2008 JCO Study of Orthodontic Diagnosis and Treatment Procedures, Part 3: More Breakdowns of Selected Variables
Our three-part series of articles on the 2008 JCO Study of Orthodontic Diagnosis and Treatment Procedures concludes this month with more breakdowns of the most important diagnostic and treatment techniques by number of years in practice, geographic region, and gross income level. A description of the survey methodology can be found in the first article (JCO, November 2008), which also covered the basic results and trends in orthodontics since the first Study in 1986. The second article (JCO, December 2008) contains the remainder of selected breakdowns.
Removable and Functional Appliances
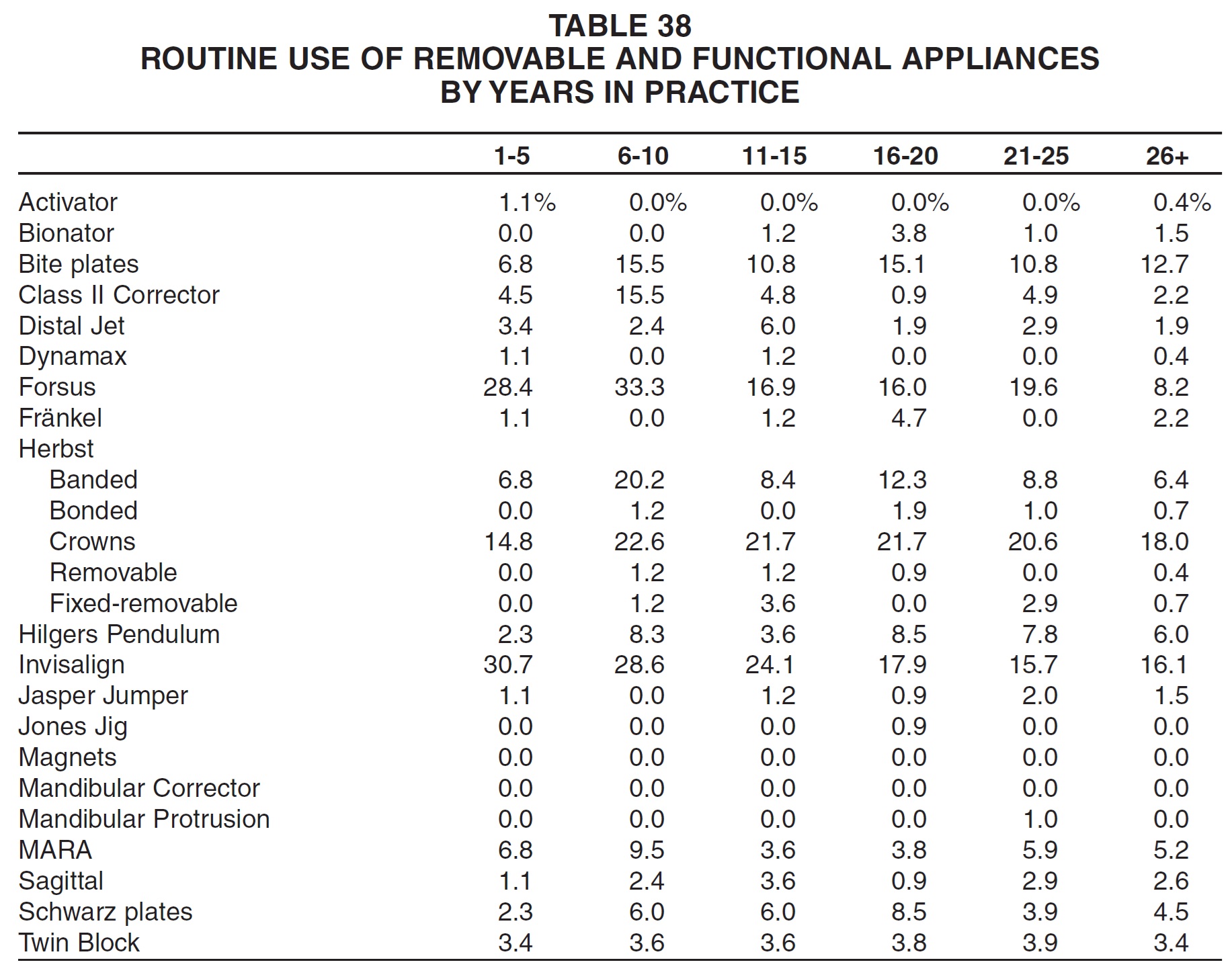
There was little apparent relationship between number of years in practice and routine use of removable and functional appliances (Table 38). Newer practices were more likely than older practices, however, to use the Forsus appliance and Invisalign.
Similar articles from the archive:
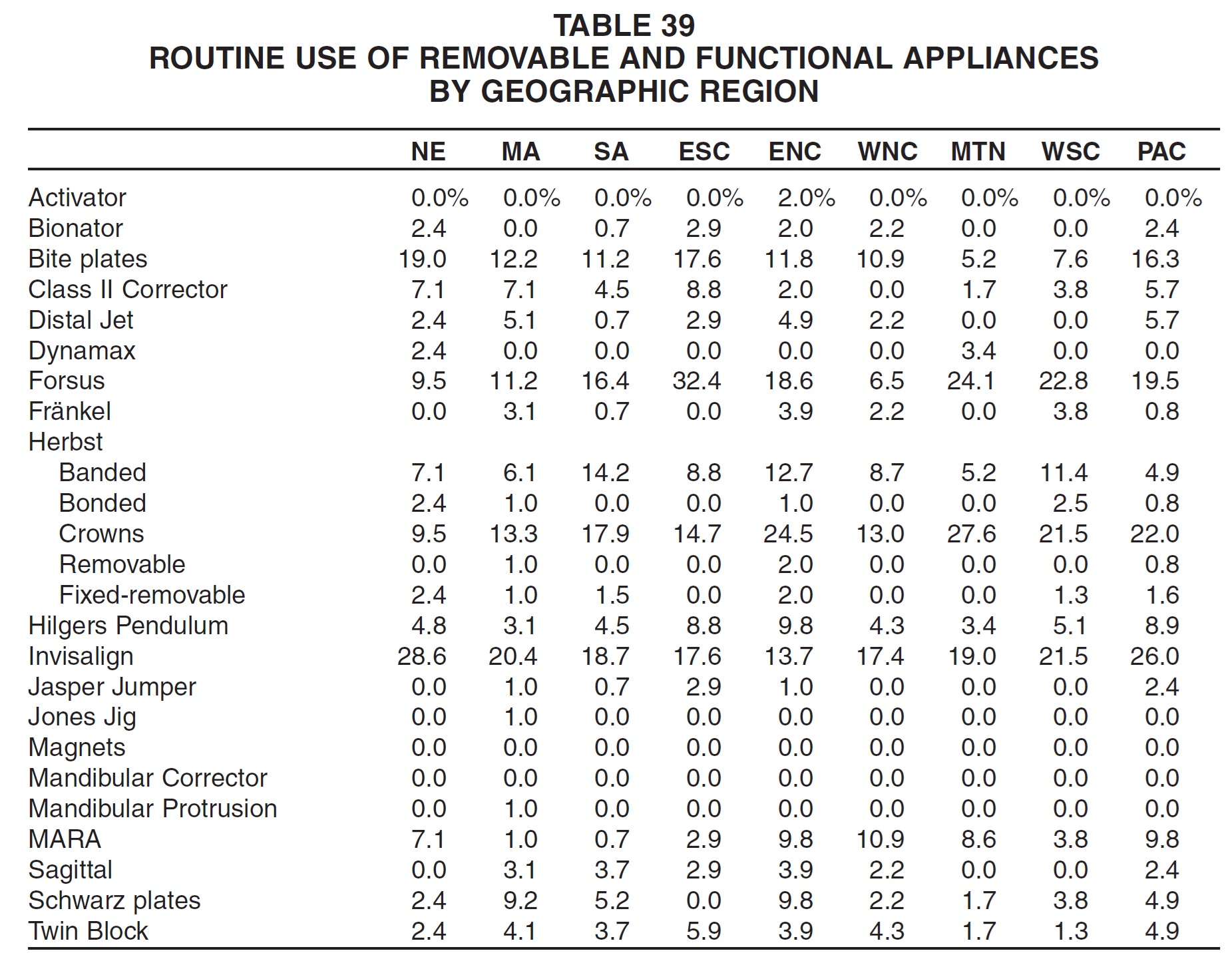
When respondents were broken down by region, the most routine users of bite plates, fixed-removable Herbst appliances, and Invisalign systems were in New England; of the banded Herbst, in the South Atlantic region; of the Jones Jig and Mandibular Protrusion Appliance, in the Middle Atlantic region; of the bionator, Class II Corrector, Forsus appliance, Jasper Jumper, and Twin Block, in the East South Central region; of the activator, Frankel, removable Herbst, Hilgers Pendulum, and sagittal appliances and Schwarz plates, in the East North Central region; of the MARA system, in the West North Central region; of the Dynamax and Herbst with crowns, in the Mountain region; of the bonded Herbst, in the West South Central region; and of the Distal Jet, in the Pacific region (Table 39).
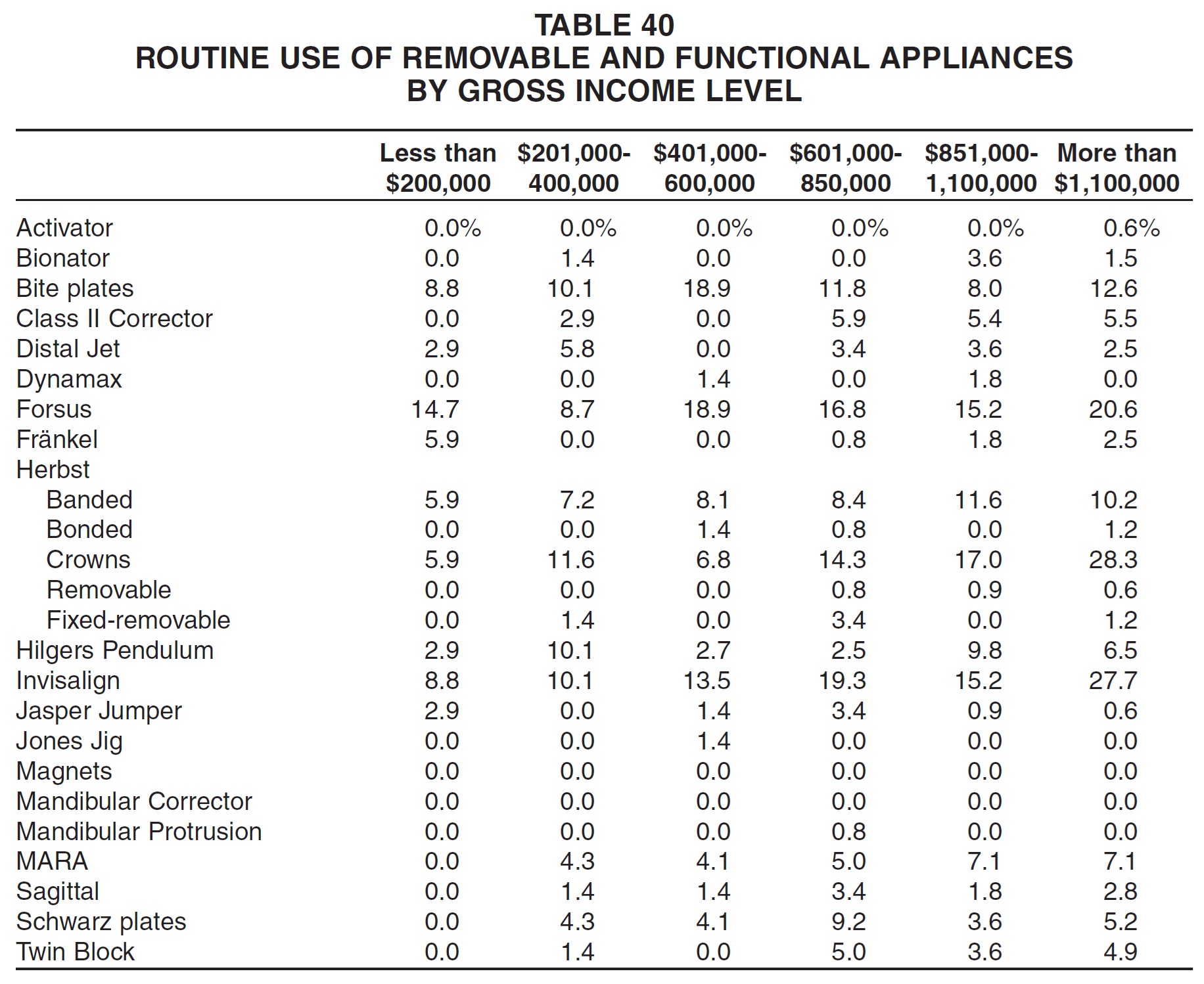
As in past surveys, routine use of removable and functional appliances tended to increase with gross income (Table 40). This pattern was especially noticeable for the Herbst with crowns, Invisalign, and MARA.
Headgear
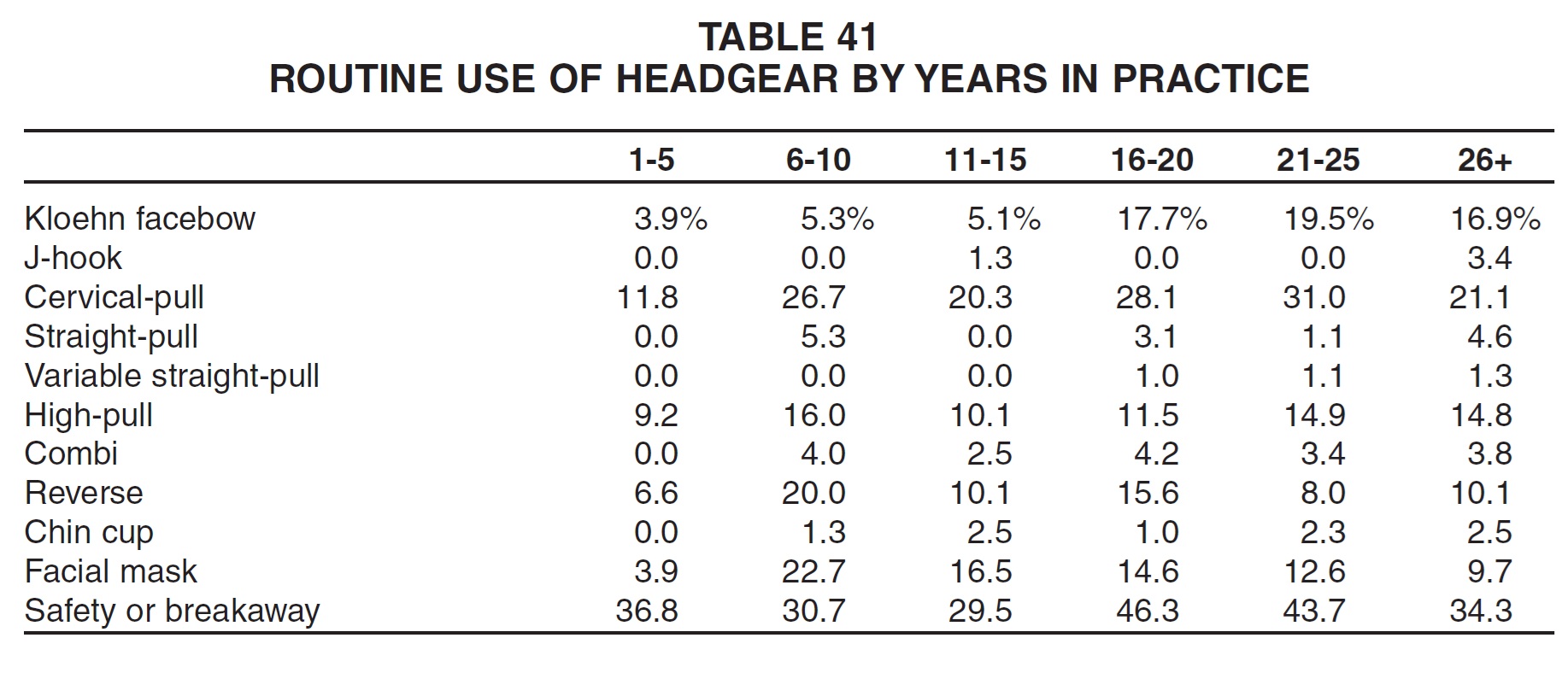
The types of headgear used for Class II treatment were prescribed more routinely by orthodontists who had been in practice longer (Table 41). On the other hand, Class III devices such as reverse headgear and facial masks were more popular in newer practices.
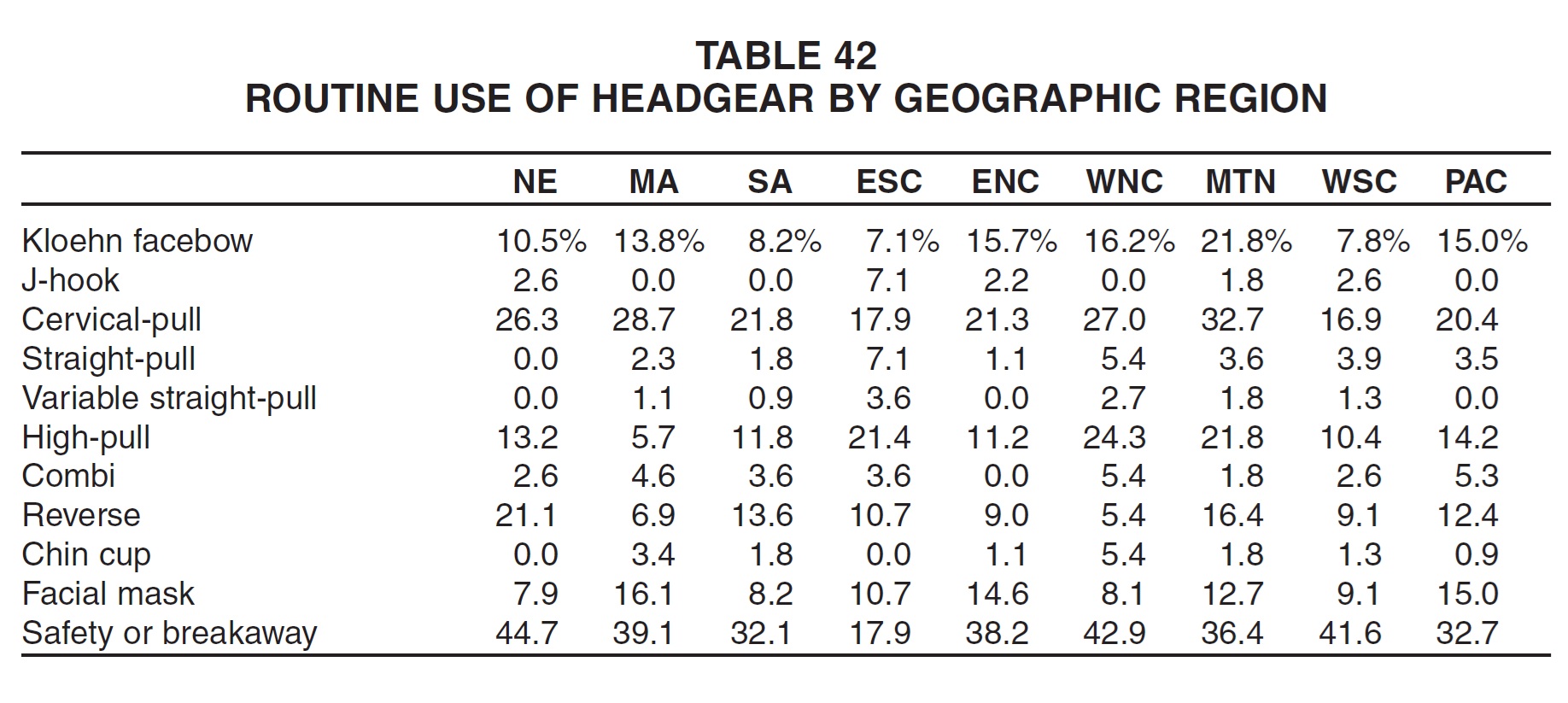
Kloehn facebows and cervical-pull headgear were used most routinely in the Mountain region, while J-hook, straight-pull, and variable straight-pull devices were used most commonly by East South Central orthodontists (Table 42). High-pull and combi headgear and chin cups were used most routinely in the West North Central region, reverse headgear in New England, and facial masks in the Middle Atlantic region. Safety or breakaway devices were most frequently employed by New England orthodontists and least frequently by East South Central respondents.
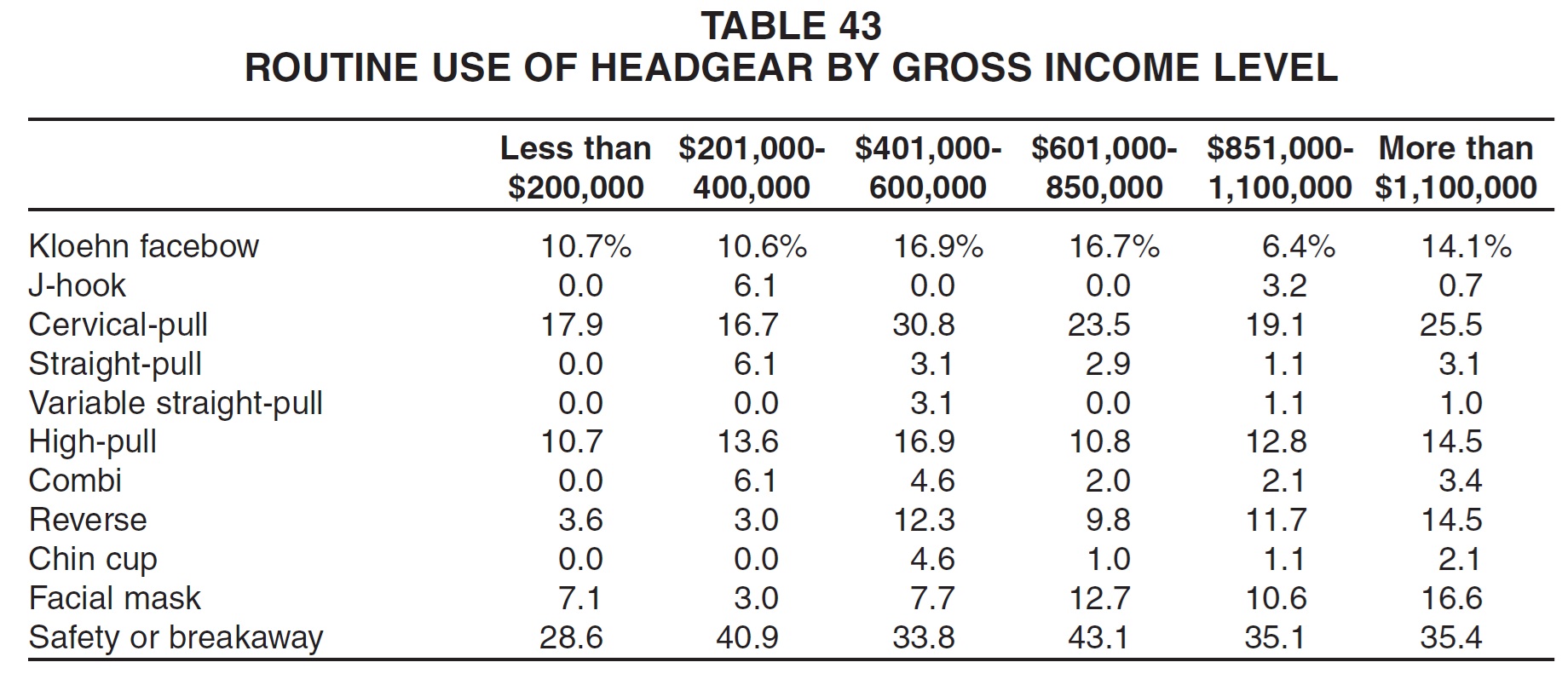
In general, Class II headgears and safety or breakaway devices were used more routinely by middle-income practices, and Class III appliances by high-income practices (Table 43).
Finishing Procedures
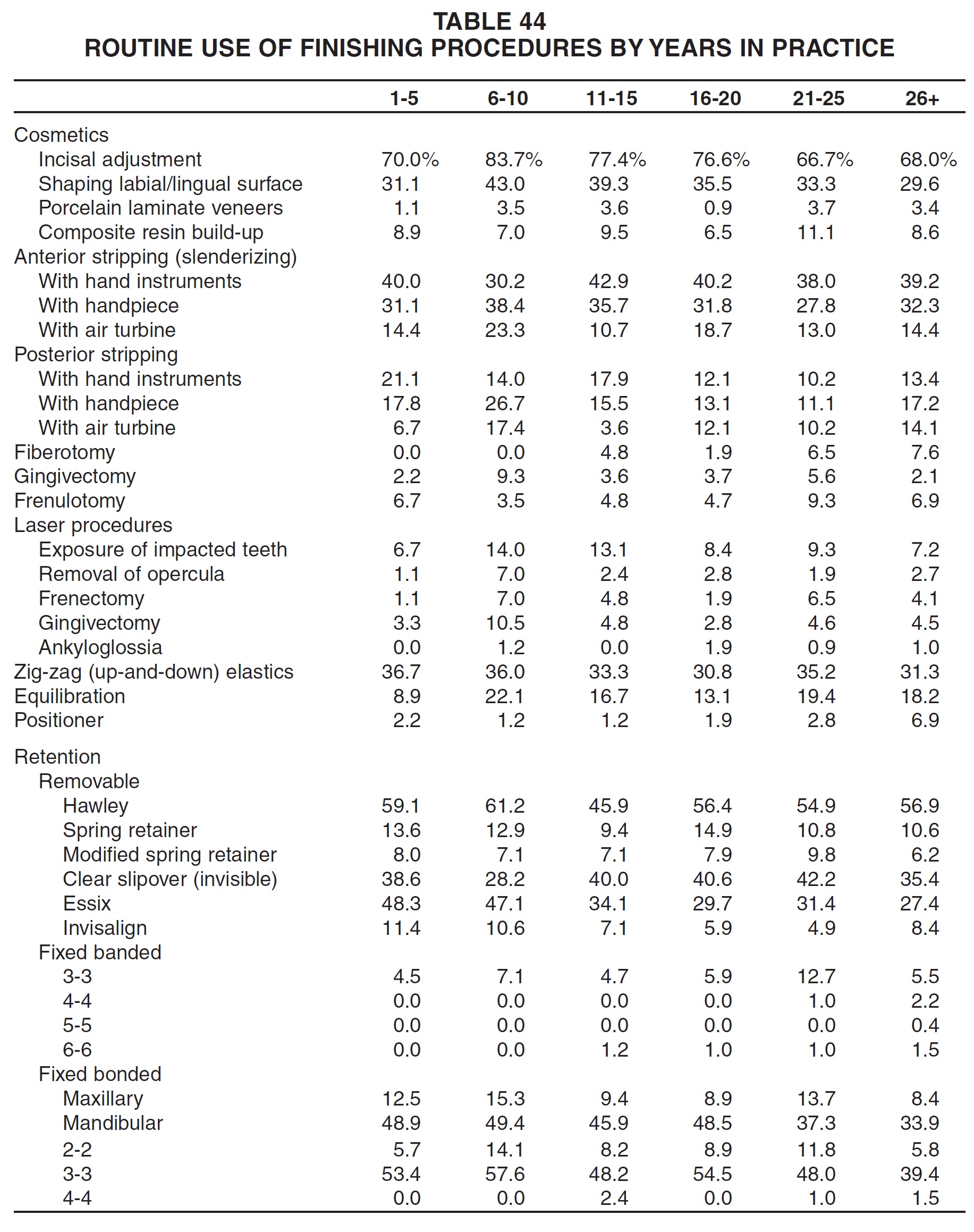
There was no obvious correlation between number of years in practice and the use of cosmetic finishing procedures (Table 44). Younger practices were slightly more likely than older practices to use hand instruments for stripping, compared to power instruments. Middle-age practices were the most routine users of laser procedures, but none of these was used by more than 14% of any group. The oldest practices were somewhat more likely than others to routinely prescribe fiberotomies and positioners. Hawley and spring retainers were used almost equally across the board, but Essix and Invisalign retainers and fixed bonded retainers were used more routinely by younger practitioners.
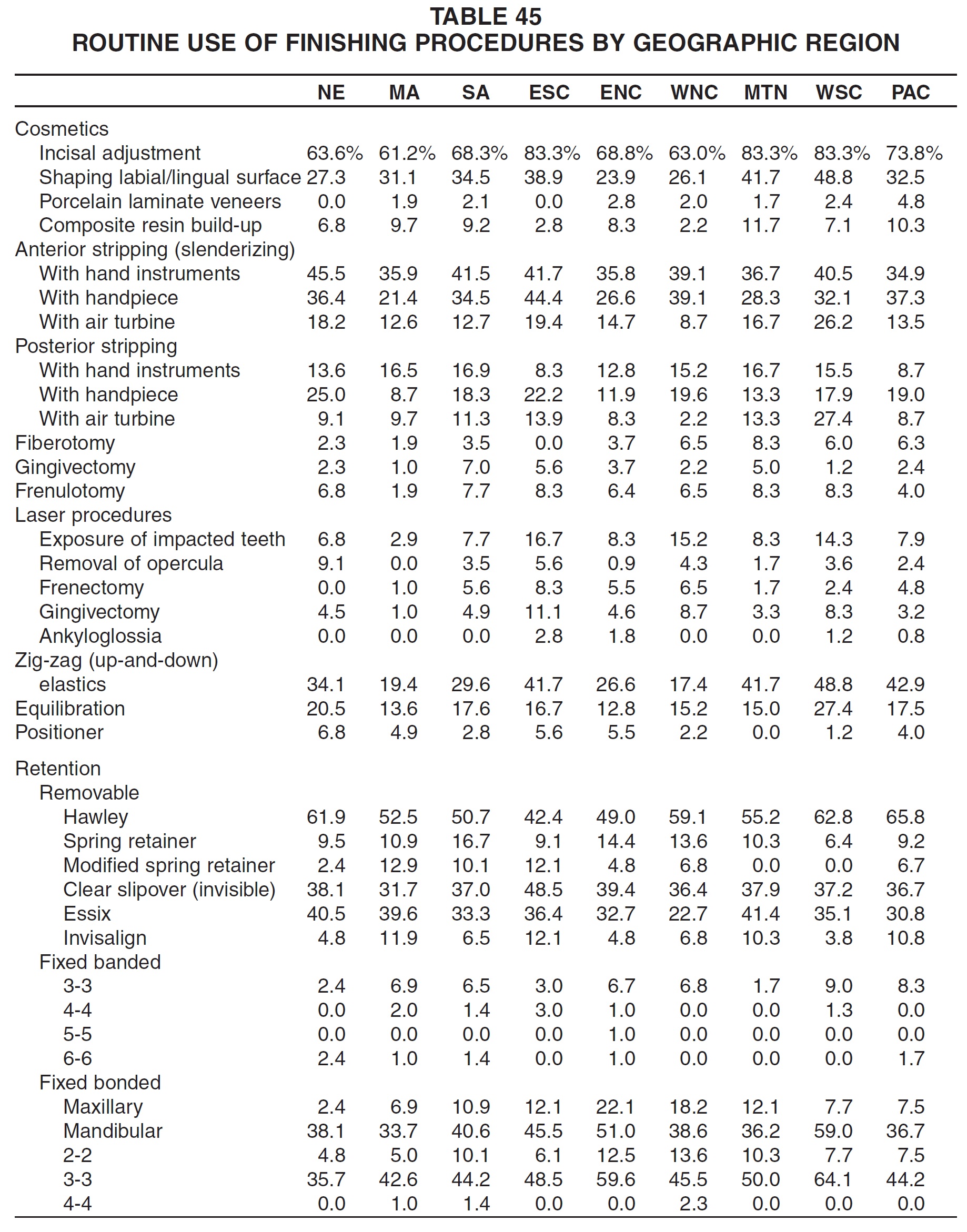
The most routine use of cosmetic procedures appeared to be in the West South Central and Mountain regions (Table 45). No geographic pattern emerged among other finishing techniques, except that laser procedures were most commonly used in the East South Central region, and zig-zag elastics and equilibration in the West South Central region. Hawley retainers were used most routinely in the Pacific region; spring retainers in the South Atlantic region; modified spring retainers in the Middle Atlantic region; clear slipover and Invisalign retainers in the East South Central region; and Essix retainers in the Mountain region. Fixed bonded retainers seemed to be most popular among West South Central orthodontists.
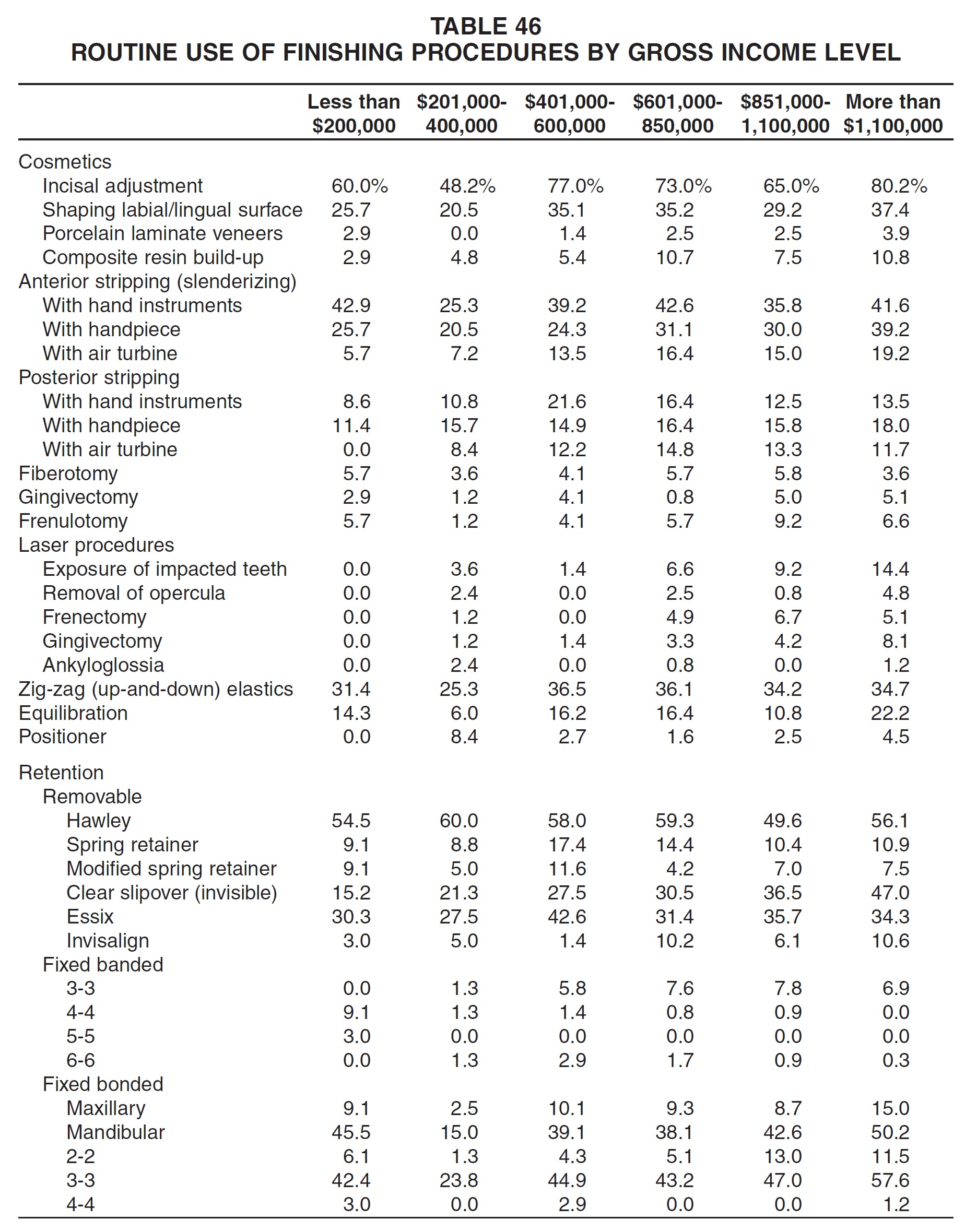
Routine use of finishing procedures tended to increase with gross income, but not as sharply as in past surveys (Table 46). Practices with the highest income were also the most likely to use clear slipover, Invisalign, and fixed bonded retainers.
Invisalign
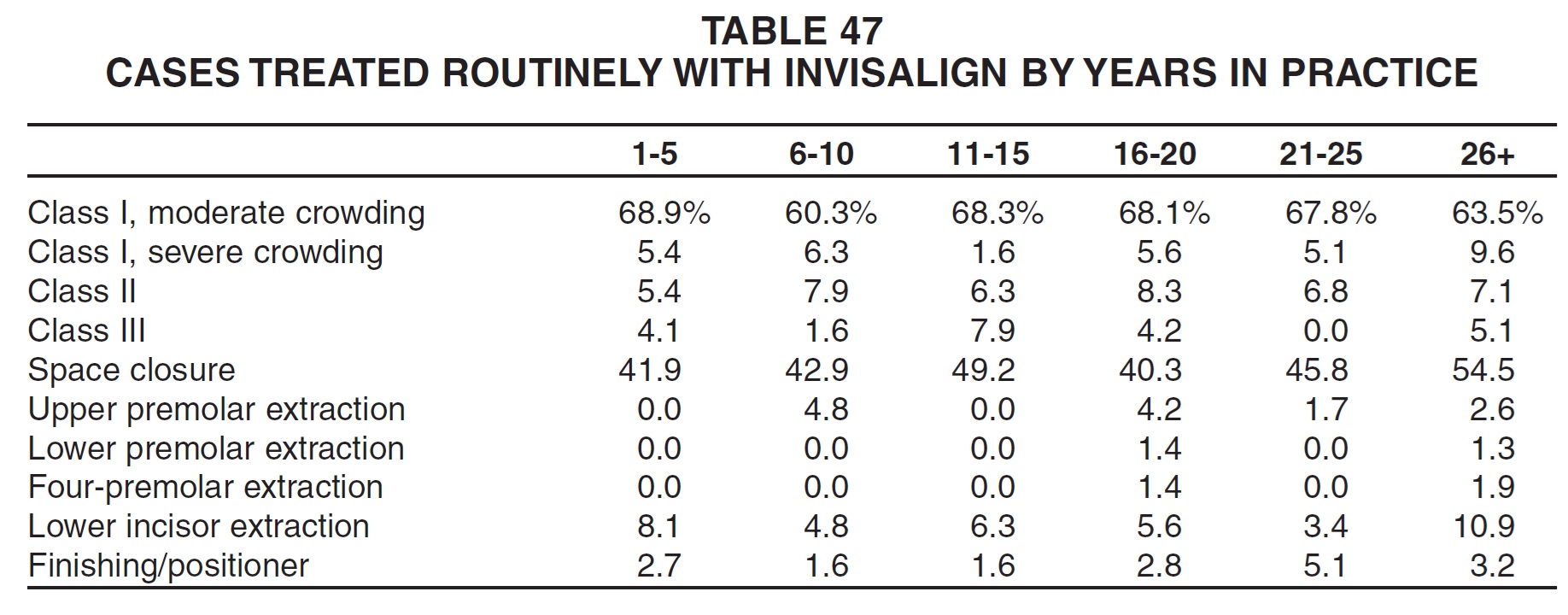
Respondents who had been in practice the longest treated space-closure and Class I cases with severe crowding more routinely with the Invisalign system than other respondents did (Table 47). Otherwise, there was not much difference in the types of cases treated with Invisalign by years in practice. (Tables on Invisalign and skeletal anchorage include only respondents who reported treating at least one case.)
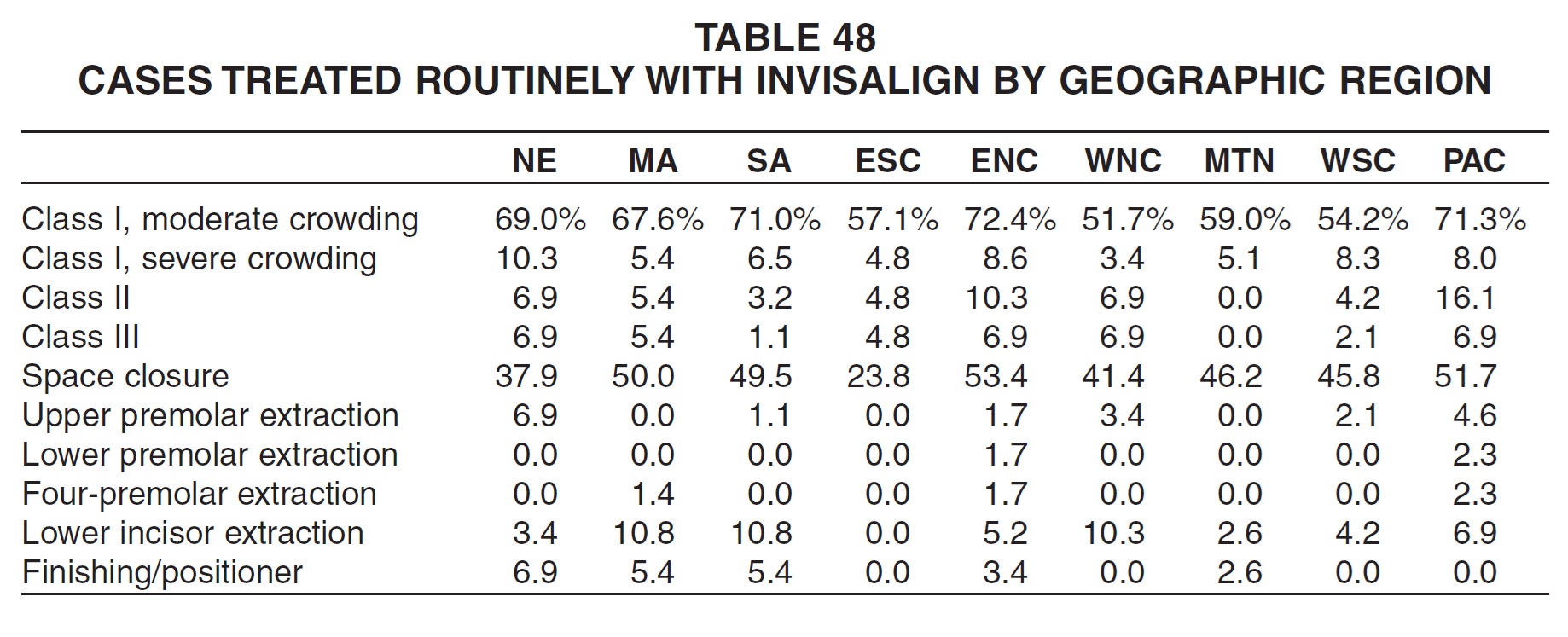
Orthodontists in the East North Central region used Invisalign most routinely for treatment of moderate Class I and space-closure cases (Table 48). New England respondents were the most routine users for severely crowded Class I patients, upper-premolar-extraction patients, and finishing. Pacific orthodontists used Invisalign most routinely for Class II and III and other premolar-extraction cases, although the differences among regions in treatment of Class III and extraction patients were not substantial.
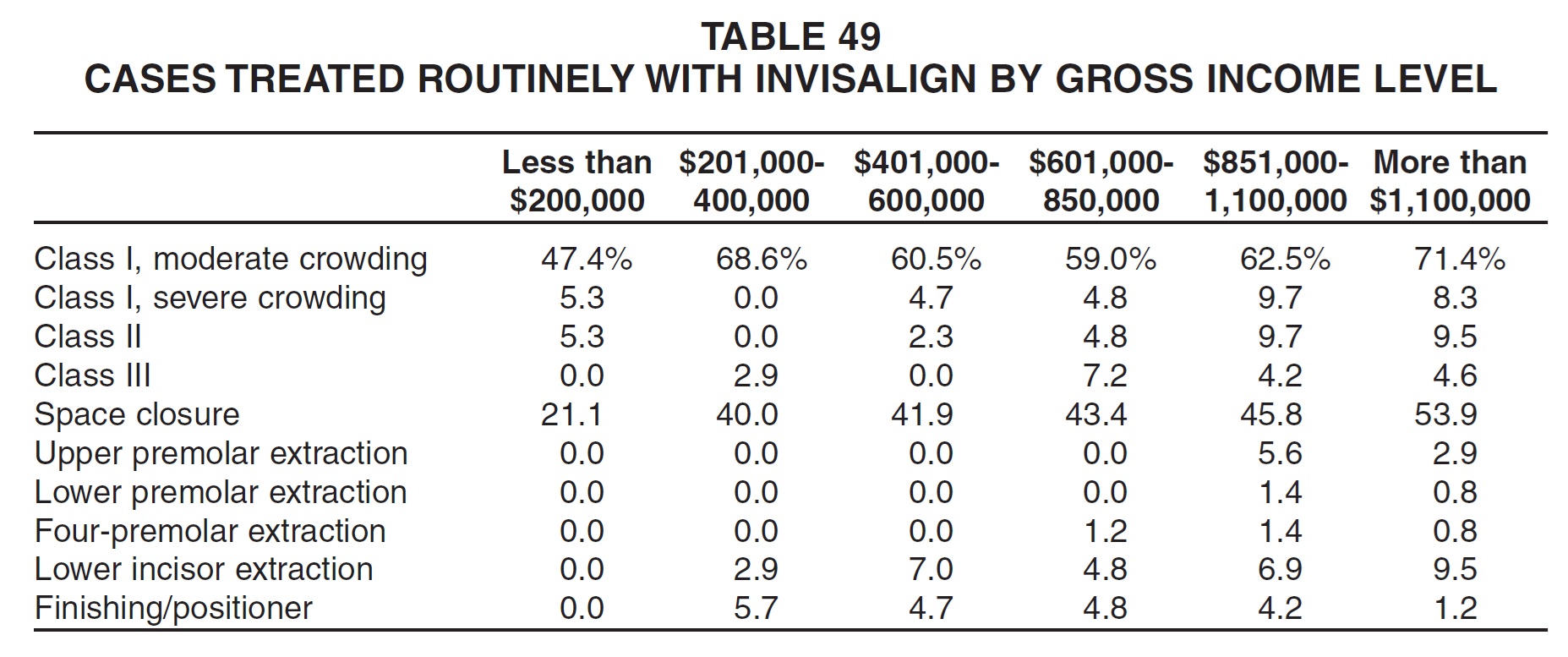
Routine Invisalign usage generally increased with gross income for every type of treatment surveyed (Table 49). Still, only Class I cases with moderate crowding and space-closure cases were treated routinely by as many as 10% of the respondents in any group.
Skeletal Anchorage
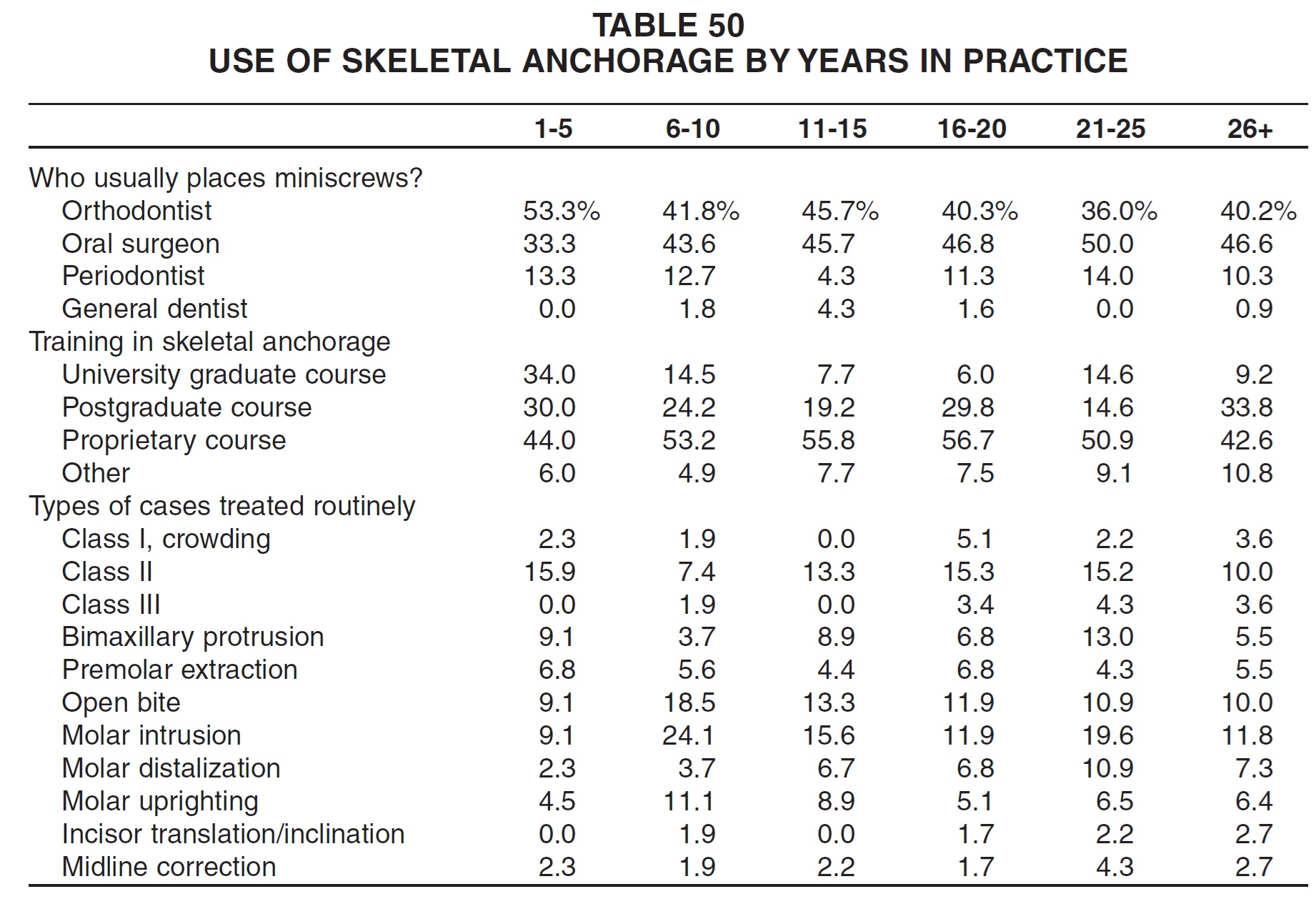
Orthodontists who had been in practice for less than six years were clearly more comfortable than others in placing miniscrews themselves, and they had also received more of their training in university graduate and postgraduate programs (Table 50). Nevertheless, only Class II cases were treated more routinely with skeletal anchorage by this group than by any other age group.
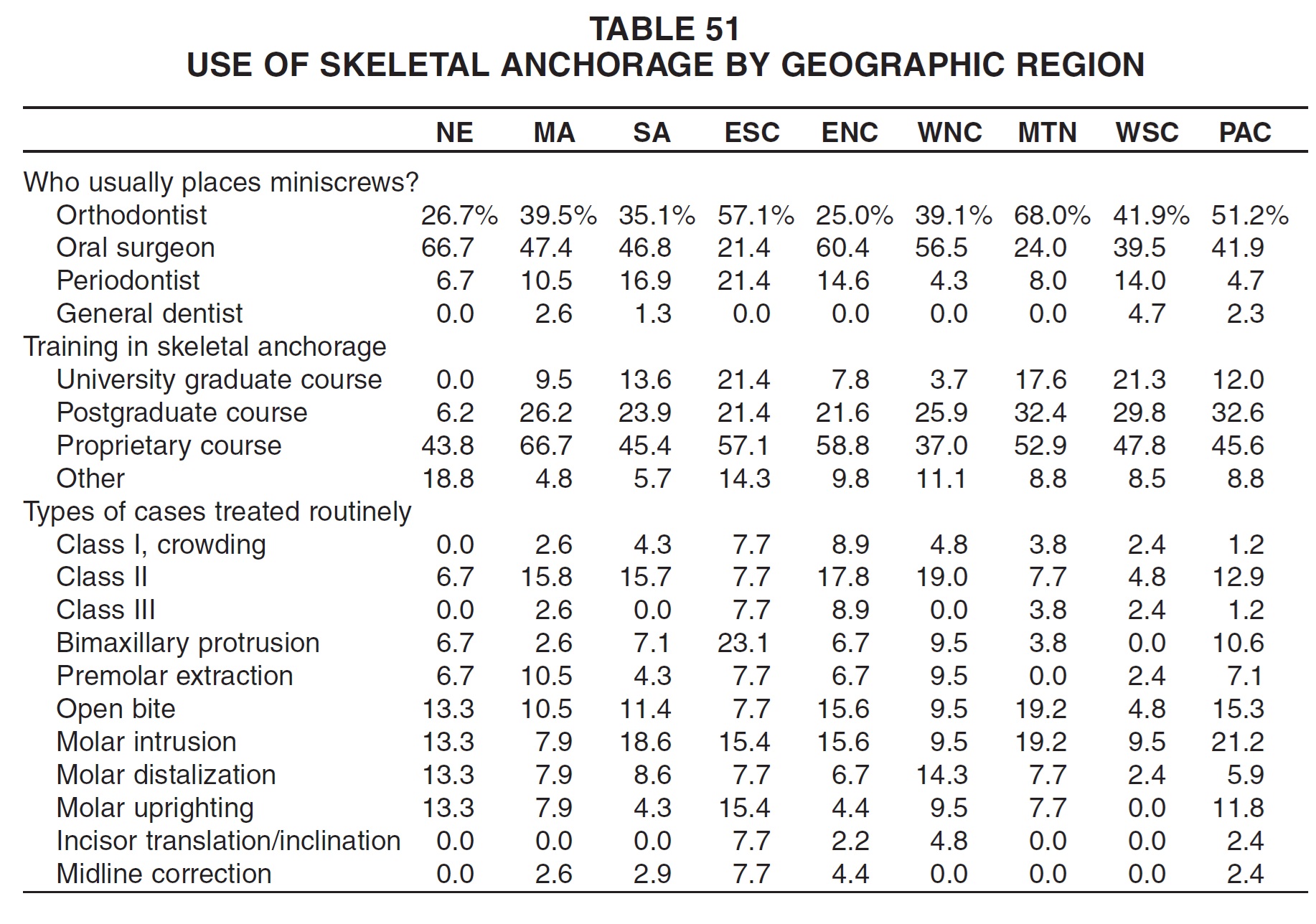
There were marked regional differences in the use of temporary anchorage devices (Table 51). New England orthodontists were the most likely to refer placement of miniscrews to oral surgeons, and they also reported the least university training. Mountain and West South Central orthodontists appeared to have received the most training in graduate and postgraduate courses, while two-thirds of all Middle Atlantic orthodontists who used skeletal anchorage had been trained in proprietary courses. The most routine miniscrew users were in the East North Central region for Class I and III treatment; in the West North Central region for Class II and molar-distalization cases; in the East South Central region for bimaxillary-protrusion treatment, molar uprighting, incisor translation and inclination, and midline correction; in the Middle Atlantic region for premolar-extraction cases; and in the Mountain region for open-bite and molar-intrusion treatment.
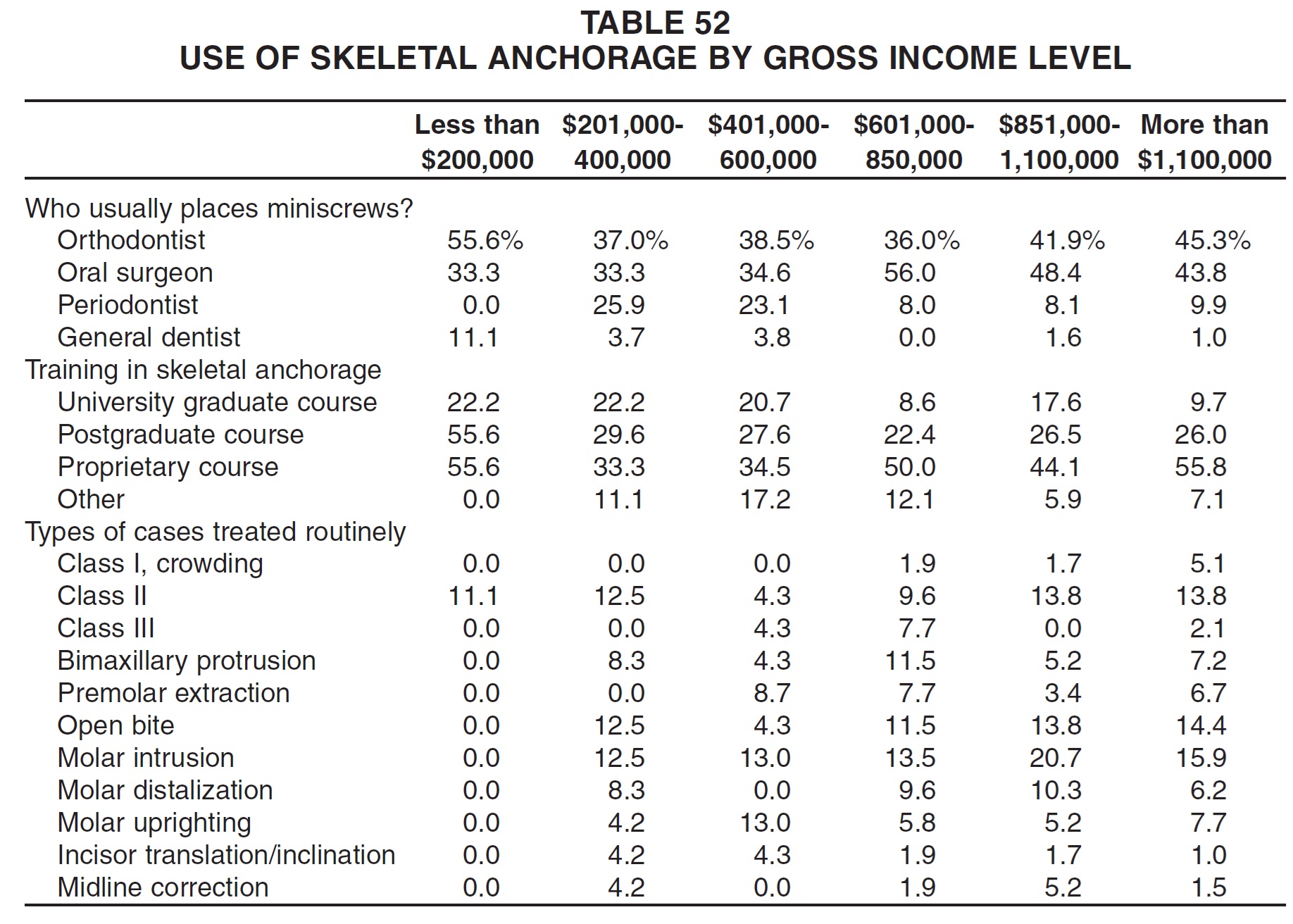
Practices with the lowest income were most likely to place miniscrews themselves and to have had graduate or postgraduate training, which probably reflects the preponderance of younger orthodontists in this category (Table 52). As in Table 50, however, the low-income practices tended not to use skeletal anchorage on a routine basis.
Conclusion
Results of the 2008 JCO Study of Orthodontic Diagnosis and Treatment Procedures demonstrate the continuation of several trends noted in the four previous surveys:
- Fewer routine diagnostic records are being taken.
- The use of esthetic brackets and titanium-alloy archwires is increasing compared to stainless steel materials.
- Banding has been almost completely replaced by bonding, increasingly using indirect techniques; light-cured adhesives are gradually replacing chemical composites.
- Fixed functional appliances are gaining popularity compared to removable appliances, and routine headgear use (except for reverse headgear) is declining.
- Extractions are becoming almost rare in orthodontic treatment.
- Cosmetic finishing procedures are becoming fairly routine.
- Clear, removable retention appliances are gaining over Hawley and spring-type retainers, but bonded retainer wires are now almost standard in the mandibular arch.
- Routine TMJ treatment is not being performed by many orthodontists.
Significant new developments in technology, materials, and treatment methods are also apparent since the last Study in 2002:
- Digital imaging and computerized analysis are continuing a rapid growth.
- Self-ligating brackets have shown a dramatic increase compared to standard edgewise systems.
- Most orthodontists now feel they need to offer Invisalign treatment to their adult patients.
- Skeletal anchorage is also becoming a basic tool in the orthodontic armamentarium, especially as university curricula develop and new graduates open their practices.
-
 DR. KEIM
DR. KEIM -
 DR. GOTTLIEB
DR. GOTTLIEB -
 DR. NELSON
DR. NELSON -
 MR. VOGELS
MR. VOGELS
Dr. Keim is Editor, Dr. Gottlieb is Senior Editor, and Mr. Vogels is Managing Editor of the Journal of Clinical Orthodontics, 1828 Pearl St., Boulder, CO 80302. Dr. Nelson is Director and Research Consultant, Nelson Associates, Nederland, CO.