CASE REPORT
Pre-Restorative Treatment with the Invisalign System
Malocclusions treated with the Invisalign* system initially involved only mild crowding of 3-6mm.1 Recently, however, more complex cases involving premolar extractions, molar distalization, deep bites, open bites, crossbites, and periodontal complications have been reported.2-8
This article demonstrates the use of Invisalign appliances for pre-restorative treatment of a non-growing patient.
Diagnosis and Treatment Plan
A 32-year-old female with missing lower first molars was referred by her general dentist for space opening to allow implant placement (Fig. 1). She had a Class I molar and canine relationship and a mild deep bite. The upper first molars had overerupted due to a lack of antagonists, and overeruption of the lower anterior teeth resulted in an excessive curve of Spee in the lower arch. Anterior spacing in the lower arch was accompanied by upper anterior rotations. The third molars had been previously extracted.
Treatment objectives were to close the lower anterior spaces by moving the lower incisors, canines, and premolars mesially, while uprighting the lower second molars to provide space for prosthetic replacement of the missing first molars. The lower curve of Spee would be leveled by intruding the upper first molars, and the upper anterior rotations would be corrected.
Similar articles from the archive:
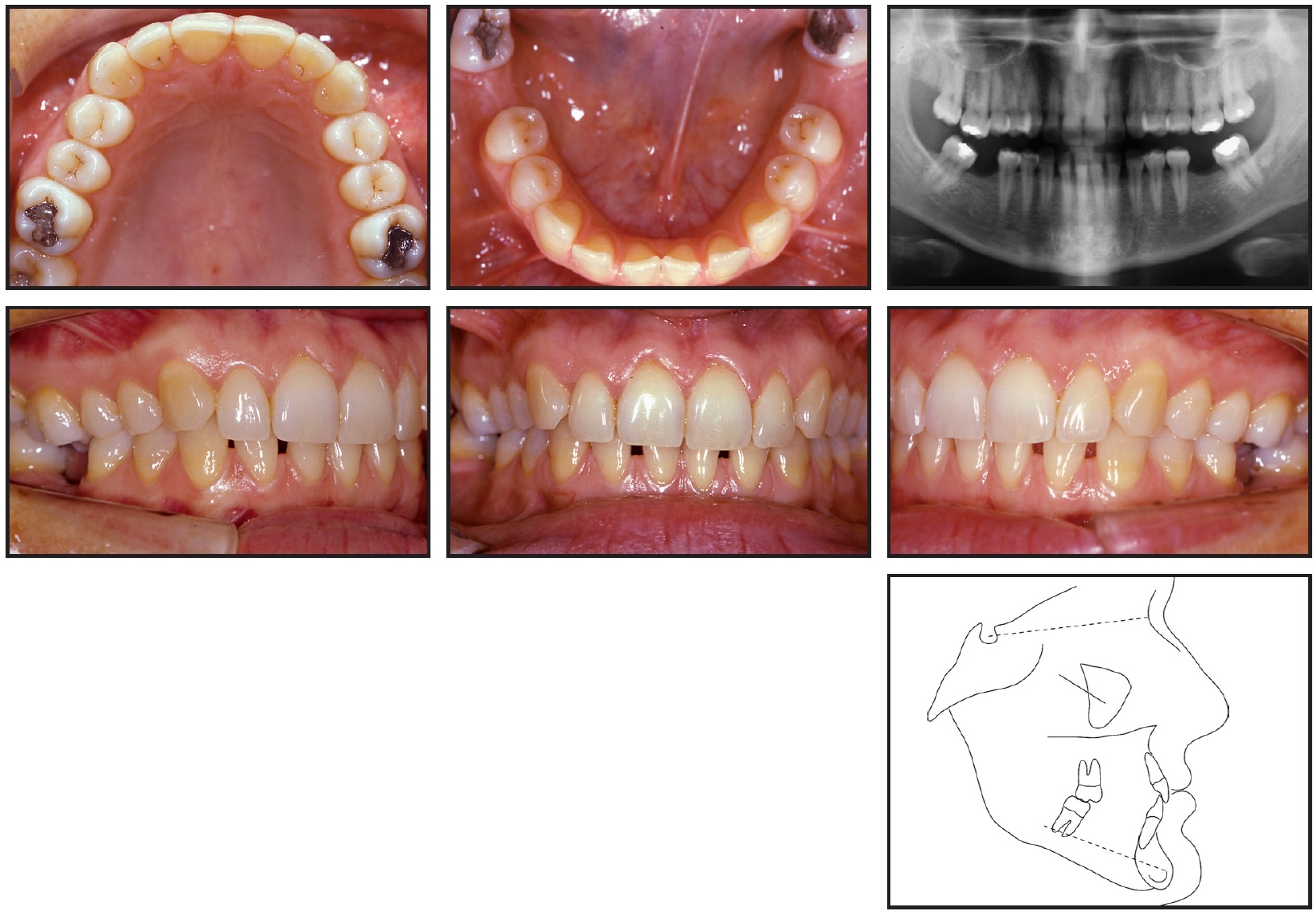
Fig. 1 32-year-old female patient with missing lower first molars and lower anterior spacing before treatment.
The patient was motivated to have the lower anterior spaces closed, but did not want to wear braces. Therefore, full-arch Invisalign treatment was planned.
ClinCheck
The ClinCheck** projection showed an improvement in the deep bite due to leveling of the mandibular arch and alignment of the upper anterior teeth (Fig. 2).
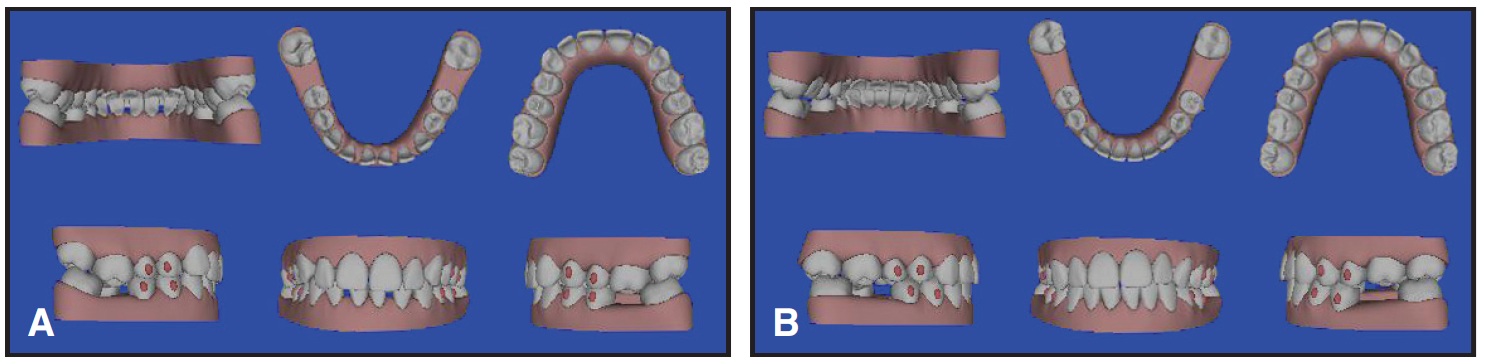
Fig. 2 A. Pretreatment ClinCheck. B. Final ClinCheck projection.
Standard .75mm elliptical attachments were placed on the upper and lower first and second premolars to intrude the upper first molars, and to provide reciprocal anchorage for mesial movement of the lower canines and premolars and distal uprighting of the lower first molars. No reproximation was necessary.
Seventeen aligners were planned for the upper arch and 24 for the lower arch, over 12 months of treatment.
Treatment Results
The patient was highly cooperative in wearing each aligner for two weeks as planned. The upper anterior teeth were aligned, and the upper first molars were intruded about 1.5mm without unwanted side effects on the adjacent teeth (Fig. 3A). The lower second molars were uprighted, while the lower anterior spaces were closed by mesial tipping of the incisors, canines, and premolars. Because the lower right lateral incisor did not follow the prescribed aligner movement, lingual and labial buttons were bonded, and the patient was instructed to wear 2oz elastics for 30 days (Fig. 3B).

Fig. 3 A. Aligners in place during leveling and alignment. B. Elastics attached to lingual and labial buttons for extrusion of lower right lateral incisor.
After 13 months of Invisalign treatment (Fig. 4), the patient was given a clear overlay retainer to wear at night in the upper arch; a fixed retainer was bonded in the lower arch.
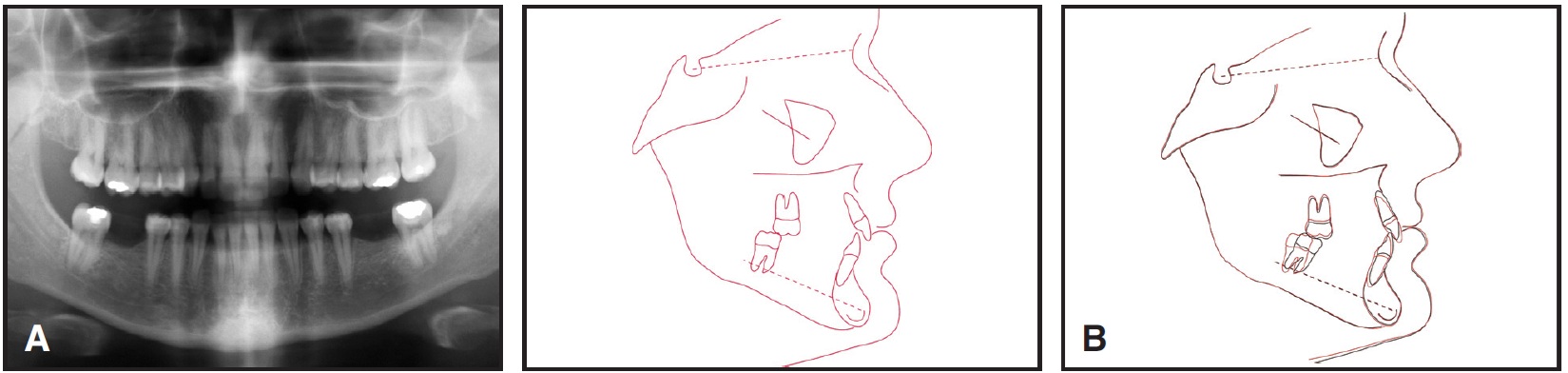
Fig. 4 A. Patient after 13 months of Invisalign treatment, before implant placement. B. Superimposition of cephalometric tracings before and after treatment.
Discussion
This case demonstrates how the Invisalign system can be successfully used for molar intrusion and uprighting. Anterior vertical anchorage was preserved without compromising the adjacent teeth, and the upper molar intrusion was performed gradually so that the roots would keep pace with the tooth movement. Distal lower molar uprighting was achieved with a mesial shift of the entire arch. This reciprocal movement lengthened the lower arch enough to provide space for prosthetic replacement of the missing first molars (Fig. 5).

Fig. 5 Patient after prosthetic replacement of lower first molars.
FOOTNOTES
- *Registered trademark of Align Technology, Inc., 851 Martin Ave., Santa Clara, CA 95050; www.aligntech.com.
- **Trademark of Align Technology, Inc., 851 Martin Ave., Santa Clara, CA 95050; www.aligntech.com.
REFERENCES
- 1. Boyd, R.L.; Miller, R.J.; and Vlaskalic, V.: The Invisalign System in adult orthodontics: Mild crowding and space closure cases, J. Clin. Orthod. 34:203-212, 2000.
- 2. Boyd, R.L. and Vlaskalic, V.: Three-dimensional diagnosis and orthodontic treatment of complex malocclusions with the Invisalign appliance, Semin. Orthod. 7:274-293, 2001.
- 3. Ellis, C.P.: Invisalign and changing relationships, Am. J. Orthod. 126:20A-21A, 2004.
- 4. Miller, R.J. and Derakhshan, M.: The Invisalign System: Case report of a patient with deep bite, upper incisor flaring, and severe curve of Spee, Semin. Orthod. 8:43-50, 2002.
- 5. Miller, R.J.; Duong, T.; and Derakhshan, M.: Lower incisor extraction treatment with the Invisalign System, J. Clin. Orthod. 36:95-102, 2002.
- 6. Sheridan, J.J.: The Readers’ Corner, J. Clin. Orthod. 38:544-545, 2004.
- 7. Vlaskalic, V. and Boyd, R.L.: Orthodontic treatment of a mildly crowded malocclusion using the Invisalign System, Austral. Orthod. J. 17:41-46, 2001.
- 8. Wheeler, T.T.: Invisalign material studies, Am. J. Orthod. 125:19A, 2004.
-
 DR. GIANCOTTI
DR. GIANCOTTI -
 DR. RONCHIN
DR. RONCHIN
Dr. Giancotti is an Assistant Professor, Department of Orthodontics, University of Rome “Tor Vergata”, Fatebenefratelli Hospital, Isola Tiberina, Via Ponte Quattrocapi 34, 00184 Rome, Italy; e-mail: giancott@uniroma2.it. Dr. Ronchin is an Assistant Professor, Department of Orthodontics, University of Cagliari, Italy.