JCO INTERVIEWS
Dr. Birte Melsen on Adult Orthodontic Treatment
DR. CACCIAFESTA Prof. Melsen, I feel a bit humbled to be interviewing you for JCO, since I was one of your residents at the University of Aarhus from 1996 to 1999. Is it true that your practice in Germany is now limited to adult orthodontics?
DR. MELSEN Yes, I actually started my office in Germany about 15 years ago. At that time there was a center in Germany (IFZ Lubeck) where I was giving a course once or twice a year, demonstrating treatment of adult patients. At a certain point, it became clear that the patients we used for demonstration had to be completed, and since I had become well acquainted with my colleagues running the course center, I agreed to work there once a month. Since then, I have basically been seeing adult patients needing interdisciplinary treatment. This has given me a good experience in working with different colleagues and sharing responsibilities regarding treatment of patients. I collaborate with colleagues in the office as well as colleagues from other cities in Germany, who refer to me their adult patients for preprosthetic orthodontic preparation.
DR. CACCIAFESTA Have you seen an increase in the number of adults seeking orthodontic treatment?
DR. MELSEN In the United States, there seems to be a constant increase in the number of adults seeking treatment. In the European countries, it varies from place to place. This variation is partly caused by the socioeconomic situation of the population, but also by the availability of adult orthodontics and the awareness of the benefits of having your own teeth throughout life.
DR. CACCIAFESTA In 2001, you published an article on tissue reaction to orthodontic tooth movement.1 Can you explain the "new paradigm" that you described?
Similar articles from the archive:
DR. MELSEN When I got involved in research related to bone biology, I could not help wondering why orthodontists generate resorption by adding pressure, whereas orthopedic surgeons cause an apposition by putting a surface under pressure. We can gain bone by loading in the fitness center, and we lose bone by unloading when we go into space. By looking at the orthodontic tissue reaction in more detail, it became clear to me that what we are producing is probably two reactions--two cascades--occurring simultaneously: one in the bone and one in the periodontal ligament. The activity on the alveolar surface is most likely monitored by osteocytes, as in the rest of the skeleton.
As early as 1961, Epker and Frost indicated that a change in the curvature of the alveolar wall may be the factor that releases what is happening on the "tension" side.2 The reaction on the "pressure" side depends on the force level. When one occludes on a tooth, the periodontal fibers are stretched, thereby loading the alveolar bone--a physiological loading. When the tooth is displaced orthodontically within the periodontium without generating ischemia, it can be demonstrated by finite element analysis that the bone on the so-called "pressure" surface is not loaded during occlusion3,4 (Fig. 1). The direct resorption can be compared to a remodeling that occurs as a result of unloading. In the case of higher forces resulting in indirect resorption, ischemia will lead to hyalinization of the periodontal ligament, but also to necrosis of the lining cells needed for the vitality of the underlying bone's osteocytes. The indirect resorption can therefore be perceived as a repair with the purpose of removing necrotic tissue.
DR. CACCIAFESTA How does the finite element method help us study orthodontic tooth movement?
DR. MELSEN The stress and strain developed in the periodontium during orthodontic loading and during occlusion can be simulated by finite element analysis. This method was introduced into dental biomechanics in the '70s, but in some studies it was treated as a magic box, thus producing results that were not meaningful. When correctly used, finite element analysis is a very powerful tool to calculate the loading condition in structures characterized by a complex morphology, where the calculation of the stress and strain fields may be almost impossible using an analytical approach. Therefore, finite element analysis is well suited to studying the complexity of load transfer in the periodontium. For valid results, it is of the utmost importance to generate models that are accurate in respect both to morphology and to the material properties of the various tissues. Once the model is well built, the results can provide answers regarding the mechanism of orthodontic tooth movement. The model we have been using is based on micro-CT and the realistic, non-linear behavior of the PDL (Fig. 2).
DR. CACCIAFESTA What PDL, bone, and local modifications occur with aging?
DR. MELSEN There is a progressive reduction of the periodontium, an increase in the root-crown ratio, and a decrease in the resistance to spontaneous tooth migration. The changes in the PDL depend on the function of the individual teeth, but it is obvious that the initial reaction to orthodontic loading is delayed, whereas tooth displacement, once started, can be performed in the same way as in young patients--taking the reduced periodontium into consideration, of course.
DR. CACCIAFESTA How is the center of resistance of periodontally involved teeth affected by such modifications?
DR. MELSEN The center of resistance of periodontally involved teeth is affected in several ways. First of all, it is moving apically according to the marginal bone level, but other changes are occurring, such as an increase in bone porosity, especially at the marginal aspect (Fig. 3). The displacement of the center of resistance therefore depends not only on the marginal bone level, but also on the force level applied to the teeth.
DR. CACCIAFESTA Are there any age or anatomical limitations to orthodontic tooth movement in adults? Any contraindications?
DR. MELSEN So far, we haven't really reached the limit. Both Dr. Bjorn Zachrisson5 and I have been treating patients with very limited bone, and we have observed them over many years. It seems as if you can maintain teeth and the bone level over many years, even in the case of severe bone loss. However, one precondition is that the periodontium has to be healthy when the tooth movement is initiated, both at a clinical and a subclinical level--meaning that no necrotic cementum or calculus should be present. Therefore, we recommend that a modified Widman flap surgery be performed when the pockets are more than 4mm (Fig. 4).
There is a definite difference whether you want to move teeth or just want to keep them stable. If you only want to keep them stable, you can probably maintain the teeth over longer periods without reducing the pockets to 4mm. This has been shown by several periodontologists.6-10 The situation is entirely different when the tooth has to be moved, because the tissue reaction can be compared to a sterile inflammation. An exception may be when teeth have to be extruded.
DR. CACCIAFESTA How do your treatment objectives for adults differ from those for adolescents?
DR. MELSEN The treatment objectives for adults are almost always compromises. They cannot be ideal, because adult teeth are characterized by wear, abrasion facets, fillings, and changes in the local morphology of the periodontium--in addition to the loss of periodontium, which cannot be regained during orthodontic treatment. The cost/benefit ratio of doing orthodontics as part of a reconstruction should be evaluated. The effectiveness of the prosthetic reconstruction, which is almost always necessary, should also be taken into consideration.
DR. CACCIAFESTA Is this a multidisciplinary or an interdisciplinary approach?
DR. MELSEN A multidisciplinary approach means that various disciplines are involved without necessarily interacting. On the other hand, an interdisciplinary approach indicates that you have an ongoing interaction between the disciplines. In other words, in a multidisciplinary approach, one plus one is two, whereas in an interdisciplinary approach, each of the disciplines can stretch the capability of the other, so that one plus one may add up to much more than two. Therefore, it is the interdisciplinary approach that is needed.
DR. CACCIAFESTA What is your treatment protocol for periodontally involved patients?
DR. MELSEN The treatment protocol is pretty rigid. The most important part is to obtain a healthy periodontal status before treatment is initiated, and to ensure that the patients are able and willing to maintain the necessary hygiene program during and after treatment. So far we have done the treatment plan two-dimensionally with a combination of occlusograms and profile radiographs. We are in the process of changing that protocol now, working up to a three-dimensional, virtual treatment goal on the digital models, whereby we describe the tooth displacements necessary to obtain the goal. This will allow us to calculate the most efficient force system and design the individual appliances. It is very important to avoid "round-tripping" in periodontally involved patients, and as a general rule, vertical control is also of utmost importance.
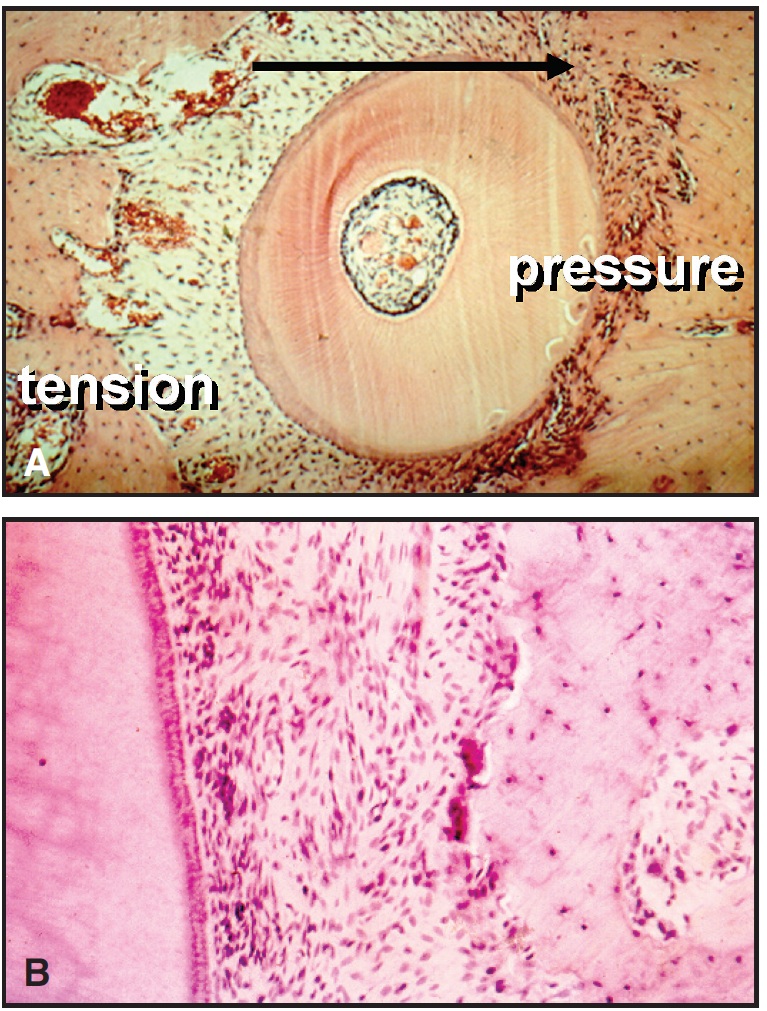
Fig. 1 A. Histologic image of tooth displacement. On “pressure” side, fibers are curled due to root displacement within viscoelastic membrane. When tooth is loaded by forces of mastication, fibers cannot be stretched, so that bone on “pressure” side is not loaded. Resorption can therefore be seen as remodeling in reaction to unloading. B. Histologic image of “pressure” zone. Note irregularity of fibers, which would normally be stretched when tooth is subjected to occlusal loading.
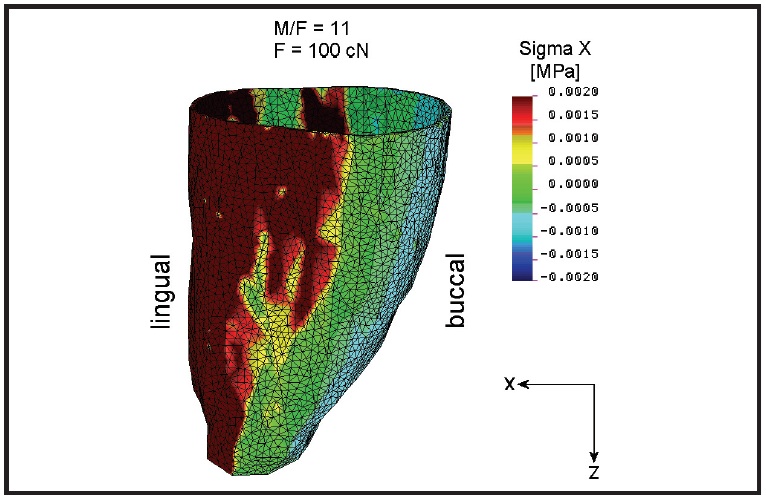
Fig. 2 Finite element model of strain on alveolar wall when tooth is displaced by translation (courtesy of P. Cattaneo). Dark red area shows tension strain, dark blue area indicates compression strain, and light blue and green areas reflect low strain where tissue is unloaded.
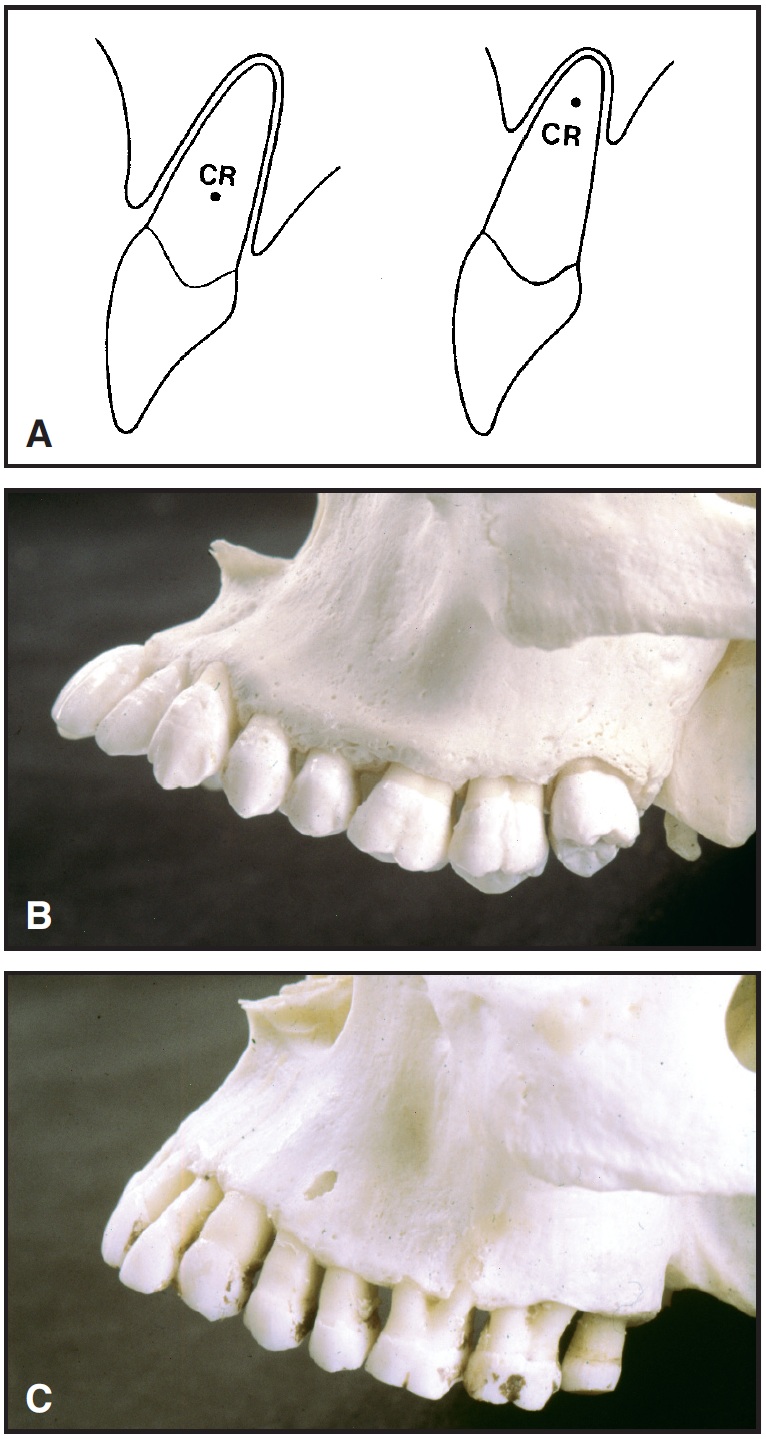
Fig. 3 A. Displacement of center of resistance with apical displacement of alveolar bone. B. In skull of young individual, enamel cementum border is close to marginal bone level. C. In skull of older individual, note apical displacement of marginal bone and multiple fenestrations of alveolar bone.
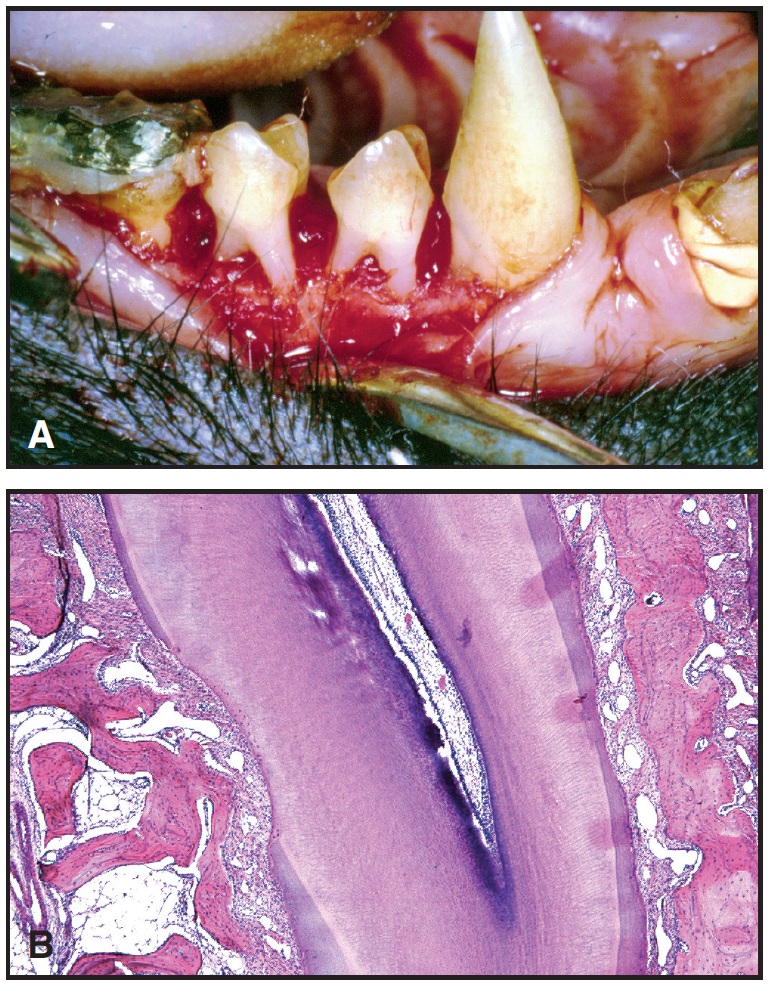
Fig. 4 A. Widman flap surgery performed on Macaca fascicularis monkey after development of 4-5mm pockets. B. Histologic image demonstrating formation of new attachment above notch made during surgery to indicate level of attachment before orthodontic intrusion.
A lot of attention has been focused on the idea that intrusion of the upper incisors may "age" these patients. However, the secondary malocclusion is frequently developed through eruption combined with migration of periodontally involved teeth. The most reasonable treatment would be to re-intrude these teeth. Any extrusion of teeth in the buccal segments will worsen the sagittal relationships, and it is still crucial in the treatment of periodontally involved patients to avoid changes in the lower facial height and to gain new attachment, which we have proved possible. Reattachment can be generated through intrusion, and even more can be gained with guided tissue regeneration (GTR), as recently shown by Diedrich in animal experiments.11,12 Patients treated with intrusion back in the late '70s and the '80s have now been out of treatment for more than 30 years, and many of these patients have maintained their treatment results (Figs. 5 and 6).

Fig. 5 A. 38-year-old male patient with severe attachment loss and long clinical crowns before treatment. B. Intrusion of most extrusive and protrusive tooth with three-piece mechanics. C. Intrusion of three incisors. D. After intrusion. E. Cast retainer with built-up lingual tuberculum. F. Five years after treatment. G. 15 years after treatment.
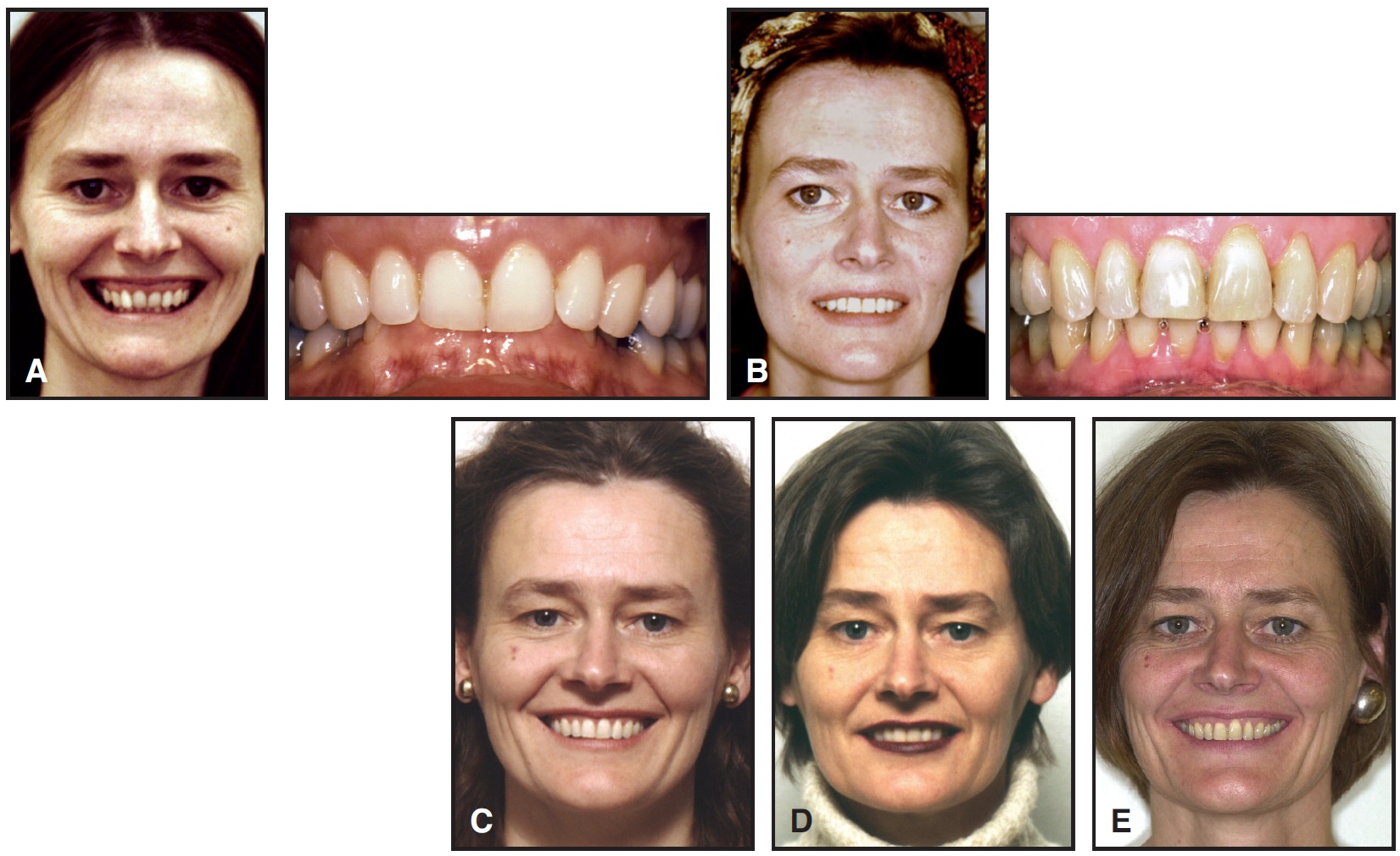
Fig. 6 A. Adult female patient with deep bite and gummy smile before treatment. B. After intrusion of upper incisors. C. Five years after treatment. D. 10 years after treatment. E. 20 years after treatment.
DR. CACCIAFESTA How much expansion can the periodontium tolerate?
DR. MELSEN We are not completely sure. It seems that with our current self-ligating brackets and thin nickel titanium wires, the periodontium can tolerate much more expansion than we anticipated. On the other hand, many colleagues are critical of this approach. Right now we are in the midst of performing a NewTom* study whereby we can evaluate the amount of bone deposits occurring around the teeth in all dimensions before and after treatment. I think we will be better able to answer that question in a year or so.
DR. CACCIAFESTA What are the indications for bodily labial movement of mandibular incisors? How do you achieve this movement, and what is the long-term stability?
DR. MELSEN For bodily labial movement of the incisors, the biotype must be correct--meaning the gingiva and bone are not too thin, and you do not have a "washboard" effect from the beginning. If the biotype is acceptable, you can move the incisors forward, which would frequently be an advantage in adult patients as a means to correct an increased overjet. Retraction of the upper incisors is always going to "age" the face. Dr. Allais did his thesis on this topic; we looked at 150 consecutively treated patients and found that the side effects were limited to a very few patients, and highly related to hygiene and biotype, not to the amount of forward movement of the incisors.13,14 To us, opening space for a third premolar would therefore be a way of treating a large overjet, instead of extracting two premolars in the upper jaw (Fig. 7). In Aarhus, long-term stability in our adult patients is managed by both biological and mechanical means. The mechanical maintenance is a 4-4 bonded retainer, or filling in the opened space with a bridge or an implant. The biological maintenance is the maintenance of the periodontium--the same as after any major periodontal treatment.
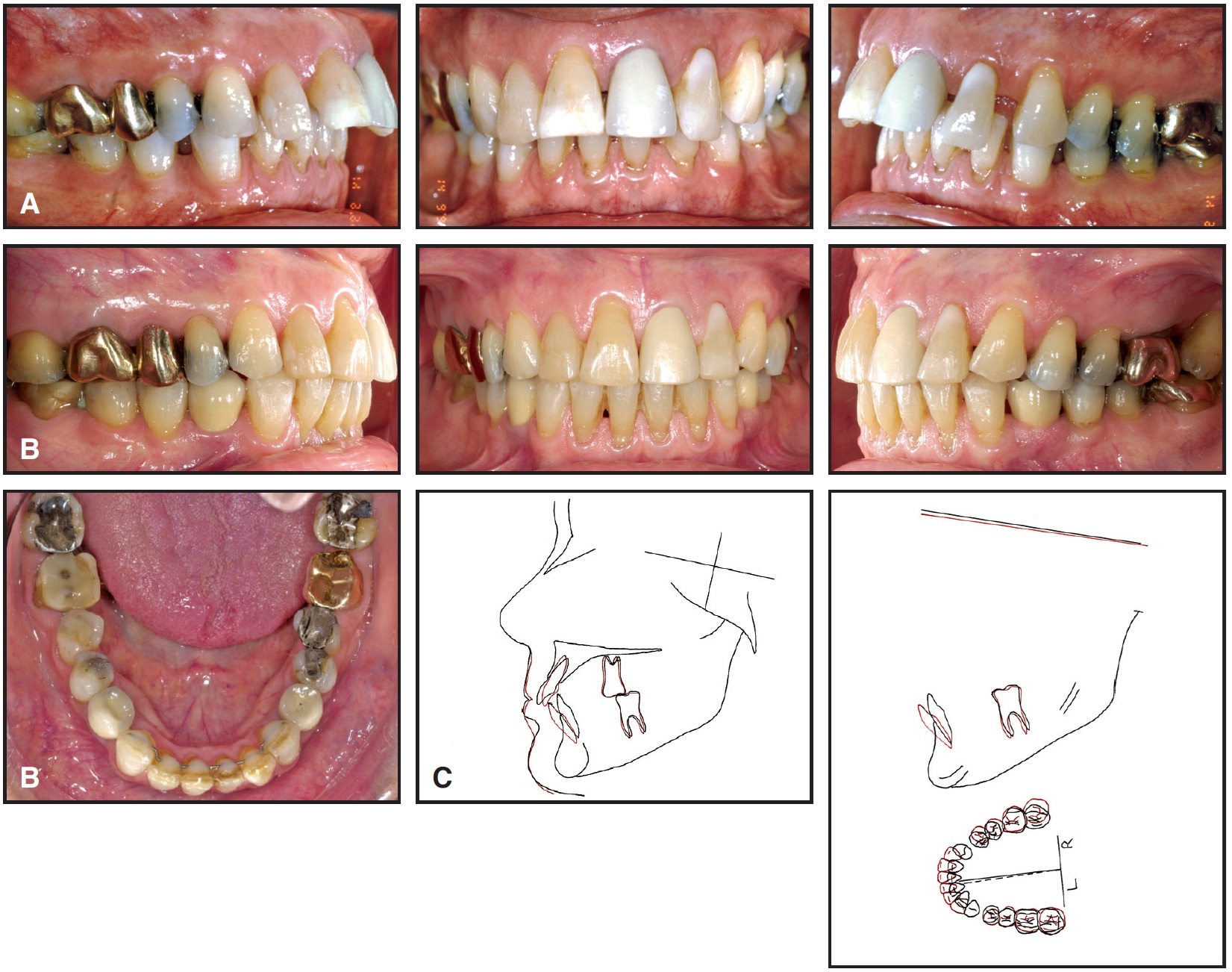
Fig. 7 A. Patient with excessive overjet and buccal spacing following extraction of first molars. Note gingival recession around lower incisors. B. After substantial forward movement of lower incisors, opening space for three premolars. C. Superimposition of cephalometric tracings before and after treatment.
DR. CACCIAFESTA What are the principles of absolute anchorage in adults? How do you achieve stable anchorage?
DR. MELSEN In adults, it is very important to differentiate between the active unit--the teeth to be moved--and the reactive unit--the teeth we use as anchorage. Stability of the anchorage unit can be obtained in many ways. The best anchorage is, in my opinion, a good, stable occlusion. The patient's sense of occlusion is very fine, and even minor changes in occlusion will be perceived immediately. Therefore, we encourage the patient to chew as much as possible and to tell us when the anchorage is changing. We add thin layers of light-cured acrylic on the occlusal surfaces to make the occlusion not only point-to-point, but really surface-to-surface.
DR. CACCIAFESTA Do you ever use headgear for reinforcing anchorage in adults?
DR. MELSEN We would never dream of using headgear to reinforce anchorage. We have recently demonstrated that although teeth can be displaced distally, they are always moving back to the position where they can best transfer occlusal forces to the cranial base. A headgear contributes to a jiggling of the teeth, because the force is not acting 24 hours a day, and a jiggling of the molars has a detrimental effect on the incisors as well.
DR. CACCIAFESTA Is it possible to distalize the molars in adults?
DR. MELSEN Yes, you can distalize molars in adults, but as I said, it is never stable. All you can do is to reposition a mesially tipped or rotated molar.
DR. CACCIAFESTA I have heard you talk about the "Iron Cross". What is that device, and when do you use it?
DR. MELSEN An Iron Cross is a reinforcement of the transpalatal bar used for the stabilization of the lateral segments across the palate (Fig. 8). We use it to reinforce the impact of occlusion on anchorage, especially where you have a loss of teeth.
DR. CACCIAFESTA Do you use ankylosed teeth as absolute anchorage? If so, how do you align the ankylosed teeth after anchorage reinforcement?
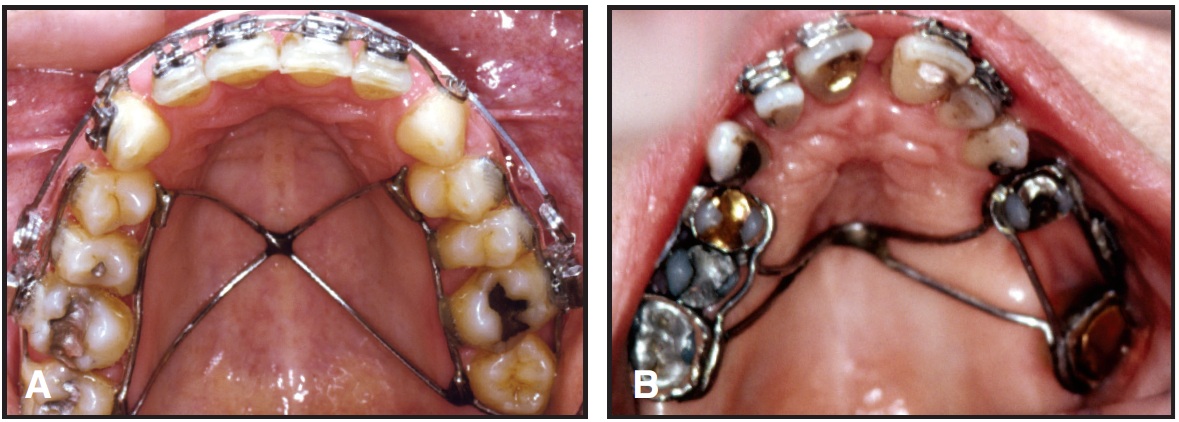
Fig. 8 A. Bonded Iron Cross made from .032" round stainless steel wire. B. Iron Cross welded to molar and premolar bands.
DR. MELSEN Yes, we do use ankylosed teeth as absolute anchorage. They are usually deciduous teeth in cases of agenesis of permanent teeth. But since you want to close the spaces completely, you can only use them for a certain time. The alignment of an ankylosed tooth that has been used for anchorage has to be done by the surgeon, as in a recent paper where we used an ankylosed incisor to correct a distal occlusion before we made a local osseodistraction of the incisor segment.15
DR. CACCIAFESTA What do you mean by the concept of "free anchorage"?
DR. MELSEN There is an old saying that there is no free lunch, but there may be free anchorage--namely, teeth you want to extract. This may be in a case with an asymmetry where you want to extract teeth, either on both sides or on only one side. You can design the appliance so that you can use the tooth to be extracted as free anchorage for the correction of the asymmetry (Fig. 9).
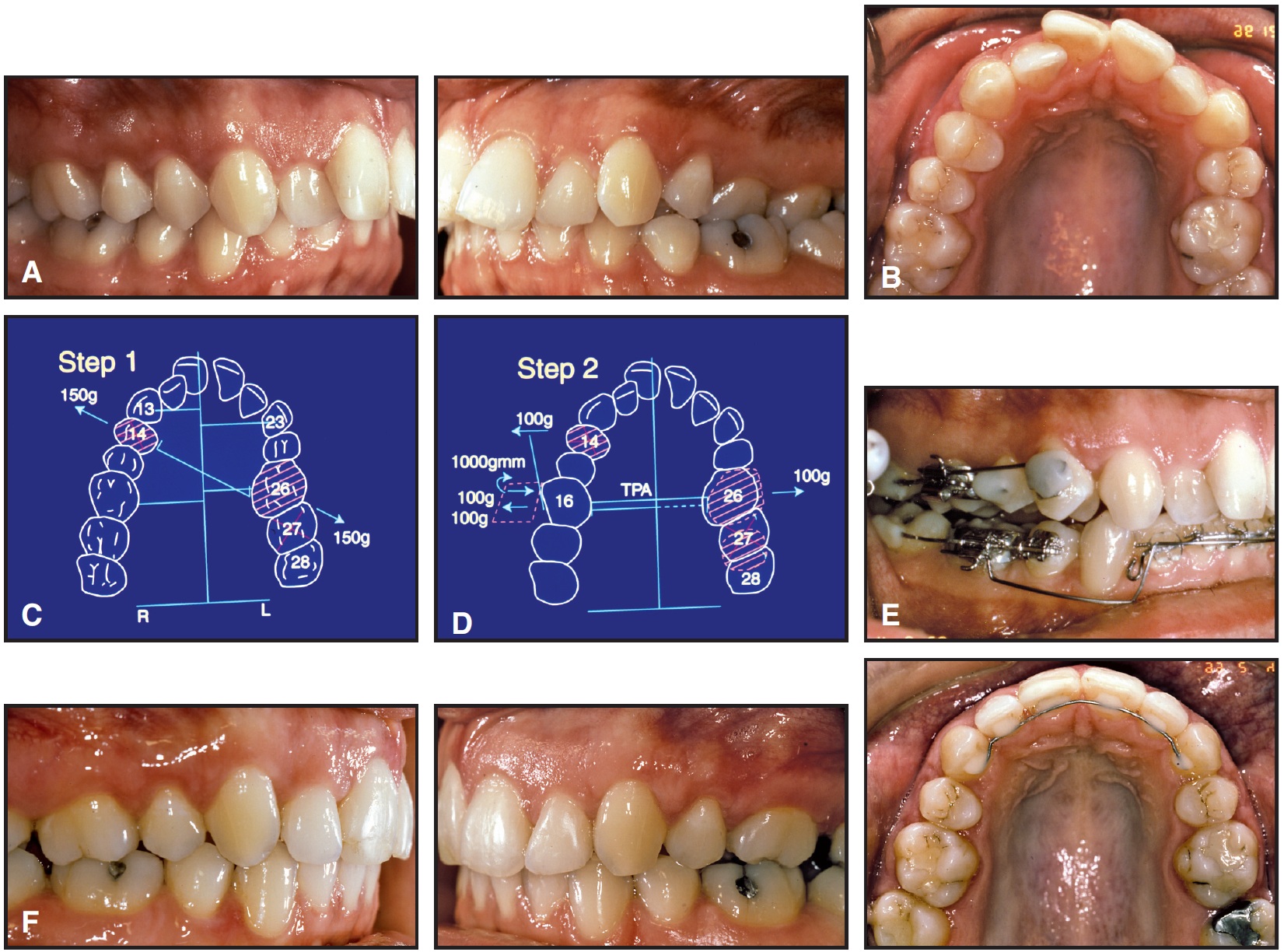
Fig. 9 A. Patient with posterior crossbite on left side. Intermaxillary forces could not be used because of TMD resulting from forced bite. B. Asymmetrical upper arch created by left first premolar extraction. C. Left first molar displaced distally and buccally. D. Transpalatal expander placed between molars during second phase of treatment, with buccal force on right side transferred to first premolar by cantilever. E. Right first premolar displaced into scissor bite before being extracted. F. Patient after treatment.
DR. CACCIAFESTA When do you use osseointegrated implants for absolute anchorage instead of miniscrews?
DR. MELSEN Osseointegrated implants can be very useful if they are part of a later reconstruction and can be inserted before orthodontic treatment (Fig. 10). A different type of osseointegrated implant would be the palatal implant, which we are using in some cases, but not nearly as frequently since the introduction of the mini-implants. The palatal implants are short and rather large in diameter, and they have to be osseointegrated before they can resist the magnitude of forces to which they are submitted. These implants are connected to adjacent teeth and thus used for indirect anchorage, or are used instead of a headgear. But as I mentioned, we do not use headgear anyway. We have used these palatal implants occasionally in cases of agenesis or in adult patients with a limited number of teeth.

Fig. 10 A. Patient after extraction of lower left first and second molars. B. First molar replaced with implant for anchorage during third molar movement. Mesial displacement of third molar initiated with nickel titanium coil spring between two power arms, bringing line of action below CR for molar uprighting. Extrusive force was expected to be neutralized by occlusal forces. C. Two-cantilever mechanics used after mesial molar movement for intrusion and uprighting. Cantilever from auxiliary molar tube delivered large moment and undesirable extrusive force (a), which was neutralized by second cantilever from implant to distal extension from molar tube (b). Because intrusive force was slightly greater than extrusion from uprighting, net movement was uprighting and intrusion. D. Patient after treatment.
DR. CACCIAFESTA You published an article some time ago on zygoma wires.16 Can you tell us more about this procedure?
DR. MELSEN The zygoma wire was actually developed out of necessity, when my periodontist wanted me to reduce a large overjet in a patient with only two upper molars. With no opposing molars in the lower jaw, we decided that a surgical wire through the zygoma could be used for anchorage. We used the zygoma ligatures as anchorage in 15 cases, but 20% of the ligatures worked their way through the bone and became loose before the requirements for anchorage were fulfilled. This was an inexpensive way of obtaining anchorage, but the zygoma ligatures have now been replaced by the mini-implants.
DR. CACCIAFESTA What are the clinical advantages of miniscrews compared to other anchorage systems?
DR. MELSEN Mini-implants have entered the market with great impact. In principle, all types of tooth movement can be accomplished with mini-screw anchorage, but I do not like to use skeletal anchorage as the solution to all problems. I think it should be limited to the cases you cannot treat with conventional appliances; therefore, the role of mini-implants is to widen the indications for orthodontics. For example, they can be used in patients with insufficient teeth for conventional anchorage and in cases where the forces acting on the reactive units are detrimental, as with severe asymmetries (Fig. 11).
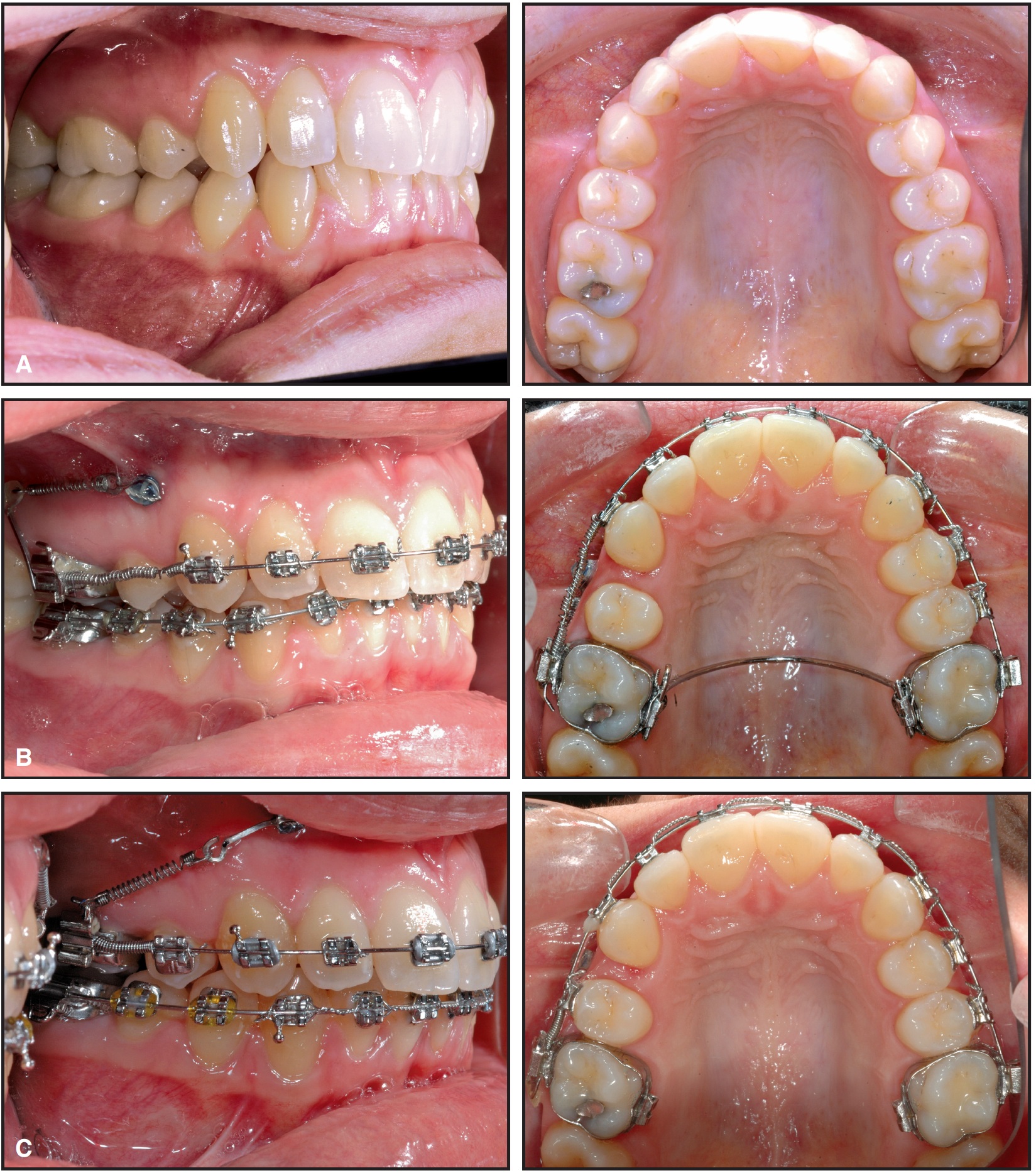
Fig. 11 A. Patient with asymmetrical upper canines after extraction of right first premolar. B. Mini-implant used to hold right first molar position while canine and second premolar were moved forward against molar anchorage. C. Treatment progress.
DR. CACCIAFESTA Are miniscrews absolutely stable after loading?
DR. MELSEN Yes; if you can obtain primary stability, you can maintain it. In cases where you do not have primary stability, it is very doubtful whether you will ever get it, even if you leave the implant unloaded. If you have primary stability, I see no reason why you cannot load the implant with a limited force immediately after insertion. Implants that are not loaded by orthodontic forces are subject to forces acting on the bone, because they have a different stiffness than the surrounding bone. However, it seems that the line of action of the force should not create major torsion, as the shearing forces tend to loosen the mini-implants.
DR. CACCIAFESTA Do miniscrews become osseointegrated?
DR. MELSEN If by osseointegration you mean bone-to-implant contact, yes, we do get an increased bone-to-implant contact. The mini-implants are still called non-osseointegrated by some colleagues because the intraosseous part is polished. The surface contact is therefore less than with implants that are surface-treated or coated. The smooth surface of the implant does allow it to be unscrewed without great difficulty and without a surgical intervention.
DR. CACCIAFESTA When do you prefer to start with a lingual approach?
DR. MELSEN It all depends on what type of tooth movement I want. If the necessary line of action can best be obtained on the lingual surface, we would use lingual for good biomechanics more than for esthetics.
DR. CACCIAFESTA How do you treat patients with infrabony defects?
DR. MELSEN Moving a tooth through a bony defect is different from moving a tooth with an infrabony defect. A tooth with a vertical defect should generally be extruded so that the vertical defect is filled in, or it should be treated for the vertical defect before becoming involved in orthodontic tooth movement. Moving a tooth through an infrabony defect following, for instance, an extraction with bone loss, is absolutely possible. Tooth movement builds up bone, whereas implants need bone.
DR. CACCIAFESTA What is your protocol after guided tissue regeneration? When do you start moving a tooth through a regenerated area?
DR. MELSEN After GTR, we usually start the treatment the day the sutures are removed, and the movement will be a combination of a slight intrusion and a sagittal movement.
DR. CACCIAFESTA Is it possible to move a tooth through an edentulous area?
DR. MELSEN When I want to move a tooth through an edentulous area, it is important to avoid tipping the tooth into the region; the roots should, in principle, be moved ahead of the crown. This builds up bone by exerting a slight pressure, thereby increasing the density of the bone ahead of the tooth (Fig. 12).
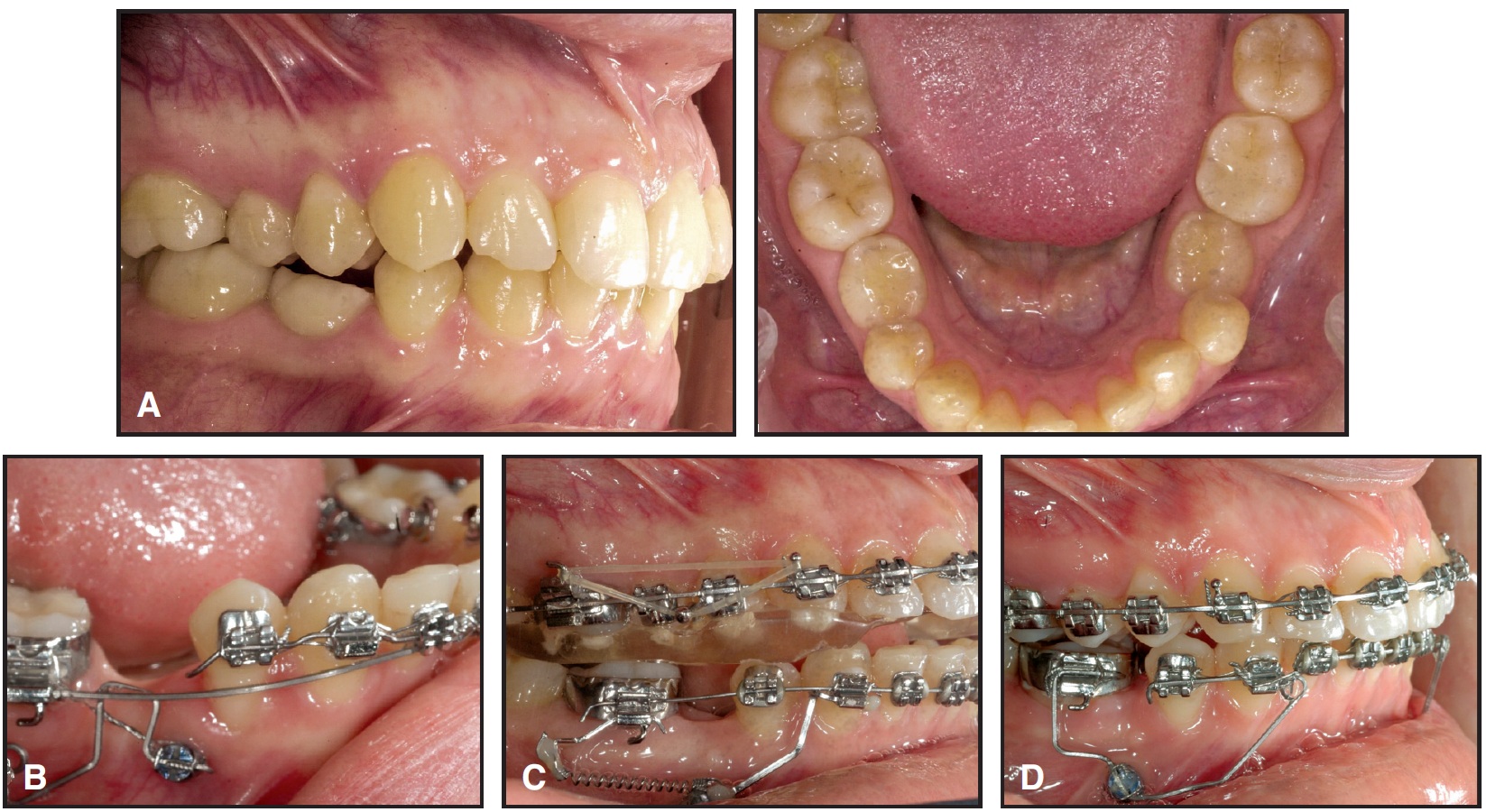
Fig. 12 A. Class II patient with agenesis of two lower premolars. B. Aarhus mini-implant placed in alveolar process to hold lower right first molar position during mesial displacement of incisors and canines. C. Mini-implant used as anchorage for mesial displacement of molar through atrophied alveolar process. D. Mini-implant used as anchorage for 1st- and 2nd-order molar correction and alignment of lower midline.
DR. CACCIAFESTA Are there any limitations?
DR. MELSEN The only limitations I know of are related to the hygiene and periodontal health of the area, and also that the tooth movement should be done with a sufficiently low and well-controlled force.
DR. CACCIAFESTA What do you mean by "movement with bone" or "movement through bone"?
DR. MELSEN Movement through bone can always be obtained, as long as the tooth is displaced within the given alveolar process. When teeth have to be moved into areas with an atrophic alveolar process due to extraction of teeth, a balance between resorption and apposition has to be kept, and the tooth is, so to speak, "carrying its alveolus along".
DR. CACCIAFESTA Is it possible to move a tooth through the maxillary sinus?
DR. MELSEN When you are moving teeth with bone, you can also move them through the maxillary sinus, as we showed 15 years ago.17
DR. CACCIAFESTA How do you perform orthodontic tooth movement of periodontally involved teeth?
DR. MELSEN Tooth movement of periodontally involved teeth has to be done with a minimum of jiggling, meaning that you have to know exactly where you are going, which again indicates that you have to work with segmented appliances where the forces are controlled in all three dimensions.
DR. CACCIAFESTA Do you advocate intrusion or extrusion of teeth with a compromised periodontium?
DR. MELSEN You can use both intrusion and extrusion. When you have a horizontal bone loss, you can use intrusion and regain some lost attachment. Extrusion would be recommended if you have a vertical defect that cannot be treated. The tooth movement will thus help you build up the bone, but, of course, will generate a very long crown and probably require endodontic treatment of the tooth before reconstruction. The need for leveling of the bone would be an indication for extrusion of periodontally involved teeth. Indications for intrusion would be a deep bite and elongated, flared anterior teeth with horizontal bone loss.
DR. CACCIAFESTA How do you intrude periodontally involved teeth?
DR. MELSEN I generally do not intrude periodontally involved teeth. Our animal experiments have shown that it is very detrimental, and all you actually obtain is a reduction of alveolar height without gaining more support for the tooth. When we have to intrude periodontally involved teeth, our force level is as low as we can control it, often down to about 10-12g per tooth, or 50g for four incisors. The appliance is always segmented, and we would most likely use cantilever mechanics. The configuration of the cantilever would be determined by the direction in which the tooth is being displaced, and the line of action of the forces compared to the center of resistance determines the type of intrusion (Fig. 5).
DR. CACCIAFESTA How do you avoid vertical extrusion of a molar during uprighting?
DR. MELSEN Molar uprighting is most frequently done in combination with extrusion, which is fine if you want to finish the case with a bridge and you can lower the molar by placing a crown. If, on the other hand, you want to avoid the extrusion, you should use two-cantilever mechanics, which we have shown in several publications18-20 (Fig. 10).
DR. CACCIAFESTA Is it always possible to intrude molars?
DR. MELSEN We have shown that it is possible to avoid extrusion of lower molars and to intrude overerupted upper molars. I have not been able to intrude normally erupted molars or to correct a genetically determined open bite, as Dr. Sugawara has demonstrated.21
DR. CACCIAFESTA How do you maintain the results of adult treatment in the long term?
DR. MELSEN We actually leave it to the dentist responsible for the reconstruction and the periodontium of the adult patient to take responsibility for the final occlusion. We recommend that when the bone loss is extensive, a cast lingual retainer with tuberculae adjusted for articulation should be produced by the prosthodontist (Fig. 5E). We deliver the product, but the final result, as when you buy a car, depends on life-long retention and life-long maintenance. Other than diamonds, everything has to be maintained; true stability only occurs post mortem.
DR. CACCIAFESTA Prof. Melsen, thank you for an enlightening interview.
FOOTNOTES
- *Trademark of AFP Imaging Corp., 250 Clearbrook Road, Elmsford, NY 10523; www.aperioservices.com.
REFERENCES
- 1. Melsen, B.: Tissue reaction to orthodontic tooth movement—a new paradigm, Eur. J. Orthod. 23:671-681, 2001.
- 2. Epker, B.N. and Frost, H.M.: Correlation of bone resorption and formation with the physical behavior of loaded bone, J. Dent. Res. 44:33-41, 1965.
- 3. Cattaneo, P.M.: Orthodontic aspects of bone mechanics and bone remodeling, thesis, University of Aarhus, Aarhus, Denmark, 2003.
- 4. Cattaneo, P.M.; Dalstra, M.; and Melsen, B.: The finite element method: A tool to study orthodontic tooth movement, J. Dent. Res. 84:428-433, 2005.
- 5. Zachrisson, B.U. and Keim, R.G.: JCO Interviews Bjorn U. Zachrisson, DDS, MSD, PhD, on current trends in adult treatment, J. Clin. Orthod. 39:231-244, 285-296, 2005.
- 6. Badersten, A.; Nilveus, R.; and Egelberg, J.: 4-year observations of basic periodontal therapy, J. Clin. Periodontol. 14:438-444, 1987.
- 7. Badersten, A.; Nilveus, R.; and Egelberg, J.: Effect of nonsurgical periodontal therapy (VIII): Probing attachment changes related to clinical characteristics, J. Clin. Periodontol. 14:425-432, 1987.
- 8. Claffey, N.; Kelly, A.; Bergquist, J.; and Egelberg, J.: Patterns of attachment loss in advanced periodontitis patients monitored following initial periodontal treatment, J. Clin. Periodontol. 23:523-531, 1996.
- 9. Nordland, P.; Garrett, S.; Kiger, R.; Vanooteghem, R.; Hutchens, L.H.; and Egelberg, J.: The effect of plaque control and root debridement in molar teeth, J. Clin. Periodontol. 14:231-236, 1987.
- 10. Renvert, S.; Nilveus, R.; Dahlen, G.; Slots, J.; and Egelberg, J.: 5-year follow up of periodontal intraosseous defects treated by root planing or flap surgery, J. Clin. Periodontol. 17:356-363, 1990.
- 11. Diedrich, P.; Fritz, U.; Kinzinger, G.; and Angelakis, J.: Movement of periodontally affected teeth after guided tissue regeneration (GTR)—an experimental pilot study in animals, J. Orofac. Orthoped. 64:214-227, 2003.
- 12. Diedrich, P.R.: Orthodontic procedures improving periodontal prognosis, Dent. Clin. N. Am. 40:875-887, 1996.
- 13. Allais, D. and Melsen, B.: Does labial movement of lower incisors influence the level of the gingival margin? A case-control study of adult orthodontic patients, Eur. J. Orthod. 25:343-352, 2003.
- 14. Melsen, B. and Allais, D.: Factors of importance for the development of dehiscences during labial movement of mandibular incisors: A retrospective study of adult orthodontic patients, Am. J. Orthod. 127:552-561, 2005.
- 15. Kofod, T.; Wurtz, V.; and Melsen, B.: Treatment of an ankylosed central incisor by single tooth dento-osseous osteotomy and a simple distraction device, Am. J. Orthod. 127:72-80, 2005.
- 16. Melsen, B.; Petersen, J.K.; and Costa, A.: Zygoma ligatures: An alternative form of maxillary anchorage, J. Clin. Orthod. 32:154-158, 1998.
- 17. Melsen, B.: Limitations in adult orthodontics, in Current Controversies in Orthodontics, ed. B. Melsen, Quintessence, Chicago, 1991, pp. 147-180.
- 18. Fiorelli, G.; Melsen, B.; and Modica, C.: Two-vector mechanics, Prog. Orthod. 4:62-73, 2003.
- 19. Fiorelli, G. and Melsen, B.: Biomechanics in Orthodontics, CD-ROM, Libra Ortodonzia, Arezzo, Italy, 2002.
- 20. Melsen, B.; Fiorelli, G.; and Bergamini, A.: Uprighting of lower molars, J. Clin. Orthod. 30:640-645, 1996.
- 21. Sugawara, J.; Baik, U.B.; Umemori, M.; Takahashi, I.; Nagasaka, H.; Kawamura, H.; and Mitani, H.: Treatment and posttreatment dentoalveolar changes following intrusion of mandibular molars with application of a skeletal anchorage system (SAS) for open bite correction, Int. J. Adult Orthod. Orthog. Surg. 17:243-253, 2002.
-
 DR. MELSEN
DR. MELSEN -
 DR. CACCIAFESTA
DR. CACCIAFESTA
Dr. Melsen is Professor and Head, Department of Orthodontics, Royal Dental College, Aarhus University, Vennelyst Boulevard 9, DK-8000 Aarhus C, Denmark, and an Associate Editor of the Journal of Clinical Orthodontics; e-mail: orthodpt@odont.au.dk. Dr. Cacciafesta is an Assistant Clinical Professor, Department of Orthodontics, University of Pavia, Pavia, Italy. He is also in the private practice of orthodontics in Pavia; e-mail: vcacciafesta@hotmail.com.