The Effect of Vibration on the Rate of Leveling and Alignment
Numerous concepts have been developed with the aim of increasing the speed of orthodontic tooth movement and potentially reducing overall treatment time. Unfortunately, most have failed to generate the supporting data needed to gain wide acceptance.1,2 Even if treatment time were not a significant issue for many patients and practitioners,3 the prospect of improving the effectiveness of biomechanics through enhanced tooth movement would be a worthy goal that warrants further clinical investigation.
The purpose of this study was to evaluate the effects of vibration with AcceleDent* (Fig. 1) on the speed of orthodontic leveling and alignment.
Biological and Mechanical Effects of Vibration
As early as 1979, Shapiro and colleagues reported the use of pulsating force-induced piezoelectricity to stimulate tooth movement.4 In 1982, Kurz received a patent for a vibrating headgear/ mouthpiece device.5 In 1986, investigators at the Children's Clinical Hospital No. 2 of Kiev concluded that vibration at 50Hz for 60-360 seconds every two or three days reduced the time needed to move a tooth by a factor of 1.5-2 times.6 Although academic interest in the orthodontic effects of vibration waned until the beginning of the 21st century, it persisted in orthopedic medicine.
Similar articles from the archive:
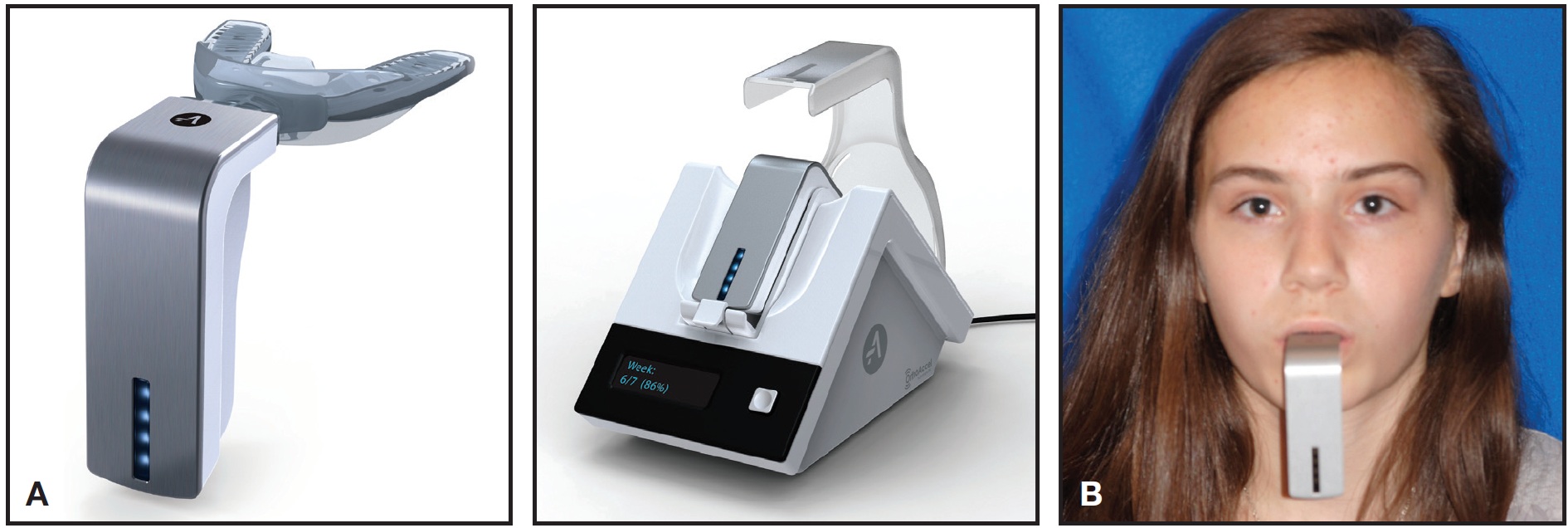
Fig. 1 A. AcceleDent* activator and charging port (images used by permission of OrthoAccel Technologies). B. AcceleDent device in use.
Beginning in 2003, animal studies demonstrated an increased sutural response7,8 and more rapid tooth movement after vibratory stimulation.9,10 One investigation did find an inhibition of translational tooth movement in rats during a brief two-week experimental period,11 but another reported a 40% increase in the rate of tooth movement in mice after light daily vibration over four weeks.12 Since vibration stimulates inflammation, these animal models suggested the potential to alter the periodontal apparatus or create osteogenic effects13 through genetic expression, cytokine activity, cellular changes,14 or recruitment, thereby enhancing tooth movement.
In addition to producing biological effects, vibration may also work on a biomechanical level to accentuate orthodontic tooth movement. Braun and colleagues credited the dynamic environment of the oral cavity ("vibrational" perturbations) as the primary influence in moderating the rate of tooth movement with fixed appliances.15 Researchers at the University of Missouri-Kansas City found that the most important factor was the amplitude of archwire vibrations.16 Other authors have refuted the simplistic claims that "reducing [elastic] friction" by the mere choice of appliance can shorten treatment time. It is actually the inelastic friction (or "notching") that must be overcome with perturbations, and all brackets are subject to that property--we are not just sliding pearls along a string.17-19 Consequently, it appears that vibration could affect the rate of orthodontic tooth movement in two ways: reducing the "lag"phase by stimulating changes in the periodontal apparatus, or inducing mechanical perturbations within the appliance interface.
Materials and Methods
This retrospective evaluation of the effects of vibration on the time required for mandibular leveling and alignment included 117 consecutively treated Class II nonextraction patients (47 male, 70 female) who underwent maxillary molar distalization and concurrent mandibular leveling and alignment (Table 1).
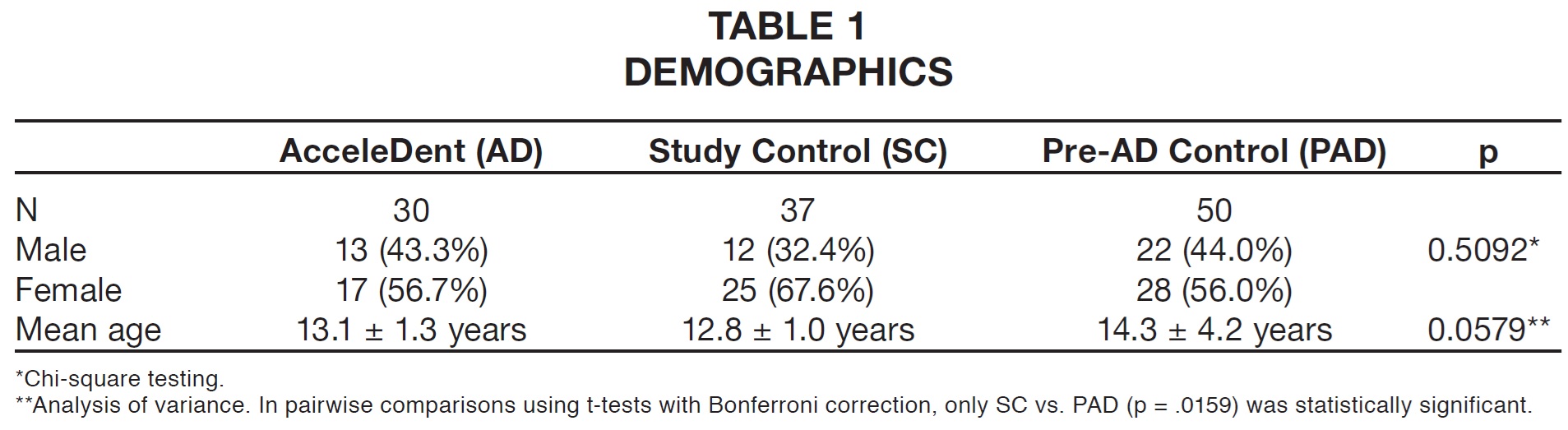
Thirty patients were enrolled in the AcceleDent vibration (AD) group (mean age = 13.1 years) and 37 in the study control (SC) group (mean age = 12.8 years). The pre-AD (PAD) control group comprised 50 Class II patients (mean age = 14.3 years) who were treated prior to the initiation of a separate prospective examination of the effects of vibration on molar distalization, whose results will be published later.
Each patient presented with a half-to-fullstep Class II molar relationship and mild-to-moderate crowding. The nonextraction treatment involved a miniscrew-supported Horseshoe Jet** maxillary molar distalizer20 and a preadjusted .022" Butterfly System***21 mandibular appliance (Figs. 2AB, 2C-E, 2F, 3AD, 3E, 4A-E, 4E.

Fig. 2 A. 14-year-old female Class II patient before treatment. B. After placement of Horseshoe Jet** maxillary molar distalizer and preadjusted Butterfly System*** mandibular brackets with initial .016" nickel titanium archwire. Patient was scheduled for appointments every four weeks and instructed to use AcceleDent vibration unit for 20 minutes per day.
Upon completion of molar distalization, the Horseshoe Jet was "locked" to serve as indirect miniscrew anchorage for subsequent retraction of the remaining maxillary teeth, and upper brackets were bonded for the finishing stage.
The PAD patients had been previously treated with orthodontic adjustments at five-to-seven-week intervals. The AD and SC subjects were instructed to return every four weeks as part of a different prospective investigation of molar distalization. Otherwise, all patients experienced the same sequence of treatment mechanics.
Each patient in the AD sample received an AcceleDent vibrational unit with directions to use the device 20 minutes per day during the entire course of orthodontic treatment. The AcceleDent activator supplies mild vibration (30Hz, .25N) to the teeth as the patient lightly bites down on a mouthpiece to hold the device in place.22
For purposes of this study, alignment was defined as the sufficient resolution of dental irregularities to permit complete seating of a rectangular archwire with a minimum dimension of .017" x .025" stainless steel or superelastic alloy (but smaller than .019" x .025" stainless steel) into .022" x .028" brackets (Fig. 2C).
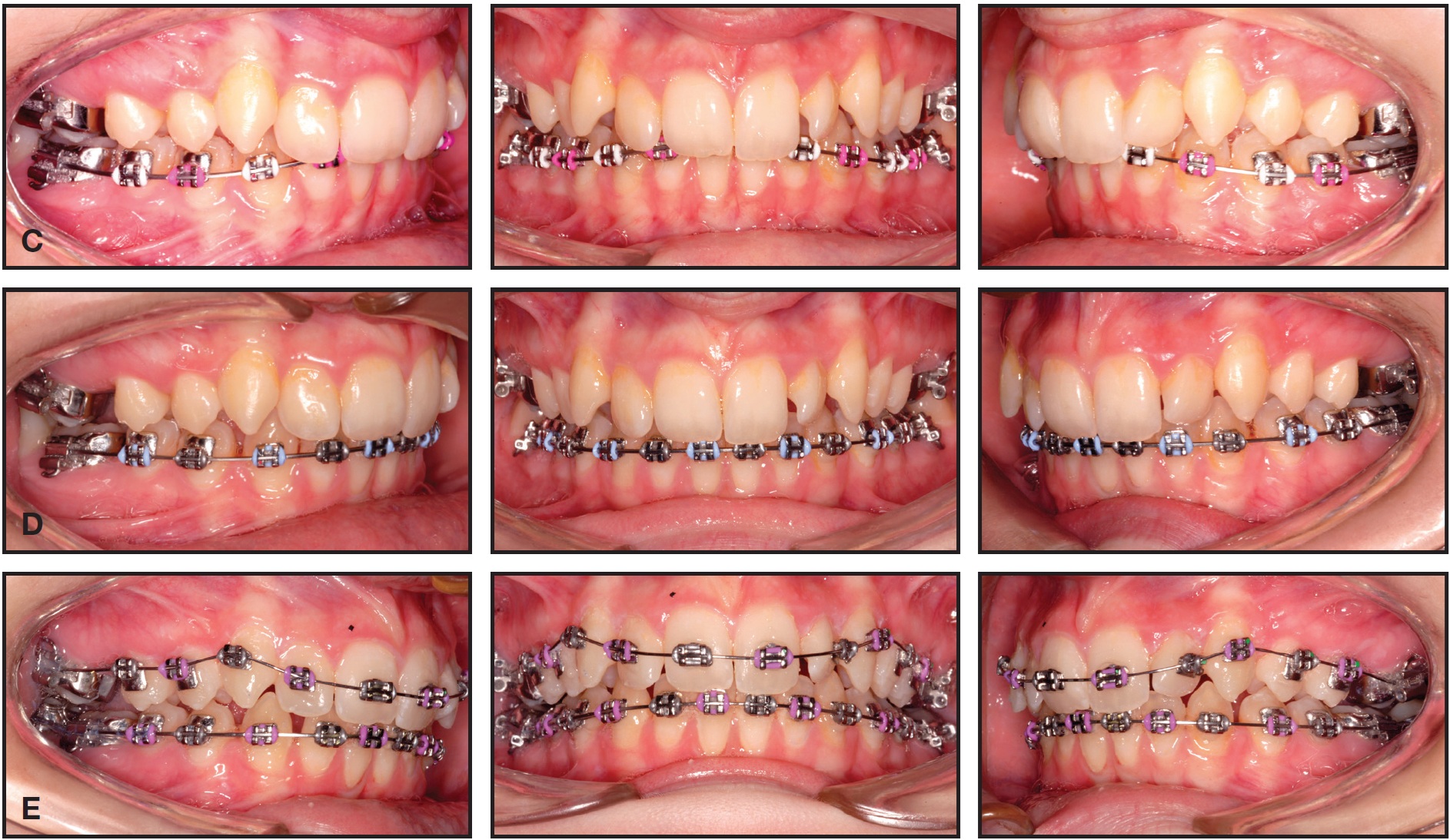
Fig. 2 (cont.) C. Mandibular .019" × .025" nickel titanium archwire inserted after 95 days of treatment, marking end of alignment phase. D. Mandibular .019" × .025" stainless steel archwire inserted after six months of treatment, marking completion of leveling. E. Maxillary brackets bonded and second molars banded after seven months of treatment.
Every patient began treatment with an .016" nickel titanium archwire, usually followed by .017" x .025" nickel titanium.
Leveling was defined as the sufficient resolution of vertical dental discrepancies to allow complete seating of a rectangular archwire with a minimum dimension of .019" x .025" stainless steel into the bracket slots (Figs. 2D, 3C,4C).

Fig. 2 (cont.) F. Treatment completed in 20 months.

Fig. 3 A. 13-year-old female Class II patient before treatment. B. After insertion of maxillary Horseshoe Jet, bonding of mandibular Butterfly System brackets, and delivery of AcceleDent. C. After 55 days of alignment and 83 days of leveling. D. Maxillary brackets bonded and right canine exposed with diode laser after nine months of treatment.

Fig. 3 (cont.) E. Treatment completed in 20 months.

Fig. 4 A. 12-year-old female Class II patient before treatment. B. After insertion of maxillary Horseshoe Jet, bonding of mandibular Butterfly System brackets, and delivery of AcceleDent. C. After 37 days of alignment and 95 days of leveling. D. Maxillary brackets bonded after 14 months of treatment.

Fig. 4 (cont.) E. Treatment completed in 20 months.
Although most subjects achieved this degree of leveling with a three-wire sequence, some also received an interim .017" x .025" stainless steel or .019" x .025" nickel titanium archwire before the larger stainless steel working wire was placed. Some patients were excluded from the study because their archwire sequences were interrupted by earlier bonding of second-molar brackets prior to insertion of the .019" x .025" stainless steel wires. This reduced the sample size for completion of leveling from 117 to 93 subjects.
The time points and subjective goals selected for analysis did not guarantee that all rotations were absolutely resolved, nor that every curve of Spee was completely leveled, when the working archwire was placed. Since the clinical decisions were all made by the same orthodontist and all patients were selected for the same type of treatment mechanics, it seems reasonable to make comparisons among these three groups. Statistical analysis was conducted using SAS version 9.2†. The significance of differences in age was tested by analysis of variance, while gender differences were evaluated with chi-square testing. For the primary outcomes, two-sided t-tests were used to compare the three groups, using a two-tailed significance level of .05.
Results
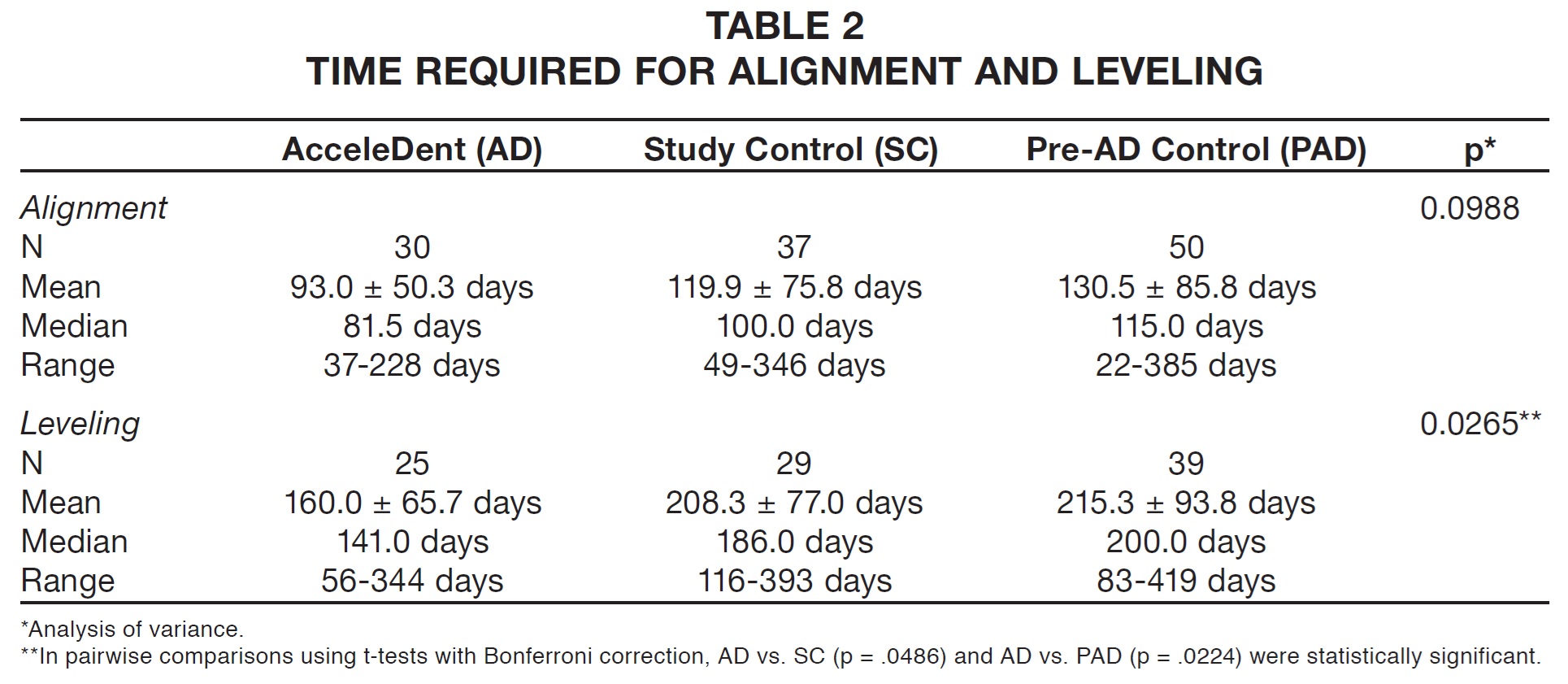
Although the PAD group was older on average than the other two samples, no statistically significant differences in age were found (Table 1). Likewise, there were no significant differences among the three groups in terms of gender. The average time period needed to attain alignment of the mandibular dentition (Table 2) was shorter in the AD group (93 days) than in either the SC group (120 days) or the PAD control group (131 days). The .017" x .025" archwire was placed in the AD patients about 27 days earlier (29% faster) on average than in the SC patients and 38 days earlier (40% faster) than in the PAD subjects. It is important to note that these differences, while clinically relevant, were not statistically significant.
The average time needed to achieve leveling (Table 2) in the AD group was 160 days--48 days less than in the SC patients (30% faster) and 55 days less than in the PAD patients (35% faster). In other words, leveling took a little more than five months with vibration, compared to seven months without vibration. These differences were both clinically and statistically significant.
Discussion
Alignment and Leveling in the Mandibular Arch
Mandall and colleagues reported that the mean time required to reach a mandibular .019" x .025" working archwire with an .022" appliance was 6.8-9.3 months, depending on which of three archwire sequences was chosen.23 Flores-Mir agreed that an archwire sequence of .016" nickel titanium, .018" x .025" nickel titanium, and .019" x .025" stainless steel was slightly more efficient than other sequences tested.24 In contrast, both Ong and colleagues25 and Jian and colleagues26 found no significant differences in alignment efficiency among three typical archwire sequences. In the Ong study, the time needed to reach an .016" x .022" stainless steel working archwire with an .018" appliance was 4.0-4.4 months using a three-wire sequence: .014" nickel titanium or copper nickel titanium followed by .017" x .017", .016" x .022", or .014" x .025" heat-activated superelastic wires.25 These authors attributed the faster leveling and alignment in comparison to the Mandall study23 to the replacement of archwires "as soon as complete engagement was possible", also noting "decreased 'play' in an .018" slot appliance". Interestingly enough, neither group found any difference in alignment efficiency between conventional nickel titanium and superelastic heat-activated wires.
In the present study, a three-to-four-wire sequence (similar to that of the Mandall23 and Flores- Mir24 investigations) was used to reach a rectangular stainless steel working wire in the mandibular arch. This required an average of five months with vibration (AD) or seven months without vibration (PAD). The difference between our results and those of Ong and colleagues25 may simply confirm their supposition that the difference in tolerance between .022" and .018" slots was responsible for the difference in the rate of alignment--especially since succeeding wires were inserted as soon as possible in both studies.
Because this was a retrospective investigation, we did not consider collecting progress records at time points representing the completion of leveling and alignment. Therefore, an objective comparative analysis such as the Peer Assessment Rating, Irregularity Index, or ABO score could not be used. On the other hand, the retrospective design prevented the introduction of a Hawthorne Effect ("preferential" alteration of archwire sequences or appointment intervals among the three samples) or a susceptibility bias that might have affected the results27; in fact, the subjects were already enrolled in a separate prospective trial. Furthermore, the study design precluded any detection or exclusion biases, since all patients presented with similar malocclusions, were treated similarly, and were not selected out of a group of finished cases.
No statistically significant difference was found between the two control groups (SC and PAD) in either leveling or alignment, even though the SC patients were seen at more regimented four-week intervals compared to the five-to-seven-week appointment windows for PAD subjects. This finding lends additional support to the validity of the three-way comparative analysis.
Effects of Vibration on the Rate of Tooth Movement
In a preliminary clinical trial of an AcceleDent prototype with 14 patients, Kau and colleagues noted 2.1mm of tooth movement per month in the mandibular arch (twice the normally reported rate) and 3mm per month in the maxillary arch.22 In a more comprehensive randomized controlled trial of AcceleDent, Pavlin reported 2.71mm per month of initial maxillary dental alignment in 23 premolar-extraction patients--a 51% reduction in treatment time compared to the control group, with no adverse findings such as root resorption or pain.28 The differences in alignment speed may be attributed to the typically faster tooth movement in the maxillary arch; in addition, the extraction spaces likely facilitated more rapid resolution of irregularities, compared to the speed of mandibular alignment without extractions noted in the present study.
In contrast, Miles and colleagues found no significant difference in the initial dental alignment of 66 consecutively treated orthodontic patients, appointed every five weeks over a 2.5-month period, when half the patients were given a vibrating device (111Hz, .06N) to use for 20 minutes per day.29 As the investigators acknowledged, however, they used consecutive patients rather than a more homogeneous sample, and the vibrational forces were applied at a higher frequency and lower force level than in comparable studies. Moreover, data collection was invariably discontinued after 10 weeks of alignment with only an .014" thermal nickel titanium archwire in an .018" appliance, while data for the present study continued to be collected until leveling was completed. It has yet to be determined exactly how the force, frequency, and duration of vibration contribute to the rate of tooth movement.
Like Miles and colleagues,29 our study found no statistical significance in the rate of alignment with vibration compared to control samples. Nevertheless, we did find a significant increase in the speed of leveling, which could not have been accomplished without the cumulative reduction in alignment time resulting from the application of vibration.
Conclusion
In the present study, the amount of time required to achieve both dental alignment and leveling in Class II nonextraction treatment was reduced by using an AcceleDent device to apply vibration. Overall, we found a clinically beneficial and statistically significant 30% increase in the rate of tooth movement during orthodontic leveling of the mandibular dentition. Future research on the effects of vibration should focus on other aspects of orthodontic treatment, different biomechanics, pain reduction, gene expression, and tissue responses, along with testing of alternative force levels, frequencies, and durations of vibration.
ACKNOWLEDGMENTS: The author would like to thank Sheri Smith, President, Courante Oncology Clinical Research Services, Excelsior, MN, for her statistical analysis and OrthoAccel Technologies for their assistance with the AcceleDent units.
FOOTNOTES
- *Registered trademark of OrthoAccel Technologies, Bellaire, TX; www.acceledent.com.
- **AOA Orthodontic Appliances, Sturtevant, WI; www.aoalab.com.
- ***Trademark of American Orthodontics, Sheboygan, WI; www.americanortho.com.
- †SAS Institute, Cary, NC; www.sas.com.
REFERENCES
- 1. McNamara, J.A. Jr.; Hatch, N.; and Kapila, S.D.: Effective and Efficient Orthodontic Tooth Movement, Craniofacial Growth Series, vol. 48, Department of Orthodontics and Pediatric Dentistry, School of Dentistry and Center for Human Growth and Development, University of Michigan, Ann Arbor, 2011.
- 2. Liou, E.: Accelerated orthodontic tooth movement, in Evidence-Based Clinical Orthodontics, ed. P.G. Miles, D.J. Rinchuse, and D.J. Rinchuse, Quintessence Publishing, Chicago, 2012, pp. 179-199.
- 3. Uribe, F.; Padala, S.; Allareddy, V.; and Nanda, R.: Patients', parents', and orthodontists' perceptions of the need for and costs of additional procedures to reduce treatment time, Am. J. Orthod. 145(4 suppl):S65-73, 2014.
- 4. Shapiro, E.; Roeber, F.W.; and Klempner, L.S.: Orthodontic movement using pulsating force-induced piezoelectricity, Am. J. Orthod. 76:59-66, 1979.
- 5. Kurz, C.H.: Vibrational orthodontic appliance, U.S. Patent No. 4348178, Sept. 7, 1982.
- 6. Krishtab, S.I.; Doroshenko, S.I.; and Liutik, G.I.: Use of vibratory action on the teeth to accelerate orthodontic treatment, Stomatologiia (Mosk.) 65:61-63, 1986.
- 7. Kopher, R.A. and Mao, J.J.: Suture growth modulated by the oscillatory component of micromechanical strain, J. Bone Miner. Res. 18:521-528, 2003.
- 8. Peptan, A.L.; Lopez, A.; Kopher, R.A.; and Mao, J.J.: Responses of intramembranous bone and sutures upon in vivo cyclic tensile and compressive loading, Bone 42:432-438, 2008.
- 9. Darendeliler, M.A.; Zea, A.; Shen, G.; and Zoellner, H.: Effects of pulsed electromagnetic field vibration on tooth movement induced by magnetic and mechanical forces: A preliminary study, Austral. Dent. J. 52:282-287, 2007.
- 10. Nishimura, M.; Chiba, M.; Ohashi, T.; Sato, M.; Shimizu, Y.; Igarashi, K.; and Mitani, H.: Periodontal tissue activation by vibration: Intermittent stimulation by resonance vibration accelerates experimental tooth movement in rats, Am. J. Orthod. 133:572-583, 2008.
- 11. Kalajzic, Z.; Peluso, E.B.; Utreja, A.; Dyment, N.; Nihara, J.; Xu, M.; Chen, J.; Uribe, F.; and Wadhwa, S.: Effect of cyclical forces on the periodontal ligament and alveolar bone remodeling during orthodontic tooth movement, Angle Orthod. 84:297-303, 2014.
- 12. Liu, D.: Acceleration of orthodontic tooth movement by mechanical vibration, AADR General Session, Washington, DC, March 2010.
- 13. Alikhani, M.; Khoo, E.; Alyami, B.; Raptis, M.; Salgueiro, M.; Oliveira, S.M.; Boskey, A.; and Teixeria, C.C.: Osteogenic effect of high-frequency acceleration on alveolar bone, J. Dent. Res. 91:413-419, 2012.
- 14. Liu, D.: Histomorphometric study of orthodontic tooth movement under mechanical vibration, AADR General Session, San Diego, March 2011.
- 15. Braun, S.; Bluestein, M.; Moore, B.K.; and Benson, G.: Friction in perspective, Am. J. Orthod. 115:619-627, 1999.
- 16. Olson, J.E.; Liu, Y.; Nickel, J.C.; Walker, M.P.; and Iwasaki, L.R.: Archwire vibration and stick-slip behavior at the bracketarchwire interface, Am. J. Orthod. 142:314-322, 2012.
- 17. Pandis, N.; Polychronopoulou, A.; and Eliades, T.: Active or passive self-ligating brackets? A randomized controlled trial of comparative efficiency in resolving maxillary anterior crowding in adolescents, Am. J. Orthod. 137:12.e1-6, 2010.
- 18. Fleming, P.S. and Johal, A.: Self-ligating brackets in orthodontics: A systematic review, Angle Orthod. 80:575-584, 2010.
- 19. Songra, G.; Clover, M.; Atack, N.E.; Ewings, P.; Sherrif, M.; Sandy, J.R.; and Ireland, A.J.: Comparative assessment of alignment efficiency and space closure of active and passive self-ligating vs conventional appliances in adolescents: A single-center randomized controlled trial, Am. J. Orthod. 145:569-578, 2014.
- 20. Bowman, S.J.: Class II combination therapy: Molar distalization and fixed functionals, in Current Therapy in Orthodontics, ed. R. Nanda and S. Kapila, Mosby Elsevier, St. Louis, 2009, pp. 115-136.
- 21. Bowman, S.J. and Carano, A.: Butterfly bracket system, J. Clin. Orthod. 38:274-287, 2004.
- 22. Kau, C.H.; Nguyen, J.T.; and English, J.D.: The clinical evaluation of a novel cyclical force generating device in orthodontics, Orthod. Practice 1:43-44, 2010.
- 23. Mandall, N.A.; Lowe, C.; Worthington, H.; Sandler, J.; Derwent, S.; Abdi-Oskouei, M.; and Ward, S.: Which orthodontic archwire sequence? A randomized clinical trial, Eur. J. Orthod. 28:561-566, 2006.
- 24. od. 28:561-566, 2006. 24. Flores-Mir, C.: Attaining a working archwire--which sequence? Evid. Based Dent. 8:48, 2007.
- 25. Ong, E.; Ho, C.; and Miles, P.: Alignment efficiency and discomfort of three orthodontic archwire sequences: A randomized clinical trial, J. Orthod. 38:32-39, 2001.
- 26. Jian, F.; Lai, W.; Furness, S.; McIntyre, G.T.; Millett, D.T.; Hickman, J.; and Wang, J.: Initial arch wires for tooth alignment during orthodontic treatment with fixed appliances, Cochran Database Syst. Rev. 4:CD007859, 2013.
- 27. Johnston, L.E. Jr.: Moving forward by looking back: "Retrospective" clinical studies, J. Orthod. 29:221-226, 2002.
- 28. Pavlin, D.: Modulation of tooth movement by vibratory forces, 41st Annual Moyers Symposium, University of Michigan, Ann Arbor, March 9, 2014.
- 29. Miles, P.; Smith, H.; Weyant, R.; and Rinchuse, D.J.: The effects of a vibrational appliance on tooth movement and patient discomfort: A prospective randomized clinical trial, Austral. Orthod. J. 28:213-218, 2012.
-
 DR. BOWMAN
DR. BOWMAN
Dr. Bowman is a Contributing Editor of the Journal of Clinical Orthodontics; an Adjunct Associate Professor, St. Louis University, St. Louis; a straight-wire instructor, University of Michigan, Ann Arbor, MI; an Assistant Clinical Professor, Case Western Reserve University, Cleveland; a Visiting Clinical Lecturer, Seton Hill University, Greensburg, PA; and in the private practice of orthodontics at 1314 W. Milham Ave., Portage, MI 49024; e-mail: drjwyred@aol.com.