JCO INTERVIEWS
Dr. Rohit C.L. Sachdeva on A Total Orthodontic Care Solution Enabled by Breakthrough Technology
DR. WHITE You have recently devoted all of your efforts to the development of what seems to be a revolutionary computer-based method of diagnosis and treatment. Could you tell us something about this system?
DR. SACHDEVA This Total Orthodontic Care Solution* provides orthodontists with a technology that delivers tremendous value throughout the entire care cycle--including diagnosis, treatment planning, therapy, monitoring of care, and patient communication. The process begins by obtaining a three-dimensional digital image of the dentition. This image is integrated with other patient records to establish a three-dimensional treatment objective. The treatment objective is then used to design and manufacture a custom appliance system that is specific to each patient's needs. The result is a comprehensive care solution that addresses many problems.
DR. WHITE What are some of the problems you see with traditional approaches to orthodontic care?
Similar articles from the archive:
DR. SACHDEVA Where should I begin? I think for the most part our profession recognizes how much variability there is in orthodontic care today. One of the first things we did when we began to develop this solution was to look at why variability exists. Let's consider the issue of diagnosis, since the hallmark of good treatment always begins with diagnosis. The challenge we have with diagnosis is that there has been no way to accurately measure complex three-dimensional anatomy. With our intraoral three-dimensional scanner (Fig. 1), we now have the capability to measure precisely the initial dentition, project and measure outcome, and monitor changes over the course of treatment.
DR. WHITE So the three-dimensional scanner allows you to accurately image the mouth and then to view the teeth at different points throughout treatment, in respect to their initial positions as well as to the treatment objective?
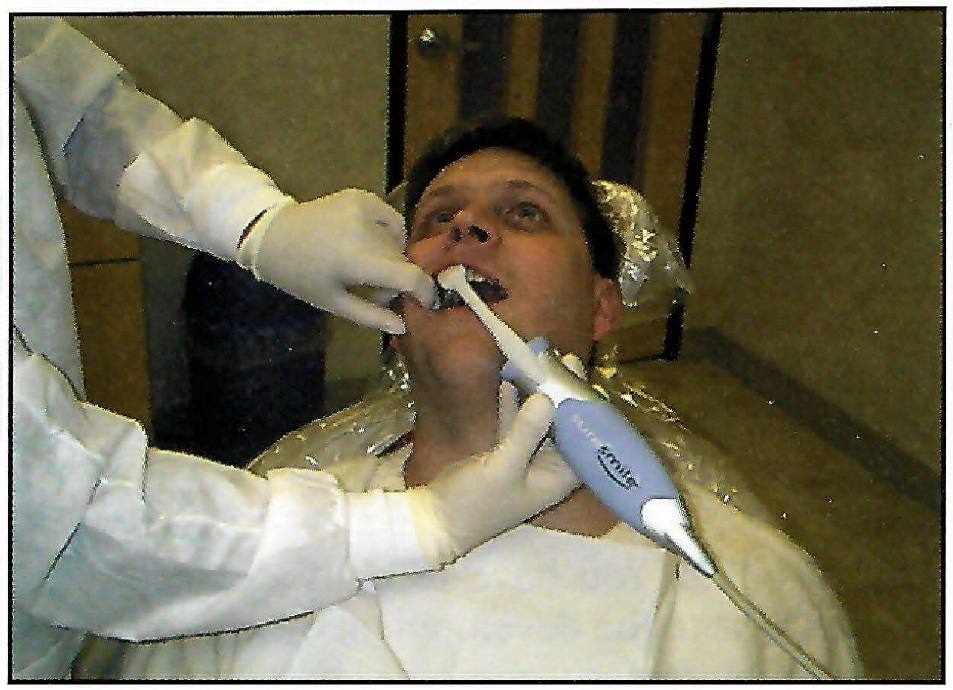
Fig. 1 Three-dimensional OraScanner* in use.
DR. SACHDEVA That is right.
DR. WHITE The ability to provide doctors with constant, immediate, and accurate feedback seems like a big breakthrough in itself.
DR. SACHDEVA We think so. For example, could you imagine a surgeon trying to provide the LASIK procedure without knowing how to measure the curvature of the eye? In order to know, we have to be able to measure accurately. In all honesty, we have never been able to measure precisely before. Our profession will benefit greatly from this.
DR. WHITE Is this a laser scanner?
DR. SACHDEVA No, it is a white-light scanner. It is noninvasive and can be used repeatedly on patients with no harmful effects. Therefore, the patient can be scanned at each visit so as to monitor treatment progress objectively. It could also reduce the number of mid-treatment x-rays needed, since root positions can be interpolated from the scan.
DR. WHITE The lack of objective feedback has certainly been a problem for orthodontists, because the biological changes of tooth movement occur so slowly that problems can creep up and establish themselves before the orthodontist is even aware of them?as with the loss of maxillary molar anchorage in extraction cases. There is no doubt that this feature is valuable, but how long does it take to scan the mouth?
DR. SACHDEVA After familiarization with the technique, the doctor or the assistant should be able to perform the initial, comprehensive full-mouth scan in no more than five minutes (Fig. 2). Sequential scans that are taken during the course of treatment should take less than 30 seconds. These can be superimposed on previous scans to provide the clinician with an accurate idea of how treatment is progressing.
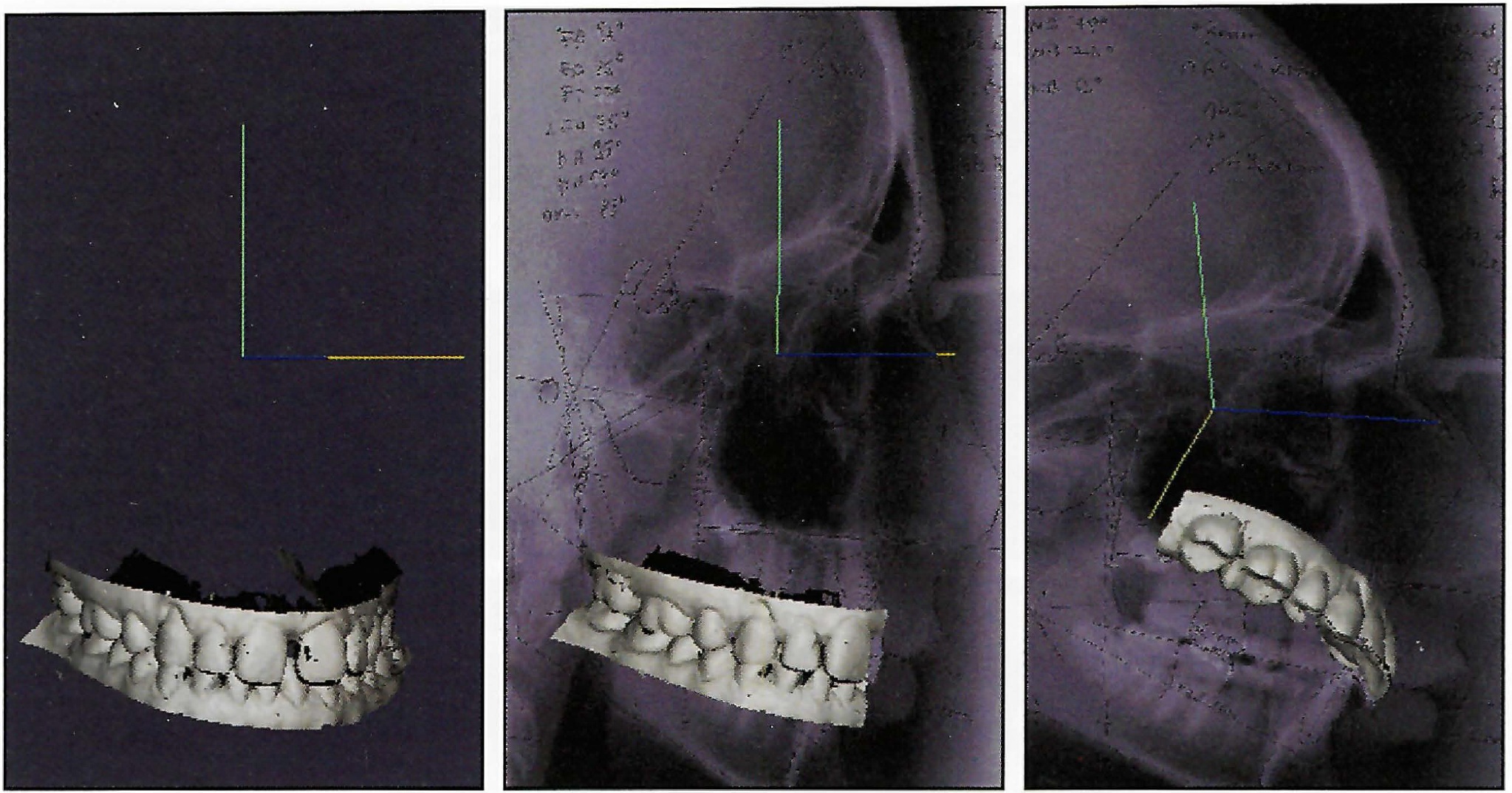
Fig. 2 OraScan* superimposed on image of cephalogram and rotated in three dimensions for viewing.
DR. WHITE So the inability to measure accurately has been a big problem, but what other problems does your technology address?
DR. SACHDEVA Another major problem, until now, has been the inability to ensure that our diagnostic knowledge and clinical intention would combine to produce the desired treatment outcome. Today, each stage of the process? diagnosis, treatment planning, appliance selection and application, and re-evaluation is conducted independently and not integrated effectively. Hence, this provides another source of variability. With our solution-based approach, we have applied technology to ensure that the orthodontist's diagnostic and clinical intentions are integrated throughout the entire process to consistently deliver the desired outcome.
DR. WHITE I can see where there will be a great deal of interest in the therapeutic part of this technology, but how much interest do you think you will create with the diagnostic part?
DR. SACHDEVA We believe strongly that the reason some orthodontists do not go through a more thoughtful diagnostic and treatment-planning exercise is because they do not perceive a direct benefit in its translation to a therapeutic device or delivery. Our approach has been to provide a tool that allows them to gain the full benefit of spending those minutes thoughtfully planning the case. Neither the diagnostic evaluation nor the therapeutic application, acting independently, can achieve a successful outcome. They have to be effectively integrated.
DR. WHITE Exactly how does the orthodontist plan treatment with your technology?
DR. SACHDEVA Let's begin by recognizing that the orthodontist will now have access to a computerized record that includes radiographic images, photographs, and the three-dimensional image of the dentition. These images are displayed in an easy-to-use format so that the clinician may easily define treatment objectives and generate various simulations representing different treatment scenarios (Fig. 3).
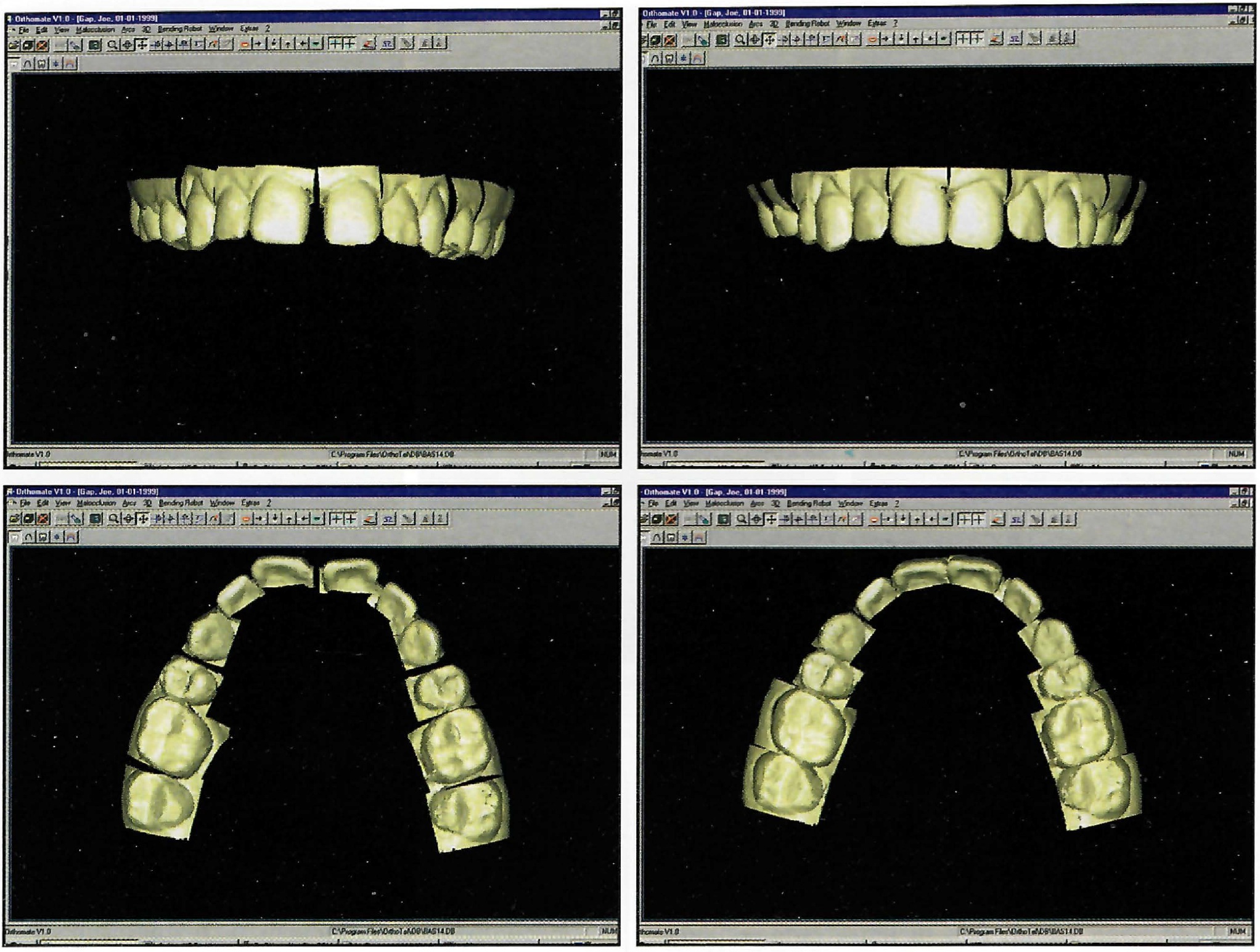
Fig. 3 Dynamic digital setup for initial and final positions.
DR. WHITE Will this be equivalent to a diagnostic setup or occlusograms?
DR. SACHDEVA Yes, but we will be able to develop multiple setups and depict different treatment scenarios. The clinician will select the desired setup, or the "preferred" scenario, and use this to define the "target" outcome. This then becomes the basis for measuring progress throughout the entire treatment.
DR. WHITE Are you integrating digital photographs or scanning in photos made with a single- lens reflex camera?
DR. SACHDEVA The technology is being developed to accommodate both approaches.
DR. WHITE So in total, you believe that the diagnostic and treatment planning capabilities you now have with the scanner and software will enhance the care patients receive?
DR. SACHDEVA Well, it is a good start. While we have provided the capability to measure and precisely diagnose and plan treatments, we have also enhanced our knowledge as it relates to the specific patient treatment needs. But using this knowledge to apply a specific therapy creates a new set of problems.
DR. WHITE Are you referring to the limitations of current fixed appliance systems?
DR. SACHDEVA Not only the systems, but also the manner in which we use them. Certainly, the preadjusted appliances offer some benefits. However, since all of them are currently based on average measurements, they do not allow precise tooth positioning. This problem is further complicated by the sensitivity to bracket placement and variation of tooth morphology. In summary, the preadjusted appliance as it now exists is not formulated for the individual needs of the patient. What we really need is an appliance system that furnishes patients with customized appliances.
DR. WHITE So teeth can be precisely positioned with this system, without the need for positioners and/or up-and-down elastics near the end of treatment?
DR. SACHDEVA Yes. Realize that positioners are limited to correcting minor vertical discrepancies and are generally ineffective in controlling torque or rotations, especially in the buccal segments. It is also difficult to esthetically position the anterior teeth with positioners. Most important, these appliances require patient cooperation. Similar challenges exist with elastics, which are best utilized for settling the dentition vertically and correcting minor anteroposterior discrepancies. Bends placed in archwires allow for complete three-dimensional control and are less sensitive to patient cooperation. This technology allows us to build the exact amount of required correction into the archwire, thus preventing any overshooting or undershooting.
DR. WHITE Exactly how do you generate such a precise appliance system?
DR. SACHDEVA Once the treatment target is defined, the orthodontist's preferred bracket prescription is selected from an electronic library and digitally placed on the three-dimensional model. Care is then taken to determine the optimum design of archwires and appliances. A simulation is run to assess the performance of the selected appliance system and to verify the correct design prior to fabrication. This activity only requires a few minutes and can be accomplished independent of location.
DR. WHITE How do you fabricate the appliances?
DR. SACHDEVA We do not fabricate brackets. Orthodontists already have access to a number of bracket systems. We custom-form the wires from a digitally controlled machine that uses specific design criteria such as archform, curve of Spee, and the position and nature of bends as input parameters (Fig. 4).
DR. WHITE This is a little like "back to the future" in that the customization is being done in the wire rather than in the bracket. Are you fearful that some will look on this as a giant step backward?
DR. SACHDEVA No. Our experience over the last 30 years has made us realize the limitations of our current systems. To obtain high-quality results, we need to complement the straight archwire system with archwire bending. In this sense, I feel we are taking a step into the future.
DR. WHITE Would it be correct to say that the bending machine replaces a great deal of the "art" in the art and science of orthodontics?
DR. SACHDEVA Yes. It significantly reduces the error that is experienced in the manual bending of archwires. We believe that orthodontists who embrace this technology will experience additional personal satisfaction, because they will continuously learn and know more throughout each case, and find ways of expressing any desired artisanship through the custom capabilities of the technology. There are good ways to exhibit the art in the art and science of orthodontics. Settling for poor wire-bending results is not one of them.
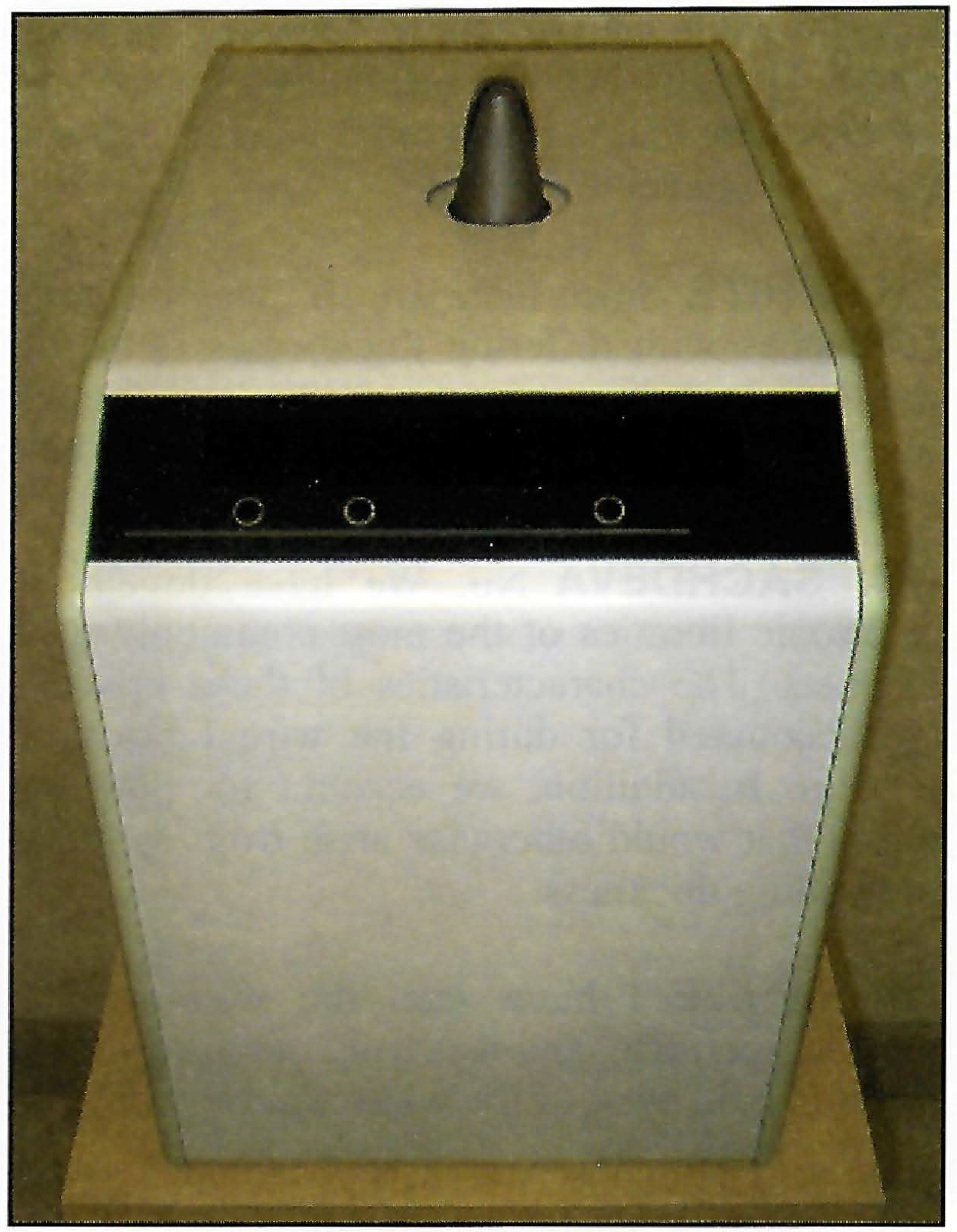
Fig. 4 Wire-bending machine.
DR. WHITE So in your mind, the custom-shaped wire is a key ingredient in your solution?
DR. SACHDEVA Absolutely! There are just too many variables involved in a manual process to allow a clinician to achieve the most optimum shape. The wire-bending technology we use produces a wire that is much more precise than any human could achieve.
DR. WHITE Since there are so many different appliances with differing thicknesses of bases, torque values, in-out arrangements, and angulations, will this not be difficult for the algorithms of the software to handle?
DR. SACHDEVA No. We have developed electronic libraries of the most commonly used brackets. The characteristics of these brackets are accounted for during the wire fabrication process. In addition, we account for potential errors that would otherwise arise from variation in bonding thickness.
DR. WHITE I have seen the wire-bending machine perform, and it is truly remarkable, but can it handle most of the wires we use today?
DR. SACHDEVA Yes, it can bend stainless steel, TMA**, TiNb, and the superelastic nickel titanium wires.
DR. WHITE Have you developed computer algorithms for handling ribbon arches such as .018" × .014" or .022" × .016"?
DR. SACHDEVA Not yet, but this will be possible in the future.
DR. WHITE Typically, few orthodontists fill the preadjusted brackets of current systems with edgewise wires. For instance, many who use .022" brackets seldom place wires larger than .019" × .025", and orthodontists who use .018" brackets ordinarily use nothing larger than an .017" × .025" wire. Does your precision wire have to be a full-size wire if it is to have the effect you prescribe?
DR. SACHDEVA No. Orthodontists generally use undersize wires in finishing because poor manufacturing tolerances for both the wire and the slot prevent engagement of large cross-section wires. Furthermore, fear of placing excessive forces on the dentition and causing brackets to debond are issues that deter the orthodontist from using full-size wires. This system will manage the use of undersize wires through compensation bends. We also have the ability to place 3rd-order bends in full-size superelastic nickel titanium wires. Again, the system is designed to cater to the needs of the orthodontist.
DR. WHITE Since this robot and software can bend a wire to an exact fit in three dimensions, it would seem economically prudent for the orthodontist to use the cheapest bracket possible rather than a more expensive preadjusted one. Is this a reasonable assumption?
DR. SACHDEVA Yes, if the orthodontist so desires. But keep in mind that good brackets have many additional features that add to their functionality. These include reduced friction, biocompatibility, anticorrosion, superior bonding bases, good tie wings, etc.
DR. WHITE Where are the precision custom appliance systems made?
DR. SACHDEVA While the scanner and work station reside in the orthodontist's office, the customized appliance systems and wires are produced in our electronic laboratory. By connecting the orthodontist's office to our lab with a secure network, we are able to service the orthodontic community in an economical and timely fashion.
DR. WHITE So a wire-bending machine in your electronic lab will customize wires from scans done in the orthodontic office? How are they supplied to the orthodontist? Does the orthodontist receive a complete series of wires that will be used sequentially in the treatment, or will they be ordered on an as-needed basis?
DR. SACHDEVA Each customized kit is sent to the orthodontist's office after it is generated. Additional wires may also be supplied to ensure that replacements are on hand for breakage or emergency situations. Additional or revised wire prescriptions can be provided at any time during the course of care.
DR. WHITE How do you manage for variation based on human error, such as the error that can be introduced during direct bracket placement?
DR. SACHDEVA Actually, this is the beauty of the "closed-loop" or complete solution we have developed. Any error that is introduced can be measured accurately with the scanner and compensated for with a precise adjustment in the wire geometry. For example, in the case of initial bonding, a bracket verification scan is performed directly after bonding to ensure that proper placement has been achieved. If an error is detected, a remedy can be provided either at chairside or soon thereafter. Usually, this will mean an adjustment in the wire. The benefit is that in all instances the problem is identified and corrected immediately, rather than six to 12 months or more into the future.
DR. WHITE Have you perfected a technique that can transfer the bracket placement developed on the screen to the patient's mouth?
DR. SACHDEVA Yes, we have a unique approach to place the brackets precisely (Fig. 5). More important, we are able to verify the placement of the brackets independent of the method of application.
DR. WHITE Do you see this technology supplanting wet labs and traditional plaster models?
DR. SACHDEVA Not in the near future. But as these labs become more integrated with current rapid fabrication processes, a transformation will occur. The traditional plaster model will eventually be replaced by a three-dimensional image. The technology also exists to fabricate physical models from a digital scan on demand.
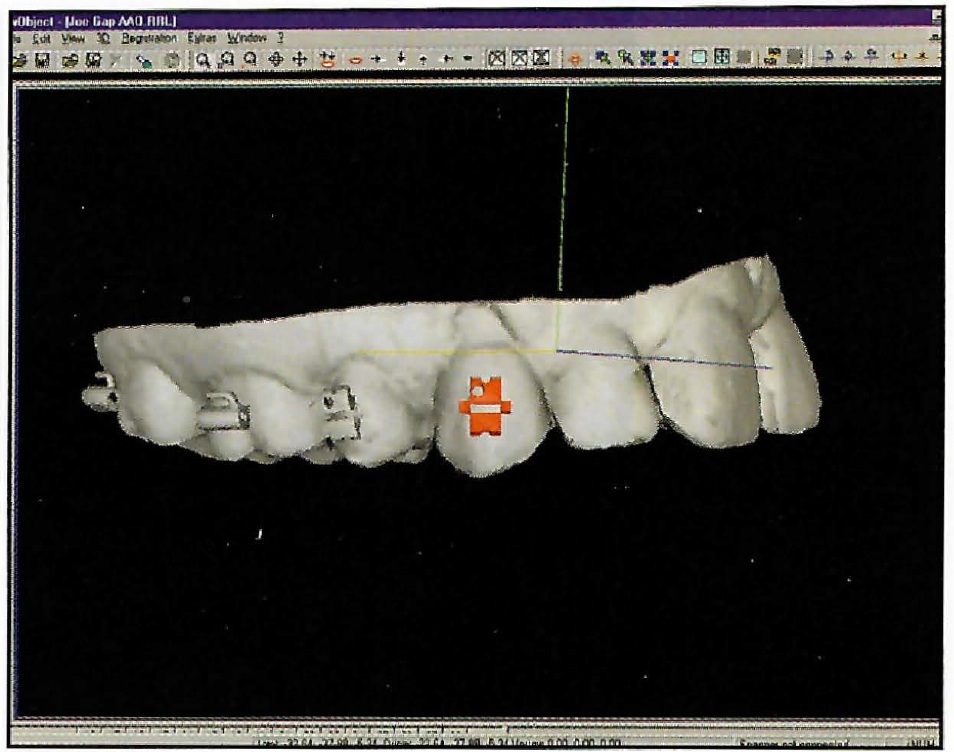
Fig. 5 Electronic bracket placement.
DR. WHITE How many visits and archwire changes and how much overall time can patients expect with this type of treatment?
DR. SACHDEVA Our clinical experiences have demonstrated treatment time reductions of 50% during finishing. We estimate that the use of this system throughout the entire care cycle will save more than 30% of the time required for overall treatment, and provide a 40% reduction in the number of required patient visits. One of the objectives of our current clinical activities is to validate these forecasts. In general, we have been treating all patients with two or three archwires. We have experienced these efficiency gains with both extraction and nonextraction cases. Most important, these improvements have been realized with improvements in overall quality of finish (Fig. 6A and 6B).
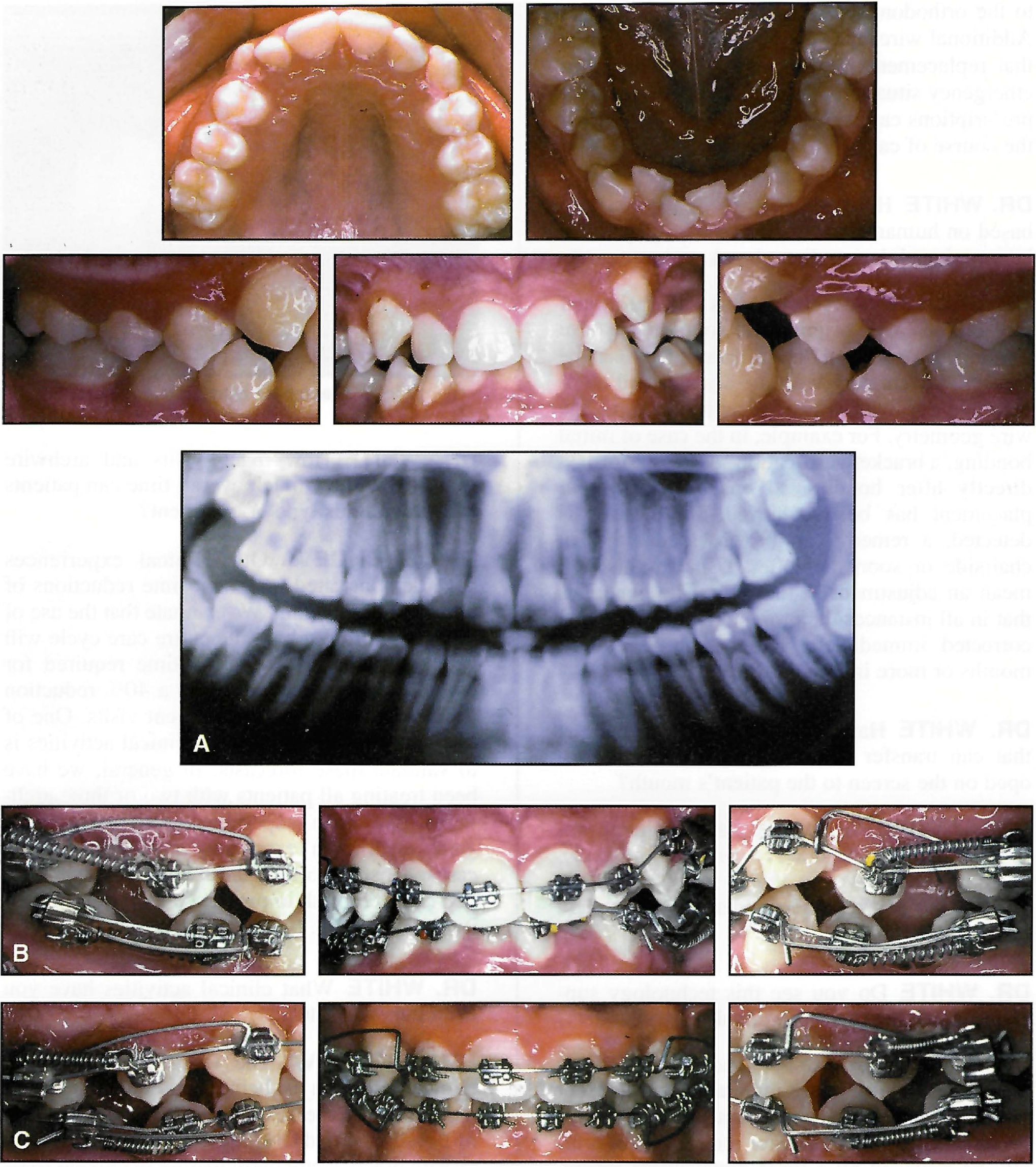
Fig. 6 A. Patient before treatment. B. After extraction of four second bicuspids and placement of initial appliances. C. After four months of leveling, alignment, and space closure with .017" × .025" TMA tipback springs and .017" × .025" Copper Ni-Ti** 35°C wires (continued in next page).
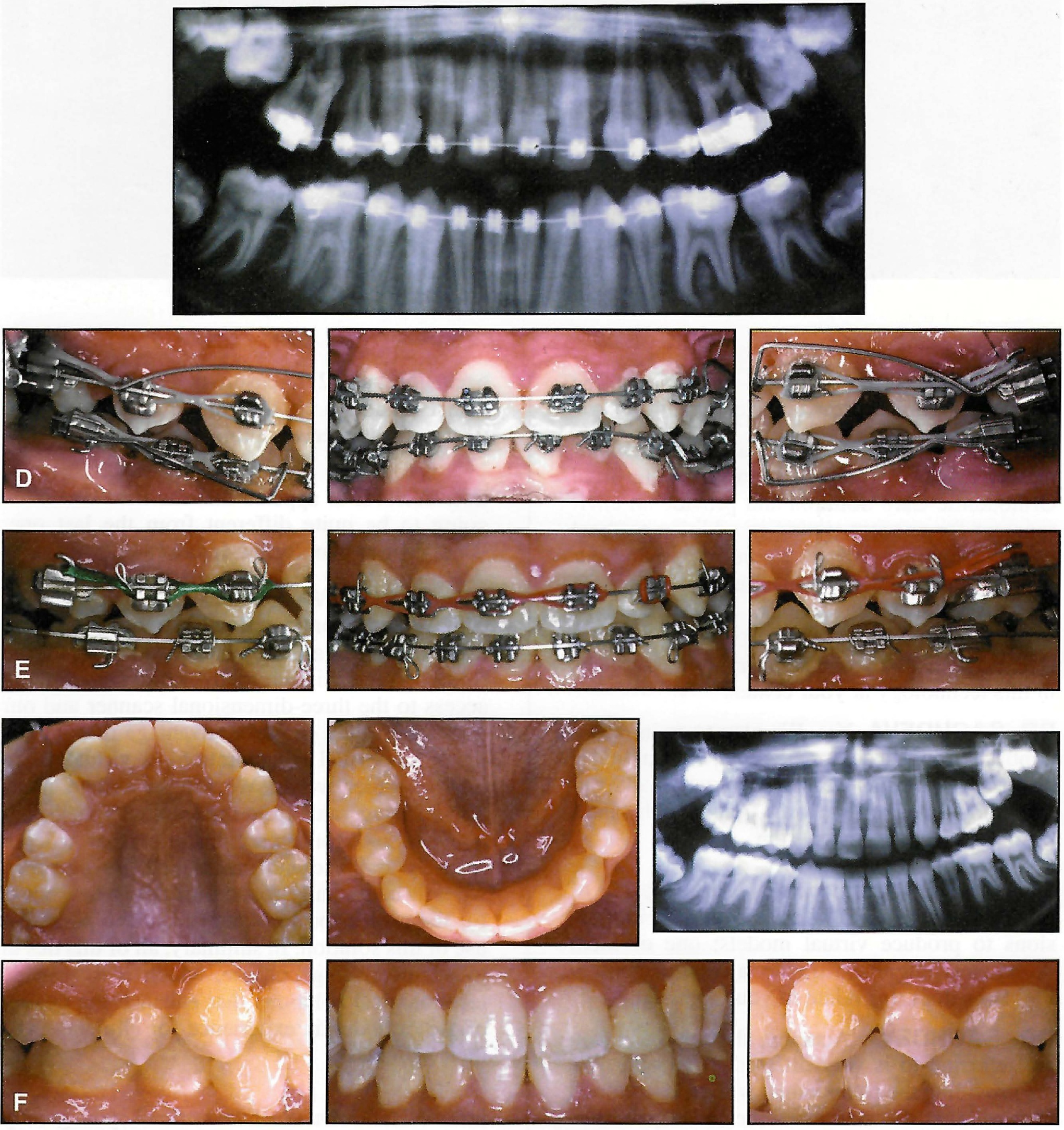
Fig. 6 (cont.) D. After six months of treatment. Note translation of canines and premolars during space closure. E. After 10 months of treatment, placement of .019" × .025" TMA finishing wires. F. Removal of appliances after 12 months of treatment.
DR. WHITE What clinical activities have you been pursuing lately?
DR. SACHDEVA The focus of our current clinical program is being coordinated through our Clinical Research Center in Dallas. A group of Board-certified OraMetrix Fellows, who are in private practice, are participating in clinical trials both in our facility and also in their independent practices.
DR. WHITE Tell us a little more about the OraMetrix Clinical Research Center (Fig. 7).
Fig. 7 OraMetrix Clinical Research Center in Dallas.
DR. SACHDEVA This is a state-of-the-art facility that we developed to evaluate our Total Orthodontic Care Solution and provide an environment for concept testing in addition to "real world" treatment. We are rigorously testing our approach prior to its implementation into the world of clinical orthodontics.
DR. WHITE Do you plan to train orthodontists in this technology at your center?
DR. SACHDEVA Yes. We plan to train orthodontists through a comprehensive program that is under development. We will eventually make our technology available to orthodontists who have been certified with the system.
DR. WHITE Right now, there are a couple of other companies that offer scanning of impressions to produce virtual models; one of them offers clear alignment trays via computer imaging. How does this relate to your approach?
DR. SACHDEVA Actually, the approach you are referring to is very different from ours. We are providing the orthodontist with an end-to-end care solution that harnesses the full capabilities of fixed appliances while providing significantly enhanced capabilities for diagnosis, therapeutics, and prognostics. Additionally, we designed our solution with two overarching principles: 1) to provide a valuable solution for treating all malocclusions, and 2) to ensure that orthodontic specialists maintain the control they need to ensure their patients receive optimum care.
DR. WHITE It appears that the next decade is going to be quite different from the last one. What do you plan for the future?
DR. SACHDEVA Obviously, our desire is to provide orthodontic specialists with access to this solution on a more widespread basis. In the future, we envision many clinicians having access to the three-dimensional scanner and our network so they can take advantage of opportunities for virtual collaboration--a virtual study club, in other words. We foresee orthodontists also deriving value from the extremely well-documented electronic case histories that will be securely archived and maintained. Beyond that, we will continually focus on finding new ways for the profession to benefit from the pervasive use of this solution. In summary, all of this ties in to our overriding purpose, which is to provide technological solutions that enhance the quality of the orthodontic experience for clinicians and their patients.
DR. WHITE Dr. Sachdeva, thank you greatly for sharing your thoughts about this amazing technology. I think most of us have been expecting something like this to appear in the future, but from your description, it seems that the future is now.
FOOTNOTES
- *Service mark of OraMetrix, Inc.
- **Registered trademark of Ormco/“A” Company, 1717 W. Collins Ave., Orange, CA 92867.
-
 DR. WHITE
DR. WHITE -
 DR. SACHDEVA
DR. SACHDEVA
Dr. Sachdeva is a Contributing Editor of the Journal of Clinical Orthodontics and the Chief Clinical Officer for OraMetrix, Inc., 12740 Hillcrest Road, Suite 100, Dallas, TX 75230. Dr. White is Editor of the Journal of Clinical Orthodontics and in the private practice of orthodontics at 111 W. Clinton, Hobbs, NM 88240.