Pink Esthetic Score Evaluation of Gingival Esthetics after Clear Aligner Treatment of Palatally Impacted Canines
Although the superior esthetics and comfort of clear aligners have led to their widespread use,1 their effectiveness in treating severe cases has not been conclusively demonstrated. Impacted maxillary canines are among the more difficult orthodontic problems to manage,2,3 not only because of the complex biomechanics involved, but also because of the potential of treatment to significantly affect facial appearance.
According to Zachrisson, the inclination and torque of the canines are crucial to smile esthetics.4 Failure to adequately control canine traction can negatively affect the appearance of the gingiva,5 resulting in irregularities such as inflammation and recession.2 The esthetics of the surrounding soft tissue after retraction of an impacted canine are therefore an essential criterion by which treatment success can be evaluated.6 Key elements of gingival esthetics include right-left symmetry of the gingival margins, with differences of at least .5mm detectable by experts and 2mm by laypersons,7 as well as the location and level of the gingival zenith, which should be distal to the long axis of the tooth, at the same height as the zeniths of the central incisors.8
Similar articles from the archive:
The Pink Esthetic Score (PES) assesses soft-tissue esthetics by comparing the gingiva of a treated tooth to that of the untreated contralateral tooth9-11; it has previously been used to evaluate unilateral lateral-incisor implants12,13 and canine autotransplantation cases.14 The present study used the PES to assess the appearance of the gingiva after Invisalign* clear aligner therapy for unilateral palatally impacted maxillary canines.
Materials and Methods
This cross-sectional retrospective study was approved by the institutional review board at the European University College, Dubai, United Arab Emirates, and involved 20 patients, 12 male and eight female, with unilateral palatal or midalveolar impacted canines. Subjects were treated consecutively with Invisalign by a single clinician in France between 2015 and 2020. Exclusion criteria were the presence of bilateral impactions, preexisting gingival or periodontal disease, and previous extractions.
Post-treatment intraoral photographs were taken on the day of treatment completion and shown to 10 evaluators (four orthodontists and six esthetic dentists), who were asked to complete a PES card for each photograph (Fig. 1).
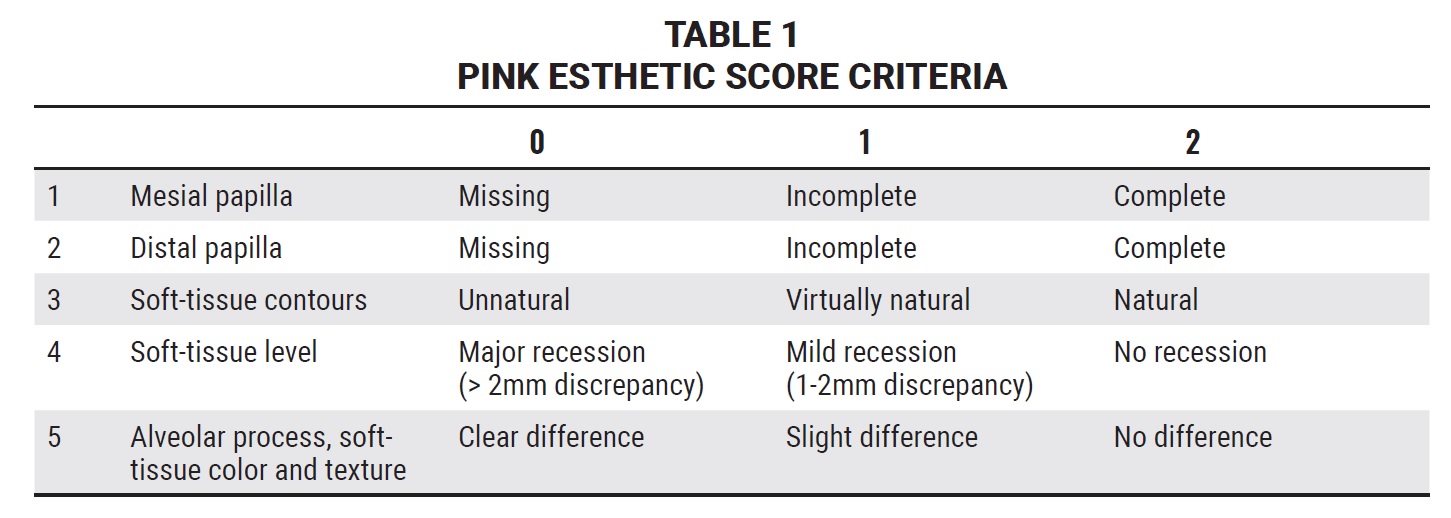
The PES index assesses five variables: the mesial papilla, the distal papilla, soft-tissue contours, gingival levels, and a combination of the alveolar profile and the color and texture of the mucosa (Table 1). Each variable is given a score between 0 and 2, with 2 indicating a healthy, normal periodontium; 1, a slight change; and 0, a marked change. The scores are added together to produce an overall score out of a maximum of 10. Belser and colleagues suggested a score of 6 as the threshold of clinical acceptability when comparing lateral-incisor implants to natural lateral incisors.15 We raised this threshold to 7 in our study, since a better gingival architecture can be expected for natural teeth.

Fig. 1 Sample lateral intraoral photographs used for Pink Esthetic Score (PES) evaluation.
Treatment mechanics in each of the 20 cases varied depending on the needs of the patient (Fig. 2). Although a comparison of treatment modalities was outside the scope of the study, the general protocol was as follows: The teeth were aligned, and space was created for the canine. The impacted canine was then exposed with either the open (six patients) or closed (14 patients) surgical technique. After the procedure, passive aligners were worn, and various mechanics were used for traction, depending on the position and inclination of the canine.

Fig. 2 Sample case treated with lingual cleat, elastomeric chains, and interarch elastics. A. Initial records. B. Treatment progress. C. Final records.
For simpler impactions, elastics were worn from the canine to hooks on the aligners (Fig. 3A), while in more complex cases, two palatal temporary anchorage devices (TADs) were inserted to support a ballista or cantilever spring (Fig. 3B). In a few patients, sectional fixed lingual appliances were used to enhance anchorage, or attachment points were added to provide better force vectors for elastomeric chains (Fig. 3C). Once the canine was nearly in position, the fixed sectional appliances assisted in the correction of its inclination and rotation.
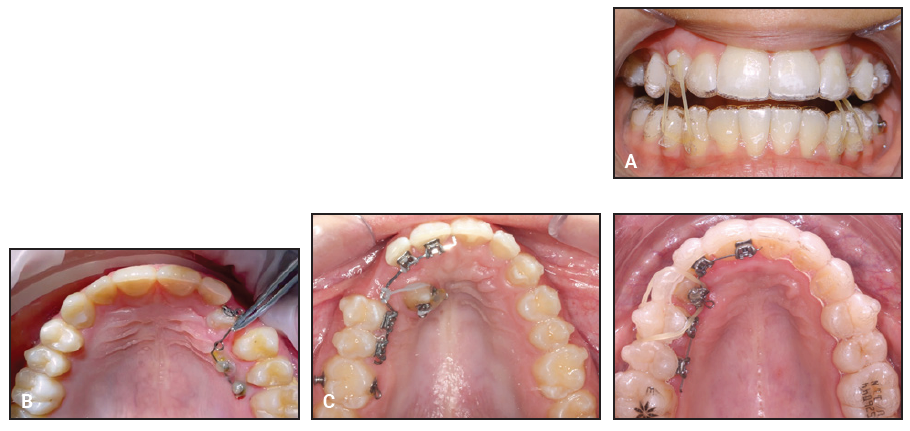
Fig. 3 Treatment modalities used in study. A. Elastics worn from impacted canines to hooks on lower aligners. B. Two palatal miniscrews inserted for attachment of ballista or cantilever spring. (Photo courtesy of Dr. Alessandro Mario Greco.) C. Sectional fixed lingual appliances used to add points of attachment for elastomeric chains and assist in correction of canine inclination and rotation.
Results
Mann-Whitney U tests were performed to compare individual components of the PES, while an independent-samples t-test was used to compare the mean total scores. The significance level was set at p < .05.
The contralateral control teeth received significantly higher scores than the treated teeth for the mesial papillae and soft-tissue contours, although both had median scores of 2 (Table 2).
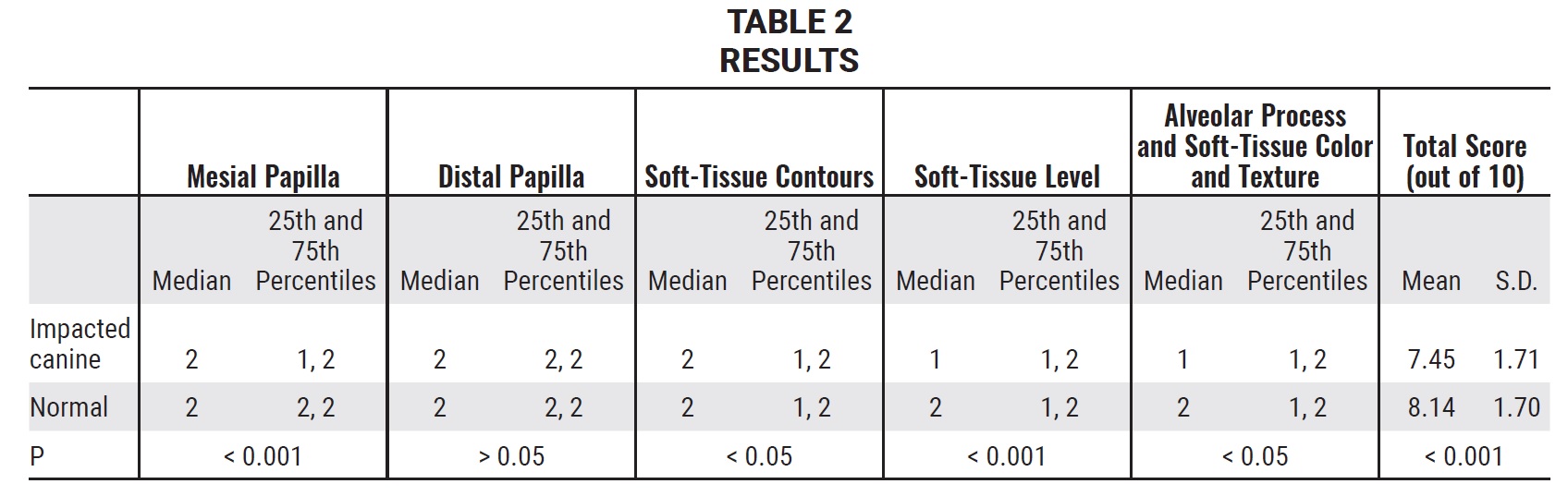
Significant differences were also found in the gingival-level scores (p < .001) and the combined scores for the alveolar process profile and mucosal color and texture (p < .05), with a median of 1 for the treated canines and 2 for the controls. There was no significant difference in the scores for the distal papillae (p > .05). The mean total score of the treated impacted canines (7.45) was significantly lower than that of the contralateral canines (8.14, p < .001), but both exceeded the threshold of clinical acceptability (Fig. 4).
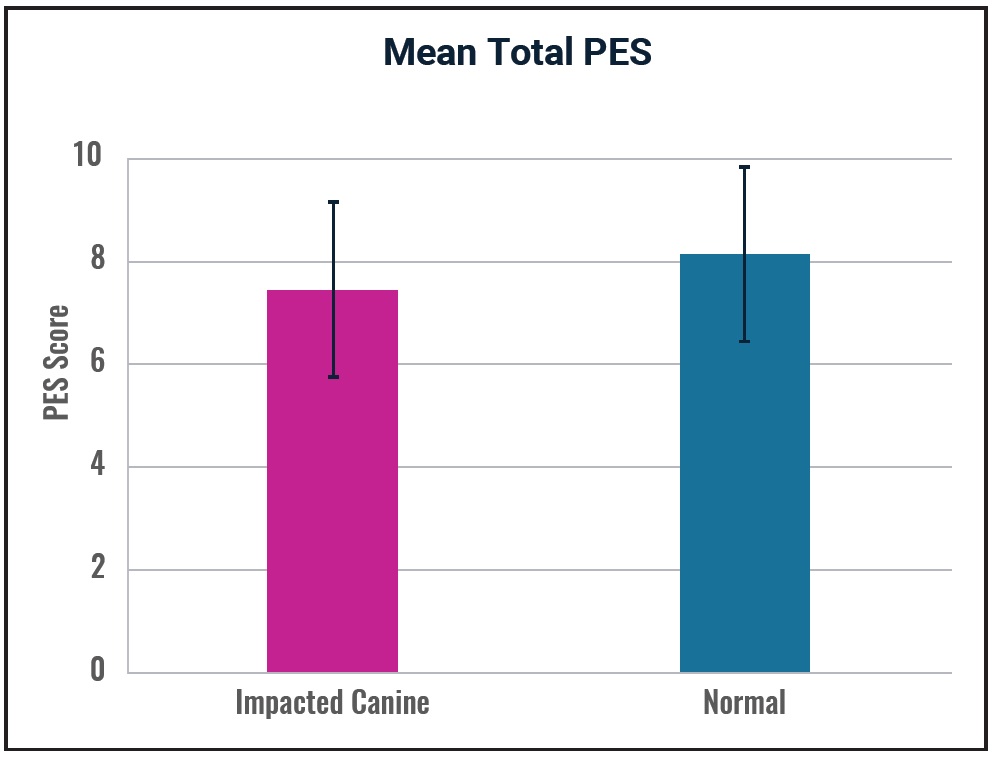
Fig. 4 Mean total PES of treated and contralateral control canines.
Discussion
A previous study of impacted canines treated with fixed appliances found that laypeople could identify the treated tooth in about 50% of cases and orthodontists in about 60%, suggesting that the esthetic impact of canine retraction is unlikely to be detectable by the general population.16 Our study of impacted canines treated with Invisalign likewise showed only a minor effect on soft-tissue esthetics. Although the mean total PES of the treated canines was lower than that of the contralateral canines, the difference was only .69, suggesting that the overall disparity in gingival esthetics was of minimal clinical significance, with differences likely to be detected only in the alveolar process and in soft-tissue level, color, and texture.
On average, the gingival levels of the treated canines were 1-2mm lower than those of the controls, validating the results of another study of impacted canines treated with fixed appliances, in which the treated teeth showed a substantial difference in clinical crown height and an average .4mm of gingival recession and .5mm of attachment loss.17 The 1-2mm discrepancy found in our study is on the border of clinical significance; whether it is an acceptable outcome will depend on the preferences of patients and clinicians.
The composite score for the alveolar-process profile and soft-tissue color and texture reflects multiple aspects of periodontal health. An erythematous color can be a sign of gingivitis—a common finding after orthodontic treatment, especially in immediate post-treatment photographs. A canine that has erupted through the alveolar rather than the keratinized mucosa may also display increased erythema and poor esthetics. An excessively prominent canine root or an alveolar deficiency due to a lack of root prominence can result from inadequate torque control. Because auxiliary appliances, including TADs and lingual fixed appliances, were used for torque control in our sample when aligners alone would not have been sufficient,18 only minor deviations from the norm occurred, comparable to those found after treatment with fixed appliances.19
Our study showed no significant difference in the scores for the distal papillae but a significant difference in scores for the mesial papillae (despite median scores of 2 for both criteria). This observation is corroborated by Woloshyn and colleagues20 and Hansson and Rindler,21 who also found greater periodontal effects on the mesial aspects of the canines. The reasons for such results remain unclear, but may involve preexisting bone levels. Both studies questioned the clinical relevance of this finding, given the minor differences noted.
Other than case reports, this is the first study to investigate the esthetic effectiveness of Invisalign therapy in the treatment of palatally impacted canines. Limitations include a small sample size, owing to the relative novelty and complexity of treating impacted canines with clear aligners. This was also a single-center study, with the patients treated by a single clinician using a variety of mechanics and auxiliaries. Finally, because the photographs used for assessment were taken at the debonding appointments, they may have indicated gingival irritation that could be attributable to the recent orthodontic treatment.
The small difference in the PES of the treated and control canines suggests that clear aligner treatment of palatally impacted canines, in conjunction with auxiliary appliances, can produce acceptable gingival esthetics. A comparison of the efficiency of Invisalign and conventional fixed appliances in the treatment of impacted canines is an area for further research.
FOOTNOTES
- *Trademark of Align Technology, Inc., San Jose, CA; www.aligntech.com.
REFERENCES
- 1. AlSeraidi, M.; Hansa, I.; Dhaval, F.; Ferguson, D.J.; and Vaid, N.R.: The effect of vestibular, lingual, and aligner appliances on the quality of life of adult patients during the initial stages of orthodontic treatment, Prog. Orthod. 22:3, 2021.
- 2. Kokich, V.G.: Surgical and orthodontic management of impacted maxillary canines, Am. J. Orthod. 126:278-283, 2004.
- 3. Mampieri, G.; Castroflorio, T.; Conigliaro, A.; and Giancotti, A.: Treatment of impacted canines with aligners: An alternative and viable option, Clin. Case Rep. 9:e04856, 2021.
- 4. Zachrisson, B.U.: Esthetic factors involved in anterior tooth display and the smile: Vertical dimension, J. Clin. Orthod. 32:432-445, 1998.
- 5. Sarver, D.M.: Enameloplasty and esthetic finishing in orthodontics- identification and treatment of microesthetic features in orthodontics, Part 1, J. Esth. Restor. Dent. 23:296-302, 2011.
- 6. Crescini, A.; Nieri, M.; Buti, J.; Baccetti, T.; and Pini Prato, G.P.: Orthodontic and periodontal outcomes of treated impacted maxillary canines, Angle Orthod. 77:571-577, 2007.
- 7. Pinho, S.; Ciriaco, C.; Faber, J.; and Lenza, M.A.: Impact of dental asymmetries on the perception of smile esthetics, Am. J. Orthod. 132:748-753, 2007.
- 8. Sarver, D.M.: Principles of cosmetic dentistry in orthodontics: Part 1—Shape and proportionality of anterior teeth, Am. J. Orthod. 126:749-753, 2004.
- 9. Fürhauser, R.; Florescu, D.; Benesch, T.; Haas, R.; Mailath, G.; and Watzek, G.: Evaluation of soft tissue around single-tooth implant crowns: The pink esthetic score, Clin. Oral Implants Res. 16:639-644, 2005.
- 10. Brandão, R.C.B. and Brandão, L.B.C.: Finishing procedures in orthodontics: Dental dimensions and proportions (microesthetics), Dent. Press J. Orthod. 18:147-174, 2013.
- 11. Gehrke, P.; Lobert, M.; and Dhom, G.: Reproducibility of the pink esthetic score—rating soft tissue esthetics around single-implant restorations with regard to dental observer specialization, J. Esth. Restor. Dent. 20:375-384, 2008.
- 12. Schneider, U.E.; Moser, L.; Pellitteri, G.; and Siciliani, G.: Orthodontic space closure vs. implant-borne crowns in patients with congenitally missing maxillary lateral incisors, J. Clin. Orthod. 52:284-296, 2018.
- 13. Schneider, U.E.M. and Moser, L.: Substituting congenitally missing maxillary lateral incisors with implant-borne crowns: A topic still worth a discussion, Semin. Orthod. 26:33-51, 2020.
- 14. Yu, H.J.; Qiu, L.X.; and Wang, X.Z.: Long-term follow-up of autogenous canine transplants with application of guided bone regeneration, Int. J. Oral Maxillofac. Surg. 43:355-361, 2014.
- 15. Belser, U.C.; Grütter, L.; Vailati, F.; Bornstein, M.M.; Weber, H.P.; and Buser, D.: Outcome evaluation of early placed maxillary anterior single-tooth implants using objective esthetic criteria: A cross-sectional, retrospective study in 45 patients with a 2- to 4-year follow-up using pink and white esthetic scores, J. Periodontol. 80:140-151, 2009.
- 16. Parkin, N.A.; Freeman, J.V.; Deery, C.; and Benson, P.E.: Esthetic judgments of palatally displaced canines 3 months postdebond after surgical exposure with either a closed or an open technique, Am. J. Orthod. 147:173-181, 2015.
- 17. Parkin, N.A.; Milner, R.S.; Deery, C.; Tinsley, D.; Smith, A.M.; Germain, P.; Freeman, J.V.; Bell, S.J.; and Benson, P.E.: Periodontal health of palatally displaced canines treated with open or closed surgical technique: A multicenter, randomized controlled trial, Am. J. Orthod. 144:176-184, 2013.
- 18. Haouili, N.; Kravitz, N.D.; Vaid, N.R.; Ferguson, D.J.; and Makki, L.: Has Invisalign improved? A prospective follow-up study on the efficacy of tooth movement with Invisalign, Am. J. Orthod. 158:420-425, 2020.
- 19. Becker, A.; Kohavi, D.; and Zilberman, Y.: Periodontal status following the alignment of palatally impacted canine teeth, Am. J. Orthod. 84:332-336, 1983.
- 20. Woloshyn, H.; Årtun, J.; Kennedy, D.B.; and Joondeph, D.R.: Pulpal and periodontal reactions to orthodontic alignment of palatally impacted canines, Angle Orthod. 64:257-264, 1994.
- 21. Hansson, C. and Rindler, A.: Periodontal conditions following surgical and orthodontic treatment of palatally impacted maxillary canines: A follow-up study, Angle Orthod. 68:167-172, 1998.
-
 DR. SABOUNI
DR. SABOUNI -
 DR. HANSA
DR. HANSA -
 DR. SHAH
DR. SHAH -
 DR. ADEL
DR. ADEL -
 DR. VAIID
DR. VAIID
Dr. Sabouni is in the private practice of orthodontics in Sanary-sur-Mer, France, and is a paid speaker for Align Technology, Inc. Dr. Hansa is in the private practice of orthodontics, Dr. Hansa Orthodontics, 9 Kensington Drive, Westville, Durban 3629, South Africa; e-mail: drismaeelhansa@gmail.com. Dr. Shah is in the private practice of orthodontics in Mumbai, India. Dr. Adel is a Lecturer, Faculty of Dentistry, Alexandria University, Alexandria, Egypt. Dr. Vaiid is an Adjunct Professor, Department of Orthodontics, Saveetha Dental College, Saveetha Institute of Medical and Technical Sciences, Chennai, India.
