2008 JCO Study of Orthodontic Diagnosis and Treatment Procedures, Part 1: Results and Trends
This is the first installment in a series of re-ports on the fifth JCO Study of Orthodontic Diagnosis and Treatment Procedures, a nationwide survey of clinical techniques and diagnostic methods. Previous studies were conducted in 1986, 1990, 1996, and 2002.
This month, we will compare the results of the current survey to those of past studies, highlighting trends in orthodontic treatment. Articles in the next two issues of JCO will break down the data from the 2008 Study into various categories.
This is the first installment in a series of re-ports on the fifth JCO Study of Orthodontic Diagnosis and Treatment Procedures, a nationwide survey of clinical techniques and diagnostic methods. Previous studies were conducted in 1986, 1990, 1996, and 2002. This month, we will compare the results of the current survey to those of past studies, highlighting trends in orthodontic treatment. Articles in the next two issues of JCO will break down the data from the 2008 Study into various categories.
Methodology
The 2002 Study questionnaire was revised to reflect responses to that survey, as well as recommendations from JCO editors and leaders of the orthodontic industry, with an emphasis on new technologies that have developed over the past six years. In an attempt to reach all the specialty orthodontic practitioners in the United States, we mailed 10,523 questionnaires during the first week of June 2008. A total of 808 forms were returned, for a response rate of 7.7%. This number of responses, along with the consistency of answers and demographic information across the 22 years of JCO treatment studies, tends to validate the results.
Similar articles from the archive:
- 2002 JCO Study of Orthodontic Diagnosis and Treatment Procedures, Part 1: Results and Trends October 2002
- 1996 JCO Study of Orthodontic Diagnosis and Treatment Procedures, Part 1: Results and Trends November 1996
- 1990 JCO Study of Orthodontic Diagnosis and Treatment Procedures, Part 1: Results and Trends March 1991
Data from the questionnaires were entered on computer by an independent company and analyzed with the Statistical Package for the Social Sciences. Individual responses that were obviously erroneous or outside the range of possibility were excluded from calculations of those specific tables.
The median (the middle number when all responses are ranked from highest to lowest) is often used in this Study rather than the mean (the arithmetical average), because medians are less affected by extremely high or low responses. Means are reported when necessary, such as for breaking down responses by category.
A notation of "NA" in a table indicates that the item was not included in the questionnaire for that Study. Results from 1990 or 1996 are sometimes omitted from this article for purposes of clarity; in most cases, these figures did not differ substantially from those of 1986 or 2002. For many questions, clinicians indicated whether they used a technique or appliance "occasionally" or "routinely"; for ease of comparison among the various surveys, the "occasionally" responses have been omitted from these tables.
Demographics
As has been found in the biennial JCO Orthodontic Practice Studies, this survey reflected an aging of the specialty and an increase in the percentage of female orthodontists over the past six years (Table 1).The median number of active cases and the percentage of adult patients remained the same as in 2002, but gross income continued to increase, to the point that nearly half of all respondents were over the $1 million mark. For the first time, the percentage of two-phase patients dropped off, to only 12%.
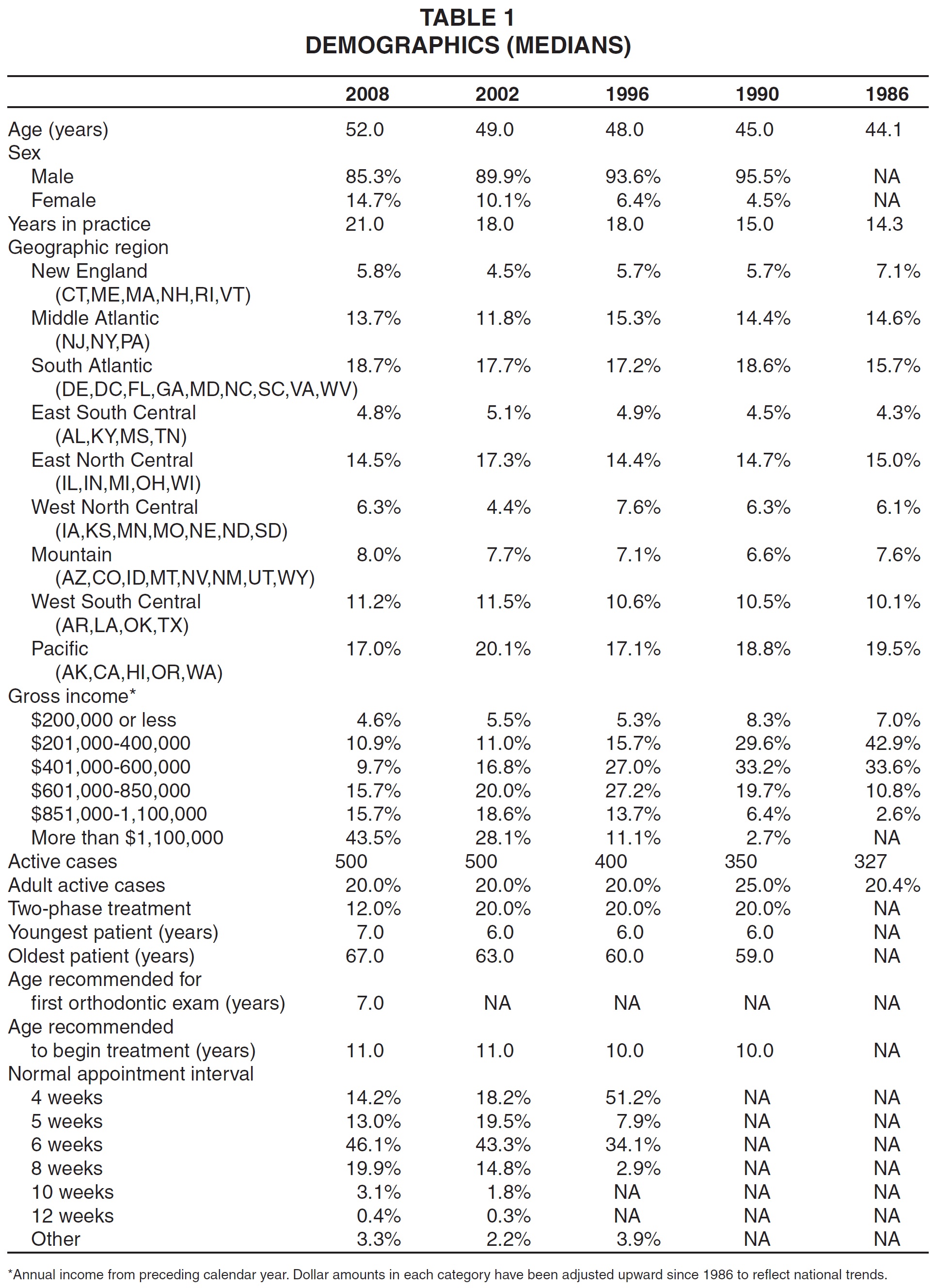
The median age of the youngest patient increased slightly to 7, while the median age of the oldest patient continued to rise. A gradual trend toward lengthening the average interval between appointments also continued.
Diagnostic Records
The most noteworthy finding of the current Study was the rapid growth in routine usage of digital records (Table 2). Digital cameras, which were not even listed on the questionnaire as recently as 1996, were now used almost exclusively. Digital radiographs and models continued to gain in popularity compared to their analog counterparts.
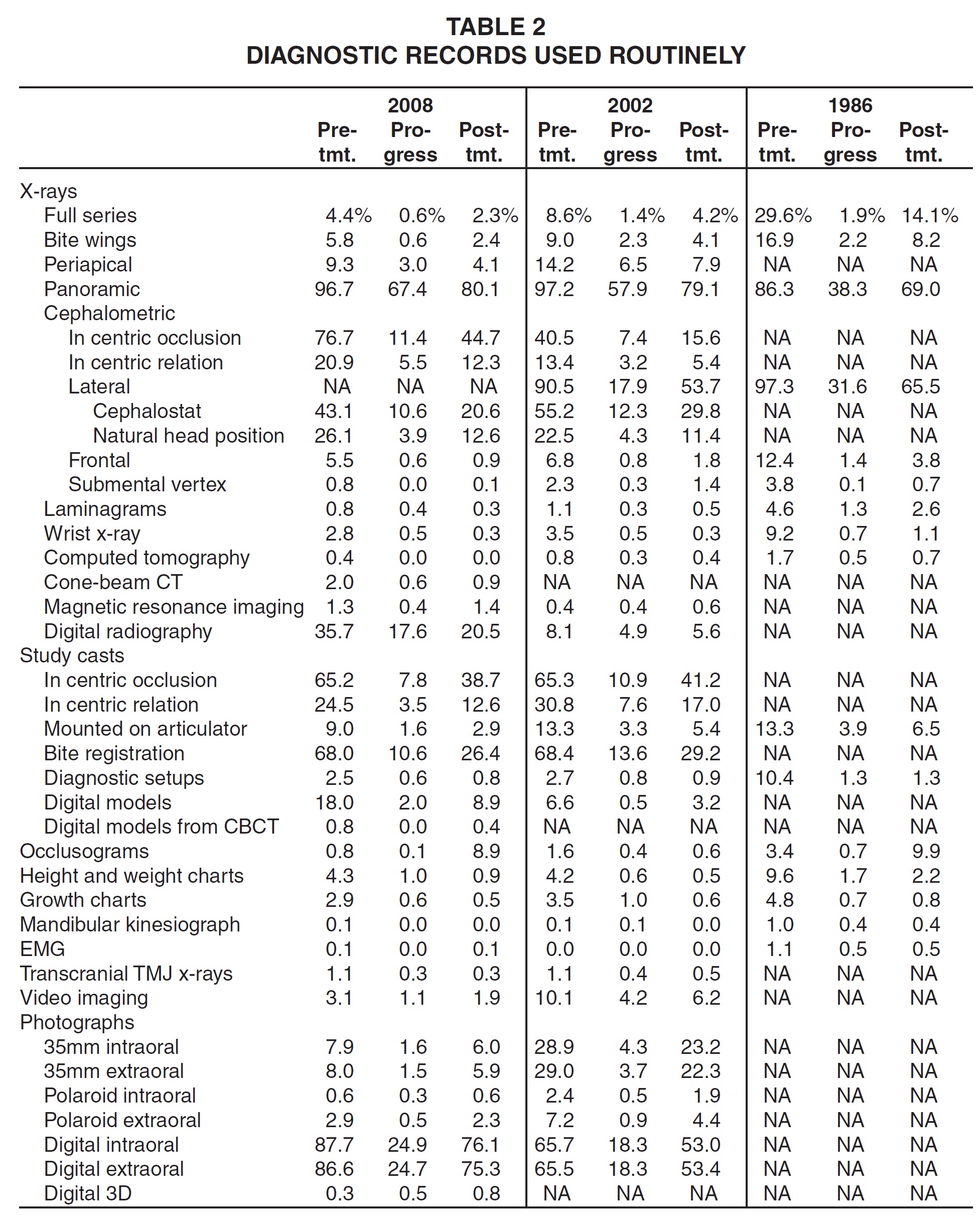
Panoramic x-rays were the only records taken by virtually all respondents before treatment and by a majority of respondents during and after treatment, although pretreatment study models in some form still seemed to be nearly universal. Most of the clinicians preferred to take their records in centric occlusion rather than in centric relation. Routine use of articulators and diagnostic setups continued a gradual decline.
The use of computerized cephalometric tracings or analyses also increased dramatically since the last survey, but the overall percentage of respondents who routinely performed cephalometric analyses decreased (Table 3). The most commonly used analyses remained the Steiner, Ricketts, Tweed, Downs, and McNamara, in that order--the same top five as in the first Treatment Study in 1986.
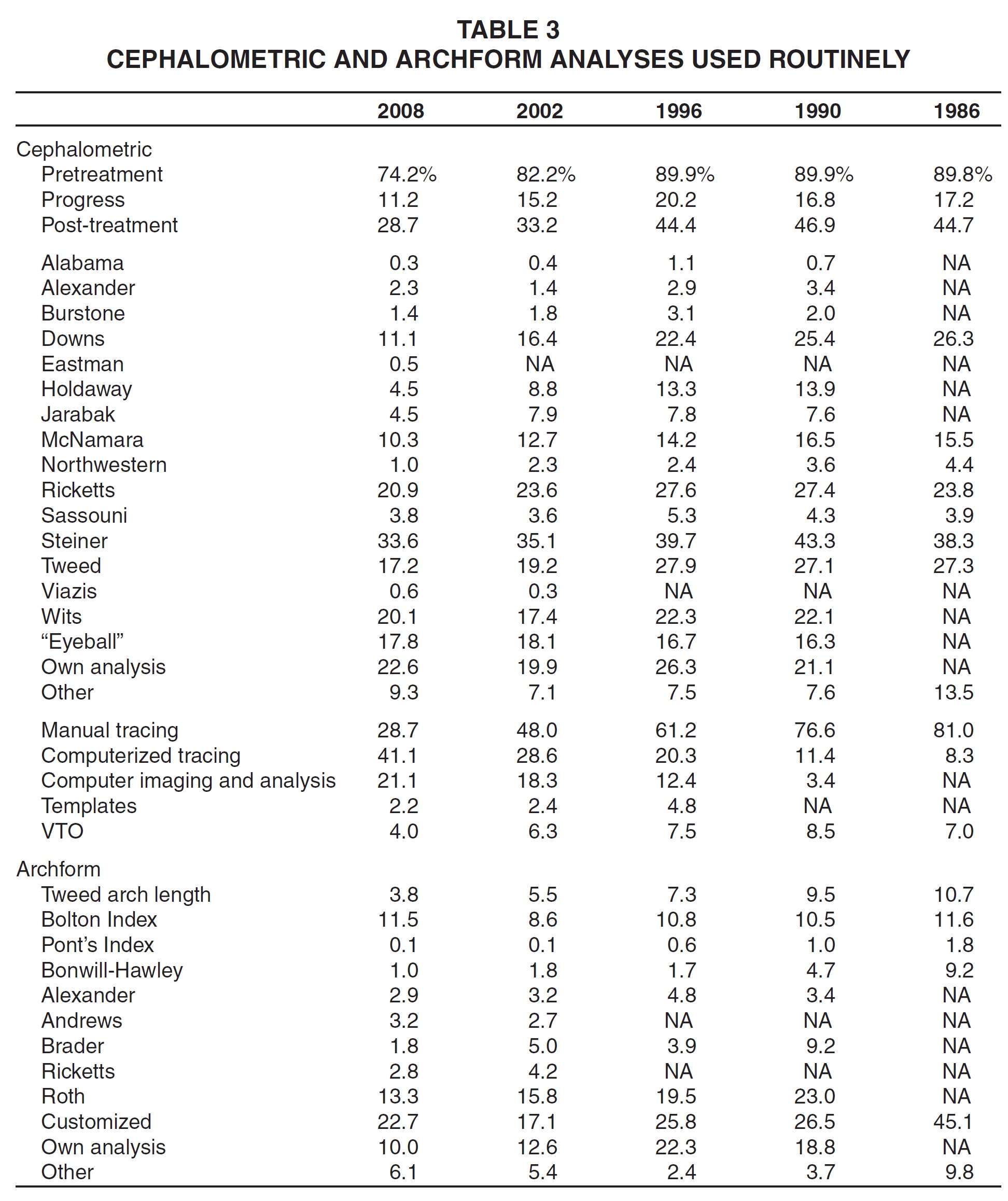
Respondents were somewhat more likely to use personalized or "eyeball" analyses for both cephalometric tracings and archforms than in 2002. Higher percentages reported using the Bolton Index and Andrews archform analysis routinely in 2008 than six years earlier, but the Roth remained the most popular standardized archform analysis.
Fixed Appliances
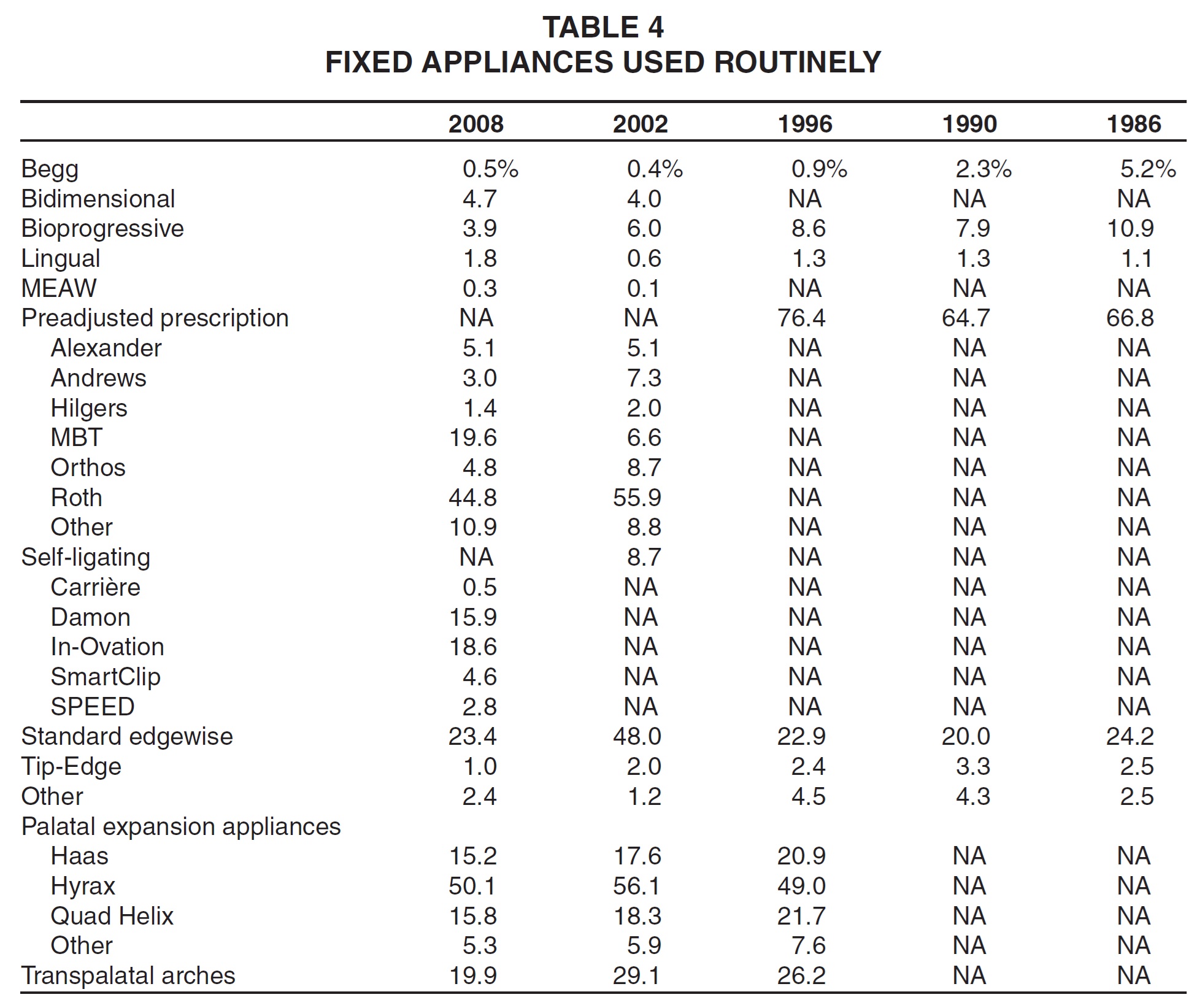
Since the 2002 Study, there was a substantial increase in the routine use of self-ligating fixed appliances compared to standard edgewise brackets (Table 4). While the Roth prescription was still the most commonly used preadjusted system, the MBT bracket was the only one to show more routine usage than in 2002. Lingual appliances registered a slight uptick, but palatal expanders and transpalatal arches were used less routinely than in previous surveys.
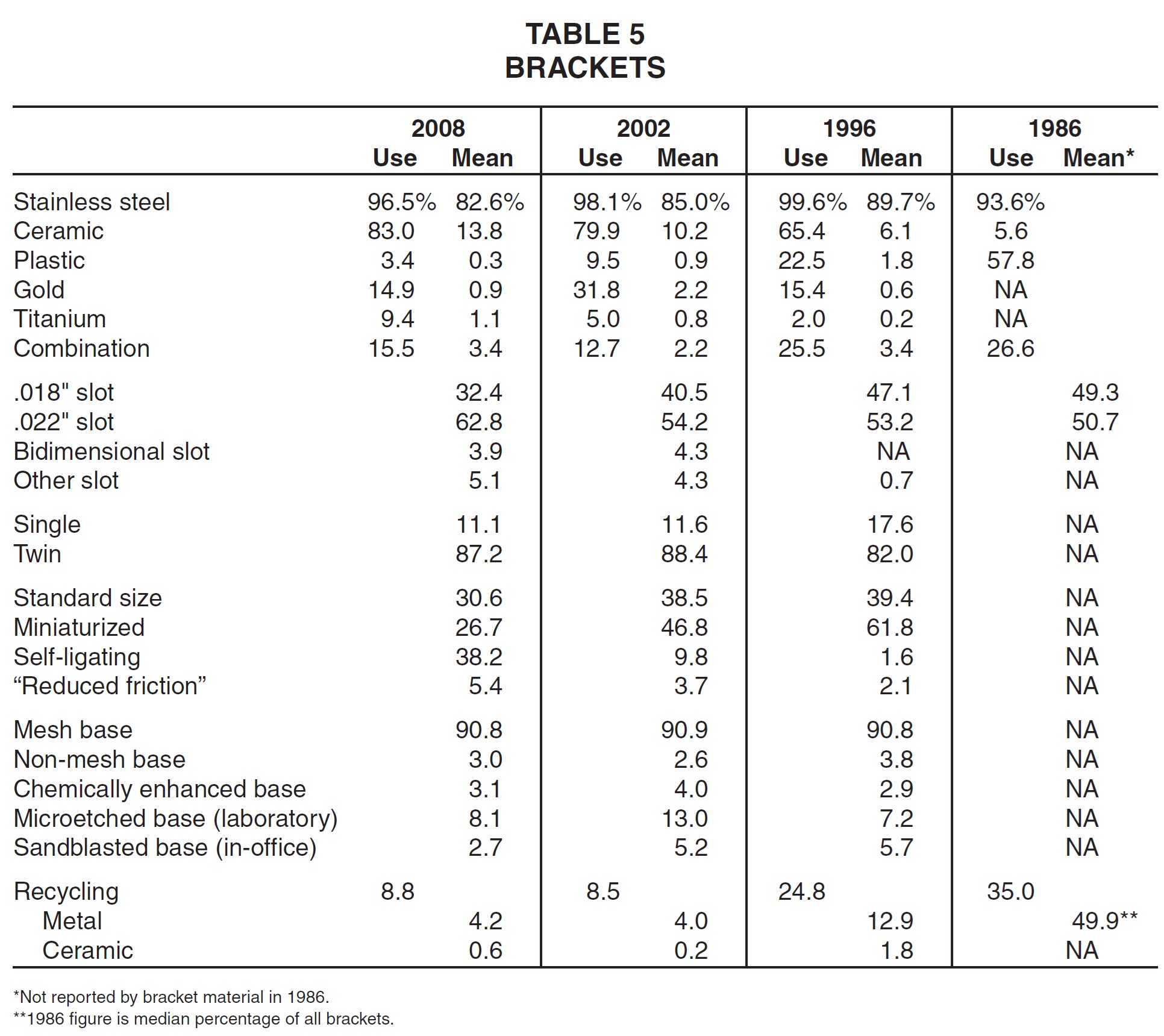
The use of ceramic brackets continued to increase in relation to stainless steel brackets (Table 5). Compared to the 2002 Study, more practices used combination or titanium brackets, but fewer used plastic or gold brackets. Appliances with .022" slots gained even more popularity over those with .018" slots, while twin brackets remained an overwhelming choice over single brackets. Both standard-size and miniaturized brackets continued to decline in usage, with self-ligating brackets again showing a notable increase. Nearly all brackets still had mesh bases, but microetching and chemical enhancement were used less often than in 2002. Recycling stayed at about the same level as it was six years ago, used by fewer than 10% of the respondents.
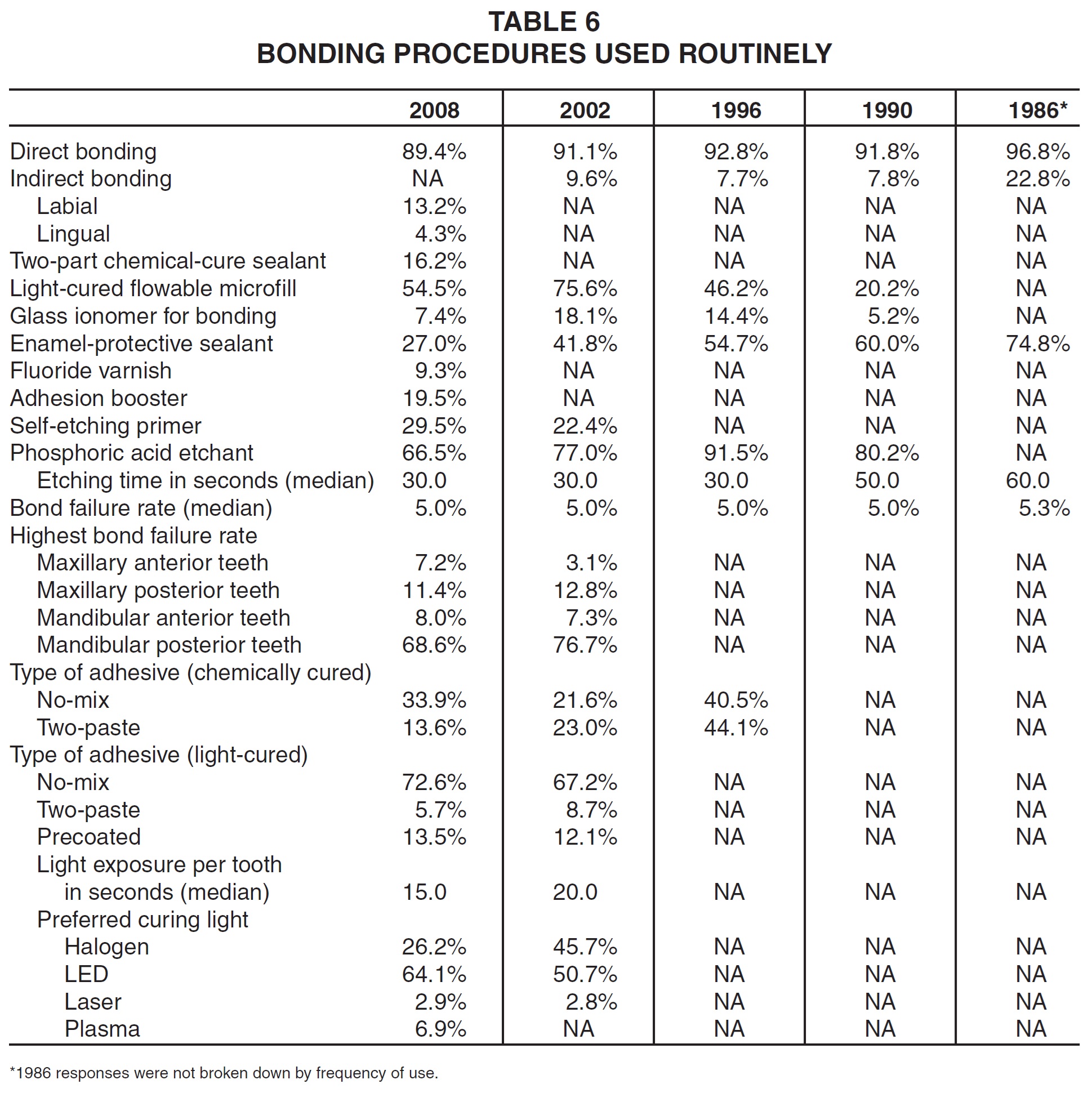
Indirect bonding continued a gradual in-crease in popularity compared to direct bonding (Table 6). Adhesive products were broken down differently from previous surveys, making comparisons difficult, but self-etching primers gained in routine usage compared to etching with phosphoric acid. The median bond failure rate was reported as 5%, as it has been in every Study to date; as in the last survey, the mandibular posterior teeth were considered the most difficult to bond successfully. No-mix adhesives gained more of an edge in routine usage for both chemical and light curing. A vast majority of respondents said they used some kind of light-cured adhesive on a routine basis, with LED units by far the most popular curing lights. The median exposure time per tooth dropped slightly since the 2002 Study, from 20 to 15 seconds.
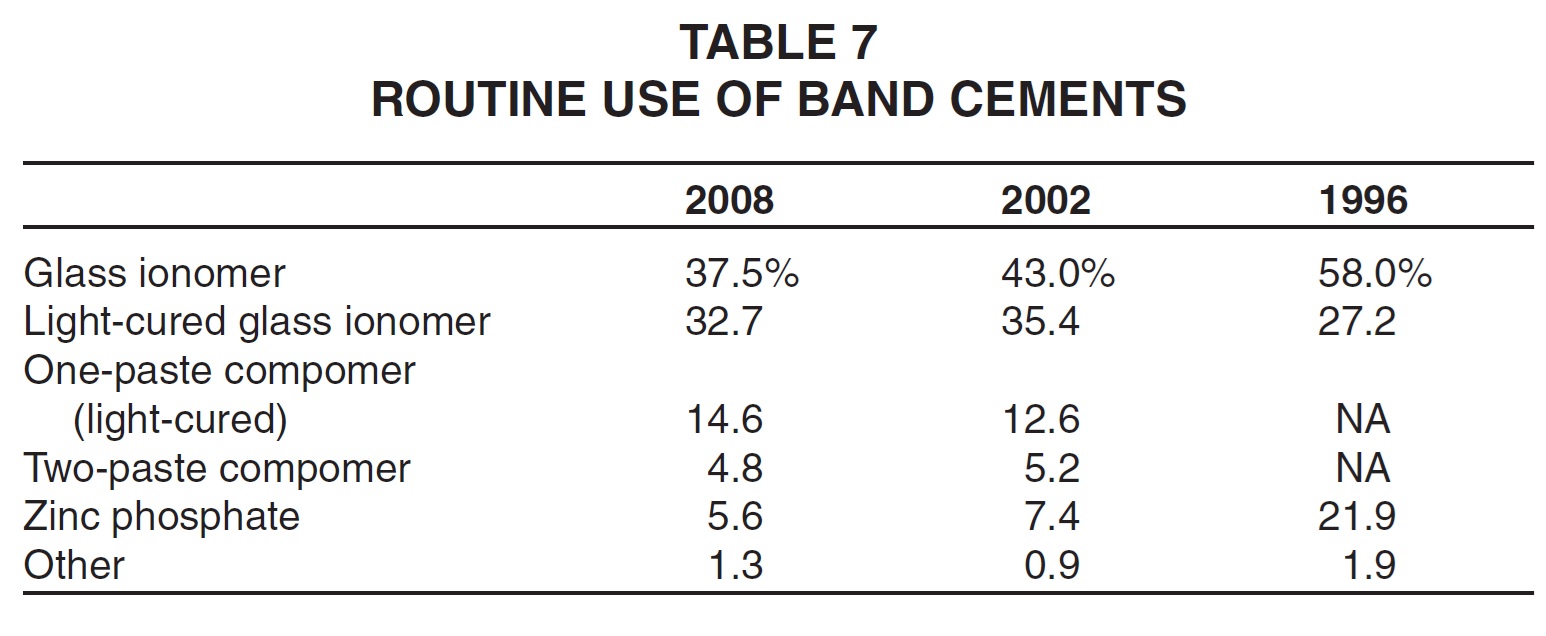
Glass ionomer band cements continued to be the most commonly used, with light-cured glass ionomers now used by nearly as many respondents as the standard varieties (Table 7). Light-cured, one-paste compomers gained slightly in routine usage compared to the 2002 Study.
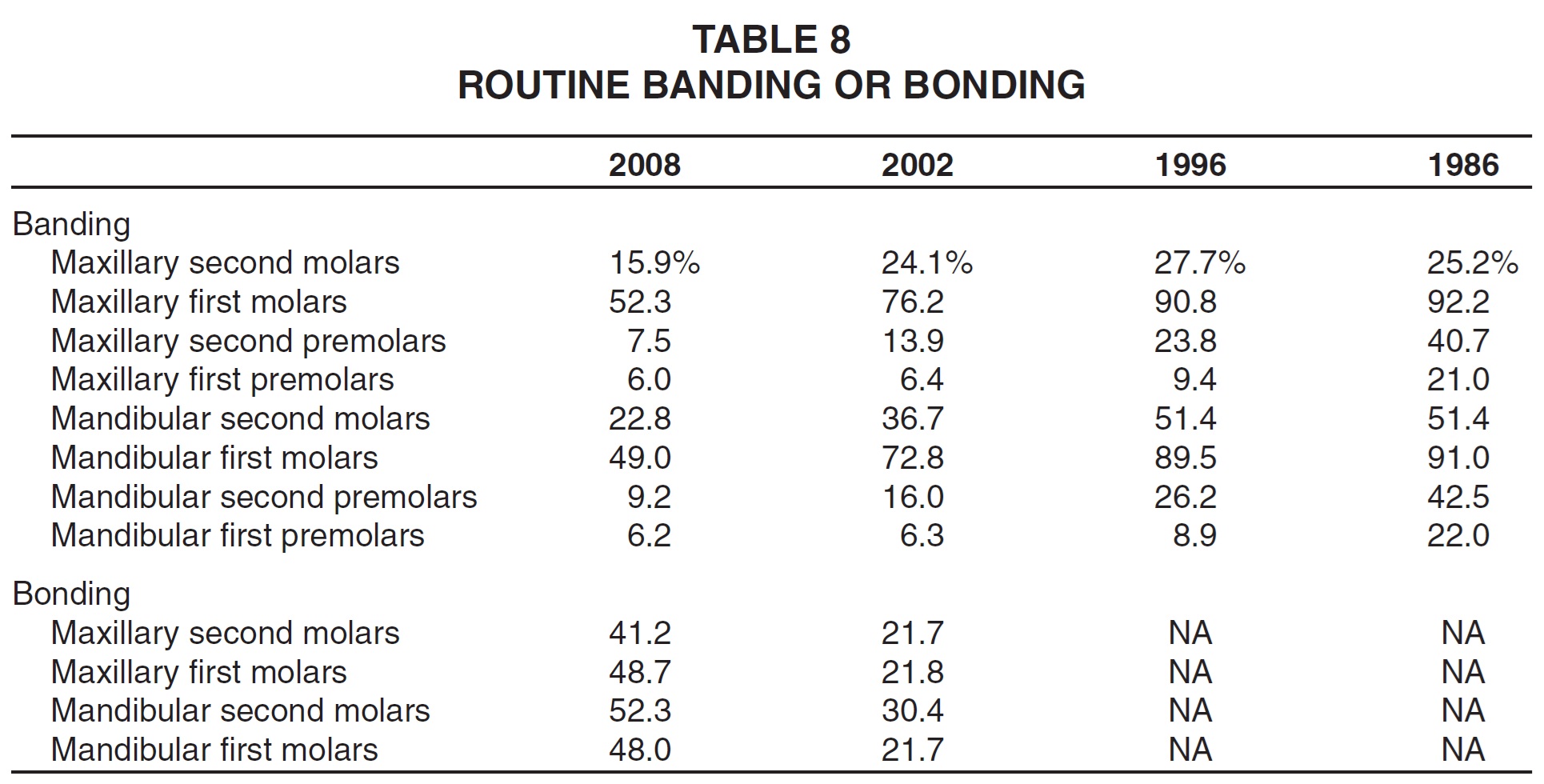
Routine bonding of posterior teeth, as opposed to banding, remained on the upswing over the past six years (Table 8).The maxillary first molars were the only teeth that were routinely banded by a majority of respondents to the current survey.
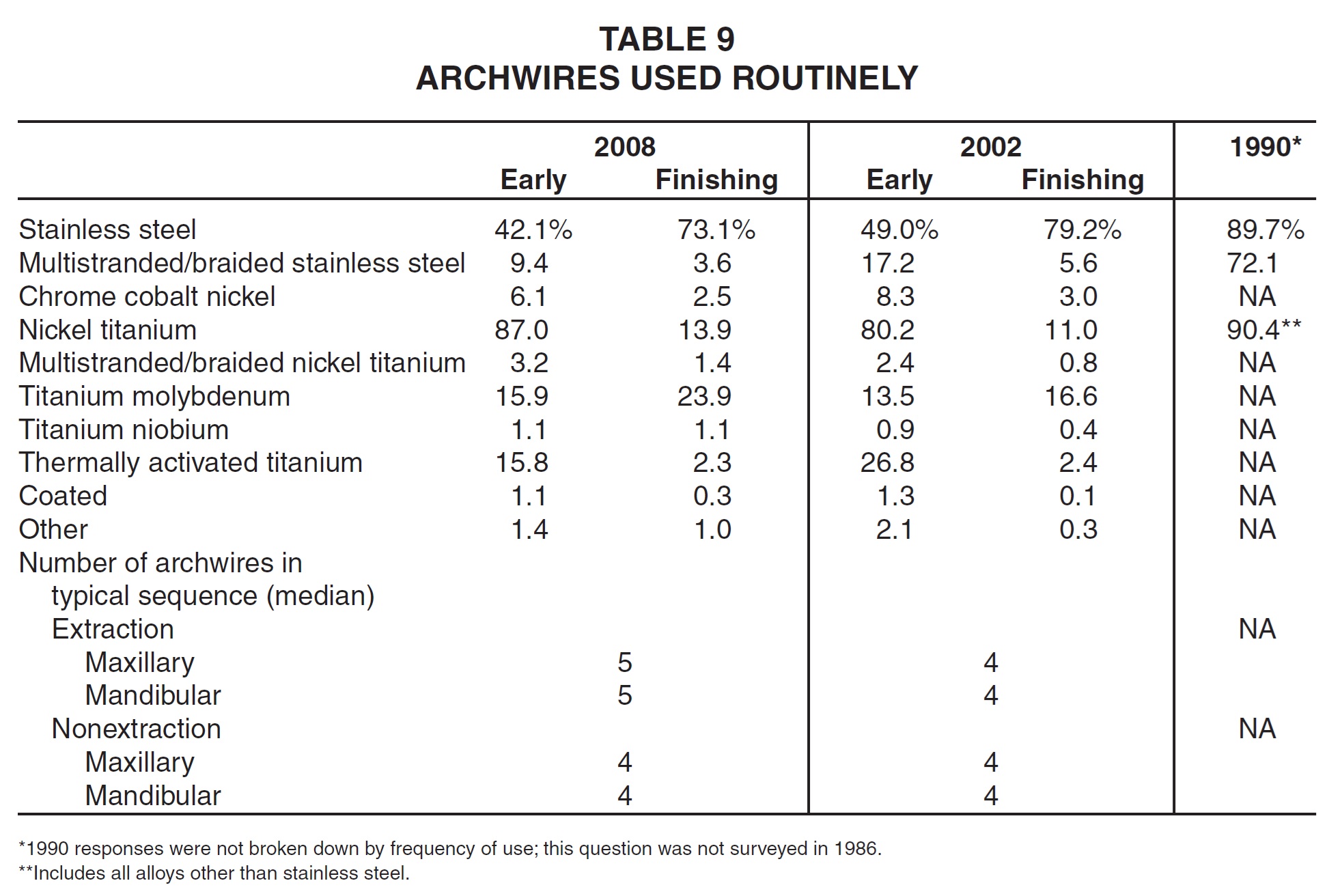
Routine use of titanium-alloy archwires, except the thermally activated type, continued to increase compared to stainless steel, especially in the early stages of treatment (Table 9). Titanium molybdenum archwires were used substantially more for finishing than in 2002, although stainless steel wires were still used routinely by nearly three-quarters of the respondents. The median number of archwires per extraction case rose slightly, from four to five in each arch.
Other Appliances
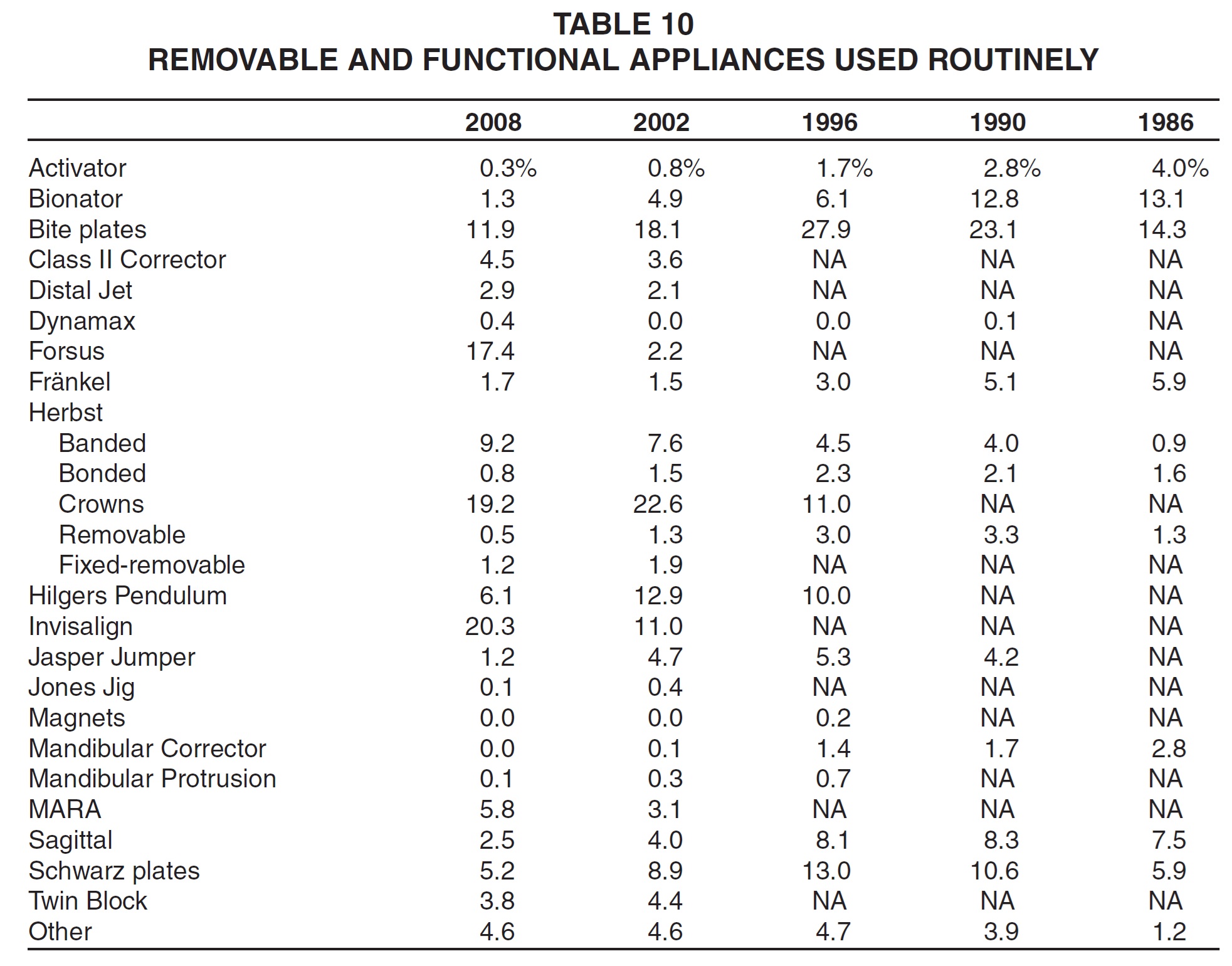
The only removable or functional appliances used routinely by more orthodontists in the 2008 Study than in the past were the Class II Corrector, Distal Jet, Forsus, banded Herbst, Invisalign, and MARA (Table 10). Both the Forsus and Invisalign systems showed sizable increases in usage compared to the 2002 Study.
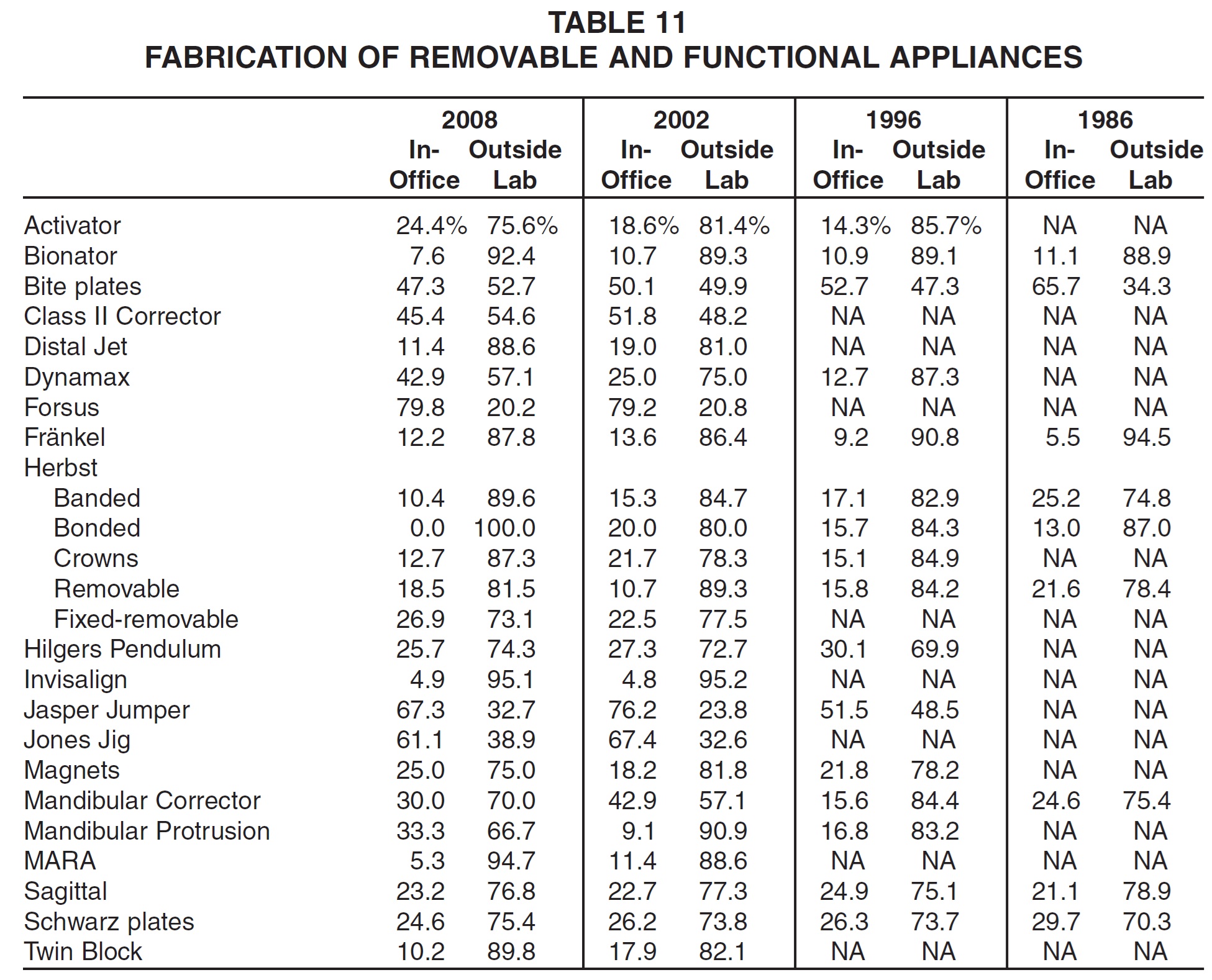
As in 2002, there was a general trend toward more use of outside laboratories for fabrication of removable and functional appliances, as opposed to in-office construction (Table 11). Only the Forsus, Jasper Jumper, and Jones Jig appliances were fabricated in-house by a majority of clinicians.
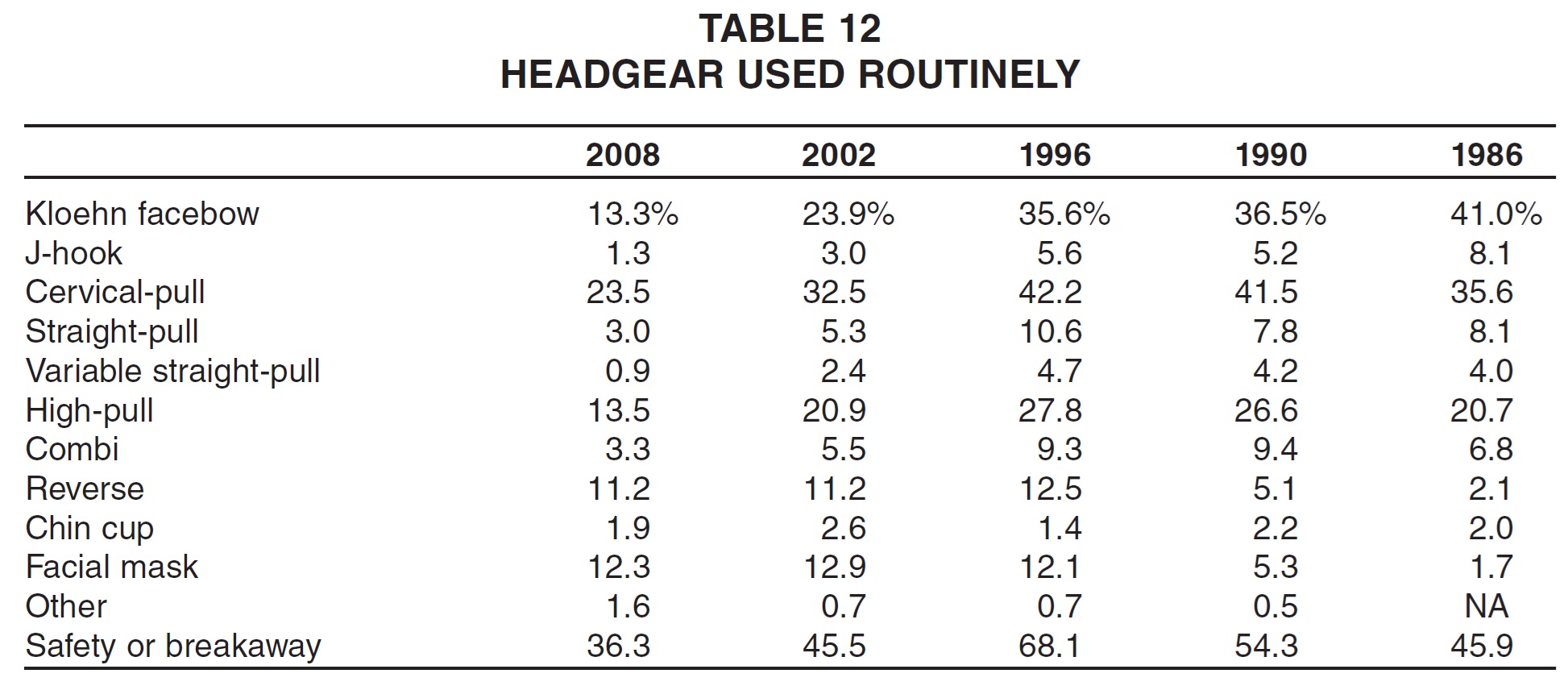
Routine prescription of headgear continued a dramatic decline since the 1996 Study, perhaps owing to the development of skeletal anchorage techniques (Table 12). Only reverse headgear was used routinely by as many respondents as in 2002. It appeared that most orthodontists who used facebows prescribed the safety or breakaway type.
Extractions
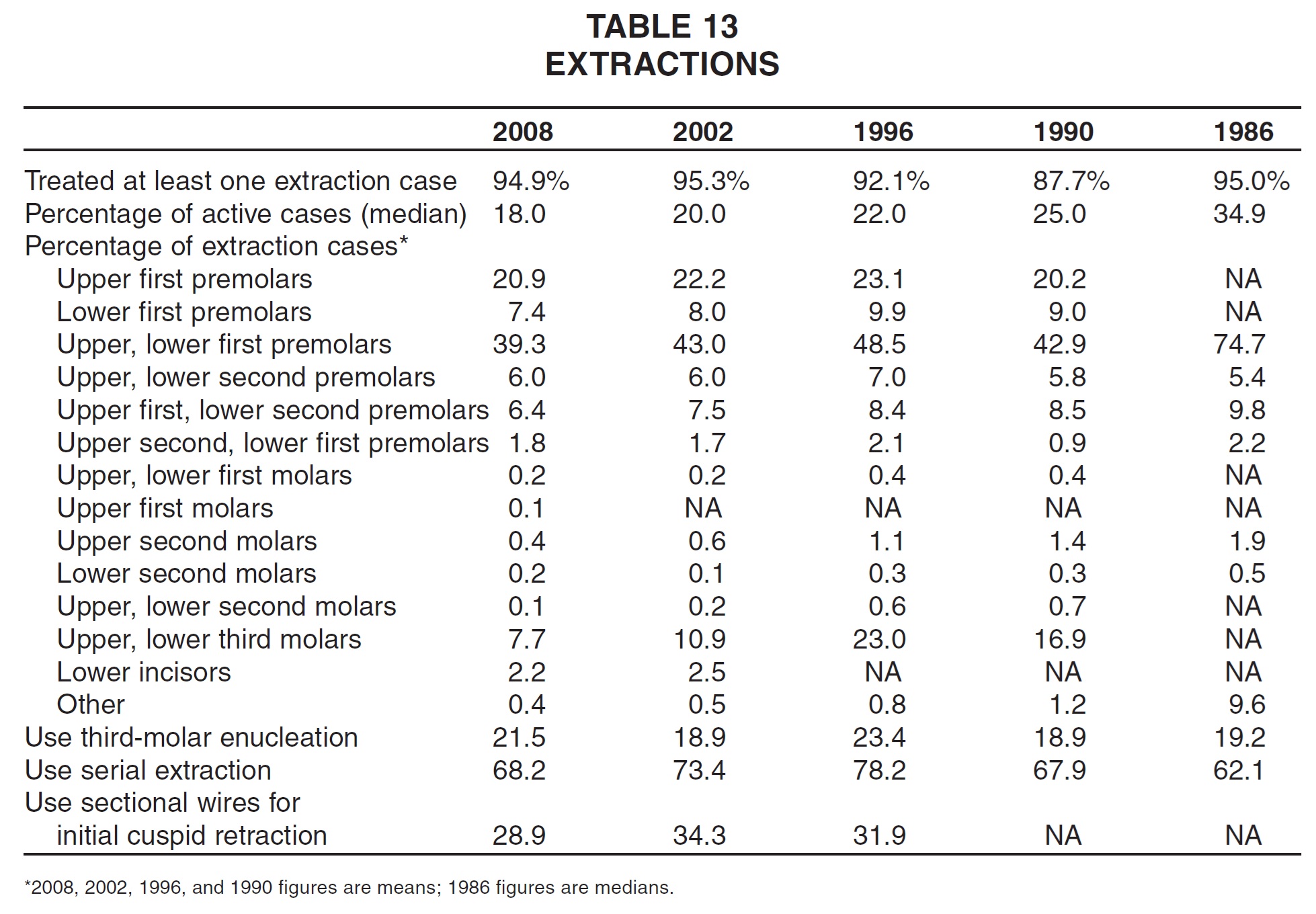
Over the past two decades, fewer and fewer patients have been treated with extractions; the median percentage in the current survey was only 18% (Table 13). As in every previous Study, nearly all extractions involved some combination of premolars. The percentage of extraction cases involving all four third molars continued to de-cline, reaching a low of 7.7%. More than two-thirds of the clinicians continued to prescribe serial extractions, but only 21.5% used third-molar enucleation. Slightly fewer used sectional wires for initial cuspid retraction than in past surveys.
Finishing and Retention
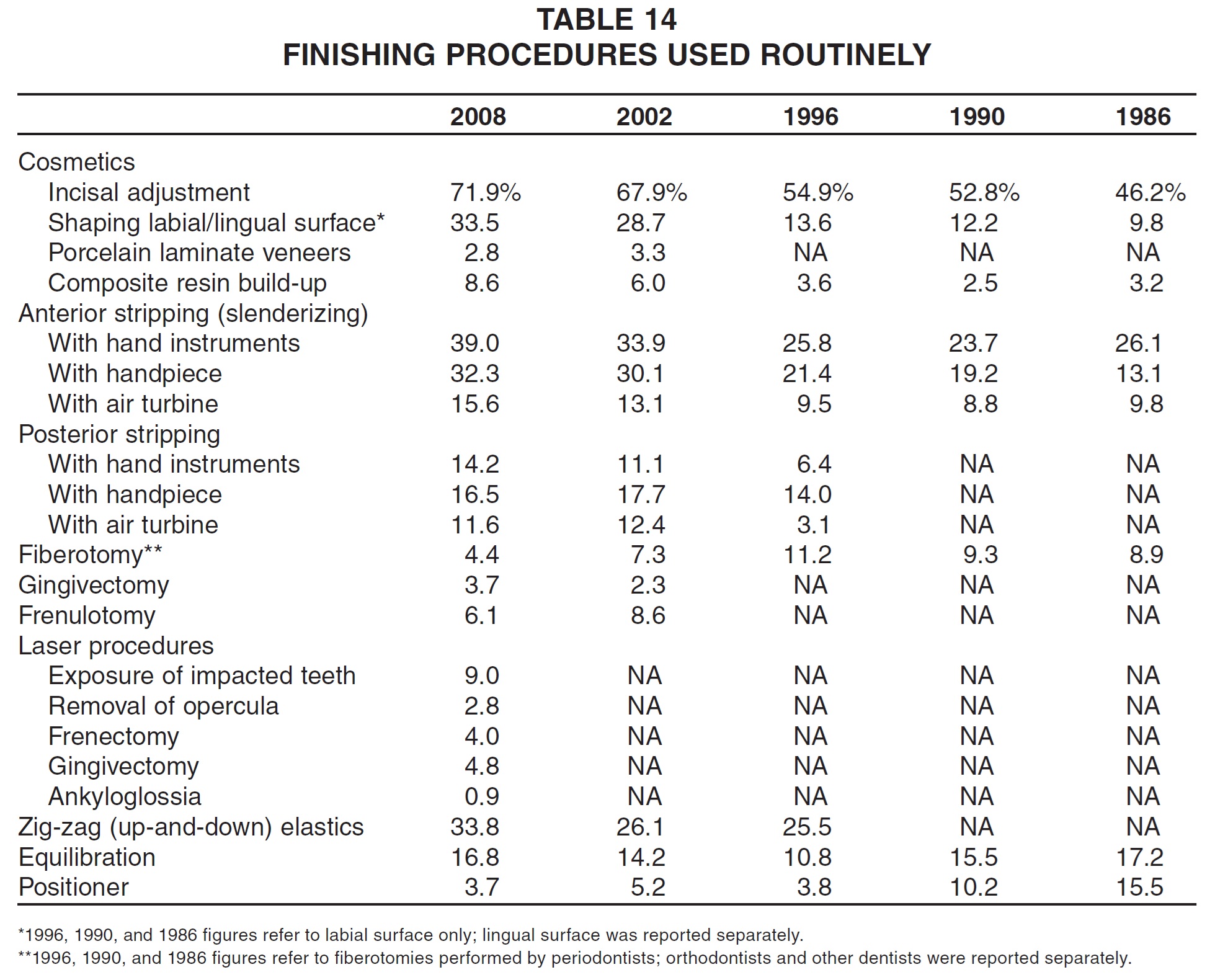
Most cosmetic finishing procedures were used more routinely in 2008 than in any Study to date (Table 14). These included incisal adjustment, reshaping, composite resin build-up, anterior stripping, and posterior stripping with hand instruments. Laser procedures, surveyed for the first time, were not used by many respondents. More than one-third of the clinicians routinely used zig-zag elastics for finishing. Routine equilibration rose for the second consecutive survey, but positioner use reached an all-time low.
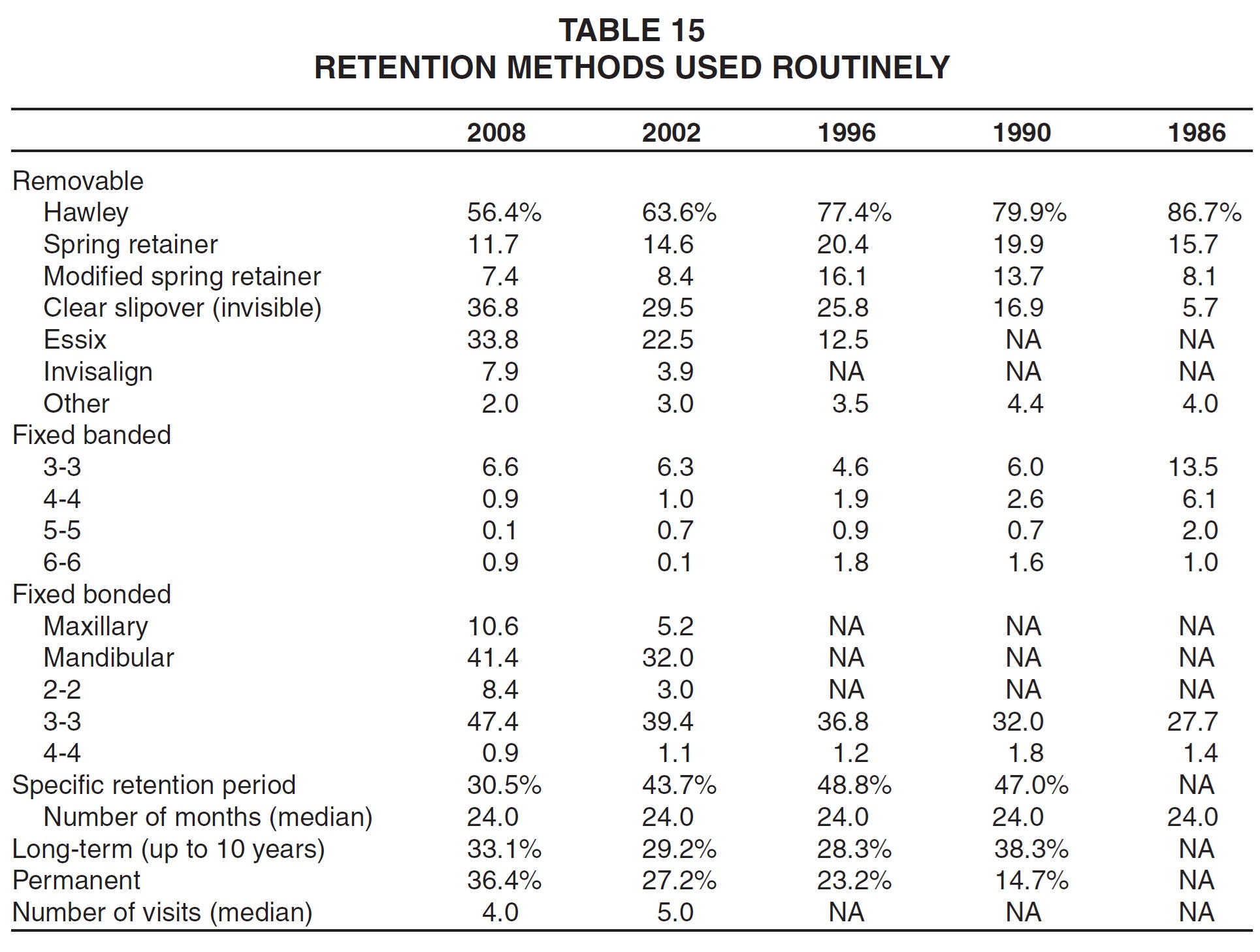
Routine use of clear retainers, as opposed to Hawley and spring-type retainers, continued to increase (Table 15). Banded retainers were used by only a few clinicians compared to 1986, but bonded retainers, especially mandibular 3-3, were used by more respondents than ever. Although the median retention period remained at 24 months, a trend continued toward more open-ended retention, with a plurality prescribing "permanent" retention for the first time.
Surgical-Orthodontic and TMJ Treatment
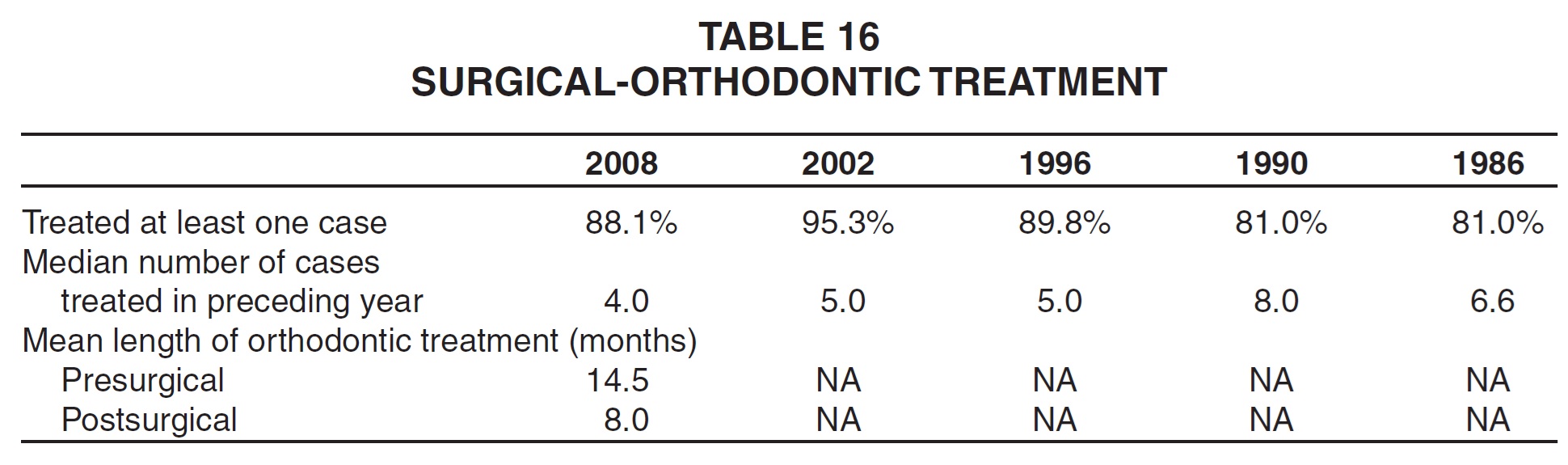
The percentage of respondents treating surgical-orthodontic patients was down slightly from its 2002 high, with an overall median of only four such cases treated in the past year (Table 16). For the first time, clinicians were asked how long they treated patients before and after surgery; the means were 14.5 months for presurgical and 8.0 months for postsurgical treatment.
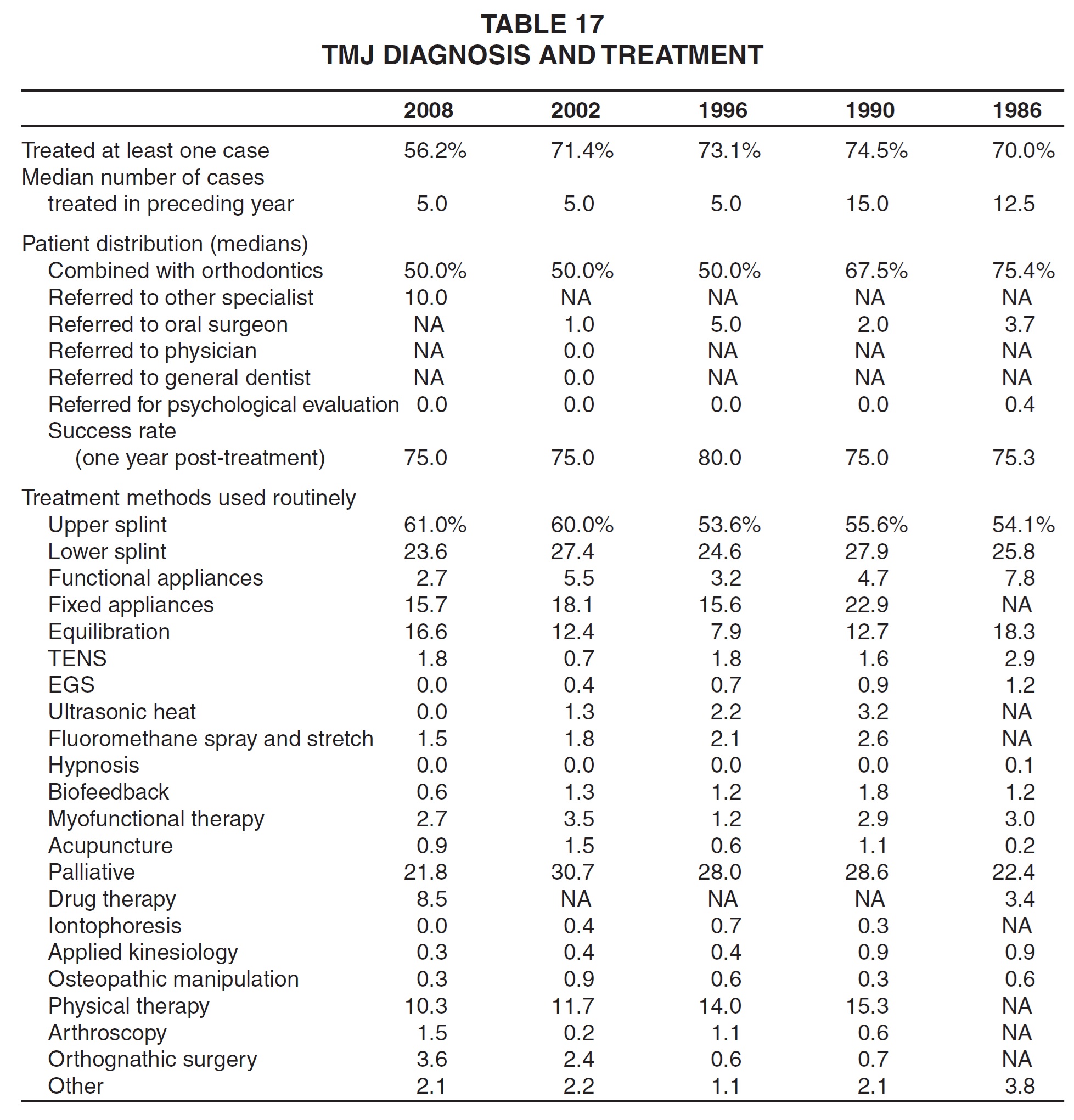
The percentage of clinicians treating at least one TMJ case reached an all-time low, but the median number of cases remained at five, as in the past two surveys (Table 17). Respondents who reported treating at least one patient said they combined TMJ treatment with orthodontics in a median of 50% of their cases--as in the 2002 and 1996 Studies--and referred 10% of their patients to other specialists. The success rate, defined as "asymptomatic one year post-treatment", remained at 75%. Upper splints and arthroscopic and orthognathic surgery were used more routinely for TMJ treatment than ever before. Equilibration and TENS were used more routinely than in the 2002 Study, but most other methods were used less frequently than in any previous survey.
Invisalign Treatment
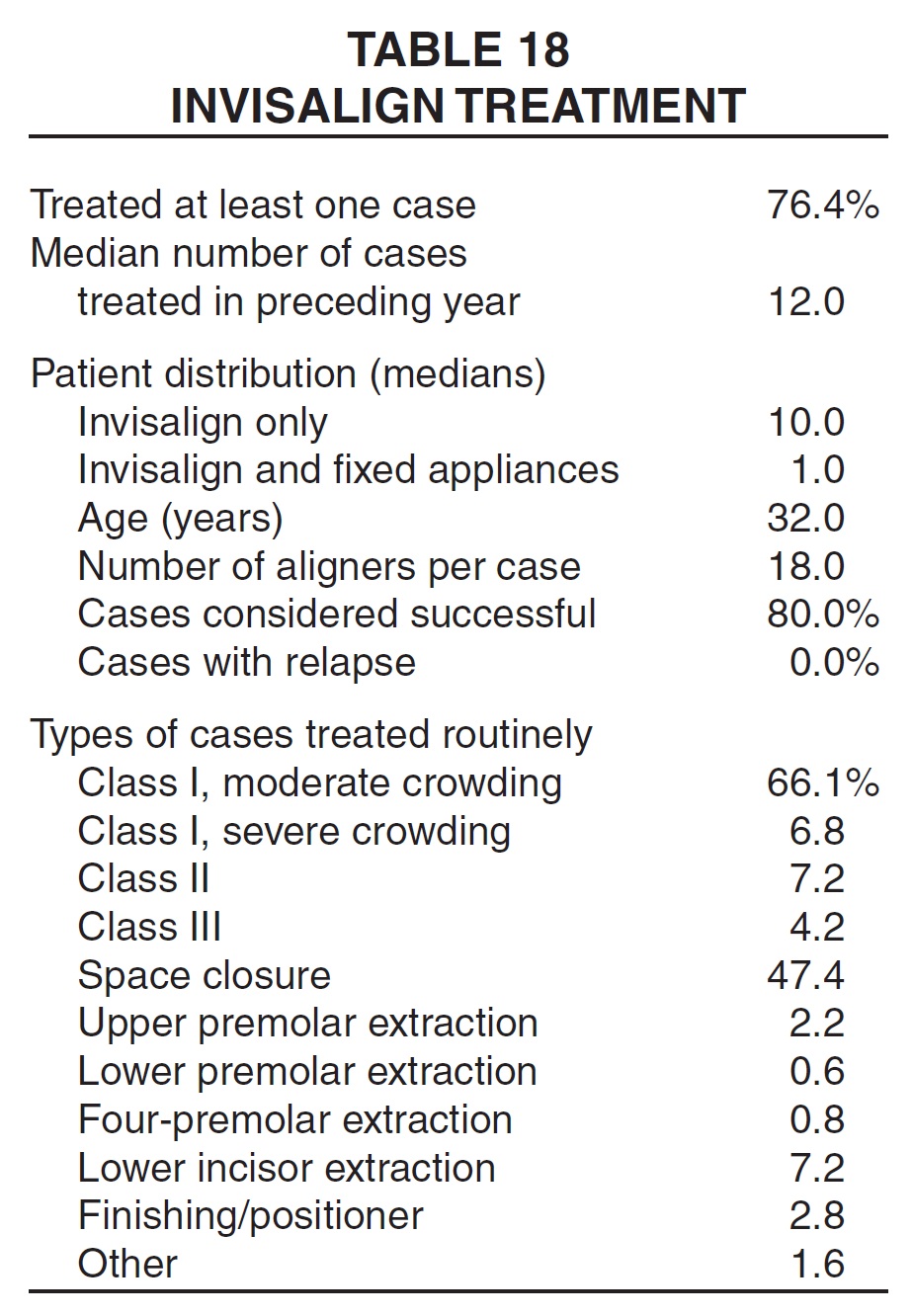
For the first time, respondents were asked for details on their use of the Invisalign system. More than three-quarters of the respondents said they treated at least one Invisalign case in the previous year, with a median of 12 patients (Table 18). Nearly all of these were treated with Invisalign only, rather than being combined with fixed appliances. The median age of Invisalign patients was 32, and the median number of aligners used was 18. Fully 80% of the cases were considered successful, with no relapse reported on average.
By far the most common use of the Invisalign system was for moderate crowding, followed by space closure. Other types of cases were treated routinely by fewer than 10% of the respondents.
Skeletal Anchorage
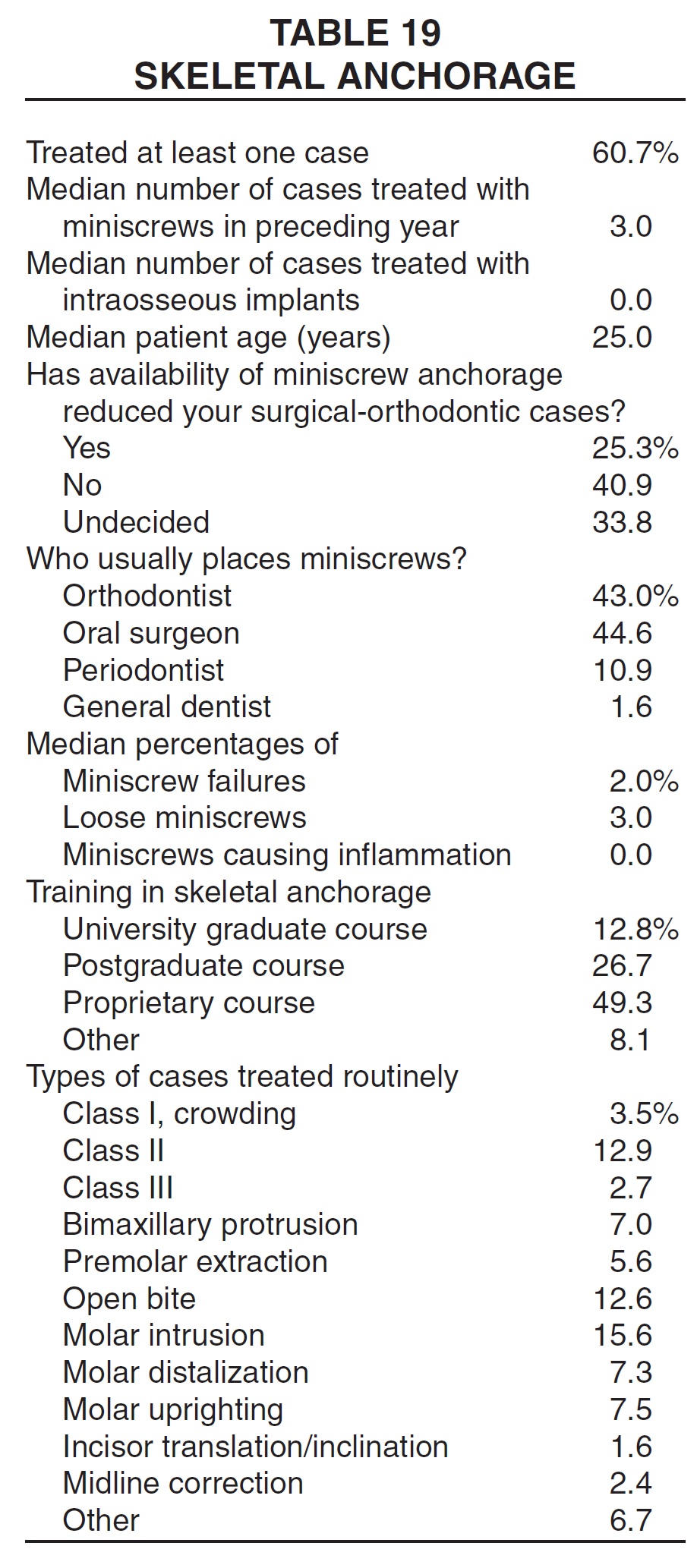
A section on skeletal anchorage was also included in the Treatment Study questionnaire for the first time (Table 19). About 60% of the clinicians reported treating at least one such case in the preceding year; miniscrews were used in a median of three patients, but intraosseous implants in a median of zero patients. The median patient age was 25.
Only a quarter of the respondents who used miniscrews thought the availability of skeletal anchorage had reduced their need to recommend surgical-orthodontic treatment. Clinicians were divided as to who inserted the miniscrews, with a slight edge going to oral surgeons over the orthodontists themselves. Miniscrew failures and loose screws were reported in only a few cases, and inflammation in a median of zero cases.Nearly half of the clinicians who used miniscrews had received their training in proprietary courses, as opposed to university settings.
A wide variety of cases were treated routinely with miniscrew anchorage, but none by more than 16% of the respondents. The most common treatments were molar intrusion, Class II, and open bite.
The appliances listed in this Study are trademarks of their respective companies, as follows.
MBT, Forsus, and SmartClip: 3M Unitek, 2724 S.Peck Road, Monrovia, CA 91016.
Orthos, Damon, Pendulum, and MARA: Ormco/"A" Company, 1717 W.Collins Ave., Orange, CA 92867.
Carriere: ClassOne Orthodontics, Inc., 5064 50th St., Lubbock, TX 79414.
In-Ovation: GAC International, 355 Knickerbocker Ave., Bohemia, NY 11716.
SPEED: Strite Industries Ltd., 298 Shepherd Ave., Cambridge, Ontario, N3C 1V1 Canada.
Tip-Edge: TP Orthodontics, Inc., 100 Center Plaza, LaPorte, IN 46350.
Hyrax, Herbst: Dentaurum, Inc., 10 Pheasant Run, Newtown, PA 18940.
Quad Helix: RMO Inc., P.O.Box 17085, Denver, CO 80217.
Distal Jet, Jasper Jumper, and Jones Jig: American Orthodontics, 1714 Cambridge Ave., Sheboygan, WI 53082.
Dynamax: Dynamax (UK) Ltd., 4 Queen Anne St., London W1G 9LQ, England.
Invisalign: Align Technology, Inc., 851 Martin Ave., Santa Clara, CA 95050.
Twin Block: DynaFlex, 10403 International Plaza Drive, St.Ann, MO 63074.
Essix: Raintree Essix, Inc., 6448 Parkland Drive, Sarasota, FL 34243.
-
 DR. KEIM
DR. KEIM -
 DR. GOTTLIEB
DR. GOTTLIEB -
 DR. NELSON
DR. NELSON -
 MR. VOGELS
MR. VOGELS
Dr. Keim is Editor, Dr. Gottlieb is Senior Editor, and Mr. Vogels is Managing Editor of the Journal of Clinical Orthodontics, 1828 Pearl St., Boulder, CO 80302. Dr. Nelson is Director and Research Consultant, Nelson Associates, Nederland, CO.