CASE REPORT
Incisor Intrusion with Invisalign Treatment
Orthodontic intrusion can be effective in adult patients with periodontal disease,1,2 as long as light, continuous forces are used and excellent oral hygiene is maintained.3,4 Such treatment can reduce infrabony defects and improve periodontal health,5-7 but requires a multi-disciplinary approach8,9 and a highly motivated patient.
Stable posterior anchorage can be difficult to achieve in patients with missing teeth.10 Although skeletal anchorage may be useful, the following case demonstrates intrusion of the upper incisors using only removable Invisalign* appliances in an adult patient with periodontal disease.
Diagnosis and Treatment Planning
A 43-year-old female presented with extruded, protrusive, and labially inclined upper incisors and generalized anterior spacing (Fig. 1). A fixed prosthesis had replaced the upper right bicuspids and molars. Bleeding was evident on periodontal probing, and the patient had a flat upper labial frenum.
Similar articles from the archive:

Fig. 1 43-year-old female patient with extruded, protrusive, and labially inclined upper incisors, prosthetic replacement of upper right posterior segment, and periodontal disease before treatment.
Invisalign treatment was planned for derotation and intrusion of the upper incisors and canines and uprighting of the upper right central incisor. The lower arch required slight intercanine expansion to allow the alignment and uprighting of the upper incisors.
The final ClinCheck* provided 15 aligners for the upper arch and 10 for the lower (Fig. 2). The predicted duration of treatment was about eight months.
Treatment Progress
Scaling and root planing were performed before the start of orthodontic treatment, with the scaling repeated every eight weeks.
The first through 10th aligners were worn for 15 days each, except that a frenectomy was scheduled during the sixth aligner period to reshape the gingival marginal without traction from the upper frenum (Fig. 3). This aligner was worn for three weeks as the tissue healed.
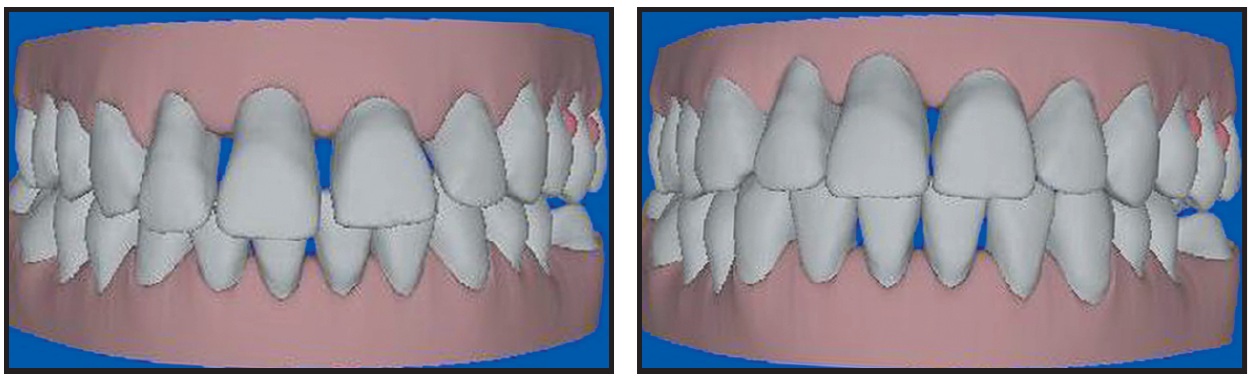
Fig. 2 Invisalign treatment planning with ClinCheck.
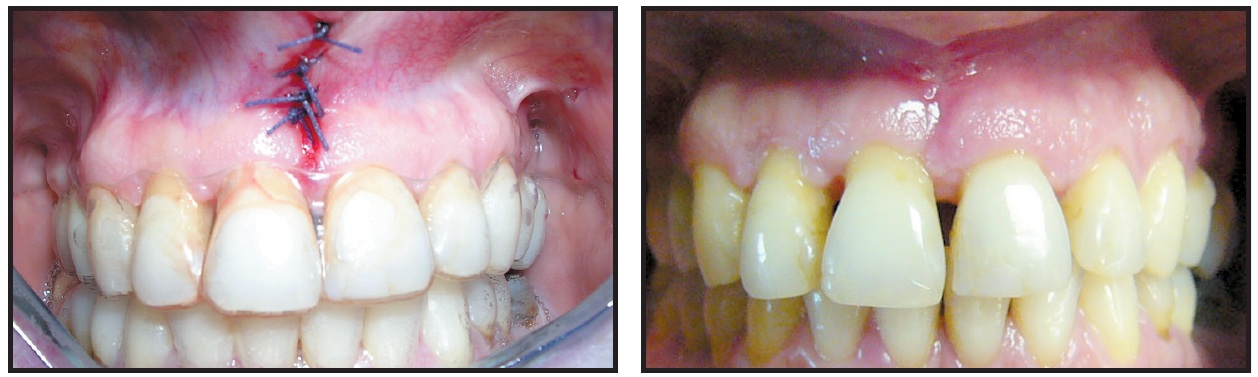
Fig. 3 Frenectomy performed to reshape gingival margin without traction from upper frenum.
The last five upper aligners were changed every three weeks, while the last lower aligner was being worn, to allow root movements. At the end of active treatment, the patient wore the last set of aligners for an additional four weeks. The entire Invisalign treatment lasted 11 months (Fig. 4). Fixed lingual retainers were then placed in both arches.
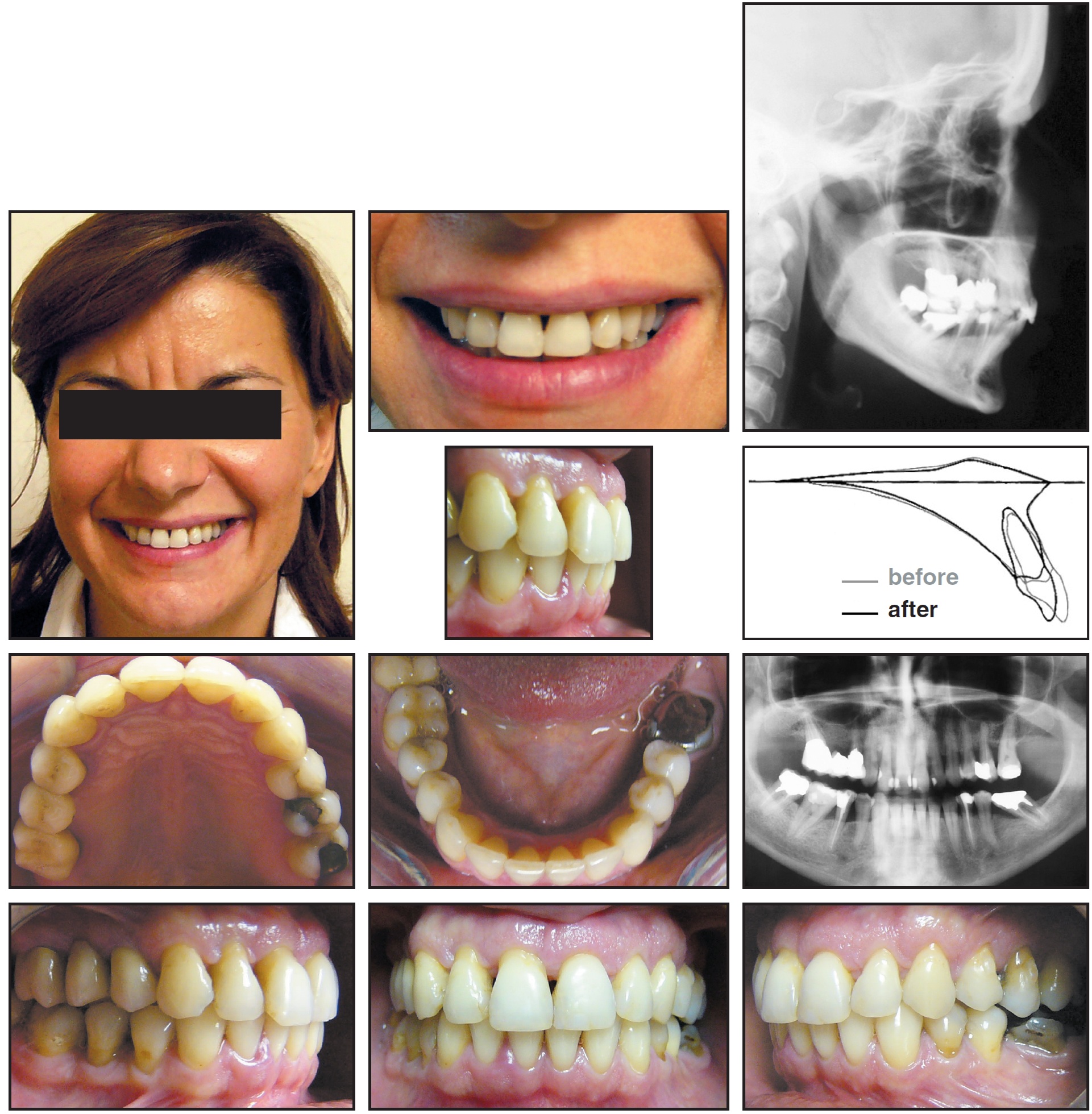
Fig. 4 Patient after 11 months of Invisalign treatment.
Discussion
Invisalign appliances provided a viable alternative to conventional orthodontic intrusion in this patient, aligning the extruded incisors in a relatively short time with no need to remove the posterior prosthesis. The post-treatment radiographs clearly showed upper incisor intrusion and a reduction of the infrabony defect.
Moving the teeth at a rate of about .25mm per aligner, Invisalign applies a light, continuous force.11 Attachments are bonded to the teeth adjacent to the extruded teeth to provide a mechanical lock for the aligners and to allow pure sectional intrusion, using the same biomechanics as the segmented-arch technique. The aligner dissipates the reactive force over the entire posterior segment, which serves as the anchorage unit.
In contrast to fixed orthodontic appliances, the aligners can be removed for eating and brushing, allowing optimal daily hygiene.12 The comfortable, esthetic appliances have been enthusiastically accepted by patients. Chairtime for aligner replacement is minimal, and the clinician can compare the patient's results with the virtual ClinCheck images to immediately verify treatment progress.
FOOTNOTES
- *Registered trademark of Align Technology, Inc., 851 Martin Ave., Santa Clara, CA 95050.
REFERENCES
- 1. Melsen, B.; Agerbaek, N.; and Markenstam, G.: Intrusion of incisors in adult patients with marginal bone loss, Am. J. Orthod. 96:232-241, 1989.
- 2. Cardaropoli, D.; Re, S.; Corrente, G.; and Abundo, R.: Intrusion of migrated incisors with infrabony defects in adult periodontal patients, Am. J. Orthod. 120:671-675, 2001.
- 3. Wennstrom, J.L.; Stokland, B.L.; Nyman, S.; and Thilander, B.: Periodontal tissue response to orthodontic movement of teeth with infrabony pockets, Am. J. Orthod. 103:313-319, 1993.
- 4. Boyd, R.L.; Leggott, P.J.; Quinn, R.S.; Eakle, W.S.; and Chambers, D.: Periodontal implications of orthodontic treatment in adults with reduced or normal periodontal tissues versus adolescents, Am. J. Orthod. 96:191-198, 1989.
- 5. Thilander, B.: Infrabony pockets and reduced alveolar bone height in relation to orthodontic therapy, Semin. Orthod. 2:55-61, 1996.
- 6. Polson, A.; Caton, J.; Polson, A.P.; Nyman, S.; Novak, J.; and Reed, B.: Periodontal response after tooth movement into infrabony defects, J. Periodontol. 55:197-202, 1984
- 7. Boyd, R.L. and Baumrind, S.: Periodontal considerations in the use of bonds or bands on molars in adolescents and adults, Angle Orthod. 62:117-126, 1992
- 8. Vanarsdall, R.L. Jr.: Adjunctive orthodontics for the generalist, J. Tenn. Dent. Assoc. 59:15-18, 1979.
- 9. Musich, D.R. and Crossetti, H.W.: Assessment and description of the treatment needs of adult patients for orthodontic therapy, III. Characteristics of the multiple provider group, Int. J. Adult Orthod. Orthog. Surg. 1:251-274, 1986.
- 10. Burstone, C.J.: Deep overbite correction by intrusion, Am. J. Orthod. 72:1-22, 1977
- 11. Clements, K.M.; Bollen, A.M.; Huang, G.; King, G.; Hujoel, P.; and Ma, T.: Activation and material stiffness of sequential removable orthodontic appliances, Part 2: Dental improvements, Am. J. Orthod. 124:502-508, 2003.
- 12. Taylor, M.G.; McGorray, S.P.; Durrett, S.; Pavlov, S.; Downey, N.; Lenk, M.; Oxford, E.; Dolce, C.; and Wheeler, T.T.: Effect of Invisalign aligners on periodontal tissues, J. Dent. Res. 82 (Spec. Iss. A):1483, 2003.
-
 DR. TURATTI
DR. TURATTI -
 DR. WOMACK
DR. WOMACK -
 DR. BRACCO
DR. BRACCO
Dr. Turatti is in the private practice of orthodontics at via F. Paolini 12, 10138 Turin, Italy. Dr. Womack is an Associate Professor, Orthodontic Department, Arthur A. Dugoni School of Dentistry, University of the Pacific, San Francisco; he has presented educational workshops for Align Technology as an independent contractor. Dr. Bracco is Chairman, Department of Orthodontics, University of Turin, Italy. E-mail Dr. Turatti at gaetanoturatti@aliceposta.it.