A Rapid Maxillary Expander with Differential Opening
A significant percentage of complete cleft lip and palate (CLP) patients who have undergone lip and palate surgeries in infancy or early childhood will later present with maxillary arch constriction. 1-3 Studies of maxillary archform in patients with complete CLP have demonstrated that the cleft segments collapse by rotating medially, with the fulcrum in the maxillary tuber, thereby causing progressive anterior constriction.4-7 This situation results in a greater reduction in intercanine width than in intermolar width, and the difference is even more pronounced in complete bilateral CLP patients than in unilateral CLP patients.6
Many attempts have been made to produce greater expansion in the maxillary canine regions of CLP patients by changing the design of conventional expanders.8-11 Although a few appliances, including the Quad Helix* and the "W" arch, have been successful,8 conventional devices for rapid maxillary expansion (RME) are limited to one direction, along the axis of the expansion screw, and thus cannot provide differential expansion. A modification such as a fan-shape design will expand only the intercanine distance, not the intermolar distance.9,11
This article presents a new expander with differential opening (EDO**) that can be used both in patients with difficult alveolar cleft deformities and in non-cleft patients with unusual archforms.
Similar articles from the archive:
Expander Design
The expansion component of the device is in the shape of a rectangle that can be converted to a trapezoid. Two expansion screws are positioned transversely, and two supporting bars are initially positioned perpendicular to the expansion screws. The wire arms are 1.5mm in diameter, similar to a Hyrax expander. Each corner of the EDO houses a 10mm screw that attaches to the turnbuckle expansion screw and pivots during expansion (Fig. 1A). The expansion screws engage the antero-posterior bars in the same manner as with a fan-shaped expander.
A 1.2mm-diameter round transverse bar between the two screws acts as a stabilizer to prevent forward or backward displacement of the expander and the supporting teeth. If the anterior and posterior screws are equally activated, the EDO opens in a parallel configuration (Fig. 1B). When more expansion is required between the canines, the anterior screw is activated further to create anterior divergence (Fig. 1C).
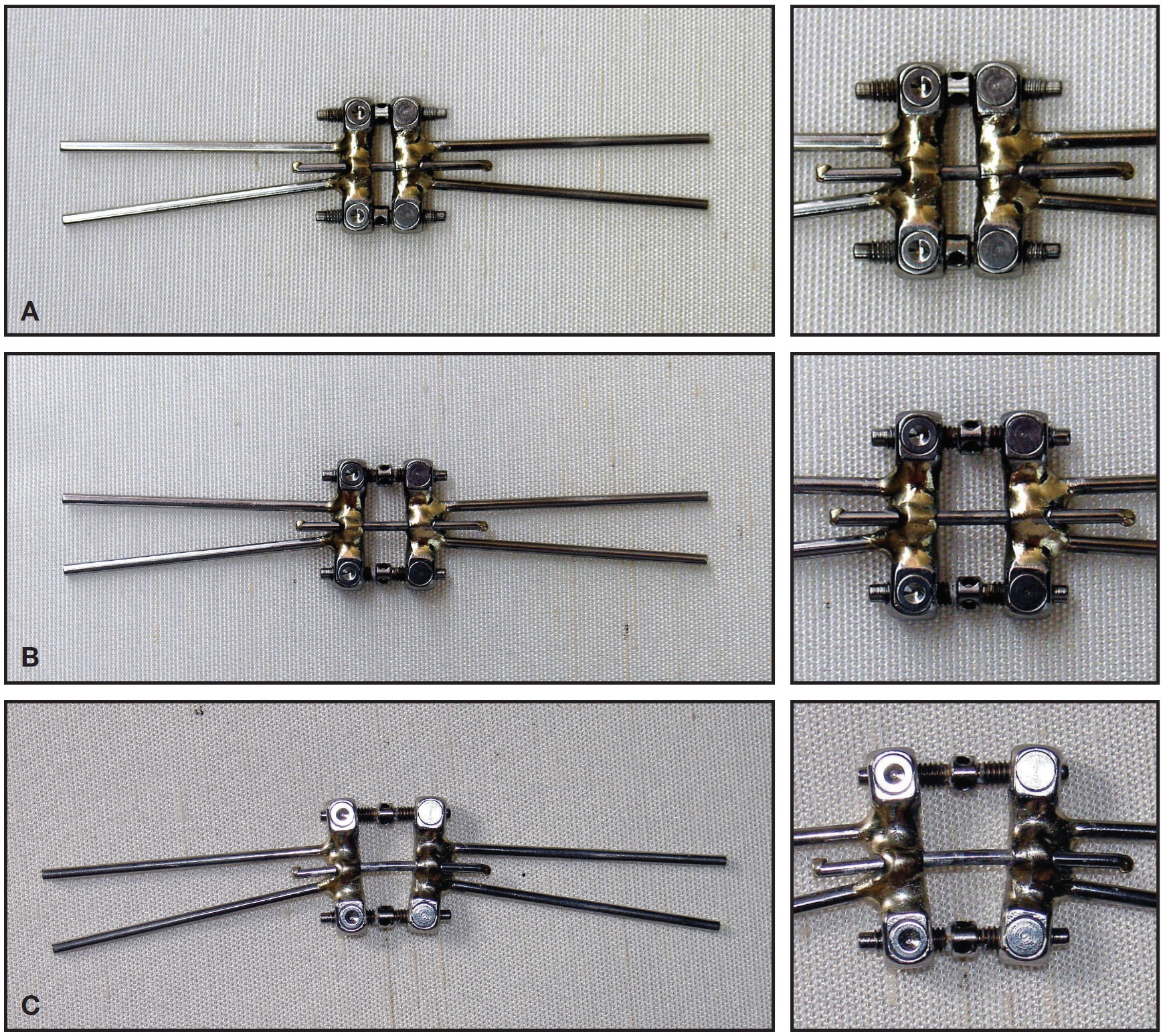
Fig. 1 Expansion screw with differential opening (EDO). A. Before activation. B. After activation of both anterior and posterior screws. C. Additional activation of anterior screw, producing differential expansion.
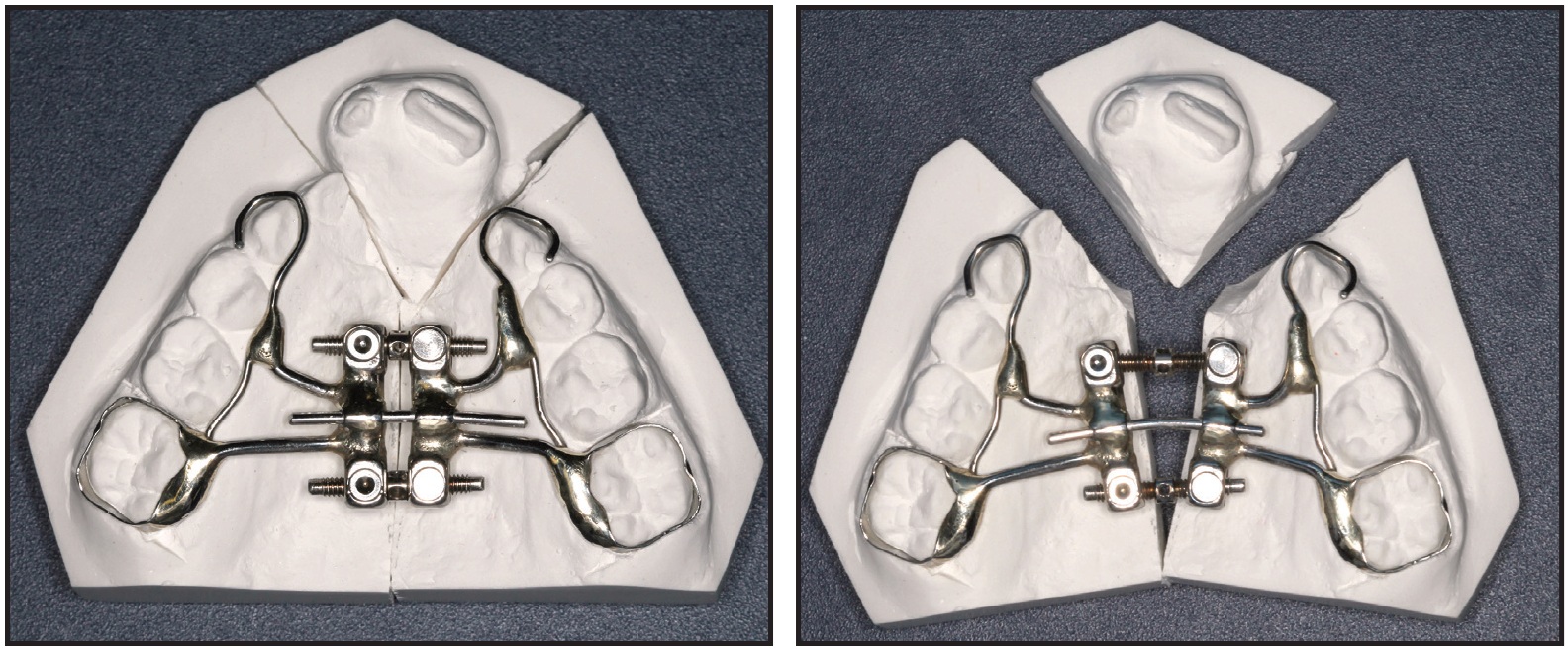
Fig. 2 Substantial differential expansion between anterior (8mm) and posterior (2mm) screws shown on plaster cast. Pivoting corner screws prevent binding of expansion screws.
Case 1
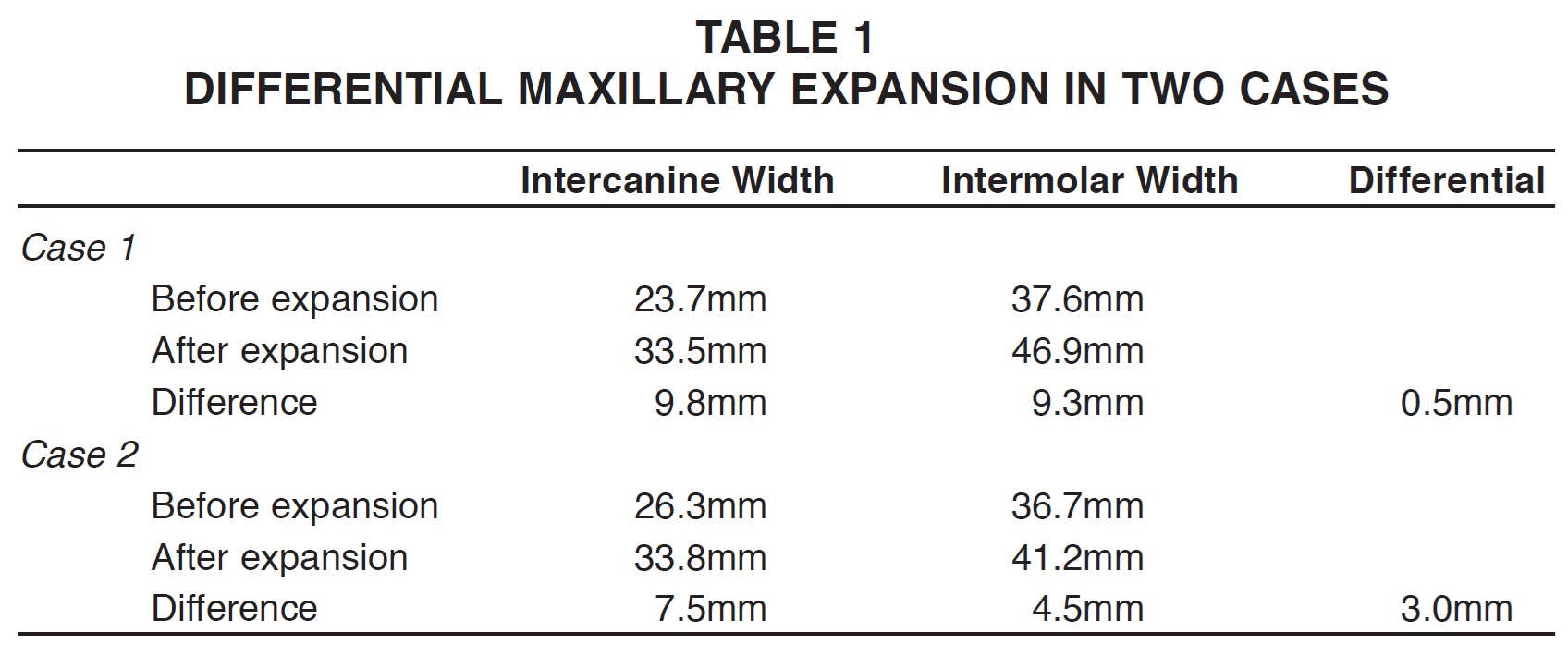
A 9-year-old female in the mixed dentition presented with bilateral CLP (Fig. 3A). An EDO was placed (Fig. 3B), and both the anterior and posterior screws were activated with one complete turn (about .8mm) per day for 10 days, until the desired intermolar expansion was achieved. The anterior screw was then activated with one complete turn for an additional two days to increase the anterior arch width (Fig. 3C). The archform was improved by a differentially greater increase (.5mm) in the intercanine distance (Fig. 3D,E, Table 1).
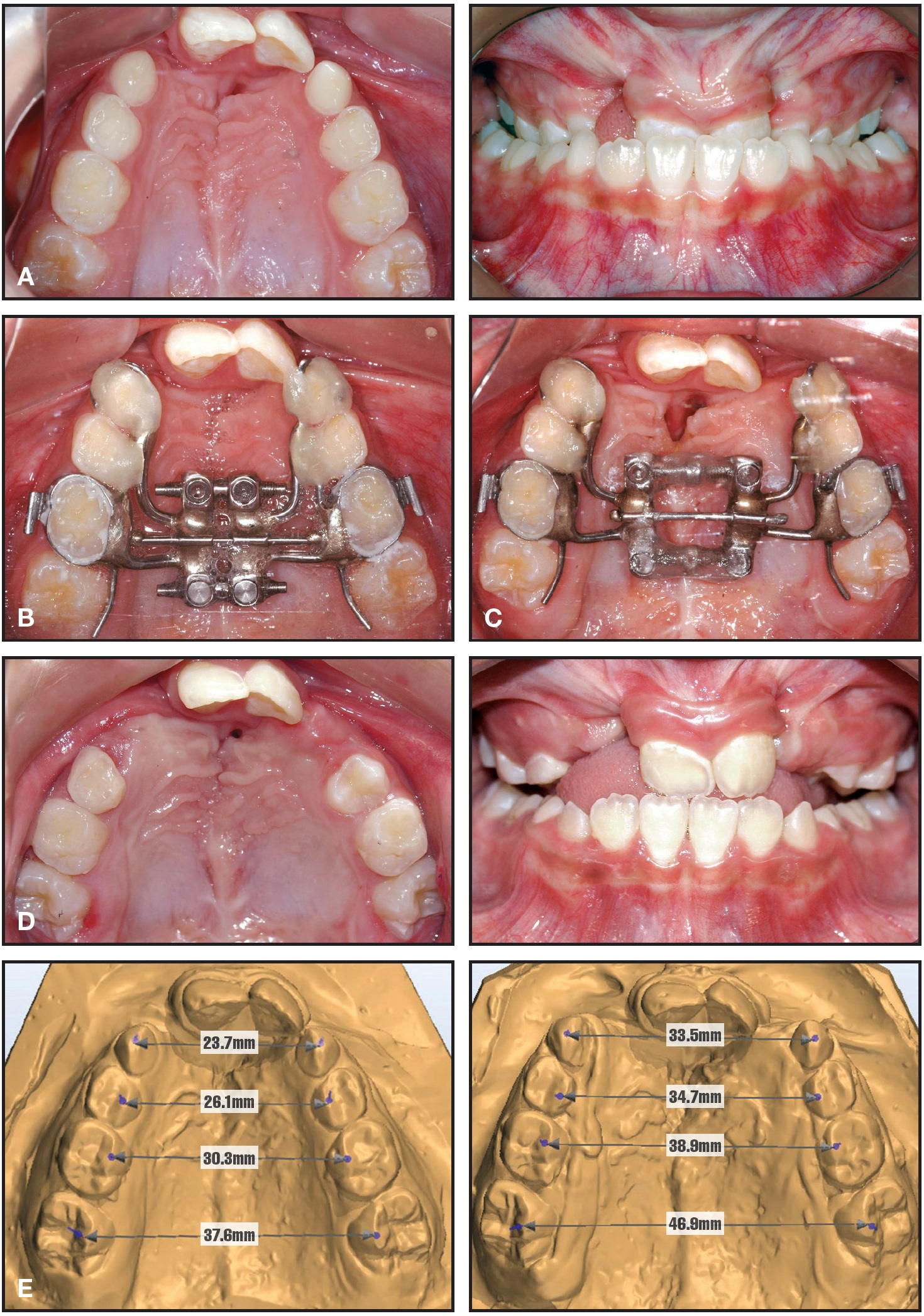
Fig. 3 Case 1. A. 9-year-old female patient with complete bilateral cleft lip and palate. B. Placement of EDO. C. After 10 days of activation of both screws and additional two days of anterior-only activation. D. Six months later, after removal of expander, exfoliation of maxillary deciduous canines, closure of oronasal fistula, and alveolar bone graft. E. Comparison of palatal widths before and after expansion.
Case 2
An 8-year-old male with bilateral CLP required even more differential expansion between the posterior and anterior segments (Fig. 4A). After an EDO was placed (Fig. 4B) and both screws were activated for five days, the anterior screw was activated for another four days (Fig. 4C). The canines were expanded 3mm more than the molars (Fig. 4D,E, Table 1).
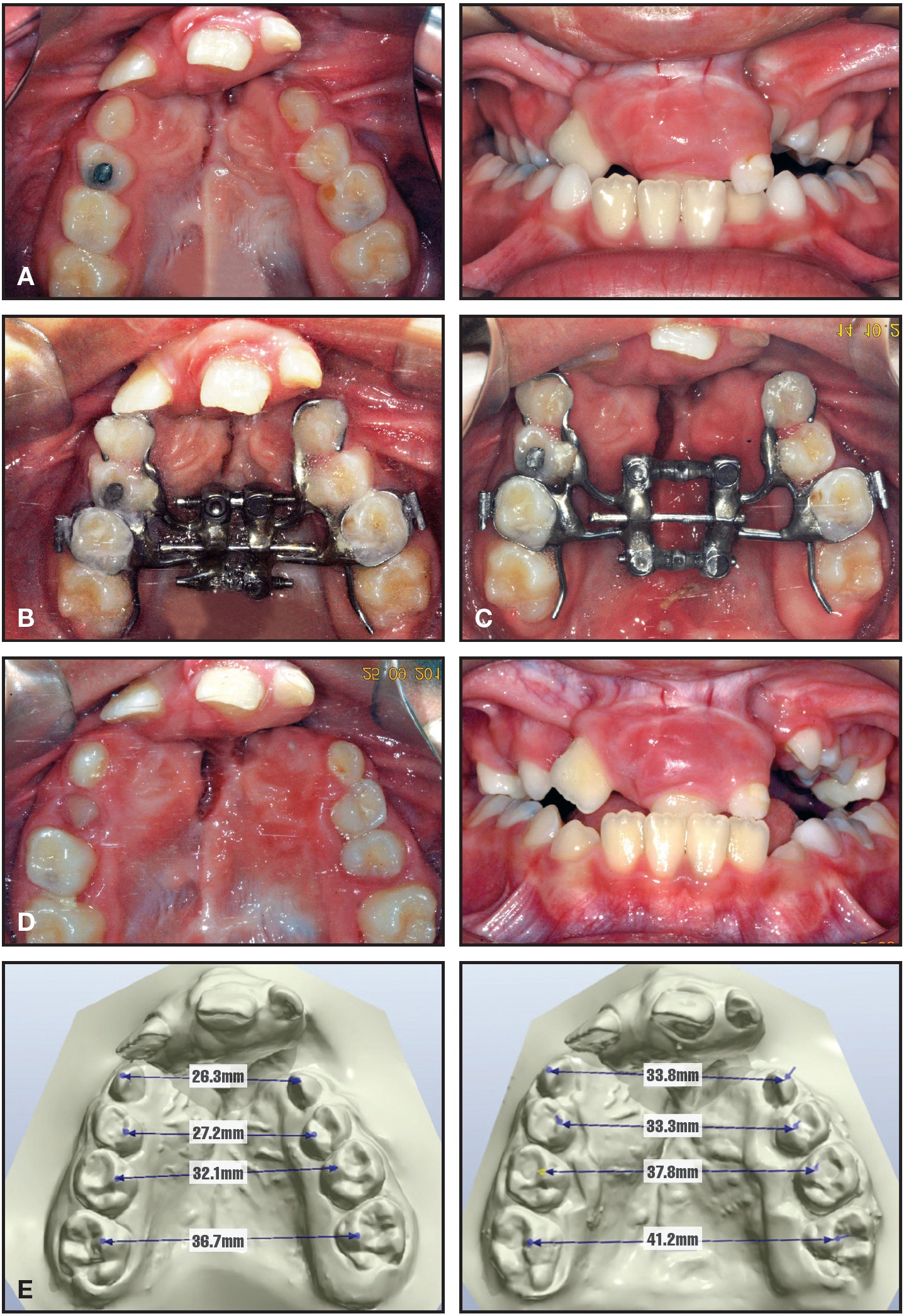
Fig. 4 Case 2. A. 8-year-old male patient with complete bilateral cleft lip and palate. B. Placement of EDO. C. After five days of activation of both screws and additional four days of anterior-only activation. D. Six months later, after removal of expander. E. Comparison of palatal widths before and after expansion, showing 3mm differential between intercanine and intermolar expansion.
Discussion
The shape of the maxillary arch in children with CLP can vary with the extent and size of the cleft defect and the technique used to repair the lip and palate, since a cleft segment tends to collapse into the void of the cleft. The goal of maxillary expansion in these cases is to coordinate the archform before an alveolar bone graft is performed. When conventional RME is used in a patient with complete CLP, the anterior and posterior segments of the arch will expand simultaneously, risking overexpansion of the intermolar distance in an effort to correct the intercanine distance. This can result in a buccal crossbite, which can produce undesirable long-term periodontal consequences such as buccal bone dehiscences and gingival recessions.12,13
An EDO allows the orthodontist to correct the intercanine width of a cleft segment relative to the intermolar width. The EDO prevents overexpansion of the intermolar distance and thus avoids negative periodontal side effects on the buccal aspects of the posterior teeth.
In an adult CLP patient who requires surgically assisted rapid maxillary expansion (SARME), neither a Hyrax expander nor a fan-shaped expander can produce an ideal archform. An EDO allows the clinician to control anterior and posterior expansion prior to SARME. The EDO can also be used in non-cleft patients to correct archforms with severe maxillary constriction, especially those with relative differences in anterior and posterior arch width.
ACKNOWLEDGMENT: The authors thank the Sao Paulo Research Foundation (FAPESP No. 2009/17622-9) for its financial support and the University of Sao Paulo Innovation Agency for its assistance in the patent process. The authors are also grateful to Dr. James A. McNamara Jr. for his support in the development of the EDO.
FOOTNOTES
- *Rocky Mountain Orthodontics, Inc., Denver, CO; www.rmortho.com.
- **Great Lakes Orthodontics, Tonawanda, NY; www.greatlakesortho.com.
REFERENCES
- 1. Da Silva Filho, O.G.; Ramos, A.L.; and Abdo, R.C.: The influence of unilateral cleft lip and palate on maxillary dental arch morphology, Angle Orthod. 62:283-290, 1992.
- 2. Mazaheri, M.; Athanasiou, A.E.; Long, R.E. Jr.; and Kolokitha, O.G.: Evaluation of maxillary dental arch form in unilateral clefts of lip, alveolus, and palate from one month to four years, Cleft Pal. Craniofac. J. 30:90-93, 1993.
- 3. Pruzansky, S. and Aduss, H.: Arch form and the deciduous occlusion in complete unilateral clefts, Cleft Pal. J. 30:411-418, 1964.
- 4. Da Silva Filho, O.G.; de Castro Machado, F.M.; de Andrade, A.C.; de Souza Freitas, J.A.; and Bishara, S.E.: Upper dental arch morphology of adult unoperated complete bilateral cleft lip and palate, Am. J. Orthod. 114:154-161, 1998.
- 5. Harding, R.L. and Mazaheri, M.: Growth and spatial changes in the arch form in bilateral cleft lip and palate patients, Plast. Reconstr. Surg. 50:591-599, 1972.
- 6. Heidbuchel, K.L. and Kuijpers-Jagtman, A.M.: Maxillary and mandibular dental-arch dimensions and occlusion in bilateral cleft lip and palate patients from 3 to 17 years of age, Cleft Pal. Craniofac. J. 34:21-26, 1997.
- 7. Heidbuchel, K.L.; Kuijpers-Jagtman, A.M.; Van't Hof, M.A.; Kramer, G.J.; and Prahl-Andersen, B.: Effects of early treatment on maxillary arch development in BCLP: A study on dental casts between 0 and 4 years of age, J. Craniomaxillofac. Surg. 26:140-147, 1998.
- 8. Aizenbud, D.; Ciceu, C.; Rachmiel, A.; and Hazan-Molina, H.: Reverse quad helix appliance: Differential anterior maxillary expansion of the cleft area before bone grafting, J. Craniofac. Surg. 23:e440-443, 2012.
- 9. Devenish, E.A.; Foster, T.D.; and Chinn, D.: An improved method of differential rapid maxillary expansion in cleft palate, Br. J. Orthod. 9:129-131, 1982.
- 10. Subtelny, J.: The importance of early orthodontic treatment in cleft palate planning, Angle Orthod. 27:148-158, 1957.
- 11. Suzuki, A. and Takahama, Y.: A jointed fan-type expander: A newly designed expansion appliance for the upper dental arch of patients with cleft lip and/or palate, Cleft Pal. Craniofac. J. 26:239-241, 1989.
- 12. Garib, D.G.; Henriques, J.F.; Janson, G.; de Freitas, M.R.; and Fernandes, A.Y.: Periodontal effects of rapid maxillary expansion with tooth-tissue-borne and tooth-borne expanders: A computed tomography evaluation, Am. J. Orthod. 129:749-758, 2006.
- 13. Rungcharassaeng, K.; Caruso, J.M.; Kan, J.Y.; Kim, J.; and Taylor, G.: Factors affecting buccal bone changes of maxillary posterior teeth after rapid maxillary expansion, Am. J. Orthod. 132:428 e1-8, 2007.
-
 DR. GARIB
DR. GARIB -
 MR. GARCIA
MR. GARCIA -
 MR. PEREIRA
MR. PEREIRA -
 DR. LAURIS
DR. LAURIS -
 DR. YEN
DR. YEN
Dr. Garib is an Associate Professor, Mr. Garcia and Mr. Pereira are orthodontic technicians, and Dr. Lauris is an orthodontist, Hospital for Rehabilitation of Craniofacial Anomalies and Bauru Dental School, University of São Paulo, Brazil. Dr. Yen is an Associate Professor, Ostrow School of Dentistry, University of Southern California, Los Angeles. E-mail Dr. Garib at dgarib@uol.com.br.