later, it returns to saltwater. HOCl is both FDA-approved and nontoxic, superior to bleach,48 and can be generated in small home units or larger industrial units, such as those from EcoloxTech being employed on cruise ships.
One proprietary HOCl option for touchless disinfection is the EPA-registered Purtabs (Fig. 11). These sodium troclosene tablets are dissolved in water in the tank of their Protexus electrostatic sprayer to disperse the material in both clinical and common areas of a practice. The cordless device electrostatically charges the liquid spray, and the aerosol will then “surround” and cling to surfaces. Although these types of sprayed disinfectants are claimed to be safe around medical and dental equipment, consider “bagging” computers, x-ray equipment, and digital intraoral scanners before spraying the environment where they reside.
Other disinfectants worthy of consideration include VitalOxide disinfectant cleaner with its Victory electrostatic sprayer (Fig. 12). Oxychlorine/ammonium chloride is touted as being noncorrosive and non-irritating to the skin and is EPA-approved for one-minute SARS-CoV-2 sanitation. There are certainly other options, such as H2O2 and stabilized aqueous ozone, but each will require diligence in examining Safety Data Sheets, applications, and instructions before being added to your disinfection armamentarium.
Ultraviolet Light
UV light has been used since the early 1900s for water purification. There are three types of UV radiation: UV-A, B, and C. UV-C is the shortest wavelength of UV light emitted by the sun and is also the most dangerous, although much of it, thankfully, is absorbed by the earth’s ozone layer.
Significant caution is warranted when considering the use of any advertised “bare bulb” UV lights. Marketing of hand-held UV wands and small tabletop units is currently bombarding virus-conscious consumers. The dangers of any UV application can be quite serious, however, since these lights can penetrate tissues and thus damage skin and retinas. Many of the “novelty” units seen online make claims (without documented proof of effectiveness) for inactivating viruses. The advertising also seems oblivious to appropriate eye protection. In contrast, the previously discussed UV-C in-duct or ceiling units for air filtration come in safe, enclosed housings.
Hospitals have been using various UV applications (UV-C range 100-580nm) that are either built into individual rooms or work as mobile units with bare UV bulbs—including mobile robots like a kind of “UV Roomba” (Fig. 13). It is critical to note that these devices can only be used when there is no one in the area to be disinfected.
Most intriguing is the recent development of pricey “far UV-C” lamps, which produce a narrow-wavelength band that can eradicate airborne viruses (including SARS-CoV-2) without harming people.49 In the future, we may actually walk through a far-UVC decontamination chamber when entering a hospital, airport, classroom, restaurant, or even dental office. Keep in mind that UV has an effect only where the light directly contacts. In other words, areas in shadows, shade, crevices, or creases or on soiled surfaces will not benefit.
On a smaller scale in the orthodontic setting, UV sterilizers may find a home near our steam autoclaves. One example is the UPang Plus UV-C sterilizer, which was designed to sterilize plastic items such as baby pacifiers, toothbrushes, remotes, toys, gadgets, and plastic containers in a 104°F drying environment (Fig. 14). This unit employs two Philips UV lamps radiating at 253.7nm—the wavelength reported to be ideal for sterilization—inside a unit (with reflective surfaces) like a tiny refrigerator. After testing such units, we might envision sterilization of a variety of orthodontic devices, including cheek retractors, tongue retractors, elastomeric ligatures, retainers, and aligners.
Lab and Sterilization Center
The orthodontic laboratory and sterilization center have been significant concerns in recent decades. In the current environment, we need to pay extra attention to lab processing and safety procedures, equipment maintenance and instructions, sterilization specifications, OSHA regulations, and PPE recommendations, along with testing and documentation. Interestingly, some offices may already have added either ductless (recirculating and filtered) or ducted (expelled outside) laboratory hood vents. These devices incorporate fans to draw away fumes, vapors, or dust—somewhat like the negative pressure concept. We should also take into account changes being made by dental and orthodontic vendors, from small to multinational. The National Association of Dental Laboratories is likely to ramp up awareness that those vendors are unregulated in most states.
Patient Health and Hygiene
Patients with fixed orthodontic appliances should always be counseled to maintain oral hygiene between appointments. Practitioners should particularly emphasize the importance of good oral hygiene during times of emergencies or lockdowns to avoid any worsening of periodontal health.
As viral load appears highest in the oropharynx as well as the nasopharynx,50 and high in human saliva,51 these anatomical areas likely seed the lower airway and serve as the main reservoirs for aerosolized transmission and progression of pulmonary disease. Furthermore, viral loads of asymptomatic and symptomatic patients are similar, suggesting the transmission potential of asymptomatic or minimally symptomatic patients.6,52,53
Following the Guidelines for the Diagnosis and Treatment of New Coronavirus Pneumonia of the National Health Commission of the Republic of China,54 chlorhexidine mouthrinse may not be effective to kill SARS-CoV-2. In contrast, the use of mouthrinses that contain cyclodextrins, combined with Citrox bioflavonoid preparations, could provide a valuable adjunct treatment.55 A pre-procedural mouthrinse with an oxidizing mouthwash such as 1.5% H2O2 (even some Colgate and Crest mouthwashes contain 2%), 1% povidine-iodine, or even HOCl acid may prove beneficial, since it has been suggested that the coronavirus could be vulnerable to oxidation.55,56 Evidence suggests that these agents may lower the SARS-CoV-2 viral load and reduce the general nasopharyngeal microbiota, which tends to coat the surface of aerosol particles and droplets during coughing or sneezing.57
ACKNOWLEDGMENTS: Thanks to Jackie Dorst of Safe Practices, Brad Bartholomew, and Paige Easley of Kalamazoo Orthodontics, PC, for their assistance in preparing this communication.
The products and suppliers listed in this article are trademarks of their respective companies, as follows:
Braun No Touch thermometer, Braun Health Products, Bethlehem, PA; www.braunhealthcare.com.
Citrox, registered trademark of Curaden, Mesa, AZ; www.curden.com.
Colgate, Colgate-Palmolive Company, New York, NY; www.colgate.com.
Crest, Proctor & Gamble, Cincinnati, OH; www.crest.com.
Digital Touch Systems, Austin, TX; www.digitaltouchsystems.com.
Doxy.me, LLC, Rochester, NY; www.doxy.me.
DryShield, registered trademark of DryShield LLC, Fountain Valley, CA; www.dryshield.com.
EcoloxTech, Miami, FL; www.ecoloxtech.com.
HealthyAir System, registered trademark of Healthy Air Inc., Miami, FL; www.healthyair.com.
HVE Dental Mirror, GoldenDent Inc., Roseville, MI; www.physicsforceps.com.
Isolite, registered trademark of Zyris, Inc., Santa Barbara, CA; www.zyris.com.
Jade Air Purifier, Surgically Clean Air Inc., Mississauga, ON, Canada; www.scadental.com.
Mr. Thirsty, registered trademark of Zirc, Buffalo, MN; www.zirc.com.
NOLA Dry Field System, Great Lakes Dental Technologies, Tonawanda, NY; www.greatlakesdentaltech.com.
Nu-Bird Inc., Maple Valley, WA; www.nu-bird.com.
OCTOdent, Harrison, AR; www.octodent.com.
Oral BioFilter, registered trademark of Astradentium Health Technologies, Barcelona, Spain; www.oralbiofilter.com.
Purevac, registered trademark of Dentsply Sirona, Charlotte, NC; www.dentsplysirona.com.
Purtabs and Protexus, EvaClean, Braintree, MA; www.evaclean.com.
PushBackVac, registered trademark of Special Dental Products, LLC, Baldwinsville, NY; www.pushbackvac.com.
ReLeaf, Vancouver, WA; www.releafdental.com.
REME HALO and MICROCON, registered trademarks of RGF Environmental Group, Inc., Riviera Beach, FL; www.rgf.com.
Silver Surf, trademark of Seal Shield, Orlando, FL; www.sealshield.com.
STARC Systems, Inc., Brunswick, ME; www.starcsystems.com.
Upang Plus, Upang USA; www.upanguvsterilizer.com.
UVD Robot, UVD Robots ApS, Odense, Denmark; www.uvd-robots.com.
Victory Electrostatic Sprayer, Vital Solutions, LLC, West Palm Beach, FL; www.vitaloxide.com.
VitalOxide, registered trademark of Vital Solutions, LLC, West Palm Beach, FL; www.vitaloxide.com.
Xuction HVE Dental Aerosol Reducer, Xuction Dental, Midlothian, VA; www.xuctiondental.com.
Zoom Video Communications, Inc., San Jose, CA; www.zoom.com.
Fig. 11 Purtabs dissolve in water in tank of Protexus sprayer to electrostatically charge resulting disinfectant for application.

Fig. 12 VitalOxide disinfectant cleaner with Victory cordless electrostatic sprayer for hands free application of disinfectants.
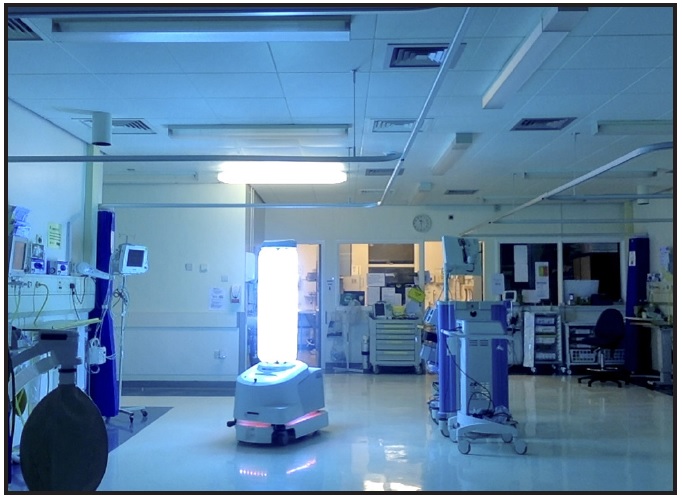
Fig. 13 UVD Robot can be programmed to cover large area with UV sterilization, but only after staff members have exited for safety.

Fig. 14 UPang Plus UV-C sterilizer, designed for baby bottles and pacifiers, might find applications in orthodontic offices, especially for plastics.
REFERENCES
- 1. Walsh, B.: COVID-19: The history of pandemics, www.bbc.com/future/article/20200325-covid-19-the-history-of-pandemics, BBC, March 25, 2020, accessed May 14, 2020.
- 2. Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.; Lau, E.H.; Wong, J.Y.; and Xing, X.: Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia, N. Engl. J. Med. 382:1199-1207, 2020.
- 3. Phelan, A.L.; Katz, R.; and Gostin, L.O.: The novel coronavirus originating in Wuhan. China: Challenges for global health governance, JAMA 323:709-710, 2020.
- 4. Mahase, E.: China coronavirus: WHO declares international emergency as death toll exceeds 200, BMJ 368:m408, 2020.
- 5. Lauer, S.A.; Grantz, K.H.; Bi, Q.; Jones, F.K.; Zheng, Q.; Meredith, H.R.; Azman, A.S.; Reich, N.G.; and Lessler, J.: The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: Estimation and application, Ann. Intern. Med. 173:577-582, 2020.
- 6. Backer, J.A.; Klinkenberg, D.; and Wallinga, J.: Incubation period of 2019 novel coronavirus (2019-nCoV) infections among travellers from Wuhan, China, 20-28 January 2020, Euro. Surveill. 25:2000062, 2020.
- 7. World Health Organization: Coronavirus disease 2019 (COVID-19)-73, situation report, www.who.int/docs/default-source/coronaviruse/situation-reports/20200402-sitrep-73-covid-19.pdf?sfvrsn=5ae25bc7_6, April 2, 2020, accessed May 10, 2020.
- 8. Santarpia, J.L.; Rivera, D.N.; Herrera, V.; Morwitzer, M.J.; Creager, H.; Santarpia, G.W.; Crown, K.K.; Brett-Major, D.; Schnaubelt, E.; Broadhurst, M.J.; and Lawler, J.V.: Transmission potential of SARS-CoV-2 in viral shedding observed at the University of Nebraska Medical Center, medRxiv, doi.org/10.1101/2020.03.23.20039446 (preprint), posted March 26, 2020.
- 9. Hamner, L.; Dubbel, P.; Capron, I.; Ross, A.; Jordan, A.; Lee, J.; Lynn, J.; Ball, A.; Narwal, S.; Russell, S.; Patrick, D.; and Leibrand, H.: High SARS-CoV-2 attack rate following exposure at a choir practice—Skagit County, Washington, March 2020, MMWR, www.cdc.gov/mmwr/volumes/69/wr/mm6919e6.htm, May 12, 2020, accessed May 13, 2020.
- 10. Stadnytski, V.; Bax, C.E.; Bax, A.; and Anfinrud, P.: The airborne lifetime of small speech droplets and their potential importance in SARS-CoV-2 transmission, Proc. Nat. Acad. Sci. U.S.A. 13:202006874, 2020.
- 11. Thanh Le, T.; Andreadakis, Z.; Kumar, A.; Román, R.G.; Tollefsen, S.; Saville, M.; and Mayhew, S.: The COVID-19 vaccine development landscape, Nat. Rev. Drug Discov. 19:305-306, 2020.
- 12. World Health Organization: Coronavirus disease 2019 (COVID-19)-82, situation report, www.who.int/docs/default-source/coronaviruse/situation-reports/20200411-sitrep-82-covid-19.pdf?sfvrsn=74a5d15_2, April 11, 2020, accessed May 10, 2020.
- 13. Kohn, W.G.; Collins, A.S.; Cleveland, J.L.; Harte, J.A.; Eklund, K.J.; and Malvitz, D.M.: Guidelines for infection control in dental health-care settings—2003, J. Am. Dent. Assoc. 135:33-47, 2004.
- 14. Samaranayake, L.P. and Peiris, M.: Severe acute respiratory syndrome and dentistry: A retrospective view, J. Am. Dent. Assoc. 135:1292-1302, 2004.
- 15. Baker, S.: The CDC is warning doctors about the mysterious inflammation disease found in children and linked to COVID-19, Business Insider, www.businessinsider.com/coronaviruscdc-warns-doctors-mis-c-multisystem-inflammatory-syndromechildren-2020-5, May 15, 2020, accessed May 15, 2020.
- 16. Hellman, J.: New York investigating 100 cases of severe coronavirus-related illness in children, The Hill, thehill.com/homenews/coronavirus-report/497601-new-york-investigating-100-cases-of-severe-coronavirus-related, May 13, 2020, accessed May 15, 2020.
- 17. Shamus, K.J.: Inflammatory syndrome linked to COVID-19 sickens more than 20 Michigan kids, Detroit Free Press, www.freep.com/story/news/local/michigan/2020/05/14/michiganpediatric-multi-inflammatory-syndrome-covid-19-coronaviruskawasaki-kids/3109695001, May 14, 2020, accessed May 15, 2020.
- 18. Centers for Disease Control and Prevention: Multisystem inflammatory syndrome in children (MIS-C) associated with coronavirus disease 2019 (COVID-19), CDC Health Alert Network, emergency.cdc.gov/han/2020/han00432.asp, May 14, 2020, accessed May 16, 2020.
- 19. Kulsrud, Z.: New OSHA guidance on COVID-19 released, triggering liability risks for reopened practices, Dentistry IQ, www.dentistryiq.com/covid-19/article/14175354/new-osha-guidanceon-covid19-released-triggering-legal-concerns, May 5, 2020, accessed May 15, 2020.
- 20. American Dental Association: Interim mask and face shield guidelines, success.ada.org/~/media/CPS/Files/COVID/ADA_Interim_Mask_and_Face_Shield_Guidelines.pdf, April 28, 2020, accessed May 16, 2020.
- 21. Lewis, D.: Is the coronavirus airborne? Experts can’t agree, Nature 580:175, 2020.
- 22. Occupational Safety and Health Administration: Guidance on preparing workplaces for COVID-19, www.osha.gov/Publications/OSHA3990.pdf, accessed May 10, 2020.
- 23. Centers for Disease Control and Prevention: Interim infection prevention and control recommendations for patients with suspected or confirmed coronavirus disease 2019 (COVID-19) in healthcare settings, www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html, April 13, 2020, accessed May 10, 2020.
- 24. Fallahi, H.R.; Keyhan, S.O.; Zandian, D.; Kim, S.G.; and Cheshmi, B.: Being a front-line dentist during the COVID-19 pandemic: A literature review, Maxillofac. Plast. Reconstr. Surg. 42:1-9, 2020.
- 25. Centers for Disease Control and Prevention: Interim standard operating procedure (SOP) for triage of suspected COVID-19 patients in non-US healthcare settings: Early identification and prevention of transmission during triage, www.cdc.gov/coronavirus/2019-ncov/hcp/non-us-settings/sop-triage-preventtransmission.html, April 15, 2020, accessed May 10, 2020.
- 26. Mayo Clinic: COVID-19 (coronavirus) self-assessment tool, www.mayoclinic.org/covid-19-self-assessment-tool, accessed May 10, 2020.
- 27. Braun Healthcare: Braun No touch + forehead NTF 3000 user’s manual, Kaz Europe, Lausanne, Switzerland, 2014.
- 28. Loeb, M.; Dafoe, N.; Mahony, J.; John, M.; Sarabia, A.; Glavin, V.; Webby, R.; Smieja, M.; Earn, D.J.; Chong, S.; Webb, A.; and Walter, S.D.: Surgical mask vs N95 respirator for preventing influenza among health care workers: A randomized trial, JAMA 302:1865-1871, 2009.
- 29. Radonovich, L.J. Jr.; Simberkoff, M.S.; Bessesen, M.T.; Brown, A.C.; Cummings, D.A.T.; Gaydos, C.A.; Los, J.G.; Krosche, A.E.; Gilbert, C.L.; Gorse, G.J.; Nyquist, A.; Reich, N.G.; Rodriguez-Barradas, M.C.; Price, C.S.; and Perl, T.M.: N95 respirators vs medical masks for preventing influenza among health care personnel: A randomized clinical trial, JAMA 322:824-333, 2019.
- 30. Long, Y.; Hu, T.; Liu, L.; Chen, R.; Guo, Q.; Yang, L.; Cheng, Y.; Huang, J.; and Du, L.: Effectiveness of N95 respirators versus surgical masks against influenza: A systematic review and meta-analysis, J. Evid. Based Med., doi.org/10.1111/jebm.12381, posted March 13, 2020.
- 31. Centers for Disease Control and Prevention: Understanding the difference, www.cdc.gov/niosh/npptl/pdfs/UnderstandDifferenceInfographic-508.pdf, 2018, accessed May 16, 2020.
- 32. Leung, N.H.L.; Chu, D.K.W.; Shiu, E.Y.C.; Chan, K.H.; McDevitt, J.J.; Hau, B.J.P.; Yen, H.L.; Li, Y.; Ip, D.K.M.; Peiris, J.S.M.; Seto, W.H.; Leung, G.M.; Milton, D.K.; and Cowling, B.J.: Respiratory virus shedding in exhaled breath and efficacy of face masks, Nat. Med. 26:676-680, 2020.
- 33. Zhu, N.; Zhang, D.; Wang, W.; Xingwang, L.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; Niu, P.; Zhan, F.; Ma, X.; Wang, D.; Xu, W.; Wu, G.; Gao, G.F.; and Tan, W.: A novel coronavirus from patients with pneumonia in China, 2019, N. Engl. J. Med. 382:727-733, 2020.
- 34. Food and Drug Administration: N95 respirators and surgical masks (face masks), www.fda.gov/medical-devices/personal-protective-equipment-infection-control/n95-respirators-and-surgical-masks-face-masks, April 5, 2020, accessed May 16, 2020.
- 35. Flynn, E.: WMU professors developing prototype to give doctors extra level of protection against COVID-19, WMU News, wmich.edu/news/2020/04/58767, April 1, 2020, accessed May 2020.
- 36. Rice University: Bacteria trapped—and terminated—by graphene filter: Laser-induced graphene to remove pathogens from the air, ScienceDaily, www.sciencedaily.com/releases/2019/10/191007123242.htm, Oct. 7, 2019, accessed May 15, 2020.
- 37. Harrel, S.K.: Contaminated dental aerosols, Dimens. Dent. Hyg. 1:16-20, 2003.
- 38. Devker, N.R.; Mohitey, J.; Vibhute, A.; Chouhan, V.S.; Chavan, P.; Malagi, S.; and Joseph, R.: A study to evaluate and compare the efficacy of preprocedural mouthrinsing and high volume evacuator attachment alone and in combination in reducing the amount of viable aerosols produced during ultrasonic scaling procedure, J. Contemp. Dent. Pract. 13:681-689, 2012.
- 39. Desara, H.; Gurav, A.; Dharmadhiki, C.; Shete, A.; and Gaikwad, S.: Efficiency of high-volume evacuator in aerosol reduction: Truth or myth? A clinical and microbiology study, J. Dent. Res. Dent. Clin. Dent. Prospects 8:176-179, 2014.
- 40. Ham, S.: Prevention of exposure to and spread of COVID-19 using air purifiers: Challenges and concerns, Epidemiol. Health 42:e2020027, 2020.
- 41. Hoffman, P.N.; Weinbrenb, M.J.; and Stuart, S.A.: A practical lesson in negative-pressure isolation ventilation, J. Hosp. Infect. 57:345-346, 2004.
- 42. Centers for Disease Control and Prevention: Guidelines for environmental infection control in health-care facilities, www.cdc.gov/infectioncontrol/pdf/guidelines/environmentalguidelines-P.pdf, 2003 (updated July 2019), accessed April 17, 2020.
- 43. Centers for Disease Control and Prevention: Environmental infection control guidelines, www.cdc.gov/infectioncontrol/guidelines/environmental/index.html, July 23, 2019, accessed May 20, 2020.
- 44. Schoen, L.J.: Guidance for building operations during the COVID-19 pandemic, ASHRAE J., May 2020, pp. 72-74.
- 45. American Society of Heating, Refrigerating and Air-Conditioning Engineers: ASHRAE position document on airborne infectious diseases, www.ashrae.org/file%20library/about/position%20documents/airborne-infectious-diseases.pdf, Feb. 5, 2020, accessed May 20, 2020.
- 46. Dorst, J.: Back-to-work coronavirus infection control, J. Clin. Orthod. 54:269-274, 2020.
- 47. Environmental Protection Agency: List N: Disinfectants for use against SARS-CoV-2, www.epa.gov/pesticide-registration/listn-disinfectants-use-against-sars-cov-2#filter_col1, May 14, 2020, accessed May 14, 2020.
-
48.
Pradham, D.; Biswasroy, P.; Naik, P.K.; Ghosh, G.; and Rath,
G.: A review of current interventions for COVID-19 prevention, Arch. Med. Res., doi.org/10.1016/j.arcmed.2020.04.020, posted April 30, 2020. - 49. Welch, D.; Buonanna, M.; Grilj, V.; Shuryak, I.; Crickmore, C.; Bigelow, A.; Randers-Pehrson, G.; Johnson, G.; and Brenner, D.: Far-UVC light: A new tool to control the spread of airborne-mediated microbial diseases, Sci. Rep. 8:2752, 2018.
- 50. Lu, C.W.; Liu, X.F.; and Jia, Z.F.: 2019-nCoV transmission through the ocular surface must not be ignored, Lancet 395:e39, 2020.
- 51. Belser, J.A.; Rota, P.A.; and Tumpey, T.M.: Ocular tropism of respiratory viruses, Microbiol. Mol. Biol. Rev. 77:144-156, 2013.
-
52.
Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Liu, H.; Wu, Y.; Zhang, L.; Yu,
Z.; Fang, M.; Yu, T.; and Wang, Y.: Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study, Lancet Resp. Med. 8:475-481, 2020. - 53. Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.; and Du, B.: Clinical characteristics of coronavirus disease 2019 in China, N. Engl. J. Med. 382:1708-1720, 2020.
- 54. National Health Commission of the Republic of China: Guidelines for the diagnosis and treatment of new coronavirus pneumonia, version 7, kjfy.meetingchina.org/msite/news/show/cn/3337.html, March 4, 2020, accessed May 15, 2020.
- 55. Carrouel, F.; Conte, M.P.; Fisher, J.; Gonçalves, L.S.; Dussart, C.; Llodra, J.C.; and Bourgeois, D.: COVID-19: A recommendation to examine the effect of mouthrinses with β-cyclodextrin combined with Citrox in preventing infection and progression, J. Clin. Med. 9:1126, 2020.
- 56. Arshad, F.; Kumar, H.C.; Swamy, G.K.; Lokesh, N.K.; and Begum, S.: Comparative effectuality of two pre-procedural mouthwashes during debonding: A clinical study, J. Ind. Orthod. Soc. 52:248-254, 2018.
- 57. Peng, X.; Xu, X.; Li, Y.; Cheng, L.; Zhou, X.; and Ren, B.: Transmission routes of 2019-nCoV and controls in dental practice, Int. J. Oral Sci. 12:1-6, 2020.
-
 DR. SRIRENGALAKSHMI M.
DR. SRIRENGALAKSHMI M. -
 DR. VENUGOPAL
DR. VENUGOPAL -
 DR. PANGILINAN
DR. PANGILINAN -
 DR. MANZANO
DR. MANZANO -
 DR. ARNOLD
DR. ARNOLD -
 DR. LUDWIG
DR. LUDWIG -
 DR. COPE
DR. COPE -
 DR. BOWMAN
DR. BOWMAN
Dr. Srirengalakshmi is an Assistant Professor, Section of Orthodontics, Saveetha Dental College, Saveetha University, Tamil Nadu, India. Dr. Venugopal is a Senior Lecturer and Clinical Instructor, University of Puthisastra, Phnom Penh, Cambodia; e-mail: avenugopal@puthisastra.edu.kh. Dr. Pangilinan is a Resident, Department of Orthodontics, University of the East, Manila, Philippines. Dr. Manzano is in the private practice of orthodontics in Manila. Dr. Arnold is in the private practice of orthodontics in Waldbröel, Germany. Dr. Ludwig is an Assistant Professor, Department of Orthodontics, University of Homburg, Saar, Germany, and in the private practice of orthodontics in Traben-Trarbach, Germany. Dr. Cope is an Adjunct Associate Professor, Department of Orthodontics, Kyung Hee University School of Dentistry, Seoul, Korea; Adjunct Associate Professor, Department of Graduate Orthodontics, St. Louis University, St. Louis; and in the private practice of orthodontics in Dallas. Dr. Bowman is an Adjunct Associate Professor, St. Louis University, St. Louis; Assistant Clinical Professor, Case Western Reserve University, Cleveland; Instructor, University of Michigan, Ann Arbor, MI; and in the private practice of orthodontics in Portage, MI. Drs. Ludwig and Bowman are also Contributing Editors of the Journal of Clinical Orthodontics.