The Leaf Expander for Non-Compliance Treatment in the Mixed Dentition
Transverse discrepancy due to a reduced palatal dimension, usually accompanied by upper-arch crowding and crossbite, is one of the most common problems seen in orthodontics.1-2 Various devices for orthopedic maxillary expansion have been described, with the common objective of minimizing dental effects and maximizing skeletal effects.3 In the early mixed dentition, a transverse discrepancy can be effectively solved by anchoring a fixed expansion device such as a rapid palatal expander or Quad Helix* to deciduous teeth,4 thus avoiding undesirable effects on the permanent teeth.1,5,6
Even slow maxillary expansion has been shown to have orthopedic effects in growing patients.7 In 2013, based on our experience with slow expansion,8 we introduced a new spring-based expander with a leaf-shaped active element. This Leaf Expander** eliminates the need for home activation and simplifies clinical management. The present article describes its use for palatal expansion in the mixed dentition.
Appliance Design
The design of the Leaf Expander is similar to that of a conventional rapid palatal expander. Instead of a midline jackscrew, however, it has a double nickel titanium leaf spring that recovers its original shape during deactivation, resulting in a calibrated expansion of the upper arch (Fig. 1). The Leaf Expander is typically anchored by deciduous teeth, with the upper first permanent molars left to expand spontaneously.
Similar articles from the archive:
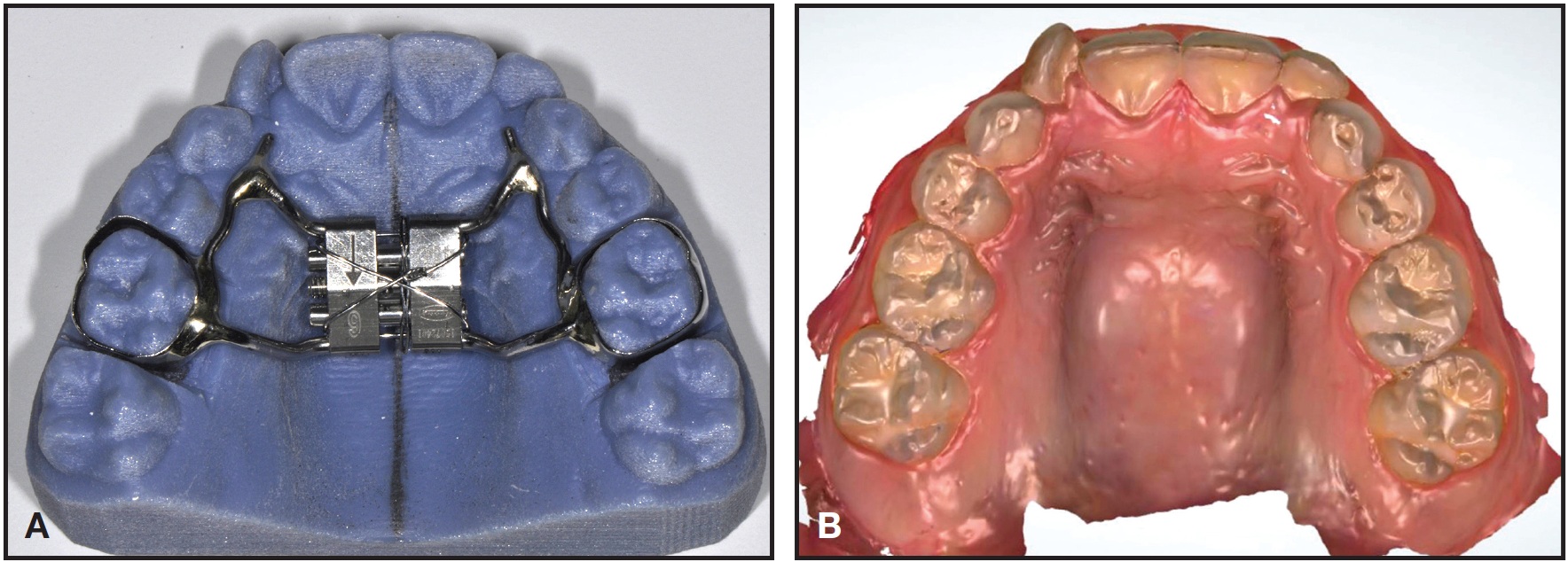
Fig. 1 Leaf Expander** on prototype model (A) produced by stereolithography (STL) from intraoral scan (B).
The 11mm × 12mm × 4mm screw is readily adaptable to a narrow palate or an arch with transverse deficiency. It delivers a maximum expansion of 6mm by activating (compressing) the spring, which generates a light (450g) and constant force.
The leaves are preactivated in the laboratory to deliver 3mm of expansion. The screw is blocked with metal ligatures or a special clip, which is removed after cementation (Fig. 2).
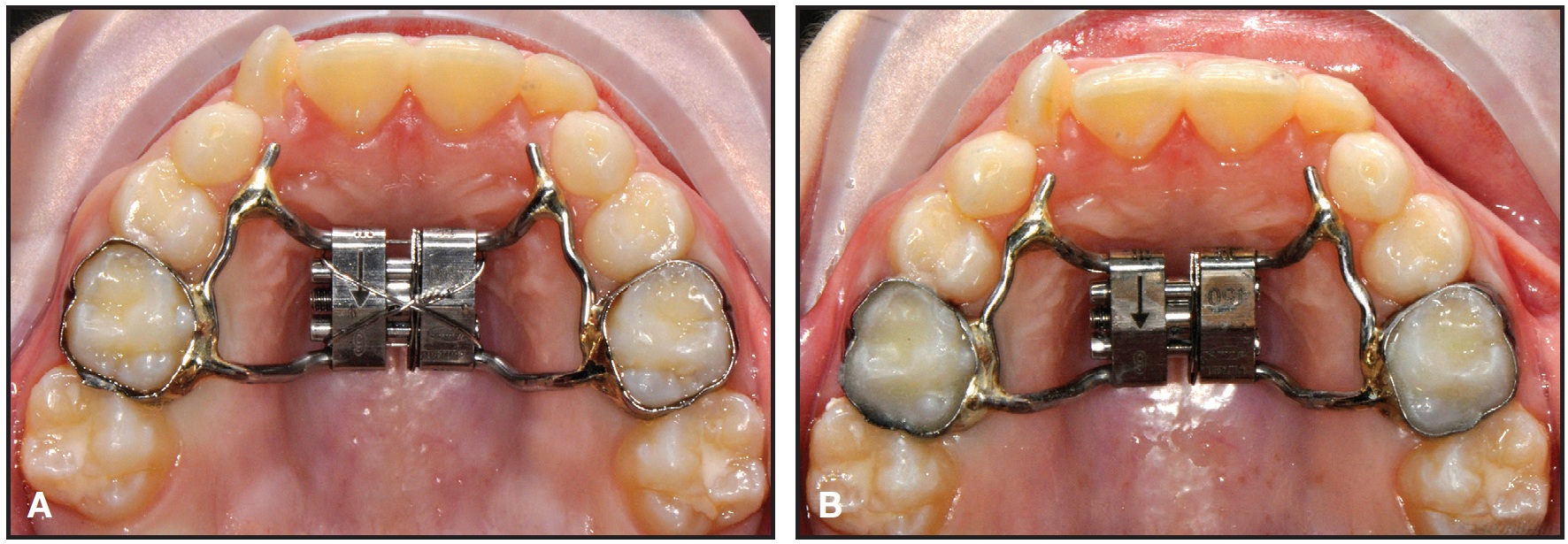
Fig. 2 A. Preactivated expander fitted in mouth, with metal ligatures blocking expansion screw. B. Ligatures removed after bonding.
Reactivation is performed in the office by 10 quarter-turns of the screw per month until expansion has been completed (Fig. 3). One-quarter turn corresponds to .1mm of activation; therefore, 10 activations of the screw generate 1mm of activation and, consequently, 1mm of spring compression. The maximum number of activations is 30 (6mm of expansion). Active expansion generally takes about six months, after which the Leaf Expander should be maintained passively in place for three months of retention.
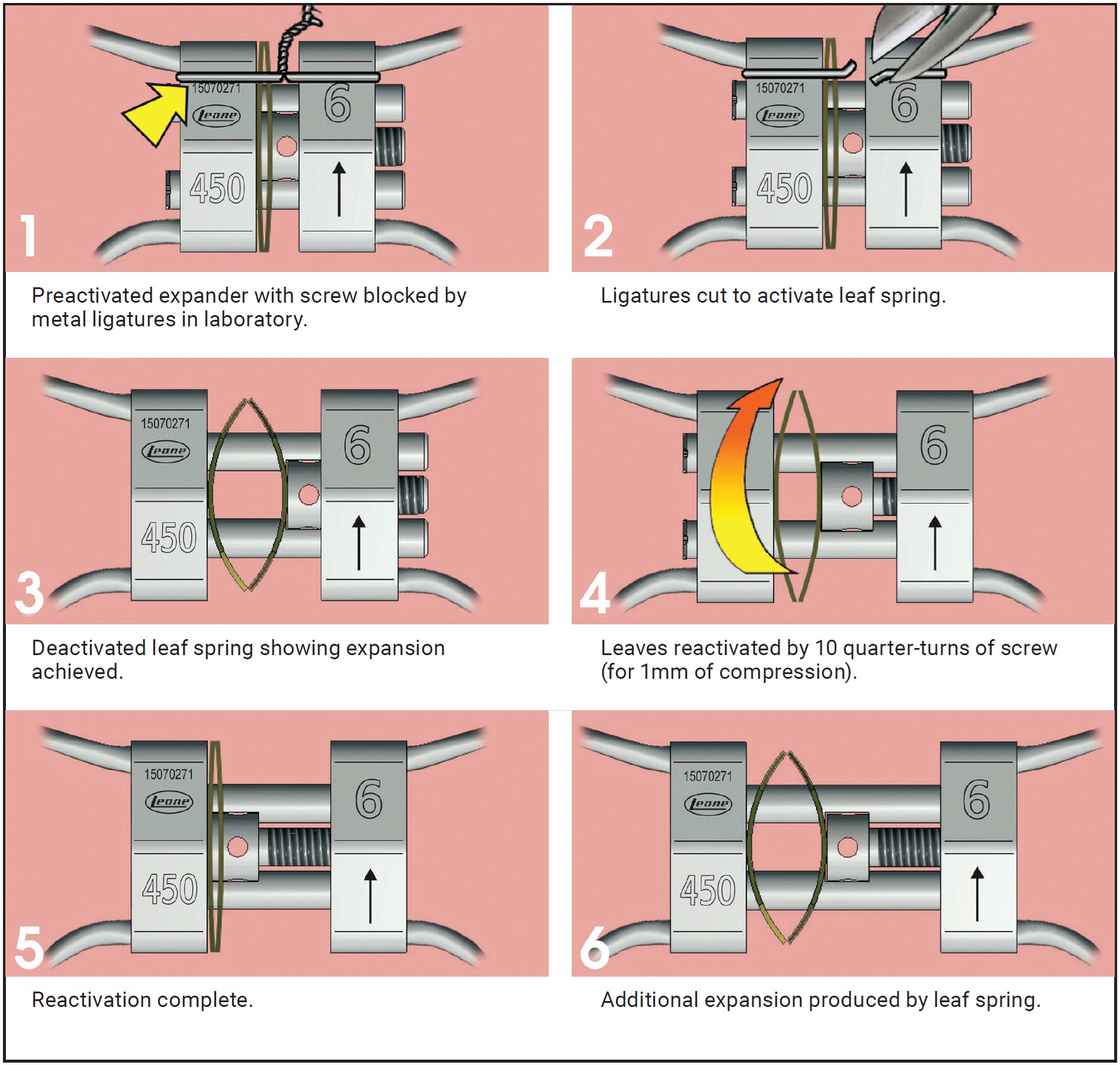
Fig. 3 Typical activation protocol for Leaf Expander.
Case 1
An 8-year-old female in the mixed dentition presented with a crossbite associated with a left lateral deviation of the mandible and a transverse deficiency (Fig. 4).
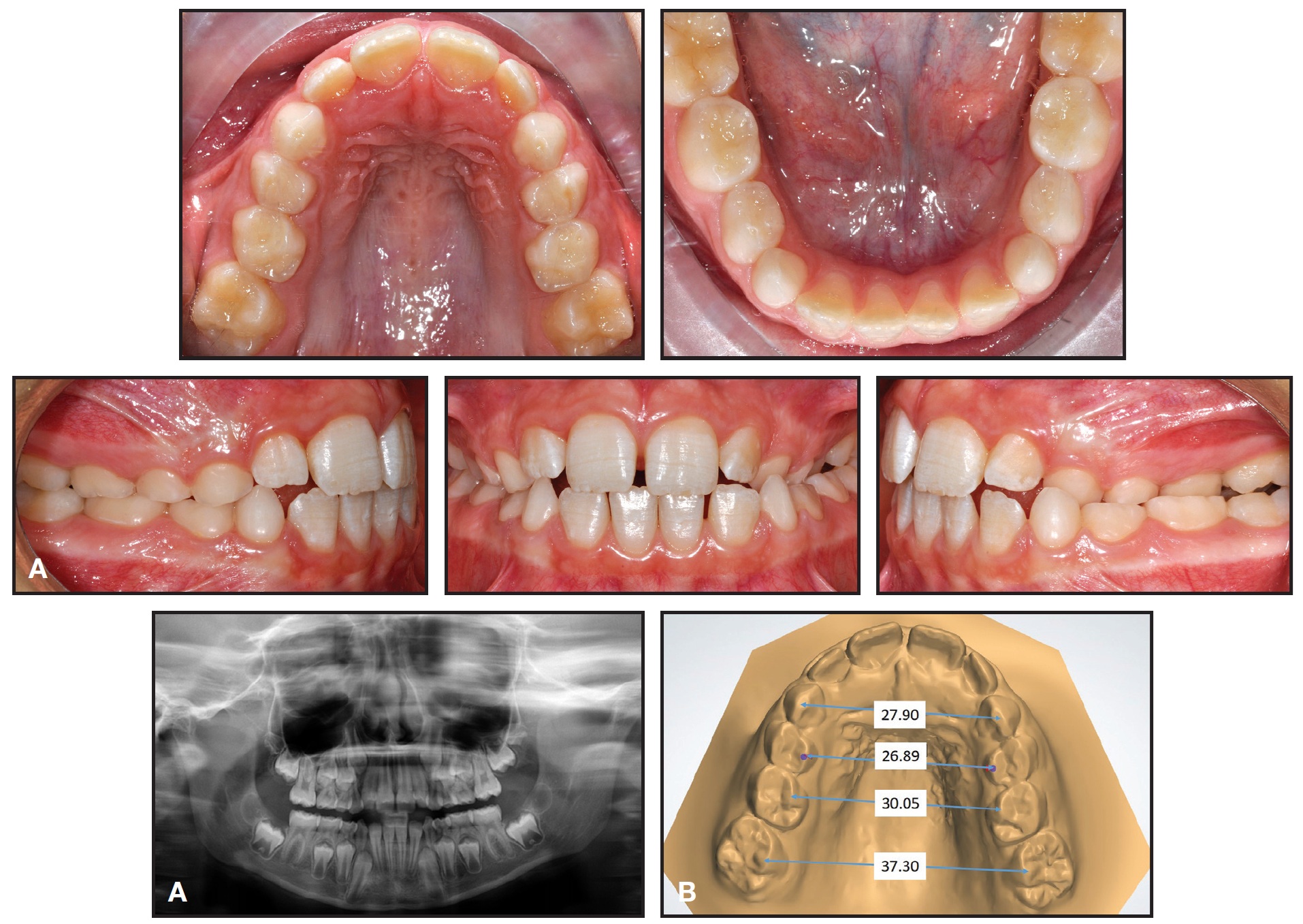
Fig. 4 Case 1. A. 8-year-old female patient with maxillary transverse deficiency, crossbite, and mandibular deviation before treatment. B. Arch-width measurements (mm) on STL digital casts obtained from laboratory scan of polyvinyl siloxane impressions.
A Leaf Expander was bonded to bands on the second deciduous molars, with extensions to the canines and first deciduous molars (Fig. 5A).
The screw was activated following the described protocol to produce 6mm of expansion (Fig. 5B).
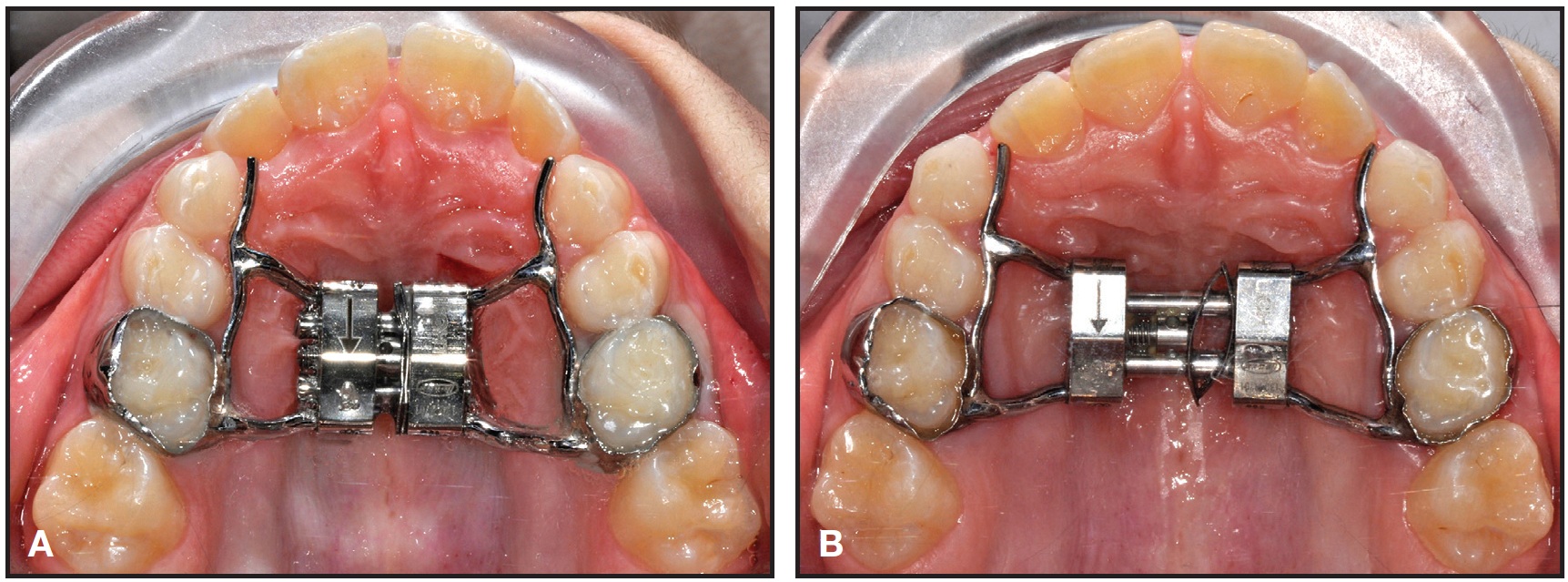
Fig. 5 Case 1. A. Leaf Expander in place. B. After six months of expansion.
Including three months of passive retention, total treatment time was nine months. The crossbite and midline deviation were corrected, the archform was improved, and the first permanent molars (especially the right one) exhibited spontaneous expansion and rotation (Fig. 6, Table 1). Results remained stable nine months after treatment (Fig. 7).
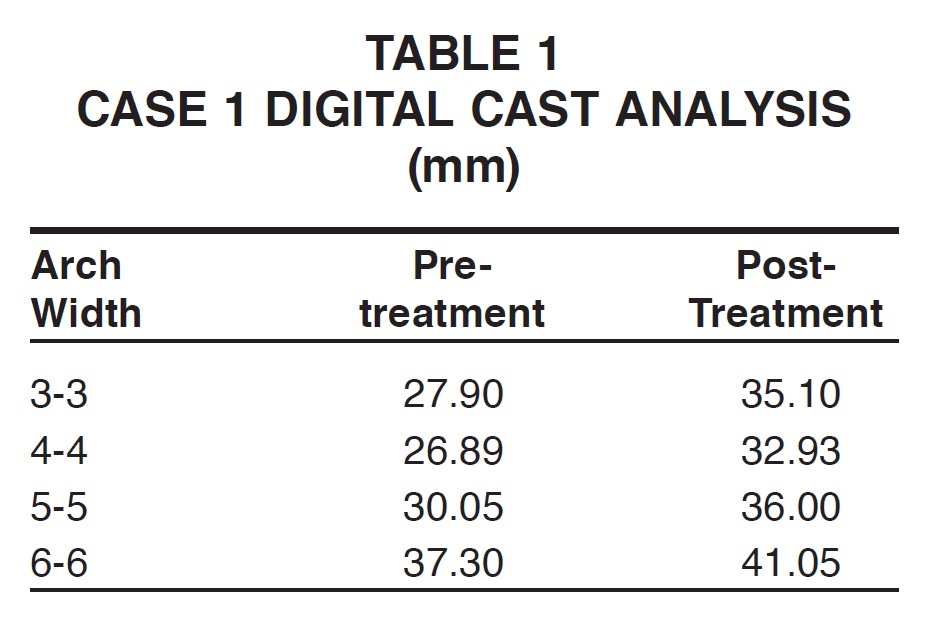
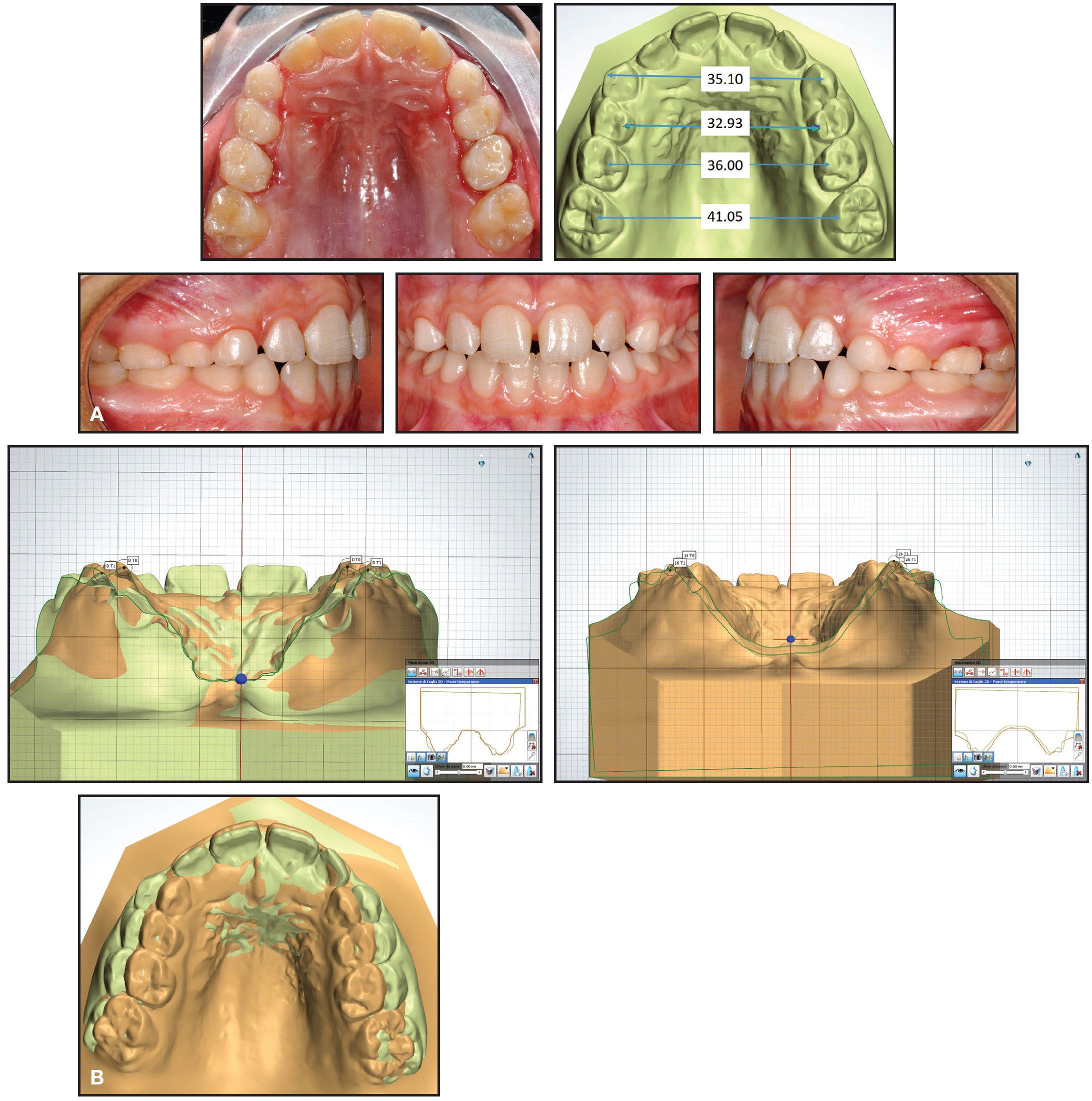
Fig. 6 Case 1. A. After three months of retention. B. Superimposition of pre- and post-treatment results on palatal rugae.

Fig. 7 Case 1. Patient nine months after treatment.
Case 2
A 7-year-old female in the mixed dentition presented with a crossbite associated with a right lateral deviation of the mandible and a transverse deficiency (Fig. 8).
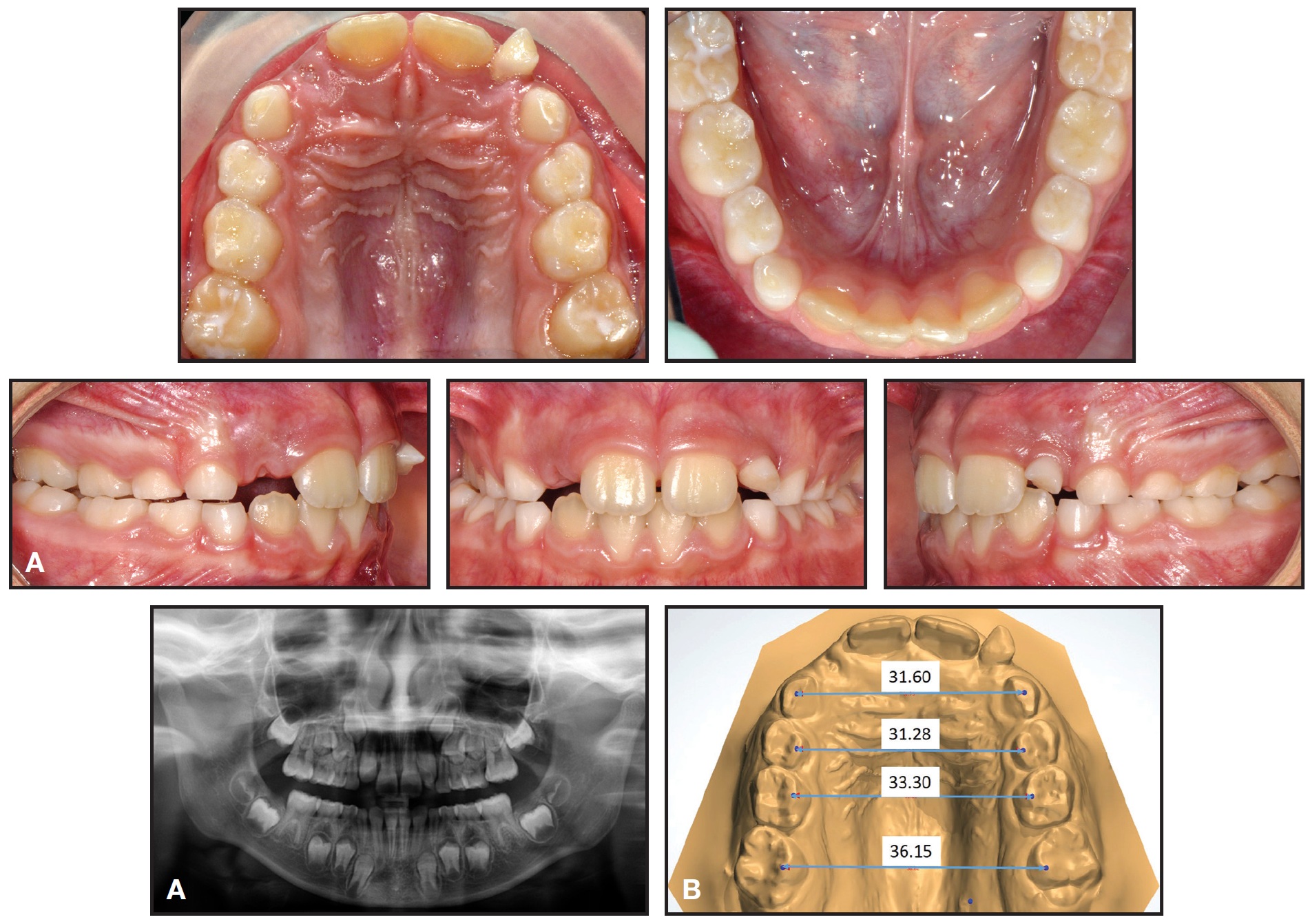
Fig. 8 Case 2. A. 7-year-old female patient with maxillary transverse deficiency, crossbite, and mandibular deviation before treatment. B. Arch-width measurements (mm) on STL digital casts obtained from intraoral scan.
A Leaf Expander was bonded to bands on the second deciduous molars, with extensions to the canines and first deciduous molars (Fig. 9A).
The screw was reactivated over the next six months to obtain 6mm of expansion (Fig. 9B).
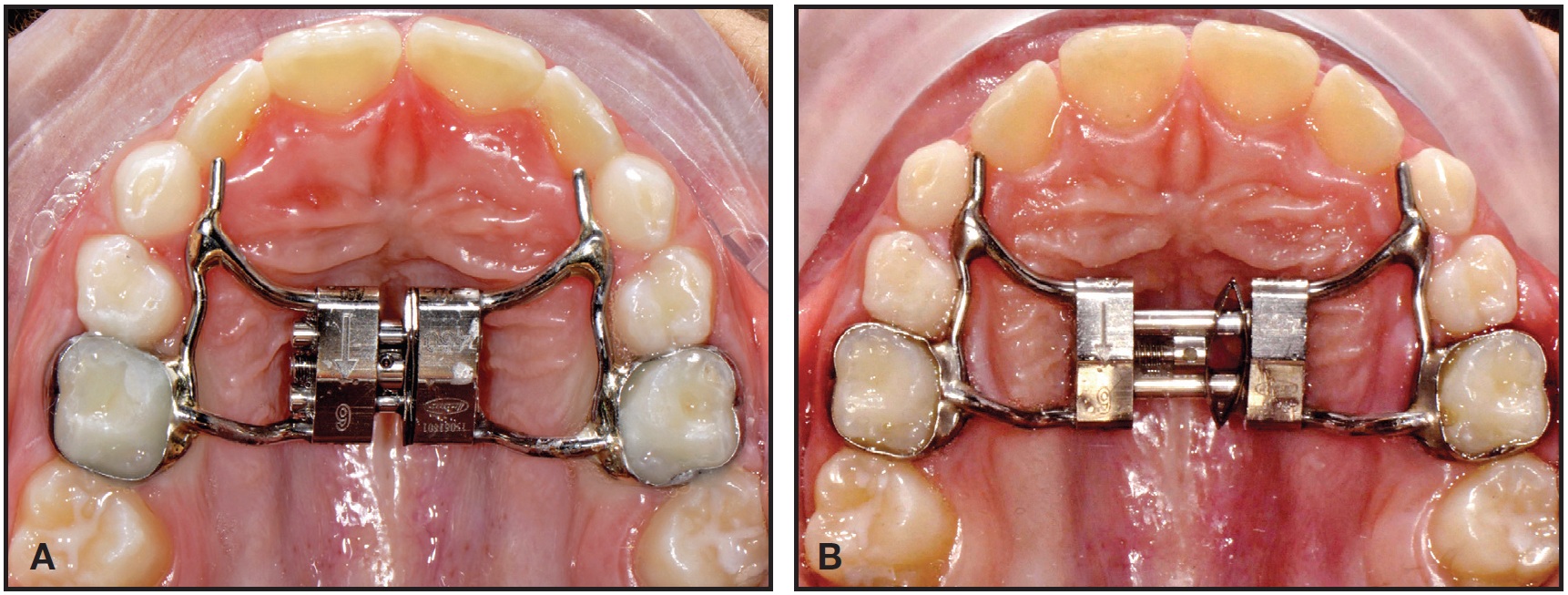
Fig. 9 Case 2. A. Leaf Expander in place. B. After six months of expansion.
After another three months of retention, the appliance was removed. Final records confirmed that the crossbite and midline deviation were corrected; the maxilla was expanded enough for eruption of the upper lateral incisors; and the first permanent molars had spontaneously expanded and rotated (Fig. 10, Table 2). Treatment results were stable nine months later (Fig. 11).
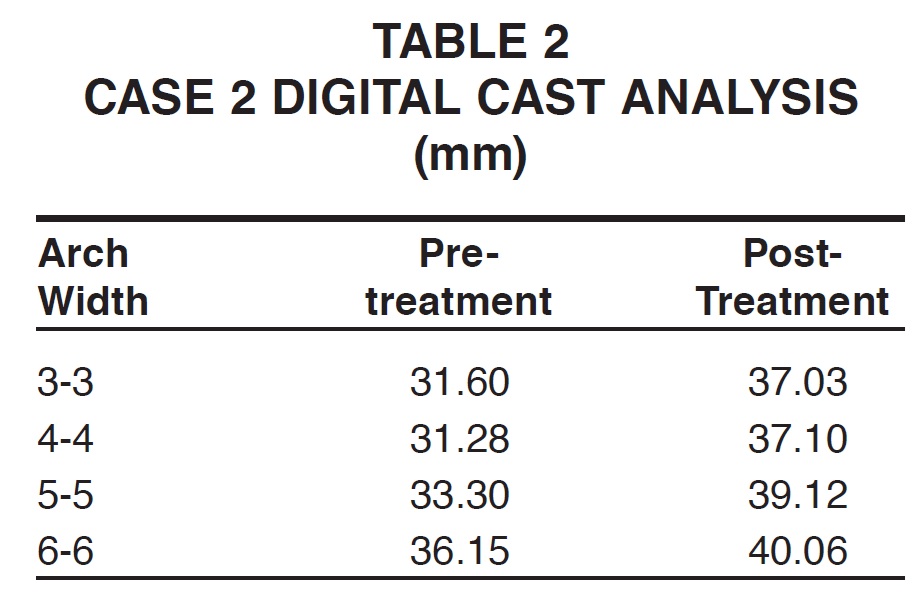
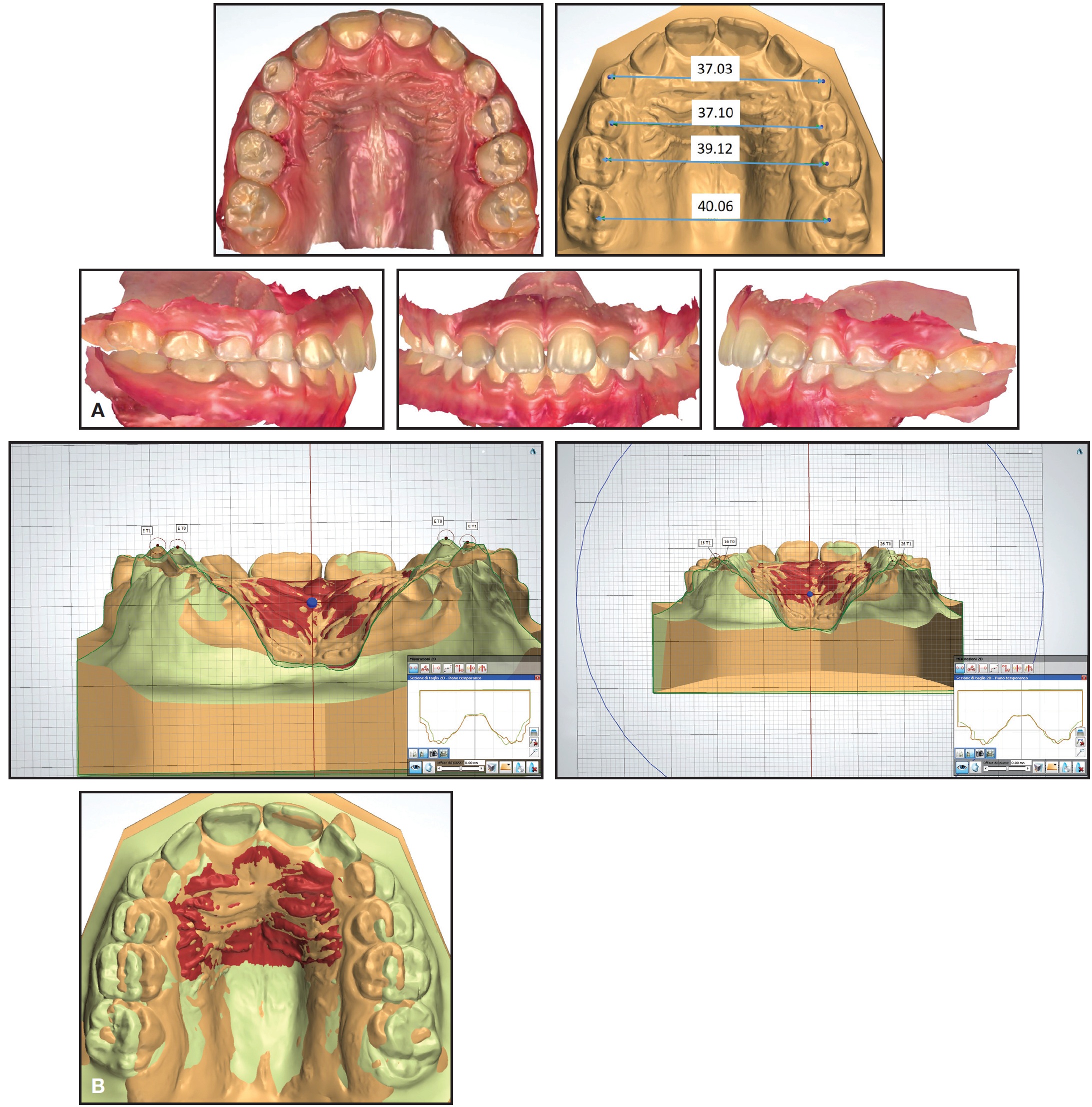
Fig. 10 Case 2. A. After three months of retention (images obtained from intraoral scan). B. Superimposition of pre- and post-treatment results on palatal rugae.

Fig. 11 Case 2. Patient nine months after treatment.
Discussion
One of the main disadvantages of a rapid palatal expander is the need for the patient's parents to perform activations at home. Moreover, it requires several closely spaced appointments to verify proper activation of the screw and determine when to stop active expansion. The Leaf Expander is an effective alternative for treatment of maxillary deficiency in growing patients. Without the need for compliance from patients or parents, it performs controlled tooth movement for expansion and avoids undesirable side effects on the permanent teeth.9 Easy and safe to activate in the office, it provides predetermined, light, and constant forces for painless expansion and predictable results.
FOOTNOTES
- *Rocky Mountain Orthodontics, Denver, CO; www.rmortho.com.
- **Leone, Florence, Italy; www.leone.it.
REFERENCES
- 1. Vardimon, A.D.; Graber, T.M.; Voss, L.R.; and Lenke, J.: Determinants controlling iatrogenic external root resorption and repair during and after palatal expansion, Angle Orthod. 61:113-122, 1991.
- 2. Pinto, A.S.; Buschang, P.H.; Throckmorton, G.S.; and Chen, P.: Morphological and positional asymmetries of young children with functional unilateral posterior crossbite, Am. J. Orthod. 120:513-520, 2001.
- 3. McNamara, J.A. Jr.: Maxillary transverse deficiency, Am. J. Orthod. 117:567-570, 2000.
- 4. Cozzani, M.; Guiducci, A.; Mirenghi, S.; Mutinelli, S.; and Siciliani, G.: Arch width changes with a rapid maxillary expansion appliance anchored to the primary teeth, Angle Orthod. 77:296-302, 2007.
- 5. Timms, D.J. and Moss, J.P.: A histological investigation into the effects of rapid maxillary expansion on the teeth and their supporting tissues, Trans. Eur. Orthod. Soc. 263-271, 1971.
- 6. Chung, C.H. and Font, B.: Skeletal and dental changes in the sagittal, vertical and transverse dimensions after rapid palatal expansion, Am. J. Orthod. 126:569-575, 2004.
- 7. Martina, R.; Cioffi, I.; Farella, M.; Leone, P.; Manzo, P.; Matarese, G.; Nucera, R.; and Cordasco, G.: Transverse changes determined by rapid and slow maxillary expansion -- A low-dose CT-based randomized controlled trial, Orthod. Craniofac. Res. 15:159-168, 2012.
- 8. Gianolio, A.; Cherchi, C.; and Lanteri, V.: Rapid and slow maxillary expansion: A posteroanterior cephalometric study, Eur. J. Paediat. Dent. 15:415-418, 2014.
- 9. Lione, R.; Franchi, L.; and Cozza, P.: Does rapid maxillary expansion induce adverse effects in growing subjects? Angle Orthod. 83:172-182, 2013.
-
 DR. LANTERI
DR. LANTERI -
DR. BERETTA
-
DR. LANTERI
-
DR. GIANOLIO
-
DR. CHERCHI
-
DR. FRANCHI
.