CASE REPORT
Lower Incisor Extraction Treatment with the Invisalign System
Single-lower-incisor extraction cases have rarely been published, perhaps because there are few patients who meet the standards for such treatment. The following diagnostic characteristics are usually required for single lower incisor extractions:
- Class I molar relationship.
- Moderately crowded lower incisors.
- Mild or no crowding in the upper arch.
- Acceptable soft-tissue profile.
- Minimal to moderate overbite and overjet.
- Minimal growth potential.
- A tooth-size discrepancy, such as missing lateral incisors or peg laterals, that can be used to resolve the inevitable tooth-size discrepancy without interproximal stripping.1
In any such case, a full diagnostic setup should be made to ensure the occlusal results will be acceptable.1 Unfortunately, diagnostic setups usually involve long and laborious laboratory procedures of cutting, setting, and waxing the teeth in place. In addition, conventional methods of tooth repositioning with removable appliances require alteration of the casts by resetting the teeth, or by scraping away plaster from the teeth to be moved and blocking out space for them with wax.2
Similar articles from the archive:
New diagnostic software now makes it simple, quick, and efficient to perform virtual setups using the Invisalign System*, an alternative to traditional orthodontic appliances. This article will show how a series of clear aligners can sequentially move teeth from start to finish in a case involving a single lower incisor extraction.
Diagnosis
A 24-year-old female presented with a chief concern of "lower incisor crowding". She had undergone orthodontic treatment 10 years previously and had recently had gingival grafts on her upper and lower anterior teeth.
Clinical examination revealed full incompetent lips with the chin deviated to the right (Fig. 1). The patient had a straight profile with mentalis muscle strain; on smiling, she displayed 100% of her incisors and 1mm of gingiva. The molar and canine relationships were Class I. The patient had a 10% overbite and 3mm overjet, with the lower midline shifted 3mm to the right. Good oral hygiene was evident, although slight gingival recession was found in the areas of the upper first bicuspids and the lower right lateral incisor.
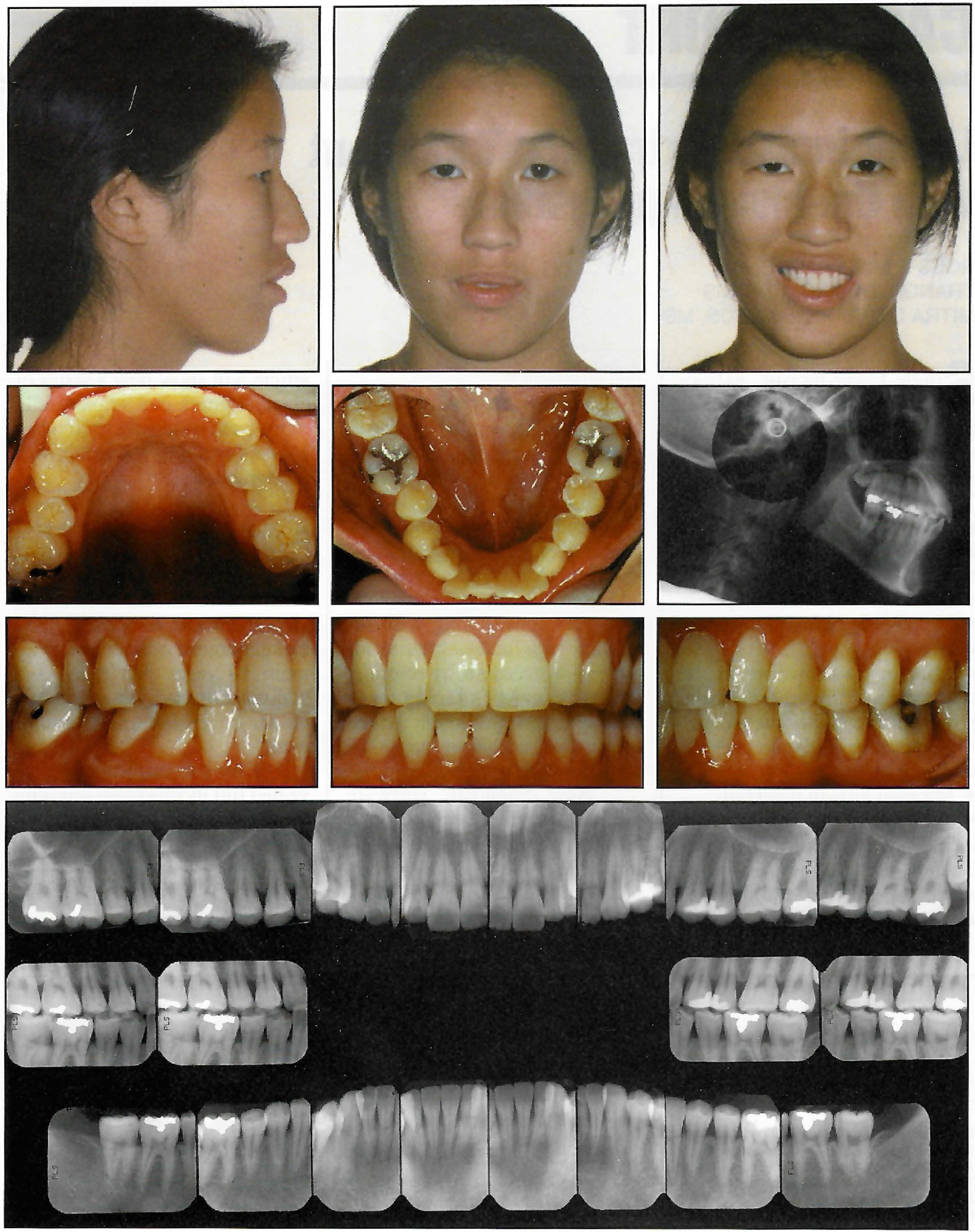
Fig. 1 24-year-old female patient before treatment.
The maxillary arch was well aligned, with a peg-shaped left lateral incisor; Bolton analysis indicated a maxillary tooth-size deficiency of 1mm. Both cuspids showed occlusal wear, and the right second bicuspid was lingually positioned and rotated mesially. There was 5mmof crowding in the lower anterior region, with lingually tipped lower cuspids and right second bicuspid.
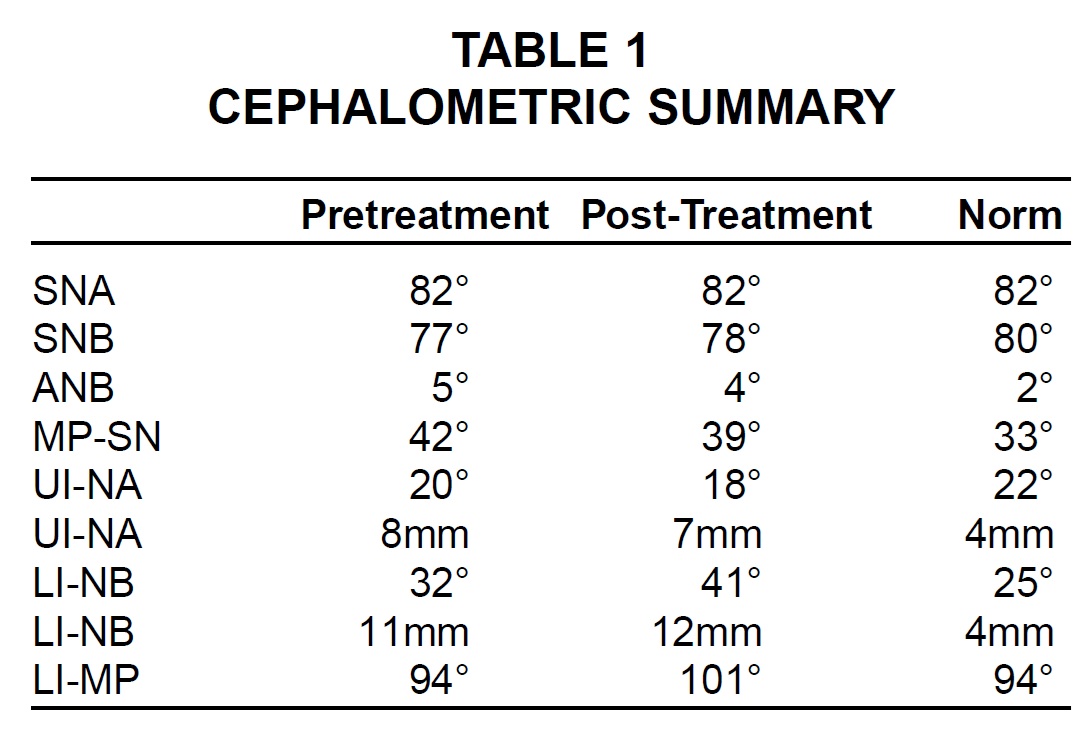
The radiographic analysis showed a full permanent adult dentition with previous extraction of third molars and minor restorations. The patient had mild generalized bone loss with normal root morphology and length. Cephalometric findings included a well-positioned maxilla and slightly prognathic mandible, resulting in a slightly excessive sagittal jaw relationship or Class III tendency (Table 1). The upper and lower incisors were protrusive and proclined.
Treatment Planning
The treatment objectives in this case were primarily to resolve the lower crowding, achieve good overjet and overbite, and avoid any further proclination of the upper and lower incisors with their thin attached gingivae. Further goals included improving the lower midline and resolving the Bolton discrepancy.
There were three treatment alternatives in this case. The first was to expand both arches to alleviate the crowding and to bond veneers to the upper lateral incisors at the end of treatment to resolve the tooth-size discrepancy. The problem with this option was that the midlines could not be centered.
The second alternative was to alleviate the lower crowding by reproximation. The lower anterior region was not suitable for stripping, however, due to the shape and small size of the lower incisors. Reproximation of the posterior segment was not a good choice because of the Class I posterior occlusion.
The final alternative was to extract a lower incisor to alleviate the crowding. The upper midline could then be aligned with the middle of the lower teeth. This plan would minimize proclination of the lower incisors and would also address the Class III tendency and Bolton discrepancy. A diagnostic setup showed that the treatment would indeed relieve crowding and allow the case to be finished with good overbite and overjet. The major drawback was that a lower incisor would have to be extracted. The lower right lateral incisor was selected because it was the most misaligned and thus contributed most to the crowding, and because its attached gingiva was the least satisfactory of all the lower incisors'.
Treatment Progress
The patient was referred to have the lower right lateral incisor extracted, and upper and lower polyvinyl siloxane impressions were taken for Invisalign appliances. A vacuum-formed retainer was made to hold the teeth in position until the aligners were delivered. The patient's final tooth setup and stages of tooth movement were generated by the three-dimensional Align Technology software and reviewed by the orthodontist on a computer, using the proprietary ClinCheck system (Fig. 2).
Prior to delivery of the first aligner, 1mm × 3mm composite attachments were bonded vertically to the lower incisors and right cuspid to prevent tipping during space closure. Lower-arch treatment was initiated with the teeth adjacent to the extraction site moving first (Fig. 3).
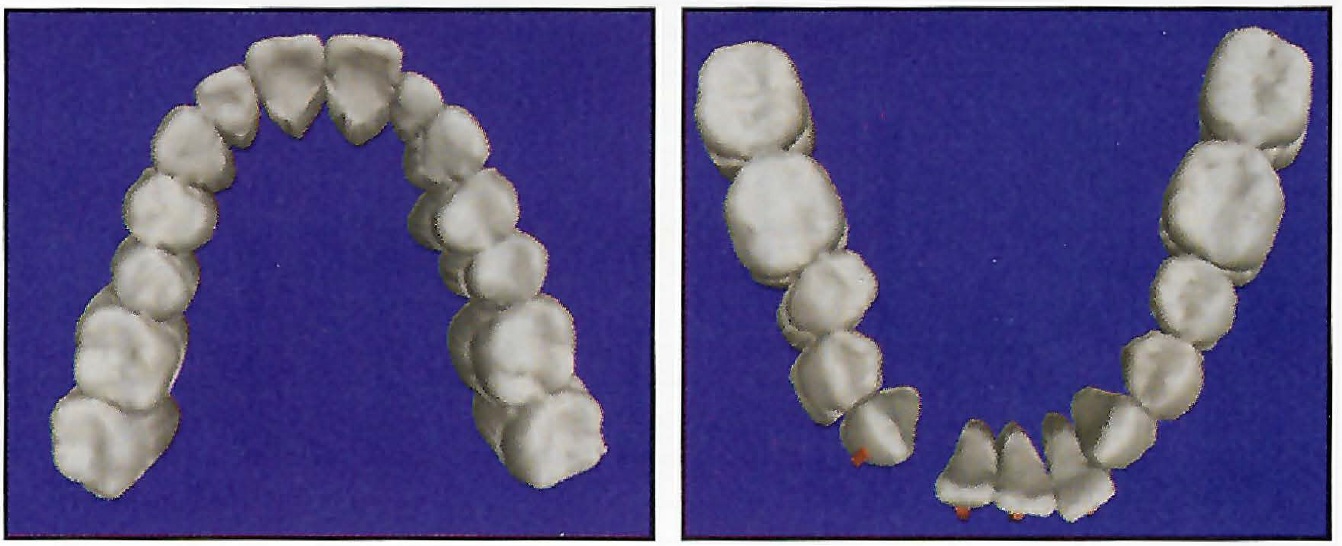
Fig. 2 Pretreatment computer images of both arches with lower right lateral incisor extracted. Objects on facial surfaces of lower anterior teeth represent composite attachments used to help resist tipping during space closure.
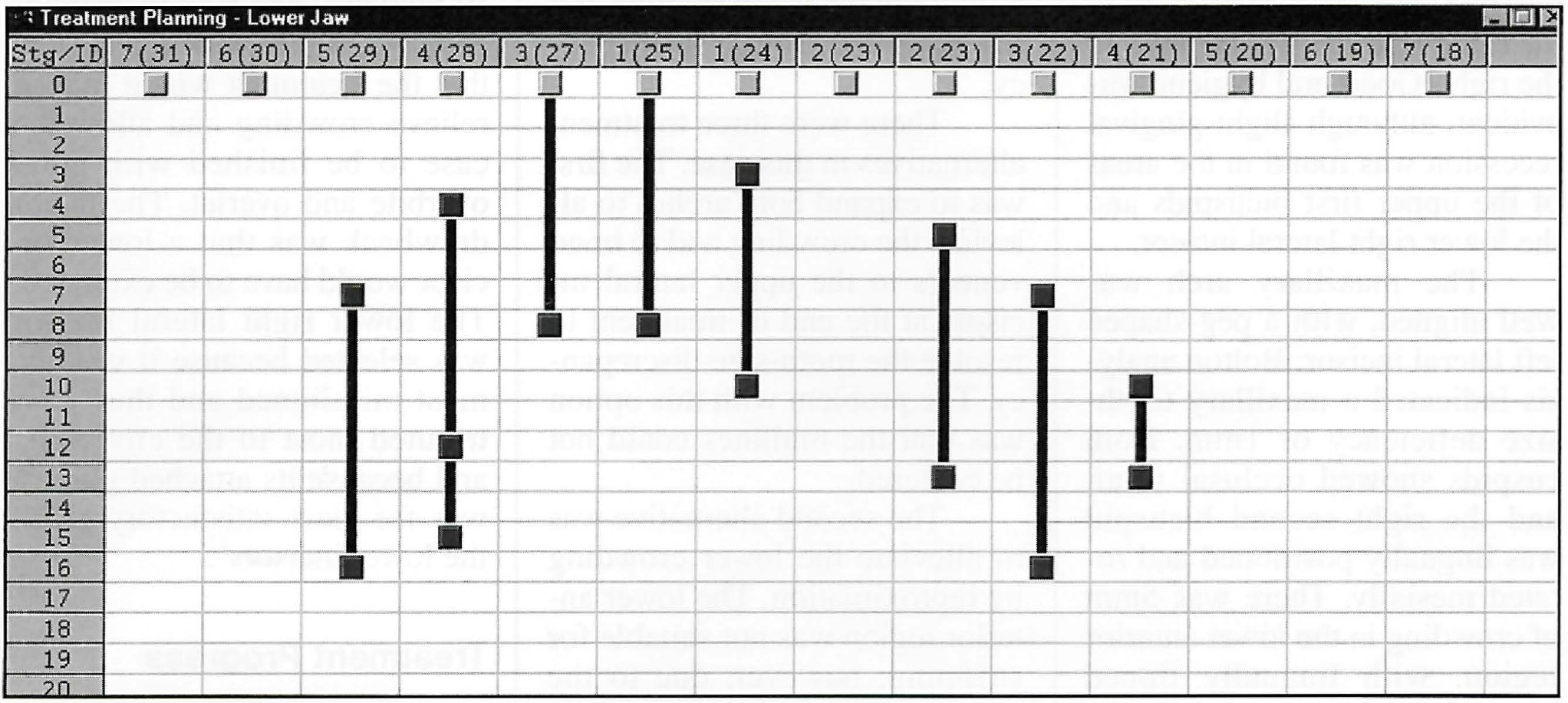
Fig. 3 Schematic representation of planned mandibular tooth movements. Each column represents one tooth; each row represents an aligner stage.
Upper aligners were not used for eight weeks, until sufficient overjet was achieved to enable incisor alignment (Fig. 4). The teeth were programmed to undergo no more than .8mm net movement per stage.
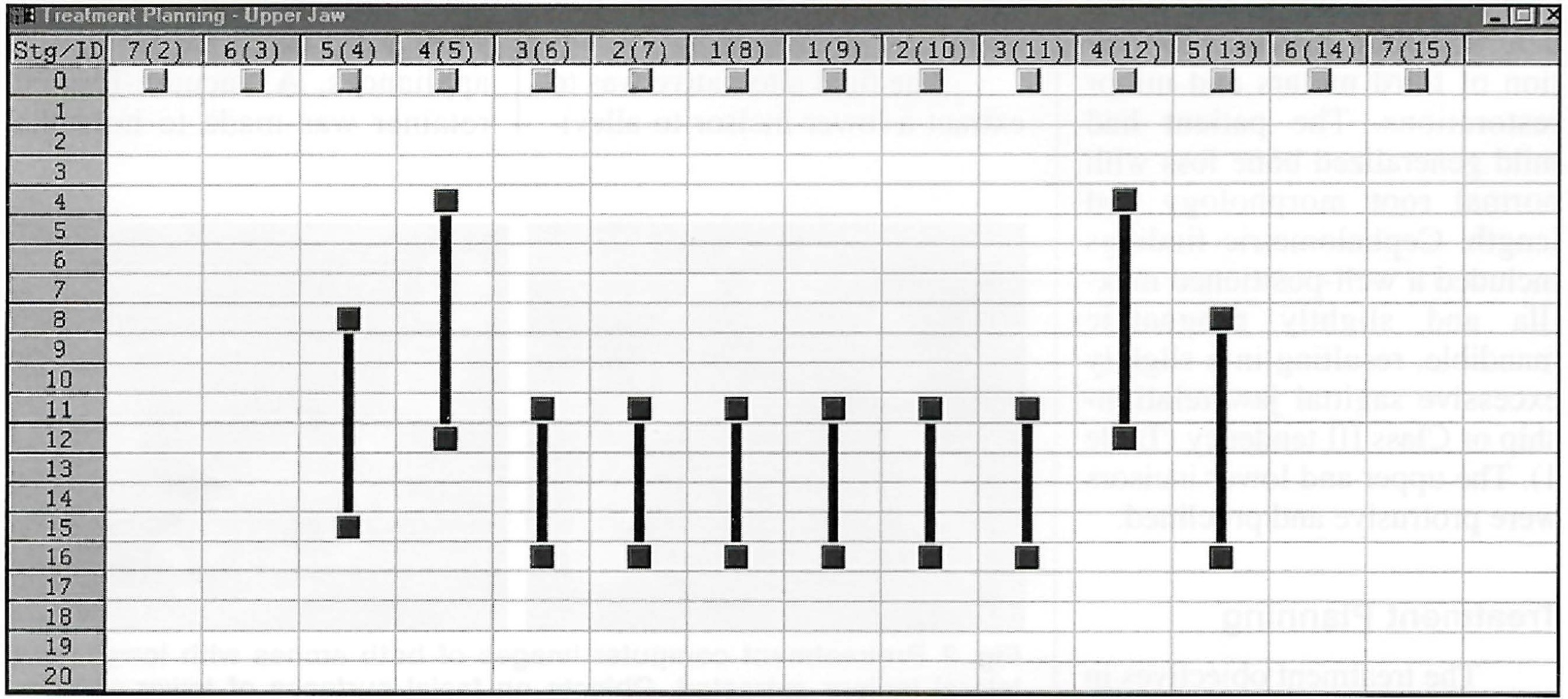
Fig. 4 Schematic representation of planned maxillary tooth movements. Each column represents one tooth; each row represents an aligner stage.
The patient was seen every four weeks for delivery of new aligners and monitoring of treatment progress and aligner fit (Fig. 5). Aligners were changed by the patient weekly at first, and later at two-week intervals. Twelve stages were required in the upper arch and 22 in the lower, with the last five mandibular aligners used in finishing to add mesial root tip of the lower right cuspid.
Total treatment time was 11 months. The patient was then given Hawley-type upper and lower retainers to be worn at night.
Treatment Results
Post-treatment facial photographs showed little change in facial profile (Figs. 6A, 6B).
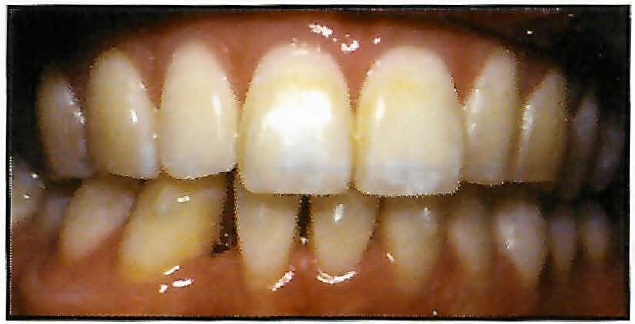
Fig. 5 Patient after two months of treatment. Note gingival recession around lower right central incisor and composite attachments on facial surfaces of anterior teeth.

Fig. 6 Patient after 11 months of treatment.
Although the patient was protrusive before treatment, her profile was acceptable to her, and there was no plan to change it. The Class I molar and canine relationship was maintained, and the mandibular spaces were completely closed. The overjet was slightly excessive due to the thick marginal ridges of the upper incisors; otherwise, good overjet and overbite were achieved despite the extraction of a lower incisor. The gingival recession in the lower right central incisor region increased during treatment.
Both arches showed good alignment, with the upper midline centered on the middle of the lower incisors. Comparison of the post-treatment occlusal photographs with the computer images of their final stage demonstrated the accuracy of the appliance in achieving the desired result (Fig. 7).
The post-treatment panoramic x-ray revealed excessive distal root tip of the lower right cuspid and a slight mesial root tip of the lower right incisor, along with mild root resorption of the lower right central incisor. The lateral cephalogram showed reduction of the overjet and increased proclination of the lower incisors (Table 1). Because the pre- and post-treatment lateral cephs were taken on different machines, the tracings were not superimposed. Superimposition of the occlusograms, however, revealed minor alignment with buccal expansion of the upper right second bicuspid, a shift of the mandibular midline to the right, and buccal expansion in the lower right second bicuspid region (Fig. 8).
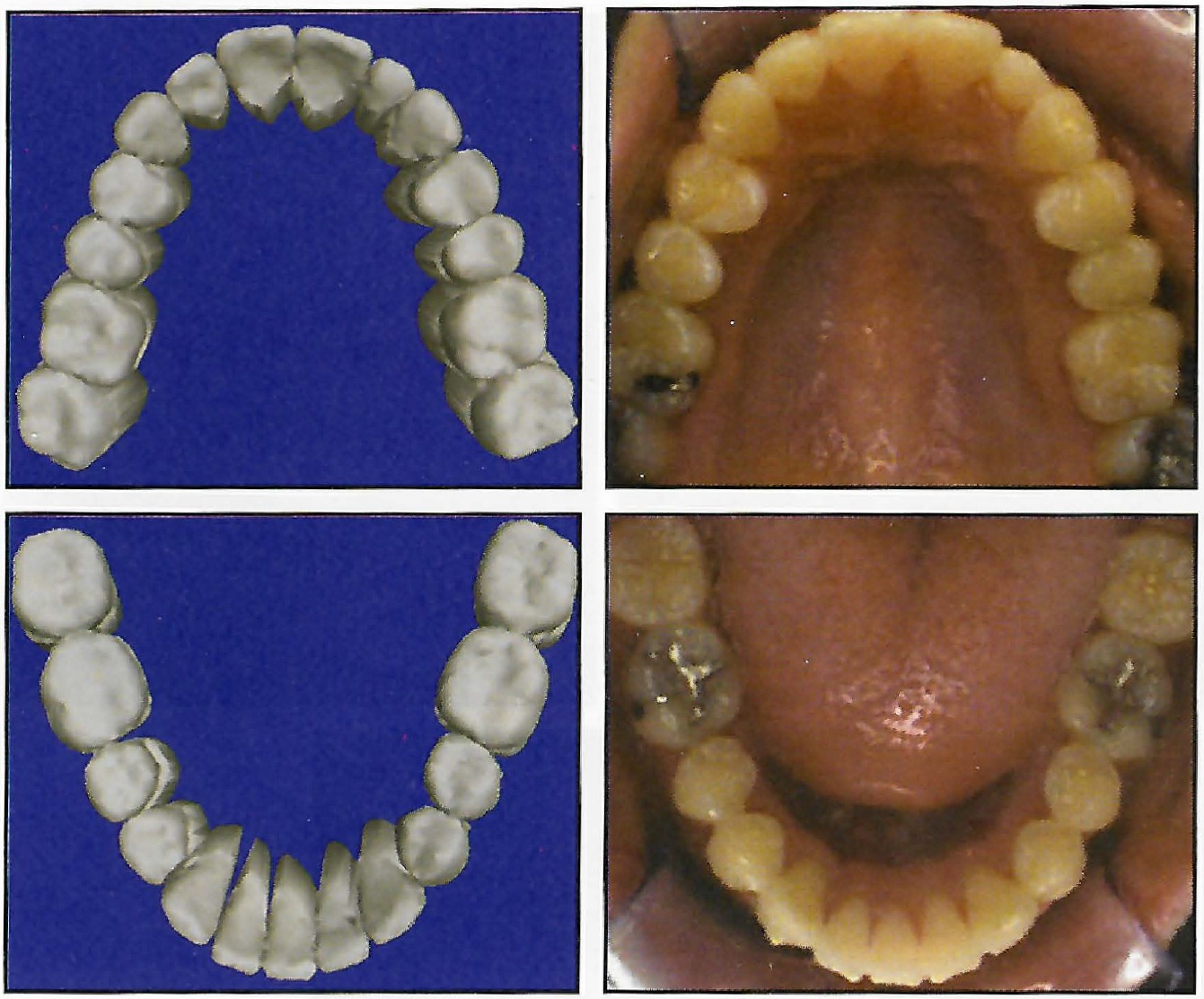
Fig. 7 Comparison of final-stage computer images and post-treatment intraoral photos.
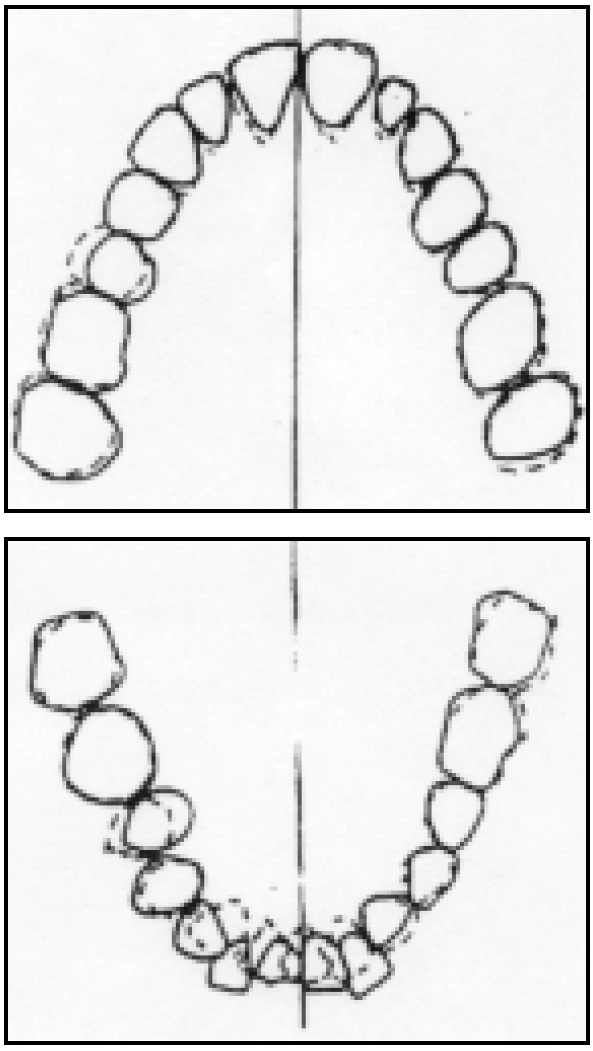
Fig. 8 Superimposition of pre- and post-treatment occlusograms.
Small interocclusal gaps between the first and second molars could be attributed to excessive forces placed on the posterior occlusion during aligner wear. Such spaces are usually transient in nature, but patients should be made aware that bite settling with appliances such as Hawley retainers, positioners, or up-and-down elastics may be required toward the end of treatment. In this case, the patient was given Hawley instead of vacuum-formed retainers, and the posterior occlusion settled, as evidenced by photographs take none year after retention (Fig. 9).

Fig. 9 Patient one year post-retention.
Discussion
The Invisalign System requires polyvinyl siloxane impressions for longer shelf life, better accuracy, and multiple pours. Full-arch impressions are difficult to take with this material, but are critical to the technique.
Invisalign treatment requires the clinician to plan out sequential movements for every tooth from beginning to end--a somewhat different diagnostic process than with conventional appliances. ClinCheck allows the clinician to evaluate the entire treatment carefully and critically in all three planes of space. In the present case, the increased proclination of the lower incisors was overlooked by the orthodontist during the ClinCheck procedure. This proclination may have exacerbated the gingival recession in the lower incisor region.
Tipping of the teeth into the extraction site may have been the result of overly aggressive tooth movement--as much as .38mm per week. That is more than the current Align Technology recommendation of .33mm per stage, with each aligner worn for two weeks.
All in all, however, it appears that lower incisor extraction was an appropriate choice in this case. The slight Class III tendency, Bolton discrepancy, well-aligned upper arch, and crowded lower arch all contributed to a good result.
This was the first lower incisor extraction case treated with the Invisalign System. The treatment time was comparable to that of fixed appliances, and therefore offers evidence of a viable alternative to conventional techniques.
ACKNOWLEDGMENTS: The authors would like to thank Amanda Ramirez for her help and Justin Tindall for his assistance with imaging.
REFERENCES
- 1. Owen, A.H. III: Single lower incisor extractions, J. Clin. Orthod. 27:153-160, 1993.
- 2. Sheridan, J.J.; LeDoux,W.; and McMinn, R.: Essix appliances: Minor tooth movement with divots and windows, J. Clin. Orthod. 28:659-663, 1994.
-
 DR. MILLER
DR. MILLER -
 DR. DUONG
DR. DUONG -
 DR. DERAKHSHAN
DR. DERAKHSHAN
Dr. Miller is Chief Clinical Officer, Dr. Duong is Director of Clinical Research, and Dr. Derakhshan is a Staff Orthodontist, Align Technology, Inc., 851 Martin Ave., Santa Clara, CA 95050. The authors are shareholders in the company. Dr. Duong is also in the private practice of orthodontics in Manteca, CA. Contact Dr. Miller at ross@aligntech.com.