Evolution of the Leaf Expander: A Maxillary Self Expander
Palatal transverse deficiency of the maxilla is a common component of both dental and skeletal malocclusions, usually accompanied by posterior crossbite, upper crowding, or both. Although crossbite occurs in 6-30% of the general population,1,2 the rate of spontaneous self-correction is only 0-9%, even after oral habits and similar etiological factors have been resolved.3,4 The chances of successfully expanding the maxillary bony base declines with patient age.5 Therefore, the clinician needs an accurate early diagnosis to classify the patient’s maxillary deficiency and apply the most appropriate clinical protocols.6
Many devices have been developed for varying degrees of orthodontic, orthopedic, or mixed maxillary expansion.7,8 All of these techniques operate by generating buccal forces on the anchorage teeth.9,10 The maxillary morphological reactions are determined by three main factors: age (skeletal maturity) of the patient, amount of force applied (orthodontic or orthopedic), and duration of force application (continuous or intermittent).
In 2017, based on our experience with slow maxillary expansion11-13 using the Leaf Expander,14,15* we introduced the completely preactivated Self Expander.* With no need for further activation either in the office or at home, the Self Expander does not rely on patient cooperation. Because the device employs light and continuous forces, it causes no pain even in the early stages of expansion.
Similar articles from the archive:
Appliance Design
The design of the Self Expander is similar to that of a Leaf Expander,16 except that it is equipped with three preactivated, nickel titanium double springs instead of a leaf spring and a reactivation screw (Fig. 1). These leaf springs, which are compressed during fabrication in the laboratory, recover their shape during deactivation, generating a constant 450g of force for as much as 9mm of calibrated expansion.
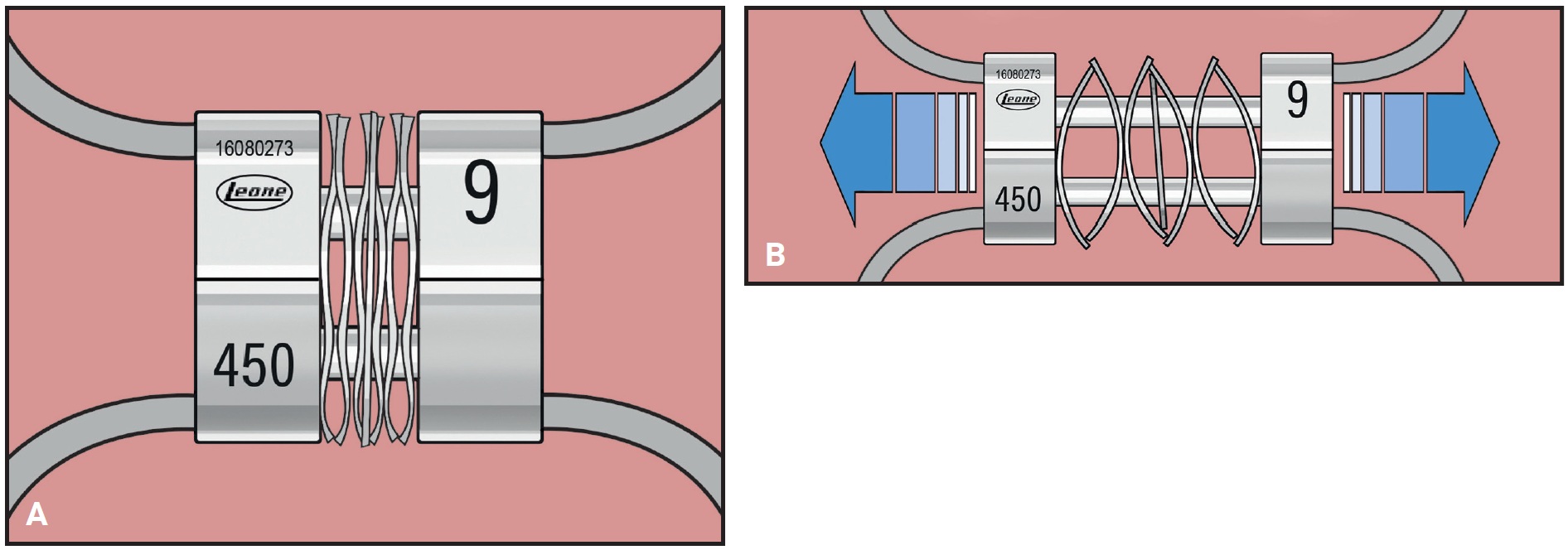
Fig. 1 A. Self Expander* with three double-leaf springs compressed by laboratory before delivery. B. Springs decompress during treatment and generate constant 450g of force.
Like the Leaf Expander, the Self Expander is typically anchored to the deciduous teeth,17,18 with the upper first permanent molars left free to expand spontaneously (Fig. 2). The body of the 11mm × 12mm × 4mm screw can be adapted to fit a narrow palate or an arch with transverse deficiency. The arms connecting the screw and the lateral components must be kept about 2.5mm clear of the palatal mucosa to avoid ulceration. The screw is blocked with metal ligatures that are removed immediately after cementation to start the self-expansion.
The patient should be monitored monthly for expansion and oral hygiene. Active expansion takes about six months, after which the appliance should be maintained passively in place for three months of retention.
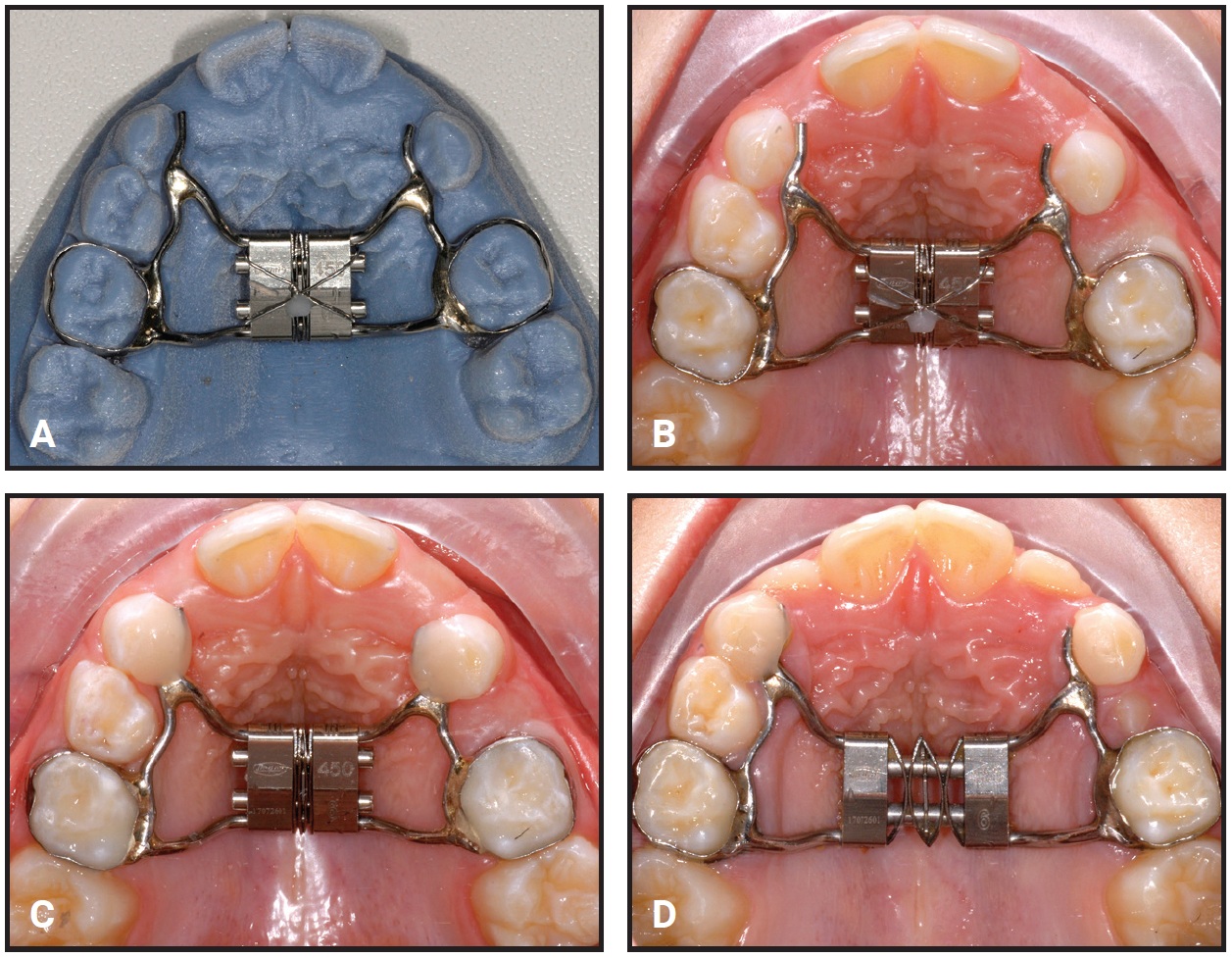
Fig. 2 A. Self Expander on prototype model created from stereolithographic (STL) file of intraoral scan. B. Expander in mouth, with metal ligature still blocking compressed expansion leaves. C. Ligature wire removed immediately after banding. D. Appliance during active expansion.
Case 1
A 6-year-old male in the mixed dentition presented with a lack of space for his lateral incisors and a crossbite associated with a lateral mandibular shift to the right and a transverse discrepancy (Fig. 3, Table 1). The upper right central incisor had been extracted following an intrusive trauma at age 4; the space had been maintained with a transpalatal arch and composite pontic.
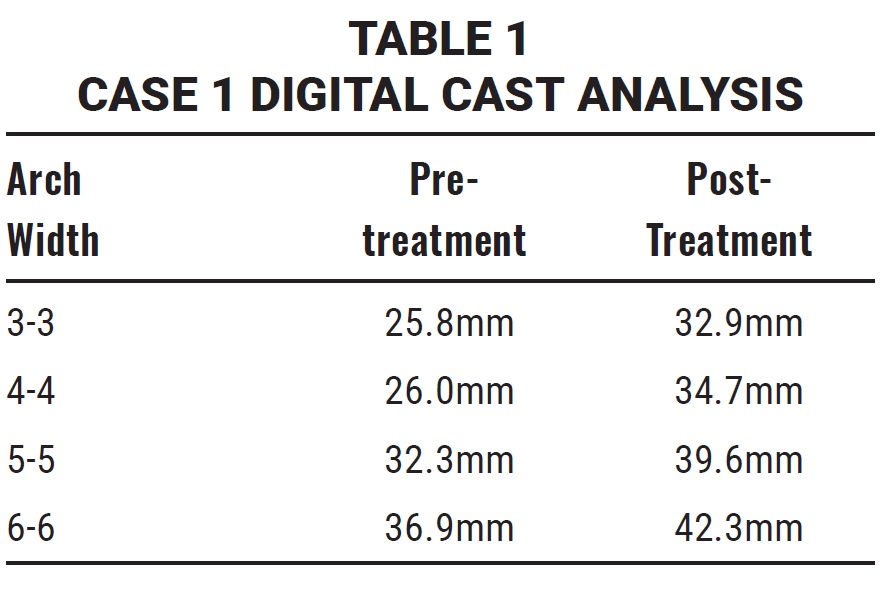
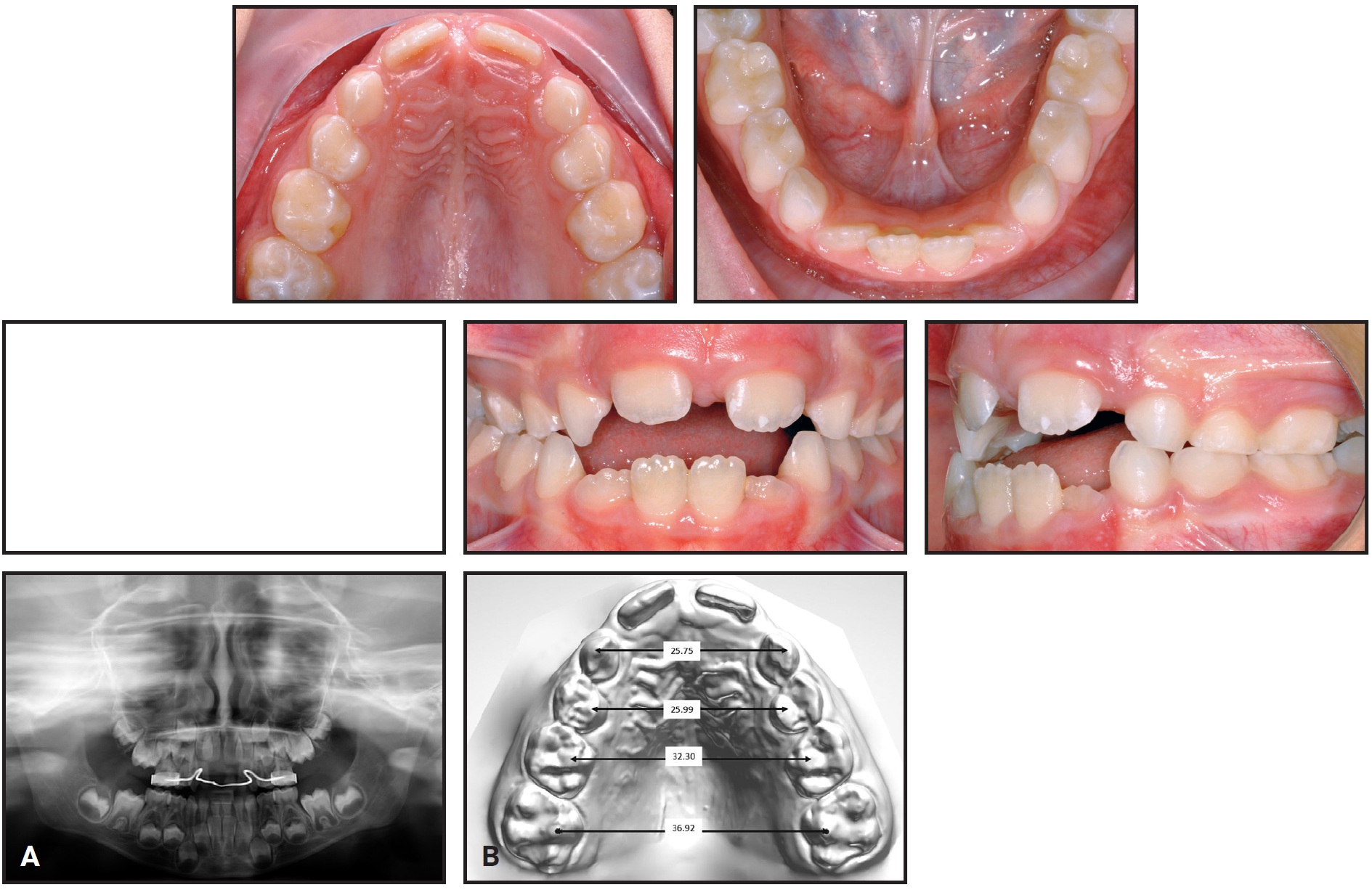
Fig. 3 Case 1. A. 6-year-old male patient with maxillary transverse deficiency, crossbite, mandibular deviation, and missing upper right central incisor (extracted at age 4) before treatment. (Panoramic radiograph taken seven months earlier.) B. Arch-width measurements on STL digital cast obtained from laboratory scan of polyvinyl siloxane impressions.
A Self Expander was placed with bands on the second deciduous molars and extensions to the canines and first deciduous molars (Fig. 4).
After six months of expansion, the crossbite was resolved, the midlines were coincident, the archform had improved, and the first permanent molars exhibited spontaneous expansion. The Self Expander was left in place for five months, until eruption of the lateral incisors. Because the screw was not blocked in any way, its flexibility could facilitate active functional adaptation of the occlusion with the lower arch (Fig. 5).
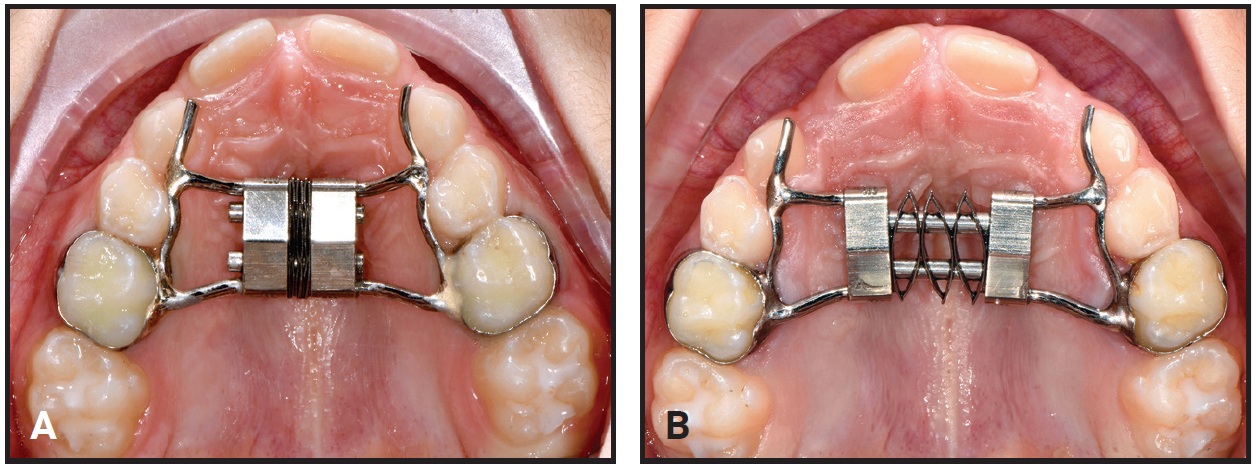
Fig. 4 Case 1. A. Self Expander in place at beginning of treatment. B. After six months of expansion.
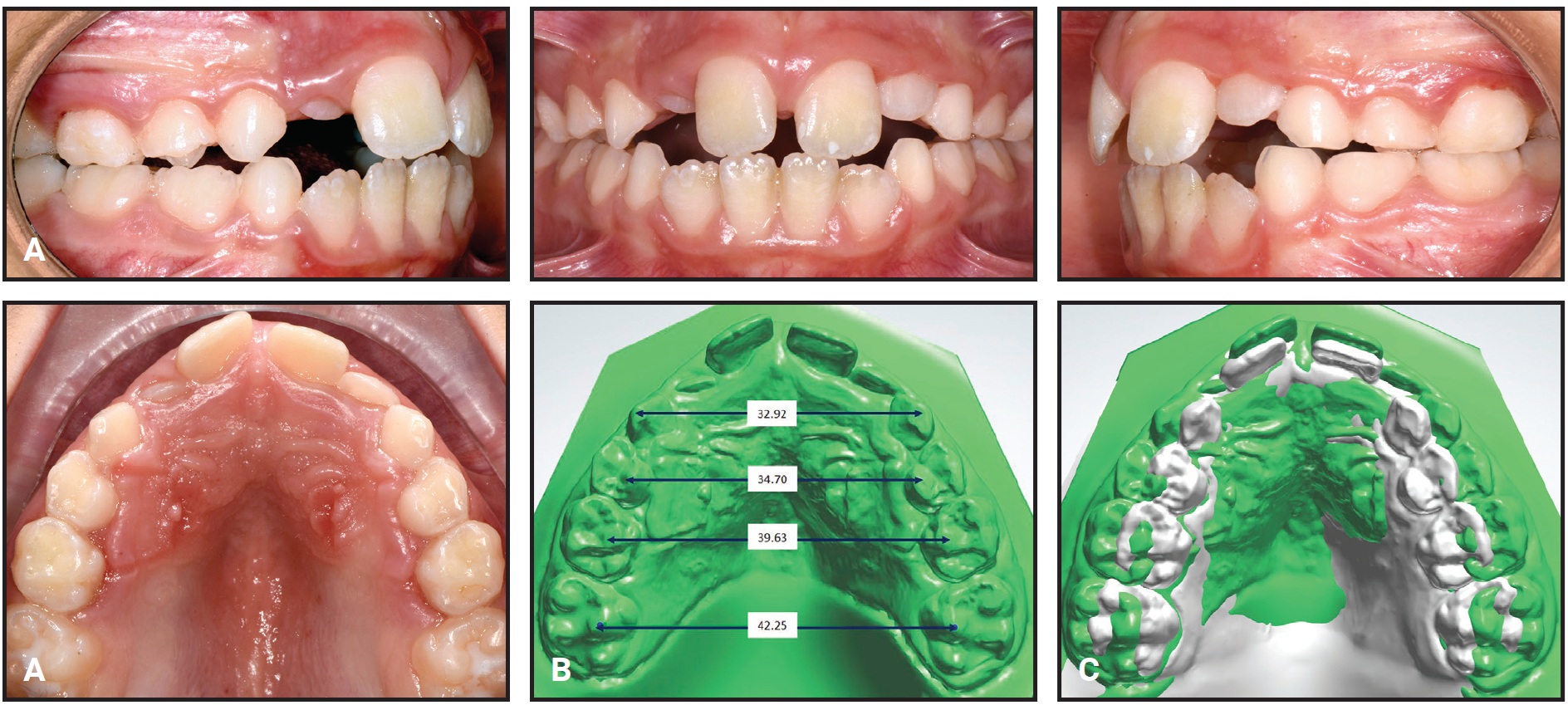
Fig. 5 Case 1. A. Self Expander removed after five months of passive retention. B. Arch-width measurements on STL digital cast. C. Superimposition of pre- and post-treatment scans on palatal rugae.
The results remained stable nine months after treatment (Fig. 6).

Fig. 6 Case 1. Patient nine months after treatment.
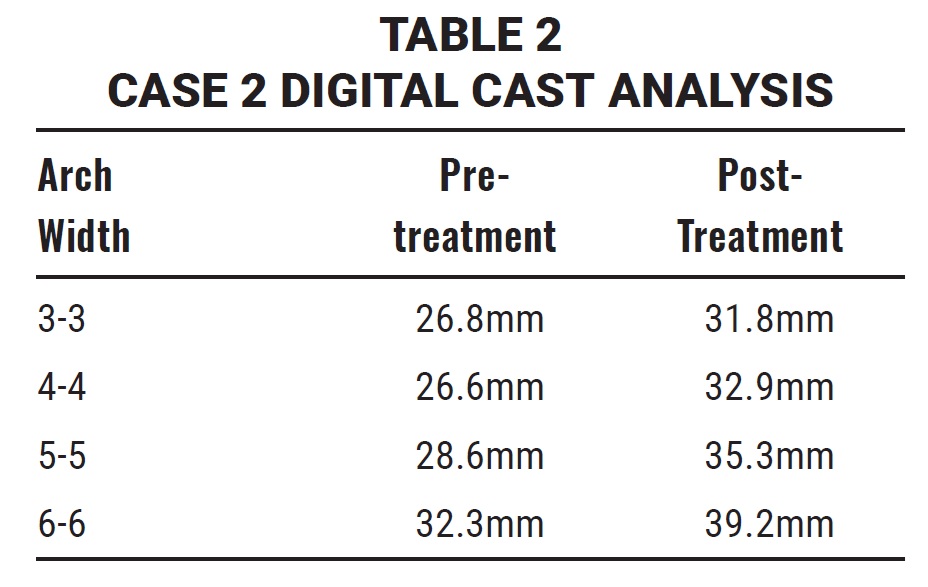

Fig. 7 Case 2. A. 6-year-old female patient with maxillary transverse deficiency and bilateral crossbite before treatment (continued in next image).
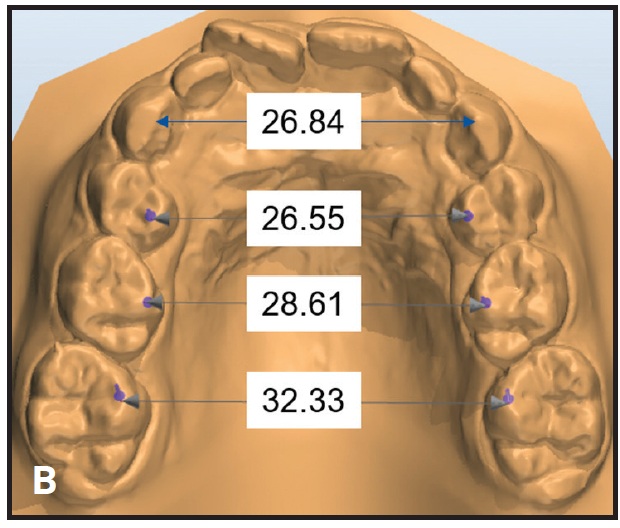
Fig. 7 (cont.) Case 2 B. Arch-width measurements on STL digital cast obtained from laboratory scan of polyvinyl siloxane impressions.
A Self Expander was bonded rather than banded to the upper first deciduous molars, with extensions to the canines (Fig. 8).
The patient was checked six times during seven months of active expansion, and the Self Expander was then left in place for three months of retention. The crossbite was corrected, the maxilla was expanded enough to allow eruption of the permanent lateral incisors, and the first permanent molars showed spontaneous expansion and derotation, guided by the occlusion (Fig. 9).
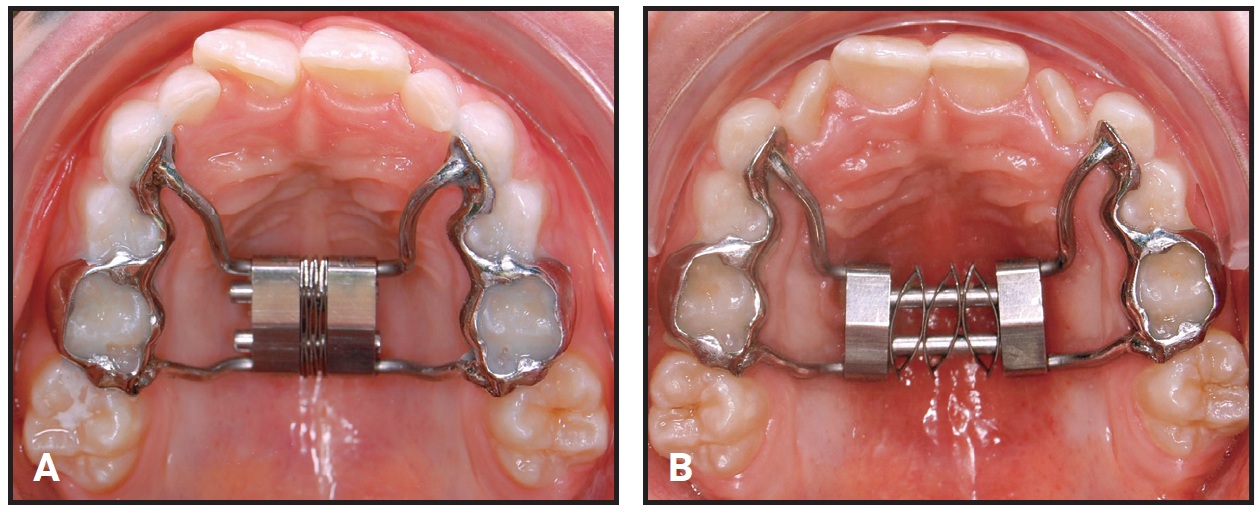
Fig. 8 Case 2 A. Self Expander in place at beginning of treatment. B. After seven months of expansion.
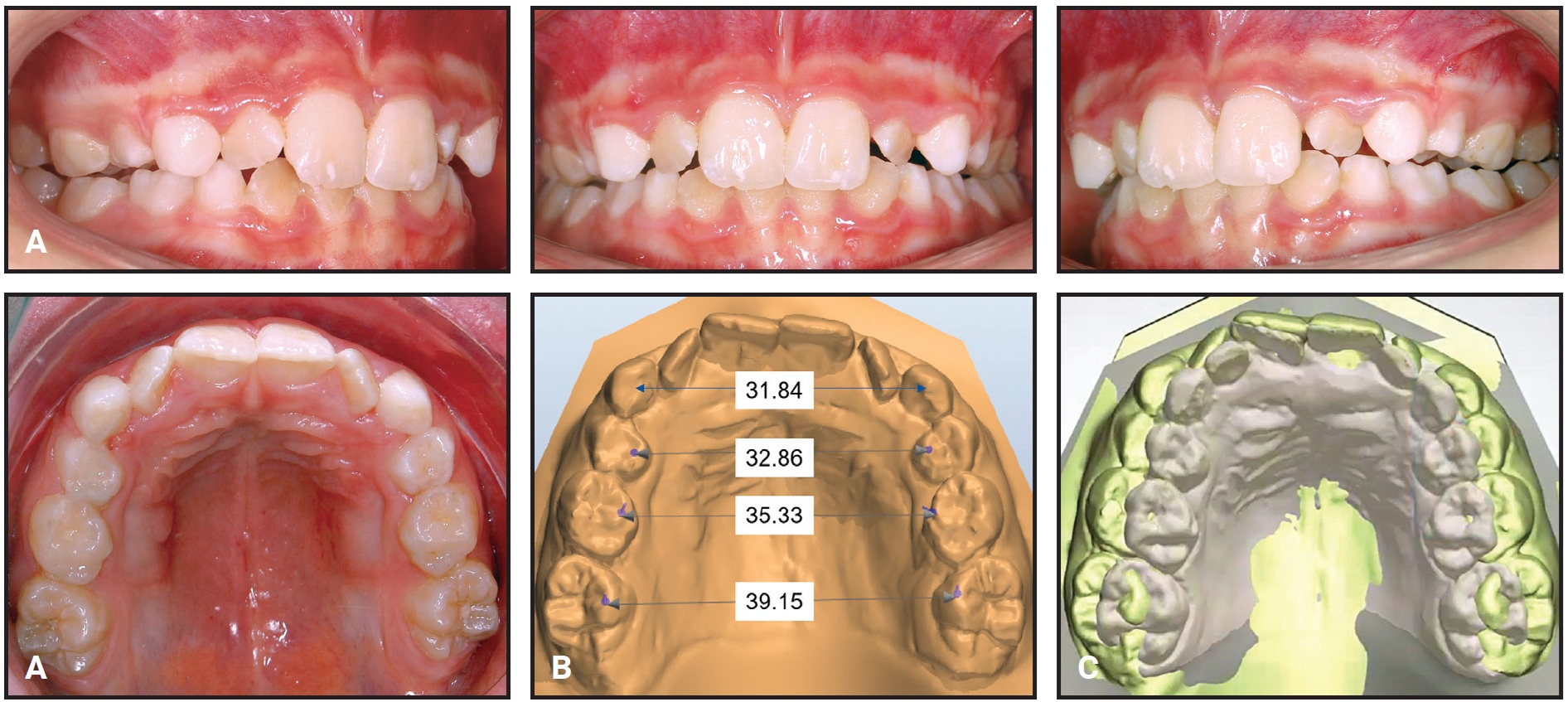
Fig. 9 Case 2 A. Self Expander removed after three months of passive retention. B. Arch-width measurements on STL digital cast. C. Superimposition of pre- and post-treatment scans on palatal rugae.
Discussion
These clinical results demonstrate the effectiveness, efficiency, and ease of use of the Self Expander in correcting transverse maxillary deficiency in the mixed dentition. Controlled tooth movement was achieved without undesirable side effects on the permanent teeth.
With no need for reactivation or patient compliance, the Self Expander is simple and safe to use. The semi-rigid yet flexible leaf system delivers predetermined light, constant forces for painless expansion and predictable results.
FOOTNOTES
- *Registered trademark of Leone S.p.A., Sesto Fiorentino, Firenze, Italy; www.leone.it.
REFERENCES
- 1. Ferro, R.; Besostri, A.; Olivieri, A.; Quinzi, V.; and Scibetta, D.: Prevalence of cross-bite in a sample of Italian preschoolers, Eur. J. Paediat. Dent. 17:307-309, 2016.
- 2. Tausche, E.; Luck, O.; and Harzer, W.: Prevalence of malocclusions in the early mixed dentition and orthodontic treatment need, Eur. J. Orthod. 26:237-244, 2004.
- 3. Kecik, D.; Kocadereli, I.; and Saatci, I.: Evaluation of the treatment changes of functional posterior crossbite in the mixed dentition, Am. J. Orthod. 131:202-215, 2007.
- 4. Lippold, C.; Stamm, T.; Meyer, U.; Végh, A.; Moiseenko, T.; and Danesh, G.: Early treatment of posterior crossbite: A randomised clinical trial, Trials 14:20, 2013.
- 5. Geran, R.G.; McNamara, J.A. Jr.; Baccetti, T.; Franchi, L.; and Shapiro, L.M.: A prospective long-term study on the effects of rapid maxillary expansion in the early mixed dentition, Am. J. Orthod. 129:631-640, 2006.
- 6. Grassia, V.; D’Apuzzo, F.; Jamilian, A.; Femiano, F.; Favero, L.; and Perillo, L.: Comparison between rapid and mixed maxillary expansion through an assessment of arch changes on dental casts, Prog. Orthod. 16:20, 2015.
- 7. Cossellu, G.; Farronato, G.; Nicotera, O.; and Biagi, R.: Transverse maxillary deficit and its influence on the cervical vertebrae maturation index, Eur. J. Paediat. Dent. 17:147-150, 2016.
- 8. Leonardi, R.; Sicurezza, E.; Cutrera, A.; and Barbato, E.: Early post-treatment changes of circumaxillary sutures in young patients treated with rapid maxillary expansion, Angle Orthod. 81:36-41, 2011.
- 9. Martina, R.; Cioffi, I.; Farella, M.; Leone, P.; Manzo, P.; Matarese, G.; Portelli, M.; Nucera, R.; and Cordasco, G.: Transverse changes determined by rapid and slow maxillary expansion—A low-dose CT-based randomized controlled trial, Orthod. Craniofac. Res. 15:159-168, 2012.
- 10. Perillo, L.; De Rosa, A.; Iaselli, F.; D’Apuzzo, F.; Grassia, V.; and Cappabianca, S.: Comparison between rapid and mixed maxillary expansion through an assessment of dento-skeletal effects on posteroanterior cephalometry, Prog. Orthod. 15:46, 2014.
- 11. Mobrici, P.; Lanteri, C.; Beretta, M.; and Caprioglio, A.: Slow maxillary expansion in adult patients: A pilot study, Mondo Ortod. 37:S7-S13, 2012.
- 12. Mobrici, P.; Lanteri, C.; Beretta, M.; and Caprioglio, A.: Dental and skeletal modifications in adult patients treated with Slow Maxillary Expander, Mondo Ortod. 37:S41-S46, 2012.
- 13. Gianolio, A.; Lanteri, V.; and Chierchi, C.: Rapid and slow maxillary expansion: A postero-anterior cephalometric study, Eur. J. Paediat. Dent. 15:415-418, 2014.
- 14. Lanteri, C.; Beretta, M.; Lanteri, V.; Gianolio, A.; Cherchi, C.; and Franchi, L.: The leaf expander for no compliance treatment in the mixed dentition, J. Clin. Orthod. 50:552-560, 2016.
- 15. Lanteri, V.; Gianolio, A.; Gualandi, G.; and Beretta, M.: Maxillary tridimensional changes after slow expansion with leaf expander in a sample of growing patients: A pilot study, Eur. J. Paediat. Dent. 19:29-34, 2018.
- 16. Manzella, K.; Franchi, L.; and Al-Jewair, T.: Correction of maxillary transverse deficiency in growing patients with permanent dentitions, J. Clin. Orthod. 52:148-156, 2018.
- 17. Mutinelli, S.; Manfredi, M.; Guiducci, A.; Denotti, G.; and Cozzani, M.: Anchorage onto deciduous teeth: Effectiveness of early rapid maxillary expansion in increasing dental arch dimension and improving anterior crowding, Prog. Orthod. 16:22, 2015.
- 18. Rosa, M.; Lucchi, P.; Manti, G.; and Caprioglio, A.: Rapid palatal expansion in the absence of posterior cross-bite to intercept maxillary incisor crowding in the mixed dentition: A CBCT evaluation of spontaneous changes of untouched permanent molars, Eur. J. Paediat. Dent. 17:286-294, 2016.
-
 DR. BERETTA
DR. BERETTA -
 DR. LANTERI
DR. LANTERI -
DR. LANTERI
-
DR. CHERCHI
-
DR. FRANCHI
-
DR. GIANOLIO
Dr. Beretta is in the private practice of orthodontics at Viale Aguggiari, 22, 21100 Varese, Italy. Drs. Claudio Lanteri and Valentina Lanteri are in the private practice of orthodontics in Casale Monferrato, Italy. Dr. Valentina Lanteri is also a doctoral student and research fellow, Department of Biomedical, Surgical and Dental Sciences, University of Milan, Italy. Drs. Gianolio and Cherchi are in the private practice of orthodontics in Bra, Italy. Dr. Franchi is an Associate Professor, Department of Surgery and Translational Medicine, Orthodontics, University of Florence, Italy. E-mail Dr. Beretta at info@matteoberetta.pro.
