JCO INTERVIEWS
Charles J. Burstone, DDS, MS, Part 1: Facial Esthetics
DR. NANDA Charlie, your career in orthodontics has spanned more than five decades. Can you tell me how you chose orthodontics and education as a profession?
DR. BURSTONE I graduated from dental school in 1950, from Washington University in St. Louis. A visiting lecturer at the university, Orin Oliver, gave a course in the use of the labiolingual appliance. As part of that appliance, a bite plate was used, and I was impressed by his ability to grow mandibles in Class II patients by employing an occlusal guide. This experience sparked my interest and showed me that orthodontics was a very exciting specialty. At that time, I did not know that the question of modifying mandibular growth would still be with us today. I have to admit that current knowledge tells me that we are very limited in altering facial growth significantly in the Class II patient, but as a young dental student, I was very enthusiastic.
DR. NANDA Who were some of your role models during your early years in the profession?
DR. BURSTONE I was greatly influenced by some of our most significant leaders and pioneers in orthodontics. These included Wendell Wylie, Alan Brodie, Bill Downs, and Charles Tweed. Tweed sent to Indiana University, where I was a graduate student in 1953, radiographs of 50 consecutive well-treated patients. I traced the films and was impressed with the treatment, but I was confused by the unpredictability of the facial results that he achieved. Even with a relatively constant position of the lower incisor, the amount of lip protrusion varied considerably. This started one of my first research interests that I carried out for my thesis--I studied the soft-tissue thickness of the lips and the relationship of facial soft tissues to the position of the teeth and bones.
Similar articles from the archive:
DR. NANDA More than 50 years ago, you wrote some classic papers on the soft-tissue profile and lip thickness. In those days, was soft-tissue analysis considered to be an important part of treatment planning?
DR. BURSTONE This research was the basis of my early publication, "The Integumental Profile",1 where I set up standards that measured the shape and proportions of the face--soft tissues, not hard tissues. At that time, although facial esthetics was considered important, little attention was paid to it in determining orthodontic goals. It was assumed that if one correctly positioned the teeth according to a preconceived standard, good facial esthetics would be automatic. Later, with the widespread use of cephalometrics, the idea was that analyses such as Tweed, Downs, and Steiner would be sufficient, and that one had only to look at the teeth and bones, not the soft tissues.
Early in my research, I realized that because of the variation in the soft tissues that covered the teeth and bones, there was no system of hard-tissue cephalometric measurements that could predict good facial esthetics.2 My research showed that in good-looking faces, there was a broad variation in the position of the lower incisor and other dentoskeletal measurements.3,4 Currently, there is much interest in facial esthetics, as evidenced by many and frequent articles in the orthodontic journals. The rediscovery of the importance of esthetics started with the introduction of orthognathic surgery as one of our important modalities of treatment.
DR. NANDA Can the average soft-tissue measurements that you established, based on good-looking faces, be used as a guide for treatment? In other words, is an average-looking face also a good-looking face? Can we also have atypical faces that may be attractive?
DR. BURSTONE As a young orthodontist, I thought in very simplistic terms that these averages of facial morphology could serve as goals. I certainly was ignoring a broad literature from philosophers and artists suggesting that a definition of beauty is not so simple. New research by anthropologists, physiologists, and psychologists has focused on the limitation of averages. Farkas and Munro made numerous soft-tissue profile measurements, comparing above-average and below-average faces, and found no significant differences in the measurements.5 Thus, there is much more to it than taking a sample of beautiful faces, selecting a given number of cephalometric measurements, and then creating averages, as I did in my early studies. On the other hand, psychologists Langlois and Roggman averaged faces by computer and showed that the simple act of averaging a number of random, not particularly good-looking faces produces a face that becomes more beautiful.6
DR. NANDA So is the use of averages, either from films or direct measurement on patients, our best bet in determining what we would like to do esthetically?
DR. BURSTONE Averages of good-looking individuals can be useful; however, we should be careful that we do not blindly misuse these averages. If we routinely treat to means, we are missing much of the important variation that clinicians should consider. At the extreme, we might consider doing some radical things such as orthognathic surgery when no surgery is indicated.
DR. NANDA Then what should we consider beyond the averages that could influence our treatment planning?
DR. BURSTONE One very important concept is the enhanced average. Langlois and colleagues have used the computer technique of averaging to create a face that went beyond just the average.7 They enhanced the average face by selecting some faces that were deemed to be more handsome or beautiful by a panel of evaluators. They modified the final face in the direction of the selected faces, rather than using the mean alone. Panels of evaluators considered this newly derived face to be much more beautiful than the average. It now seems to be well established that the most attractive face may not be average--they might be called super-average. These super-average faces tend to be more masculine for men, with more prominent chins and thin, retrusive lips. Super-average female faces tend to be more retrognathic and immature, with protrusive lips (Fig. 1). Thus, what may be preferred is not the average, but a distorted or enhanced average.
DR. NANDA Does this suggest that there is a strong sexual component to what is considered a good face that is not picked up on our typical cephalometric analyses, even when corrected for gender?

Fig. 1 Females who have more convex, shorter lower faces and protrusive lips, and who generally appear more immature, are considered more attractive than sex-corrected averages. Actress Sarah Michelle Geller demonstrates this type of feminine-accentuated face in computer drawing made from photograph.
DR. BURSTONE Numerous anthropologists and psychologists have studied this sexual component. Perrett and colleagues8 and Fink and colleagues9 have shown that faces are very important in mating and that faces, on a biological basis, reflect the health of an individual and fertility. Women, for example, prefer more masculine faces during the most fertile period of their menstrual cycle. At other times, a more feminine-looking male face could be deemed desirable. So once again, what is a beautiful face is considerably more than some statistical average, since it can change over time. No analysis, however complete, fully describes the face. Important measurements can be left out of our analyses, and factors such as skin texture, complexion, and other intangibles can influence the appearance of the face. Three-dimensional measurements are better than two-dimensional; however, three-dimensional analyses by themselves are still insufficient to define beauty.
DR. NANDA Do lay people, orthodontists, and our patients agree on what are desirable facial characteristics?
DR. BURSTONE Many studies show that different groups of people, even of the same population, evaluate faces differently. For example, plastic surgeons seem to be more concerned with the show of vermillion border and lip plumpness. Orthodontists tend to look at lip protrusion or retrusion and symmetry. Patients and their families may look at entirely different characteristics than the orthodontist. In addition, cultural differences and cultural fads, which change over time, must be considered.
DR. NANDA It is often said that beauty is in the eye of the beholder. Does everyone really have his or her own valid idea of a beautiful face? If that is true, then we must spend more time with patients to appreciate what they want.
DR. BURSTONE We all have individual experiences that lead us to what we consider a desirable face. However, new research has shown that the way the brain works is not an individual matter. What is innate or built-in is the basic mechanism of how we process visual material. A good example of this processing is how the brain evaluates bilateral symmetry. Burt and Perrett have shown that individuals who have a dominant right side of the brain will look at any given face and see both sides of the face as symmetrical mirror images of the right side.10 We orthodontists might make our measurements from a PA headfilm or photograph and see a difference in our patient between the right and left sides. Because of the working of the central nervous system, an untrained observer or patient may not see the asymmetry.
Neurologists such as Makeig and colleagues have proposed that there is a specialized face-recognition center in the brain.11 This center is very important for survival, since it allows us to quickly and accurately identify friendly or unfriendly faces. This same center is involved in identifying beautiful or attractive faces. He postulates that identification of the face is not analytical, and that we evaluate a face as a whole. Analytical evaluation is what we do in cephalometric analyses by making many measurements. The face center works, by comparison, on the template principle. That is analogous to placing a cephalometric tracing of the original malocclusion on top of the treated orthodontic tracing. Hence, in our brain, we develop a picture of what an attractive face might be, rather than a lot of angles and linear measurements, and then compare that picture or template with the person we are looking at.
DR. NANDA Can we assume that this template or picture is learned and is culturally dependent?
DR. BURSTONE Rubenstein and colleagues have shown that even 6-month-old babies can identify attractive faces.12 Some new research suggests that this may be learned, rather than genetic or inherent in our central nervous system. There have been some cross-cultural or racial studies where a Caucasian panel will select the same attractive faces of Asians as an Asian evaluator panel.13 Why is this? Is there something inherent in the way the brain works independent of our learning experience? Is the brain looking at something different than an average of a population that we are used to seeing?
DR. NANDA There is an old expression, seeing is believing. You're saying that there's more to visual processing than a simple photographic process where images are recorded and remembered by the brain.
DR. BURSTONE We now know that seeing is not always believing, since the brain is part of the process of identifying attractive faces. All of us are acquainted with optical illusions that demonstrate the role of the brain in interpreting visual material. To appreciate and to understand attractive faces, we have to look beyond our cephalometric standards that isolate the face from the role and function of the brain.
DR. NANDA How does this new research influence our clinical orthodontic practice?
DR. BURSTONE It tells us that we should be very careful in just routinely applying cephalometric averages to determine tooth position and bone position for orthognathic surgery, or even for orthodontics alone. A good example is the evaluation of lower facial height. A typical ratio of lower face height to upper face height is commonly used--for instance, the distance subnasale-menton is typically the same as glabella-subnasale (Fig. 2). However, if this ratio is larger or smaller, what is the significance? It is not necessarily an indication for orthognathic surgery. It might not differentiate between an attractive and a non-attractive face. One must consider, among other factors, if there is adequate lip length or incisor exposure. More important, the new research is showing us that you can have considerable variation in facial height proportions and still have an attractive face. We do not want to make short faces into long faces or long faces into short faces unless there is a good functional reason for doing it. There are also attractive long faces and attractive short faces.
DR. NANDA How should we look at the so-called long-face syndrome? Is that an indication for orthognathic surgery?
DR. BURSTONE I do not think there is such a thing as a long-face syndrome. There are patients who have a large vertical dimension in the lower face and who have adequate lip length with a normal interlabial gap. The display of the upper incisor to the lip is normal. This is very different from a patient with a large lower-face vertical dimension, but with short lips and interlabial gap. In the latter situation, orthognathic surgery could be considered for both functional and esthetic improvement.
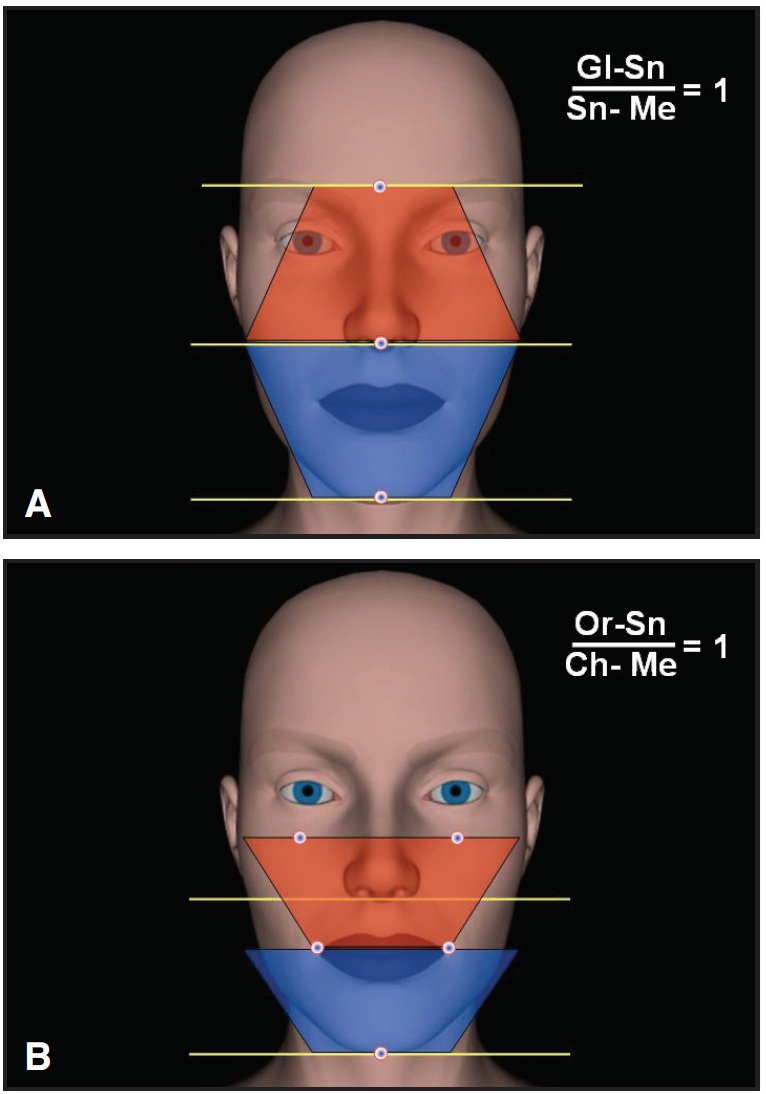
Fig. 2 A. Upper-to-lower facial dimensions (Gl- Sn/Sn-Me) in ratio of 1:1 (lower face may be slightly longer in males). B. Another way to evaluate lower facial height (Or-Ch), with same 1:1 ratio.
In the same vein, there are many different types of short lower faces. Some have adequate lip length and others a lip-length redundancy. Some have a problem and many do not.
DR. NANDA You talk about the face in five dimensions. What are the five dimensions that we must consider?
DR. BURSTONE The first three are spatial--in other words, a three-dimensional face. Traditionally, we've looked at faces primarily from the profile view. Even when we would look from the frontal view, this was done in isolation and not particularly correlated with the lateral view. Patients rarely think of themselves in these arbitrary poses. We clinicians have always had a difficult time thinking in three dimensions.
The fourth dimension is time, which recognizes that faces change during maturation and that as adults we also age. The fifth dimension is function. During function, we look at faces differently and, most important, we evaluate the dental exposure--such as the amount of incisor showing. I've always considered the most important functional position to be the relaxed lip position. It is the most reproducible functional posture and, hence, can be used as a guide to tooth position. The face mirrors our emotions, and the muscles of facial expression give a multitude of tooth exposures. For instance, the amount of incisor exposure during anger or surprise varies considerably. As dentists and orthodontists, we have a fixation on one emotional expression: the smile. We need to broaden our horizons and attempt to assess all emotions and how these functions relate to tooth position.
DR. NANDA How valid is using the smile to determine tooth position?
DR. BURSTONE The first question has to do with reproducibility. A relaxed lip position is somewhat reproducible. Smiles, on the other hand, vary considerably in the same patient. Ekman, the psychologist-anthropologist, is considered the leader and pioneer in studying the muscles of facial expression. He differentiates between a natural and a forced or posed smile.14 The natural smile is a genuine smile when we are happy. The forced or posed smile is what we do for our yearbook in high school or, typically, for a photo in the orthodontist's record. It is very difficult for a posed smile to be reproducible, and therefore it cannot be considered an accurate guide for tooth positioning (Fig. 3).
DR. NANDA How can we tell if someone is giving us a genuine or a spontaneous smile?
DR. BURSTONE The spontaneous smile is also called the zygomatic smile, since the corners of the mouth are raised upward. The orbicularis oculi muscles also contract, giving a wrinkling around the eye (Fig. 4). Some people can learn to simulate this smile. Actors and actresses can be very good at a posed smile that simulates a genuine happy smile. During smiling, they can exhibit an abnormally large amount of gingival exposure. This is usually not a problem, since when the lips are at rest, there can be a normal amount of incisor exposure. If the orthodontist used this posed smile as a guide, however, we might mistakenly believe that a surgical impaction of the maxilla is required. This variation is one of the reasons that lip position during the smile cannot be used to determine the amount of incisor exposure (Fig. 5).
DR. NANDA It sounds as if there can be many different kinds of smiles.
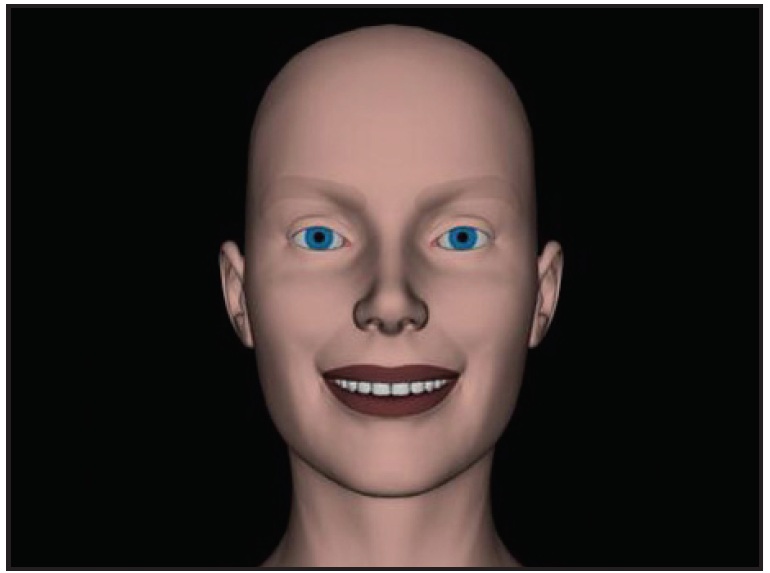
Fig. 3 Posed smile does not demonstrate happiness, is highly variable, and is not reproducible; characteristically, facial muscles surrounding eyes do not contract.
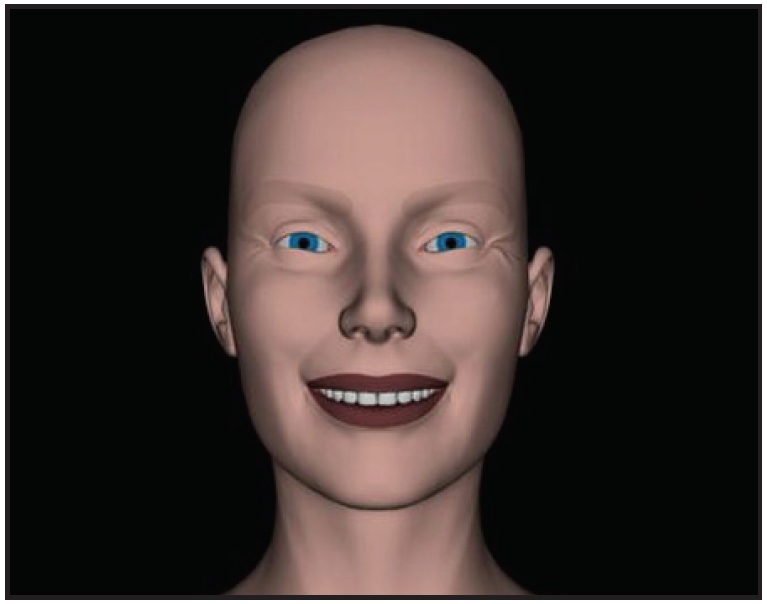
Fig. 4 Natural smile shows crinkling around eyes as orbicularis oculi contract; corners of mouth are usually brought upward and backward.
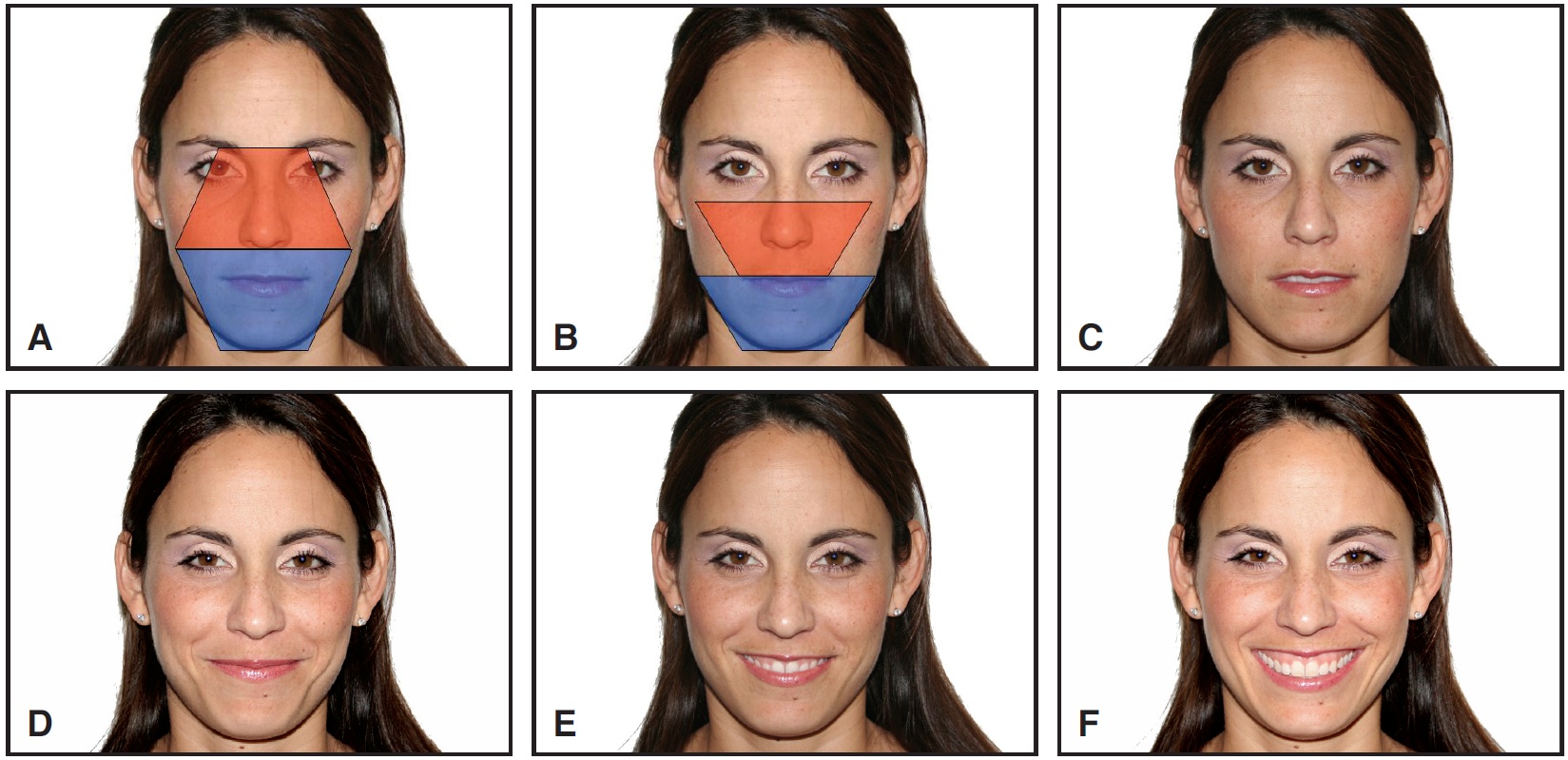
Fig. 5 Smile variation in subject who has typical vertical dimension in centric occlusion with lips closed. A. Lower vertical height compared to Gl-Sn (Fig. 2A). B. Lower vertical height compared to Or-Ch (Fig. 2B). C. Lips relaxed: Note normal interlabial gap of several millimeters and typical incisor exposure, with central incisal edges 3mm below upper lip. D. “Mona Lisa” smile: Posed smiles do not always display teeth. E. Medium-intensity smile. F. High-intensity smile, where subject is simulating natural smile: Corners of mouth are driven upward and laterally, and upper lip is moved upward. Gingival exposure is not a clinical problem, since vertical dimension and proportions are normal, lip length is adequate, and incisor exposure is normal in relaxed lip position. Orthodontist could misdiagnose based on this broad and healthy smile, which general public considers desirable.
DR. BURSTONE Ekman and colleagues have estimated that there may be over 10,000 visible facial configurations using the muscles of facial expression. They classify 18 different types of smiles--a fear-smile, a flirtatious smile, and so forth.14 In English we have basically one word for a smile; however, some languages like Thai recognize the different types of smiles and have different words to describe them. It is because of this variation that I prefer to use a relaxed lip position to determine the occlusogingival position of the incisors. Historically, orthodontists were considered experts on what is a pleasing smile--namely, ideal tooth position. However, we're beginning to learn more about the physiology and esthetics of the muscles of facial expression that produce the smile, and to recognize the inherent variation in how we smile.
DR. NANDA What about other functional activities? For example, could speech be useful in determining incisor position?
DR. BURSTONE Speech has been used to standardize jaw position and also to reproduce a posed smile. In English, the word "cheese" is constantly used for smiling poses. Certain consonant sounds may be much more reproducible than smiles. They are certainly language-specific and, hence, not universal. More research is needed to relate speech sounds to the amount of incisor exposure.
DR. NANDA We hear much about the smile arc. Do you feel this is an important consideration for esthetically aligning the anterior teeth?
DR. BURSTONE The smile arc is a prosthetic concept. During a smile, the lower lip forms an arc or curvature that should be a guide to the positioning of the teeth from the molar forward. Esthetically, the teeth should also form an arc. Here we have a paradox. Typically, the teeth forward of the first molars fall on the occlusal plane, with little or no curve of Spee. So how do we get a dental arc? This is part of the optical illusion as we look at teeth and bones in three dimensions. What determines the smile arc is the cant of the occlusal plane. We can run a very simple experiment with any patient. Have the patient move the head upward, flattening the occlusal plane, and one observes less of a smile arc (Fig. 6). Conversely, have the patient move the head downward, and more curvature is seen in the smile arc. What we are doing is altering the cant of the occlusal plane with this little experiment. Since the smile arc is partially determined by head posture, it is not a reliable method to establish dental esthetics.

Fig. 6 Although smile arc is supposed to follow curvature of lower lip, cant of occlusal plane changes as head posture moves upward, so that less curvature is seen in smile arc.
DR. NANDA Is the smile arc also affected by how we smile?
DR. BURSTONE The smile arc gets evaluated on the basis of lower lip curvature. How we smile and the magnitude of the smile influence the curvature. Furthermore, the more we open our mouths during smiling, the greater will be the lip curvature. Orthodontic tooth movement has to be very accurate; a millimeter or so of tooth movement can be very demanding. Thus, a vague soft-tissue reference line like the lower lip during smiling is not very helpful.
DR. NANDA Assuming we would like to increase the curvature of the smile arc, how could we do this?
DR. BURSTONE If we want to have good occlusion and good anterior tooth alignment, we are very limited. The cant of the occlusal plane could be steepened, but for stability, we usually do not want to radically alter the cant of the occlusal plane. We could extrude the central incisors, but a large step between the central and lateral incisors is unsightly. Some patients already complain about the normal step of a half-millimeter or so between the lateral incisor and the central incisor. The only other possibility would be to move the roots of the incisors mesially, which makes no sense anatomically. In short, not only is the concept of the smile arc a fiction, but there is also a limit to how much we can change it.
DR. NANDA Another idea that is widely discussed is the presence or absence of "black holes", or excessive buccal corridors. How important a treatment goal is the minimization of posterior black holes?
DR. BURSTONE We all learned in dental school that the black holes one sees with missing posterior teeth can be unsightly. Does this mean that a small black space between the cheek and the molars has any clinical significance? On a number of levels, there is little information to support this assumption. It is common to see advertising with attractive models showing large buccal corridor spaces (Fig. 7). There have been a number of studies reported in orthodontic journals showing no relationship between posterior black holes and facial esthetics.15,16 One study does show a relationship, but even there, an exaggerated black hole and enlarged views of the teeth were required to demonstrate any significant esthetic influence.15 The buccal corridor space does not seem to be something that our patients consider important.
It is essential to remember that the amount of buccal corridor space is not only determined by molar width, but also by muscle contraction of the buccinator. It therefore varies considerably with different smiles and how we smile. Evaluation of the buccal corridor can also be more difficult depending upon the direction of viewing. If one looks directly into the mouth, parallel to the midsagittal plane, a larger space can be seen.
DR. NANDA What do you think about dental expansion of the arches to reduce the buccal corridor space and to create a more esthetic archform?
DR. BURSTONE There are three questions here. First, is it stable to expand an arch? Second, if we want to, can we expand enough to make any difference in what the patient can see? Probably not. Third, is an expanded arch or rounded arch more esthetic? A number of studies demonstrate that lay people do not consider wider or more rounded arches more esthetic. Orthodontists may, but that has no relevance. It is easy for us to brainwash ourselves.
DR. NANDA Facial esthetics and smiles are very important to both the patient and the orthodontist. As you have pointed out, optimizing facial esthetics is more complicated than using simplistic means or the latest fad.
DR. BURSTONE I guess that is what we've always referred to as orthodontic judgment. We must weigh many factors to arrive at the best solution for our individual patients. With the use of computers, we now can make many measurements and do a more complete analysis, but judgment and maturity are still required in looking at esthetics.
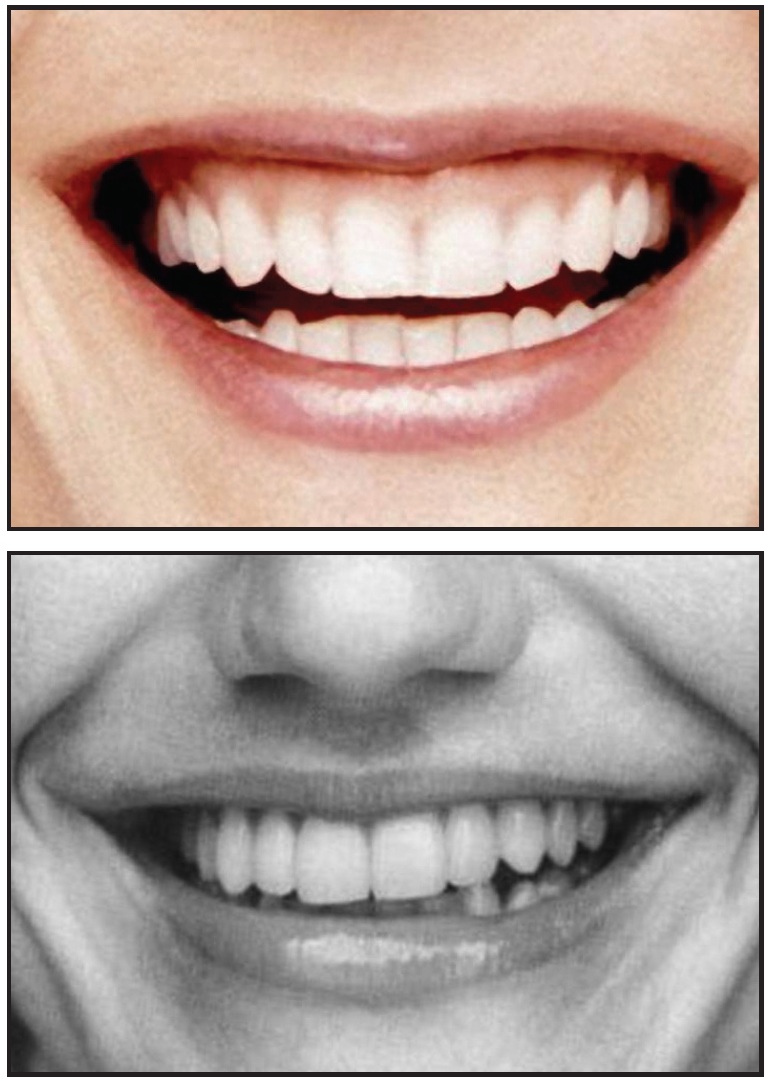
Fig. 7 Two well-known actresses who are generally considered to have attractive smiles display posterior “black holes”. Actress with considerable gingival display during smiling does not have vertical problem, but is simply good at simulating natural smile, which brings upper lip superiorly.
REFERENCES
- 1. Burstone, C.J.: The integumental profile, Am. J. Orthod. 44:1-25, 1958.
- 2. Burstone, C.J. and Marcotte, M.R.: Problem Solving in Orthodontics: Goal-Oriented Treatment Strategies, Quintessence, Chicago, 2000.
- 3. Burstone, C.J.: Integumental contour and extension patterns, Angle Orthod. 29:93-104, 1959.
- 4. Burstone, C.J.: Lip posture and its significance in treatment planning, Am. J. Orthod. 53:262-284, 1967.
- 5. Farkas, G.L. and Munro, I.R.: Anthropometric Facial Proportions in Medicine, C.C. Thomas, Springfield, IL, 1987, pp. 57-76.
- 6. Langlois, J.H. and Roggman, L.A.: Attractive faces are only average, Psychol. Sci. 1:115-121, 1990.
- 7. Langlois, J.H.; Roggman, L.A.; and Musselman, L.: What is average and what is not average about attractive faces? Psychol. Sci. 5:214-220, 1994.
- 8. Perrett, D.I.; May, K.A.; and Yoshikawa, S.: Facial shape and judgements of female attractiveness, Nature 368:239-242, 1994.
- 9. Fink, B.; Grammer, K.; and Thornhill, R.: Human (Homo sapiens) facial attractiveness in relation to skin texture and color, J. Comp. Psychol. 115:92-99, 2001.
- 10. Burt, D.M. and Perrett, D.I.: Perceptual asymmetries in judgments of facial attractiveness, age, gender, speech and expression, Neuropsychologia 35:685-693, 1997.
- 11. Makeig, S.; Bell, A.J.; Jung, T.P.; and Sejnowski, T.J.: Independent component analysis of electroencephalographic data, in Advances in Neural Information Processing Systems, vol. 8, ed. D.S. Touretzky, M.C. Mozer, and M.E. Hasselmo, MIT Press, Cambridge, MA, 1996, pp. 145-151.
- 12. Rubenstein, A.J. et al.: Why do infants prefer attractive faces? poster presentation, Society for Research in Child Development, Washington, March 1997.
- 13. Rubenstein, A.J.; Kalakanis, L.; and Langlois, J.H.: Infant preferences for attractive faces: A cognitive explanation, Devel. Psychol. 35:848-855, 1999.
- 14. Ekman, P.; Davidson, R.J.; and Friesen, W.V.: The Duchenne smile: Emotional expression and brain physiology, II, J. Pers. Soc. Psychol. 58:342-353, 1990.
- 15. Moore, T.; Southard, K.A.; Casko, J.S.; Qian, F.; and Southard, T.E.: Buccal corridors and smile esthetics, Am. J. Orthod. 127:208-213, 2005.
- 16. Roden-Johnson, D.; Gallerano, R.; and English, J.: The effects of buccal corridor spaces and arch form on smile esthetics, Am. J. Orthod. 127:343-350, 2005.
-
 DR. NANDA
DR. NANDA -
 DR. BURSTONE
DR. BURSTONE
Dr. Burstone is Professor Emeritus and Dr. Nanda is Professor and Head, Department of Craniofacial Sciences, Alumni Endowed Chair, Division of Orthodontics, School of Dental Medicine, University of Connecticut, Farmington, CT 06032. Dr. Nanda is also an Associate Editor of the Journal of Clinical Orthodontics. E-mail Dr. Nanda at nanda@nso.uchc.edu.