ALIGNER CORNER
Prospective Multicenter Investigation of Invisalign Treatment with the Mandibular-Advancement Feature: An Interim Report
This JCO column is compiled by Contributing Editor William V. Gierie, DDS, MS. Every few months, Dr. Gierie will introduce a pertinent article related to clear aligner therapy. Your suggestions for future topics or authors are welcome.
This edition of the Aligner Corner features two complementary articles on the Invisalign* mandibular-advancement (MA) feature. The first is an interim report on a prospective multicenter investigation. A number of measurements were examined, but a 3.36mm reduction in overjet struck me as both statistically and clinically significant. The authors observed that most of the Class II correction was dentoalveolar in nature, with minor skeletal changes.
I have used the MA feature extensively in my practice, and as both articles point out, it has some important benefits over other techniques. First, dental alignment and Class II correction can occur simultaneously. Second, the mandibular advancement is programmed incrementally (about 2mm every eight weeks), improving patient adaptation and comfort as compared with the one-step advancement of a conventional functional appliance. One advantage not mentioned is that the Invisalign MA fails “safe”—in other words, when problems occur, they don’t create significant patient discomfort. We all strive for effective, efficient treatment, but we should also strive for an excellent patient experience. Invisalign MA seems to hit all three goals. I look forward to seeing the final results of the multicenter trial.
WVG
Prospective Multicenter Investigation of Invisalign Treatment with the Mandibular-Advancement Feature: An Interim Report
Similar articles from the archive:
- Mandibular Advancement in Adult Skeletal Class II Patients Using Clear Aligners and Photobiomodulation January 2021
- Functional Class II Treatment with a Miniplate-Anchored Herbst Appliance April 2021
- CASE REPORT Carriere Motion Appliance with Miniscrew Anchorage for Treatment of Class II, Division 1 Malocclusion October 2020
The incidence of Class II malocclusion in North America is estimated to be 19.56%.1 Various methods have been devised for correction of this malocclusion, which is often characterized by mandibular retrognathia and excessive overjet.2 Functional appliances that reposition the mandible forward—including the Twin Block,** bionator, Mandibular Anterior Repositioning Appliance*** (MARA), and Herbst† appliance—can be used to correct Class II relationships in growing patients. Clinical studies have demonstrated the effectiveness of such appliances, as indicated by reduced overjet, improved molar and canine relationships, and orthopedic changes.3,4
Most Class II functional appliances reposition the mandible in one step, so that the patient’s jaw is in the desired final position (or an overcorrected position) throughout treatment. An alternative to this method is incremental repositioning, which has been shown to be effective with the Twin Block.5 A key advantage of incremental advancement is the enhancement of patient comfort and muscular adaptation, especially at the start of therapy.
A recent systematic review by Cacciatore and colleagues stated, “Functional appliances produced a significant improvement of the maxillo-mandibular relationship at almost all time points, although the improvement of the mandibular projection was negligible or not significant. The quality of evidence was ‘very low’ for most of the outcomes at both primary time points.”6 The authors concluded that “functional appliances may be effective in correcting skeletal Class II malocclusion in the long-term, however the quality of the evidence was very low, and the clinical significance was limited.”
Conversely, in another systematic review of mandibular changes produced by Class II functional appliances, Cozza and colleagues found that two-thirds of the 22 analyzed studies reported a clinically significant supplementary elongation of the mandible as compared with the untreated group.7 Therefore, current evidence suggests that functional appliances are effective at correcting Class II malocclusions in growing patients, owing to a combination of dentoalveolar and skeletal changes.
In the Invisalign MA protocol, Precision Wings* are incorporated into the upper and lower aligners and engaged to the mandible in a progressively forward position, replicating the mechanisms of other removable functional appliances (Fig. 1). A prospective, multicenter clinical study was conducted to test the safety and effectiveness of this appliance in growing patients with Class II malocclusions. Interim results from the study are reported here.
Materials and Methods
This clinical study was approved by Quorum IRB on Jan. 20, 2015, as a nonsignificant-risk, prospective, nonrandomized, multicenter clinical study, with subsequent approval by the U.S. Food and Drug Administration under an Investigational Device Exemption (G170061) on April 7, 2017. All appliances used in the study were fabricated by Align Technology from proprietary SmartTrack† material. Informed assent and parental consent were obtained from all participating subjects.

The sample included patients age 11-19 in the fully erupted dentition (not including second premolars and second and third molars) with bilateral Class II malocclusions of at least 3mm, as measured from the first-permanent-molar relationship. Patients who had undergone orthodontic treatment within 12 months prior to the study or any previous treatment with sagittal orthodontic appliances were excluded, as were those with interproximal spaces of more than 3mm between two adjacent teeth, active caries or periodontal disease, TMD symptoms, partially erupted first permanent molars, or known allergies to latex or plastic, and those who were pregnant or became pregnant during the study. Any subject was free to withdraw from the study without a stated reason. In addition, the investigator had the discretion to exclude noncompliant subjects at any time.
A total of 60 subjects were enrolled; 55% were male and 45% were female, with a mean age of 12.75 years at the start of treatment (13.11 for males and 12.15 for females). The mean time from the initiation of treatment (T1) to the end of the MA phase (T2) was 12.6 months, and the mean time from T1 to the end of the post-MA phase (T3)—representing the mean total treatment time—was 25.6 months.
During the MA phase (T1 to T2), only the MA appliance was used, with no elastics or other auxiliaries. In the post-MA phase (T2 to T3), Class II elastics were used in 90% of the cases. There were 23 total withdrawals: eight prior to MA, 14 after MA, and one lost to observation.
Cephalometric radiographs were taken at each time point: initial (T1), end of MA (T2), and post-treatment (T3). The cephalograms were randomized before being traced by an external academic institution. The T1, T2, and T3 radiographs were imported into Dolphin Imaging‡ version 11.8, where landmark location and superimpositions were performed (Fig. 2). Student’s paired T-test was used to evaluate the cephalometric parameters; based on the Bonferroni correction for 24 parameters, statistical significance was set at a level of < .002.
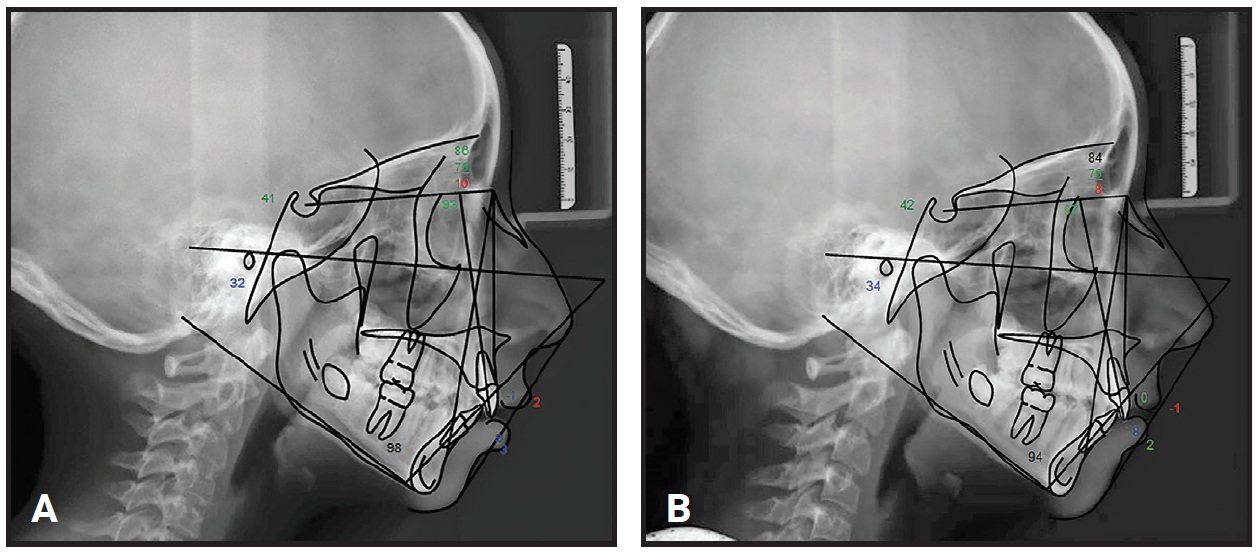
Fig. 2 Sample cephalometric tracings. A. Pretreatment (T1). B. End of MA phase (T2).
Case-report forms detailing treatment progress were collected from the study investigators at T1, T2, and T3; progress markers included millimetric measurements of overbite, overjet, and the molar relationship from the mesiobuccal cusp tip of the upper first molar to the buccal groove on the lower first molar. A quality-of-life survey focusing on the subject’s ease of use and discomfort was also administered at each time point.
Results
Mean cephalometric measurements for the 47 subjects completing T2 are shown in Table 1, and for 25 subjects completing T3 in Table 2.
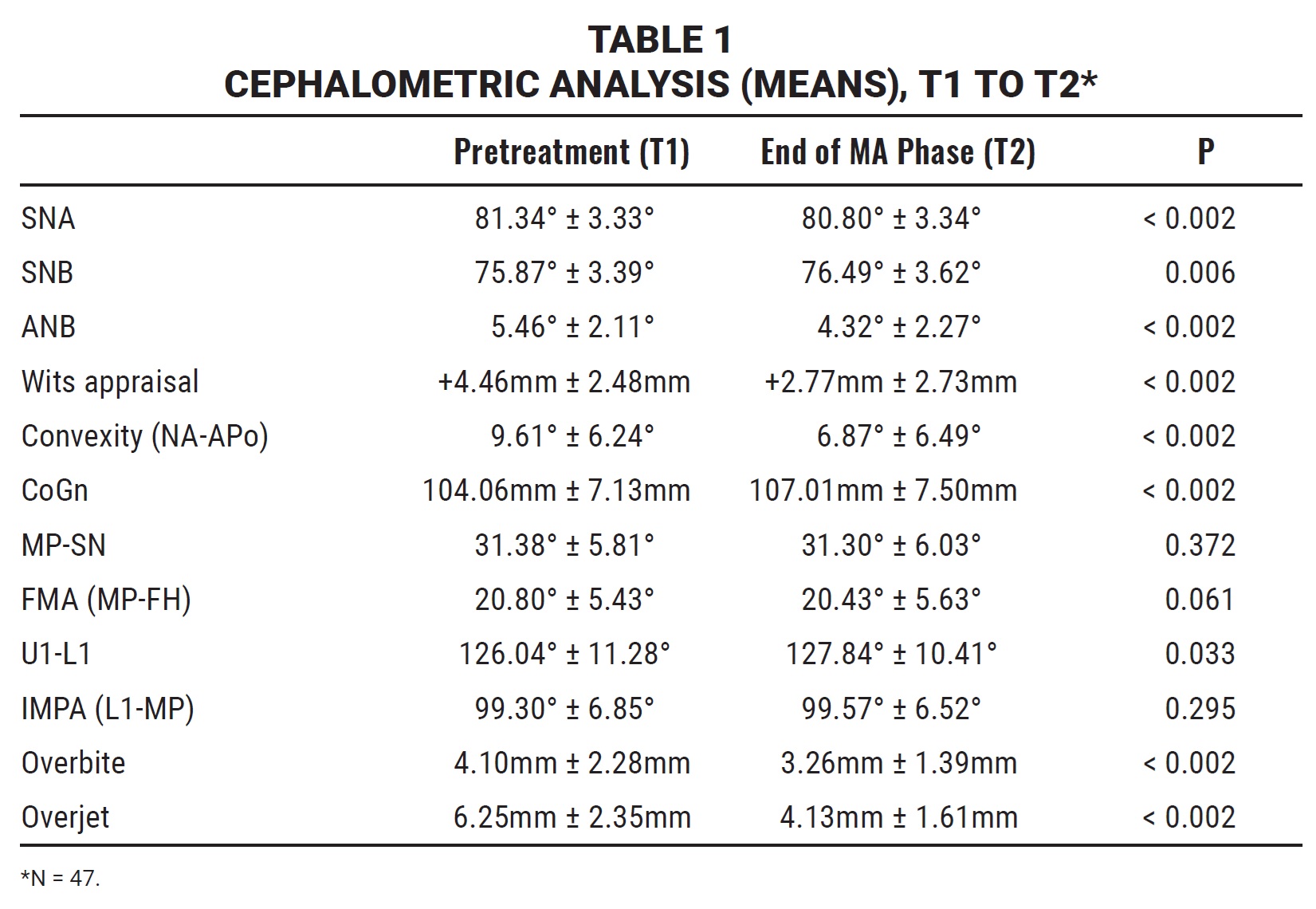
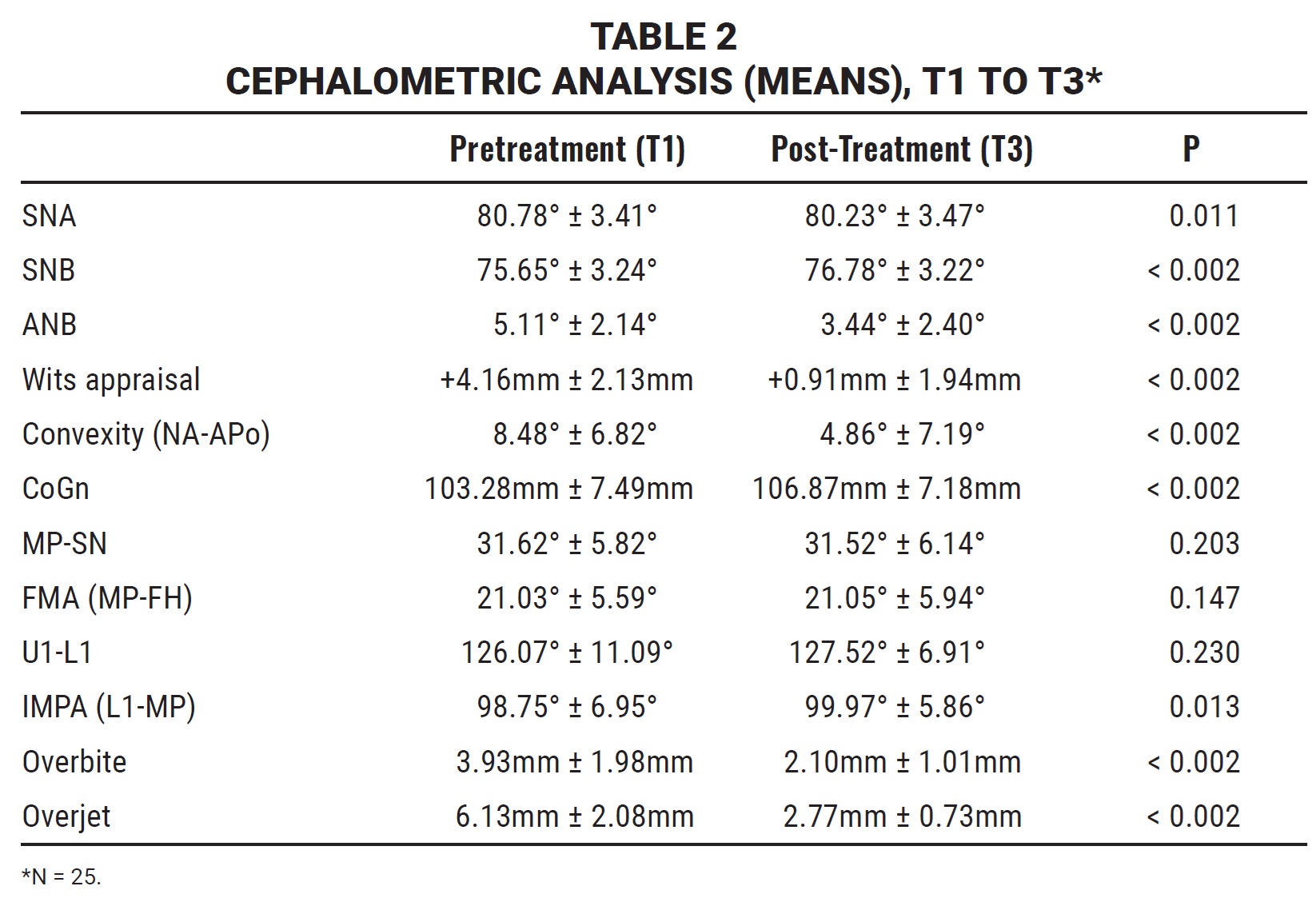
There were statistically significant changes from T1 to T3 in SNB (+1.13°), ANB (–1.67°), Wits appraisal (–3.25mm), convexity (–3.62°), mandibular length (CoGn = +3.59mm), overbite (–1.83mm), and overjet (–3.36mm). At both T2 and T3, there were no statistically significant changes in MP-SN, FMA, interincisal angle, or IMPA.
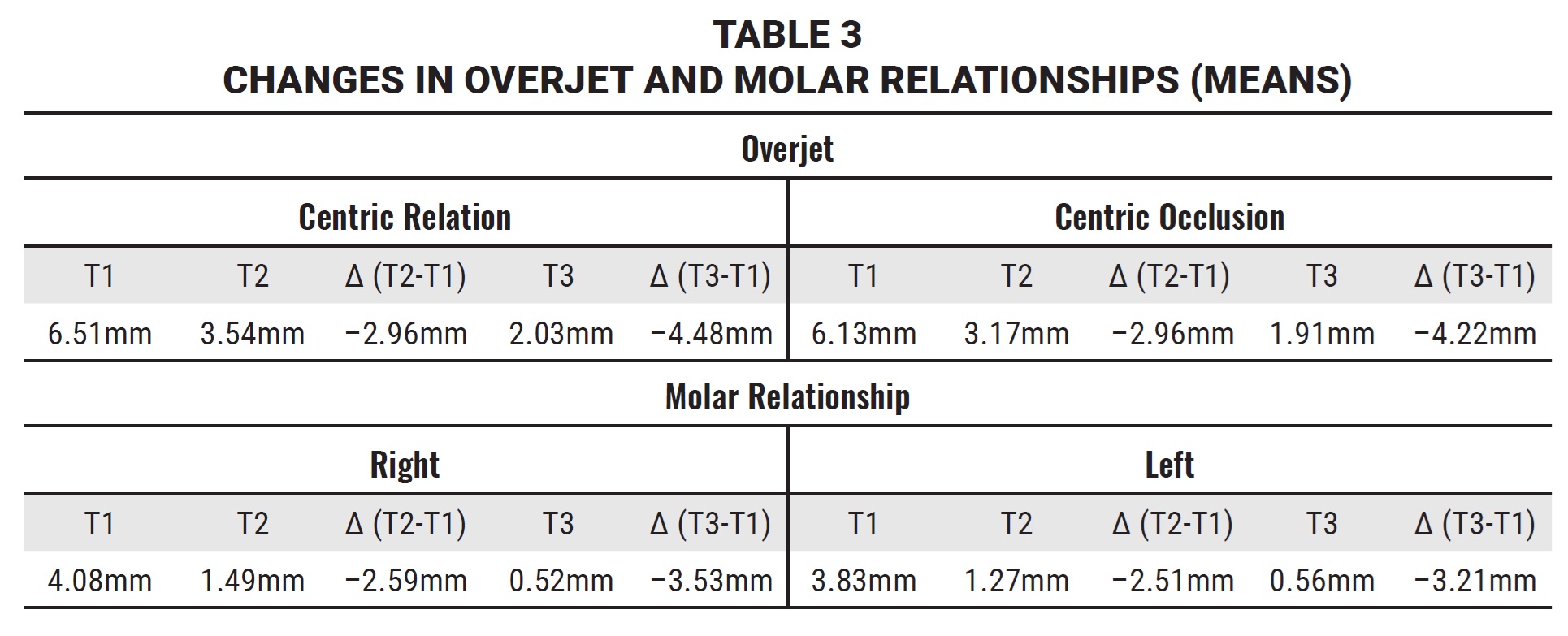
Linear dental measurements indicated a mean Class II molar discrepancy at the beginning of treatment (T1) of 4.08mm on the right and 3.83mm on the left, and a mean improvement in the molar relationship from T1 to T3 of 3.53mm on the right and 3.21mm on the left (Table 3).
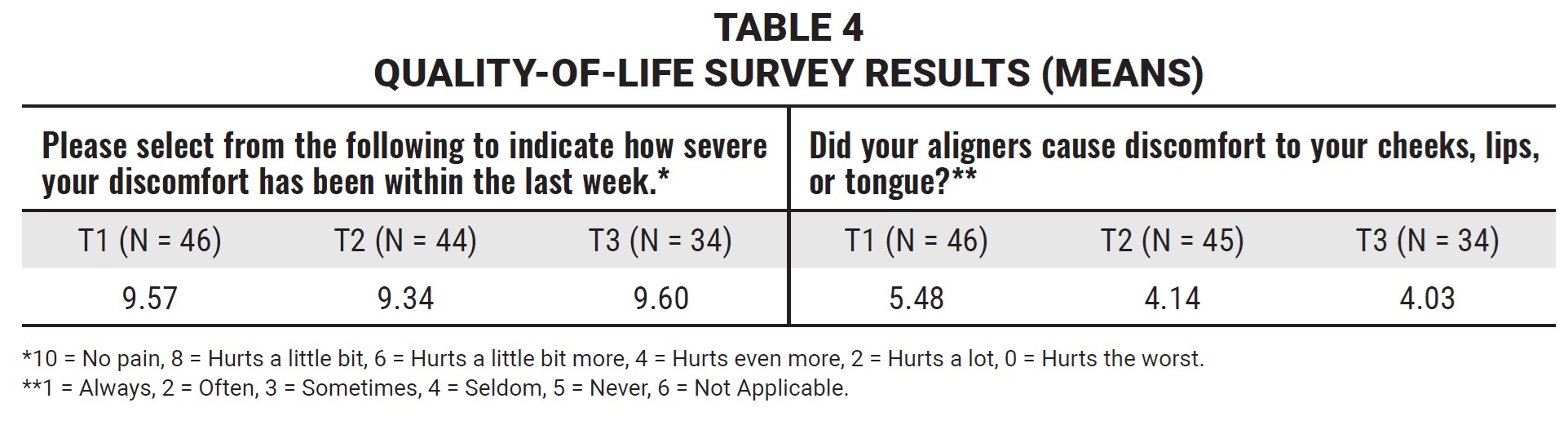
In the quality-of-life surveys, the average pain reported was minor (Table 4). At the end of T2, 89% of the subjects said they experienced discomfort between “sometimes” and “never.”
Discussion
The current consensus is that the primary mechanism of action of functional appliances in achieving Class II correction is dentoalveolar, with a smaller component of skeletal change.5,8 The preliminary results of our clinical study support this opinion. While subjects generally experienced a correction from a Class II to a Class I relationship, skeletal changes were consistent with the concept of a lesser component of “growth modification” than of dentoalveolar changes within the overall occlusal correction.
It is important to note that no Class II elastics or other auxiliaries were used during the MA phase (T1 to T2); therefore, it is reasonable to attribute the cephalometric and linear changes noted at T2 to the effects of the MA appliance, along with normal growth. On the other hand, Class II elastics were used in 90% of the subjects after the MA phase, contributing to significant changes observed at T3: a reduction in overbite and overjet and an improvement in the molar relationship. There was no significant change in the mandibular plane angle, indicating good vertical control. Similarly, there was no significant change in IMPA, indicating excellent control of lower-incisor angulation. These findings differ from studies of other functional appliances, which tend to show significant proclination of the lower incisors.9,10
Although Invisalign treatment with MA seems to produce similar treatment results, it offers several advantages over traditional Class II functional appliances. Mandibular incisor angulation and molar extrusion are well controlled, and patients rate their degree of discomfort as low. It does have some limitations, including the removable nature of the aligners, which require dedicated compliance. There is also an adaptation period in which the patient learns how to posture forward to properly engage the Precision Wings.
FOOTNOTES
- *Registered trademark of Align Technology, Inc., San Jose, CA; www.aligntech.com.
- **Trademark of Protec Dental Laboratories Ltd., Vancouver, BC, Canada; www.protecdental.com.
- ***AOA Orthodontic Appliances, Sturtevant, WI; www.aoaaccess.com.
- †Registered trademark of Dentaurum, Inc., Newtown, PA; www.dentaurum.com.
- ‡Dolphin Imaging and Management Solutions, Chatsworth, CA; www.dolphinimaging.com.
REFERENCES
- 1. Bishara, S.: Class II malocclusions: Diagnostic and clinical considerations with and without treatment, Sem. Orthod. 12:11-24, 2006.
- 2. McNamara, J.A. Jr.: Components of Class II malocclusion in children 8-10 years of age, Angle Orthod. 51:177-202, 1981.
- 3. Siara-Olds, N.J.; Pangrazio-Kulbersh, V.; Berger, J.; and Bayirli, B.: Long-term dentoskeletal changes with the Bionator, Herbst, Twin Block, and MARA functional appliances, Angle Orthod. 80:18-29, 2010.
- 4. Pangrazio-Kulbersh, V.; Berger, J.L.; Chermak, D.S.; Kaczynski, R.; Simon, E.S.; and Haerian, A.: Treatment effects of the mandibular anterior repositioning appliance on patients with Class II malocclusion, Am. J. Orthod. 123:286-295, 2003.
- 5. O’Brien, K.; Wright, J.; Conboy, F.; Sanjie, Y.W.; Mandall, N.; Chadwick, S.; Connolly, I.; Cook, P.; Birnie, D.; Hammond, M.; Harradine, N.; Lewis, D.; McDade, C.; Mitchell, L.; Murray, A.; O’Neill, J.; Read, M.; Robinson, S.; Roberts-Harry, D.; Sandler, J.; and Shaw, I.: Effectiveness of early orthodontic treatment with the Twin-block appliance: A multicenter, randomized, controlled trial, Part 1: Dental and skeletal effects, Am. J. Orthod. 124:234-343, 2003.
- 6. Cacciatore, G.; Ugolini, A.; Sforza, C.; Gbinigie, O.; and Plüddemann, A.: Long-term effects of functional appliances in treated versus untreated patients with Class II malocclusion: A systematic review and meta-analysis, PLoS One 14:e0221624, 2019.
- 7. Cozza, P.; Baccetti, T.; Franchi, L.; de Toffol, L.; and McNamara, J.A. Jr.: Mandibular changes produced by functional appliances in Class II malocclusion: A systematic review, Am. J. Orthod. 129:599.e1-e12, 2006.
- 8. Al-Jewair, T.S.: Meta-analysis on the mandibular dimension effects of the MARA appliance in patients with Class II malocclusions, Angle Orthod. 85:706-714, 2015.
- 9. Lund, D.I. and Sandler, P.J.: The effects of Twin Blocks: A prospective controlled study, Am. J. Orthod. 113:104-110, 1998.
- 10. Brunharo, I.H.V.P.; Quintão, C.A.; de Oliveira Almeida, M.A.; Motta, A.; and Barreto, S.Y.N.: Dentoskeletal changes in Class II malocclusion patients after treatment with the Twin Block functional appliance, Dent. Press J. Orthod. 16:40.e1-e8, 2011.
-
 DR. GLASER
DR. GLASER -
 DR. TAI
DR. TAI -
 DR. BLEVINS
DR. BLEVINS -
 DR. DAHER
DR. DAHER
Dr. Glaser is in the private practice of orthodontics, 1983 Crompond Road, Cortlandt Manor, NY 10567; e-mail: drglaser@glaserortho.com. Dr. Tai is a Clinical Assistant Professor, Faculty of Dentistry, University of British Columbia, Vancouver, British Columbia; an Assistant Professor of Orthodontics, University of the Pacific, San Francisco; and in the private practice of orthodontics in Vancouver. Dr. Blevins is an adjunct Clinical Professor of Orthodontics, University of Minnesota, Minneapolis, and in the private practice of orthodontics in Eagan, Minnesota. Dr. Daher is an Associate Professor, Graduate Orthodontics, University of Montreal, Montreal, and in the private practice of orthodontics in Hamilton, Ontario. The authors are paid consultants for Align Technology, Inc.