CASE REPORT
Early Management of an Edge-to-Edge Incisor Occlusion
An edge-to-edge incisor relationship can be a clinical manifestation of other anomalies, including a Class III malocclusion caused by forward sagittal displacement of the mandible, or a Class I pseudo-infraclusion induced by sagittal proclination of the incisors.1-3 This multifactorial anomaly is more common in the mixed dentition, with a prevalence of 17-18%, and is primarily found in children between the ages of 7 and 9, when it is associated with incomplete eruption of the incisors.5
Lack of anterior guidance is one of the principal causes of occlusal instability and TMD.6,7 Moreover, the absence of overjet and overbite can allow uninhibited mandibular growth, resulting in a true skeletal Class III relationship.2 Early interception is therefore crucial to achieving satisfactory esthetic and functional results.4,8-10
The following case demonstrates interceptive treatment of an edge-to-edge bite in the mixed dentition.
Diagnosis and Treatment Planning
An 8-year-old male presented with the chief complaint of an edge-to-edge incisor occlusion (Fig. 1). Clinical examination found an oval and symmetrical face with normal length, a marked labiomental furrow, and an 85° nasolabial angle. The lips closed without contraction of the perioral muscles, and a timid and unesthetic smile revealed only a portion of the upper incisors. The patient had 1mm Class III molar and canine relationships, a thin periodontium, an anterior edge-to-edge occlusion, and coincident midlines.
Similar articles from the archive:
- A Quick Fix for Pseudo-Class III Correction December 2008
- Transforce Lingual Appliances for Arch Development March 2005
- JCO ROUNDTABLE Early Orthodontic Treatment, Part 1 February 2004
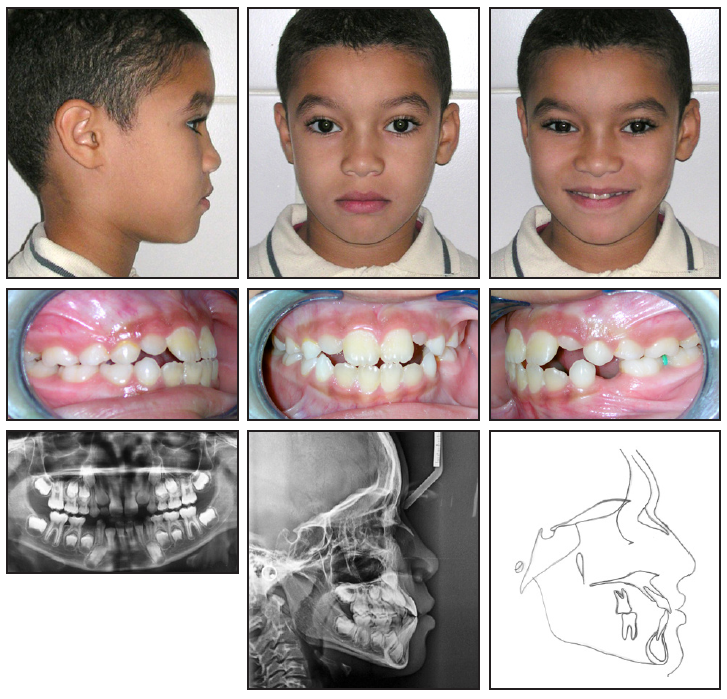
Fig. 1 8-year-old male patient with edge-to-edge incisor occlusion, proclined lower incisors, Class III molar and canine relationships, and normodivergent facial pattern before treatment.
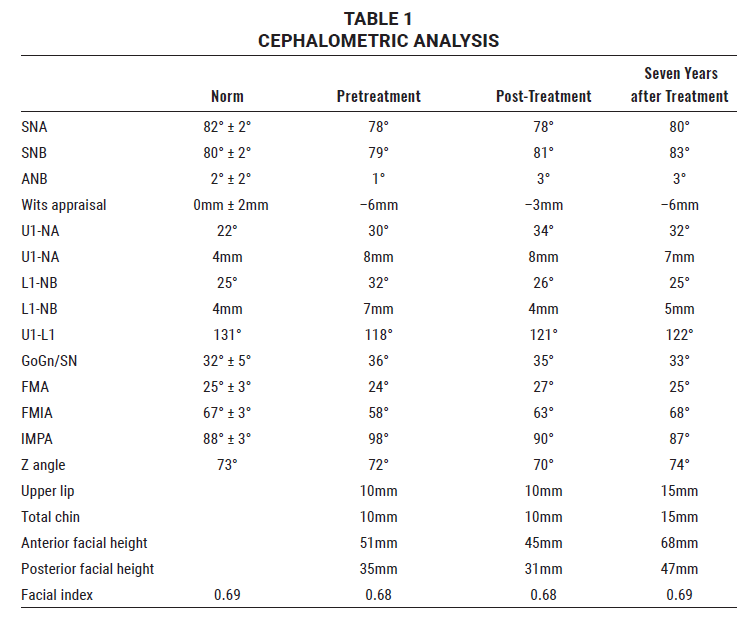
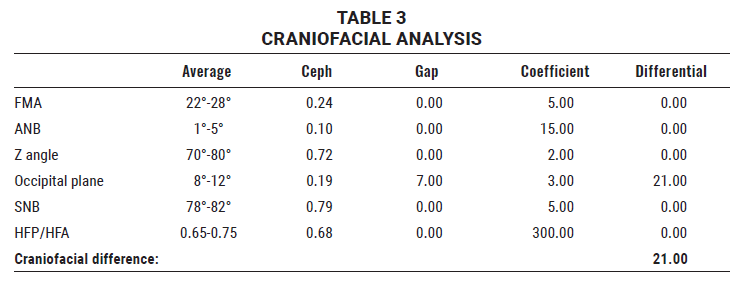
The panoramic radiograph confirmed that the patient was in the mixed dentition with good dental and periodontal health. Cephalometric analysis indicated a skeletal Class III relationship and alveolar incisor protrusion (Table 1).
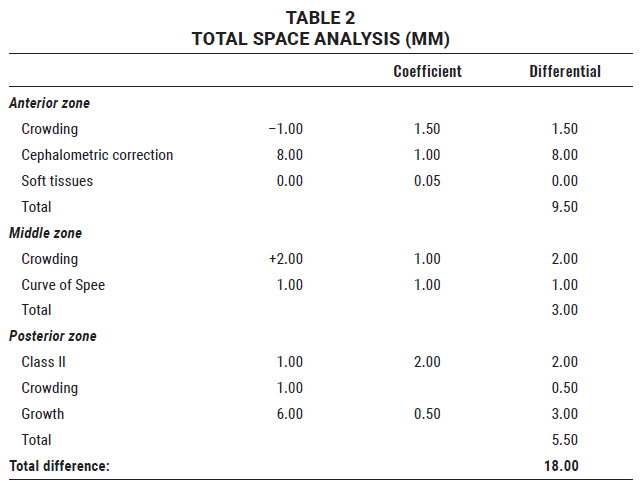
Total space analysis showed mild anterior crowding with a shallow curve of Spee (1mm), while a cephalometric correction value of 8 evidenced proclination of the lower incisors (Table 2).
Treatment goals were to restore a normal overjet and overbite and thus reorient the growth of basal bones, guide dental eruption in the buccal regions to rebuild the occlusion from front to back, restore a stable and functional Class I occlusion, correct the lower-incisor proclination, and maintain harmonious interarch relationships in the transverse dimension.
Treatment Progress
After the patient received oral-hygiene instruction, the lower deciduous canines were extracted. This space allowed the lower incisors to move distally and establish a normal overjet and overbite (Fig. 2A). Regular appointments were scheduled to monitor the development of the permanent teeth.
After dental alignment and arch coordination were achieved (Fig. 2B), the finishing stage involved refinement of the anterior and buccal occlusion, correction of the canine and molar relationships, and normalization of the overjet and overbite (Fig. 2C).

Fig. 2 A. After extraction of lower deciduous canines, lower arch bonded with 2 × 4 appliance to move incisors into created spaces. B. Dental alignment and arch coordination after six months of treatment. C. After 12 months of finishing and intercuspation with preadjusted brackets and full-size, rigid stainless steel archwires.
Treatment Results
Total treatment time was two years (Fig. 3). The patient’s soft-tissue harmony was preserved (Z angle = 70°), and he exhibited a symmetrical face and a pleasant smile. He had Class I molar and canine relationships, a normal overjet and overbite, coincident midlines, and a maxillary arch circumscribing the mandibular arch.
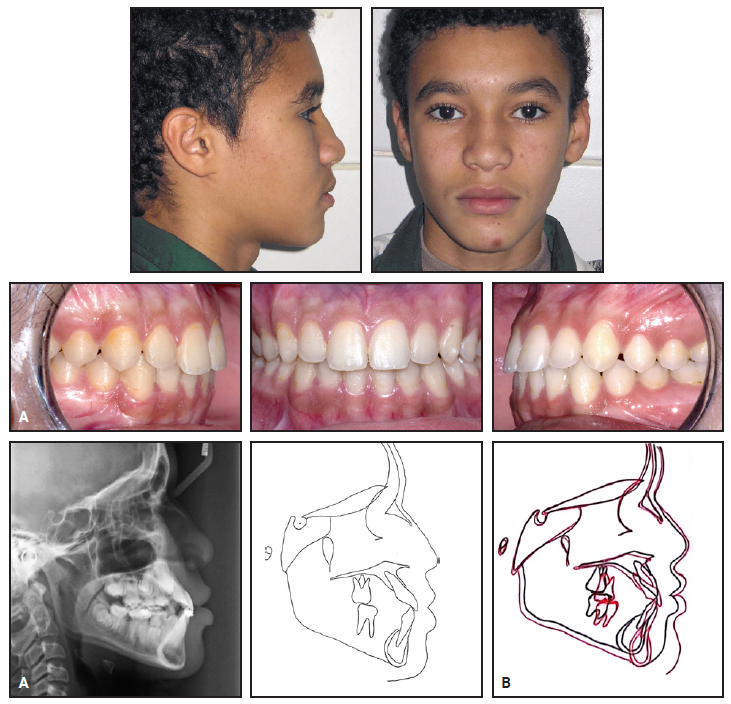
Fig. 3 A. Patient after two years of treatment. B. Superimposition of pre- and post-treatment cephalometric tracings.
Cephalometric analysis confirmed a satisfactory lower-incisor angulation, with the teeth well centered in the symphysis (Table 1). The interincisal angle therefore increased from 118° to 121°. Counterclockwise rotation of the mandible enabled correction of the open bite. The skeletal Class III was considerably improved, as evidenced by an increase in the Wits appraisal from –6mm to –3mm. The facial pattern, although slightly altered, remained normodivergent (GoGn/SN = 35°).
Seven years later, the treatment results and growth remodeling were stable (Fig. 4). The overjet and overbite helped maintain the normodivergent pattern, the corrected position of the lower incisors, and the Class I occlusal relationship, despite the mandibular growth pattern. The profile was balanced, ensuring a good labiomental relationship, but the upper lip was more supported than it was before treatment.
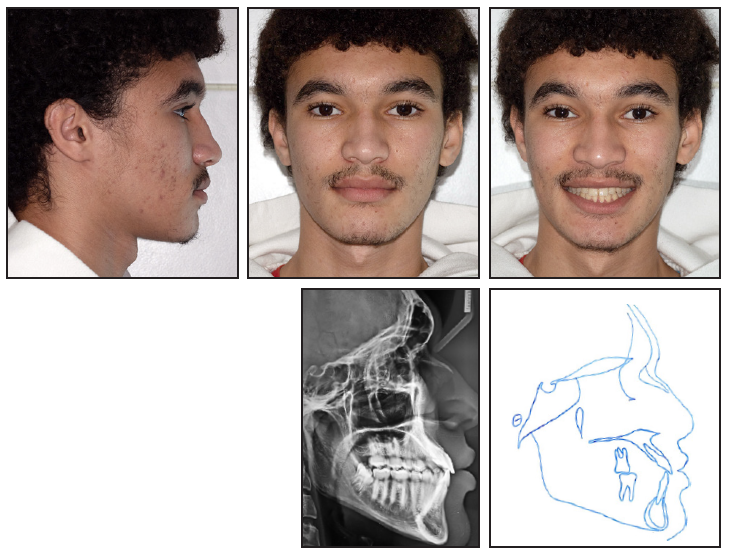
Fig. 4 Patient seven years after treatment.
Discussion
An edge-to-edge incisor occlusion in a young child can be resolved by orthodontic camouflage treatment and by growth reorientation, based on differential growth of the maxilla compared to the mandible. Early intervention can ameliorate or even eliminate many dental and skeletal abnormalities. For optimal results to be achieved, however, the patient should meet certain criteria, including a normodivergent or hypodivergent vertical pattern, a mild to moderate sagittal discrepancy, an absence of transverse deficiency, and a relatively normal esthetic appearance.12
The patient shown here benefited from a short treatment that avoided surgery and preserved the entire permanent dentition. Normal overjet and overbite were restored by relocation of the lower incisors. Counterclockwise mandibular rotation and the corrected overjet and overbite helped inhibit excessive mandibular growth, maintain a harmonious vertical pattern, and prevent relapse.
REFERENCES
- 1. Rosa, M.; Quinzi, V.; and Marzo, G.: Anterior open bite in the mixed dentition, Eur. J. Paediat. Dent. 20:80-82, 2019.
- 2. Pellegrino, M.; Caruso, S.; Cantile, T.; Pellegrino, G.; and Ferrazzano, G.F.: Early treatment of anterior crossbite with eruption guidance appliance: A case report, Int. J. Environ. Res. Pub. Health 17:3587, 2020.
- 3. Abdul-Wajid, M.; Chandra, P.; Kulshrestha, R.; Singh, K.; Rastogi, R.; and Umale, V.: Open bite malocclusion: An overview, J. Oral Health Craniofac. Sci. 3:11-20, 2018.
- 4. Kuljic, B.: Challenges in treating edge-to-edge incisal position for esthetics, Compend. Cont. Ed. Dent. 38:172-178, 2017.
- 5. Tausche, E.; Luck, O.; and Harzer, W.: Prevalence of malocclusions in the early mixed dentition and orthodontic treatment need, Eur. J. Orthod. 26:237-244, 2004.
- 6. Suzuki, S.S.; Previdente, L.H.; Garcez, A.S.; and Suzuki, H.: Camouflage treatment of severe bialveolar protrusion in skeletal Class II using miniscrew anchorage, Int. J. Orthod. Milwaukee 24:51-55, 2013.
- 7. Laplanche, O. et al.: Dysfunction of the masticatory apparatus [in French], Encycl. Méd. Chir. (Paris) 15:23435E20, 2001.
- 8. Schopf, P.: Indication for and frequency of early orthodontic therapy or interceptive measures, J. Orofac. Orthop. 64:186-200, 2003.
- 9. Al Hamadi, W.; Saleh, F.; and Kaddouha, M.: Orthodontic treatment timing and modalities in anterior open bite: Case series study, Open Dent. J. 11:581-594, 2017.
- 10. Pisani, L.; Bonaccorso, L.; Fastuca, R.; Spena, R.; Lombardo, L.; and Caprioglio, A.: Systematic review for orthodontic and orthopedic treatments for anterior open bite in the mixed dentition, Prog. Orthod. 17:28, 2016.
- 11. Horn, A.J. and Englebert, M.: Tweed analysis: An original approach to the analysis of the total dentition space [in French], Rev. Orthop. Dento-Fac. 2:165-172, 1978.
- 12. Regragui, S. and Zaoui, F.: A functional anomaly: Mandibular forward shift [in French], Actual. Odonto-Stomatol. 247:231-239, 2009.
-
 DR. NEANI
DR. NEANI -
 DR. ZAOUI
DR. ZAOUI -
 DR. AZAROUAL
DR. AZAROUAL
Dr. Neani is a Professor and Chair and Drs. Zaoui and Azaroual are Professors, Department of Orthodontics and Dentofacial Orthopedics, Dental Consultation and Treatment Center, University of Dental Medicine, Mohammed V University, Avenue Allal El Fassi, Mohammed Jazouli Street, Al Irfane, BP 6212, Rabat Institute, Rabat, Morocco. E-mail Dr. Neani at houda.neani1@gmail.com.