(Editor's Note: This quarterly column is compiled by JCO Technology Editor Ronald Redmond. To help keep our readers on The Cutting Edge, Dr. Redmond will spotlight a particular area of orthodontic technology every three months. Your suggestions for future subjects or authors are welcome.)
This month's Cutting Edge column by Dr. Randy Moles tells the story of converging technologies that have spawned a major breakthrough in orthodontics. These technologies all have a common ancestry in the digital age.
SureSmile* incorporates intraoral scanning, cone-beam computed tomography, special-alloy archwires, and precision robotic wire bending, coupling these new technologies with the orthodontist's traditional, highly developed skill sets: diagnosis and treatment planning. It has always been the clinician's dream to produce the desired orthodontic results in the shortest possible time, and SureSmile is dedicated to that goal.
I believe you will find Dr. Moles's article educational, thought-provoking, and even inspirational. Please pay attention, however, when he says that there is a definate learning curve involved. Of course, a learning curve is inherent in practically any orthodontic discipline that is worth the effort; I believe that to be the case with SureSmile.
W. RONALD REDMOND, DDS, MS
Similar articles from the archive:
The SureSmile System in Orthodontic Practice
I have always been interested in new technology and its application to orthodontics. Over the years, that interest has led to my involvement in a number of orthodontic research teams, some aimed toward the elimination of wire bending because of its inherent inaccuracy. The "holy grail" of these research efforts was a system of straight wires that, in combination with precision bracket placement (possibly even customized brackets), could obtain perfect results in as few visits as possible. Therefore, I was intrigued by the SureSmile system when I first heard about it more than five years ago.
My Decision to Implement SureSmile
SureSmile's concept of focusing on the wire instead of the bracket to achieve ideal results seemed novel, but my initial bias toward the "perfect bracket" kept me from pursuing the technology. Moreover, the system as it was first introduced to me in the beta stage was just too cumbersome to bring into my busy practice. So I played the cautious observer for more than a year. The turning point came when one of the members of my orthodontic study club who had used the system said, "It really works!"
My decision to bring SureSmile into my practice was based on the idea that it would be a way to treat patients faster, in fewer visits. I was already getting what I considered to be good results, so I was not convinced I would see a real benefit in terms of treatment quality. Of course, there was the issue of the cost of this sophisticated system in dollars, time, and energy. Because SureSmile was new and only a handful of orthodontists were using it, we would have to develop our own office procedures to make it work in our fast-paced environment. To that end, I set up a long staff meeting to explain the system to the team and review my rationale for acquiring it. I explained that new technologies were creating rapid change in the practice of orthodontics, and that I strongly believed the future success of our practice depended on embracing that change. We had been using Invisalign** for some time, but it had its limitations. I compared the various options for digital orthodontics, discussing the pros and cons of each, and we agreed that the SureSmile system would work best for us.
Our Integration Plan
Once the decision to introduce SureSmile had been made, we discussed at length how we could integrate it into the practice as seamlessly as possible. Four significant changes had to be made:
- Obtaining the initial records and transferring them to the computer to create diagnostic models.
- Scanning the bracketed teeth using the intraoral SureSmile scanner.
- Building in clinician time for the virtual setup and wire order.
Using superelastic copper nickel titanium wires for treatment. Initially, we had to scan our study models into the computer manually, using the SureSmile intraoral scanner. This took about 15 minutes per model set and required a tracking system. Fortunately, since we were already digital, it only required a few clicks to input the photographs and radiographs. With good tracking, this has proved to be no more difficult than obtaining traditional records.
The Learning Curve
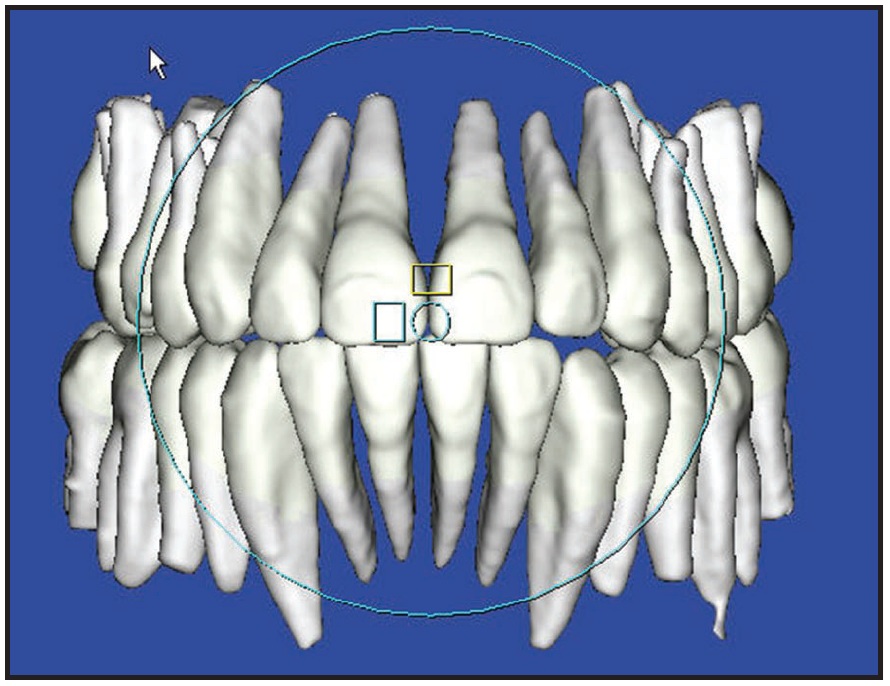
Intraoral scanning was difficult for the first few months (Fig. 1); there is definitely a learning curve here. Our first scans took as long as 45 minutes. After a few months, that time had dropped to 20 minutes. But when SureSmile added support for i-CAT*** scans, we reduced the scanning time to around 20 seconds! We can use computed tomographic (CT) scanning in approximately 70% of our patients. The other 30%, who have crowns or large fillings, are still scanned intraorally. Besides reducing chairtime, the shift to CT scans has greatly improved the quality of my results, because I can see and move not only the crowns, but also the roots of the teeth (Fig. 2). It is wonderful to have this additional perspective in treatment planning and detailing.

Most Class I nonextraction patients are scanned with the i-CAT at the initial bonding visit. Walking the patient down the hall for the scan adds only a few minutes to the appointment. For Class II, Class III, or extraction patients, because the archwires must be removed for scanning, we wait for a wire-change visit after they have progressed to Class I and the extraction spaces have nearly closed. If we placed the SureSmile wires earlier, the bends in the wires might interfere with sliding mechanics.
I had not anticipated how much SureSmile would change the treatment process. I was used to making treatment decisions on the fly at each patient visit. It was a lot like driving a car by looking in the rearview mirror, seeing what had happened, and then deciding what to do next. In contrast, with SureSmile, the desired movements are set up ahead of time. To have this kind of control and precision is exhilarating, but it does take some time to adjust to a new way of thinking. In particular, it required me to dedicate time to the planning process. I had to learn a fairly sophisticated software program and then be disciplined enough to think ahead. I have been pleasantly surprised to be rewarded by much shorter treatment times, more consistently excellent results, and less stress. I now spend about 20 minutes of total computer time on each patient. On the other hand, my time spent at the chair bending wires is literally zero!
My Findings
SureSmile allows the use of several different wires, including stainless steel and titanium niobium. But I find that copper nickel titanium is my workhorse. I can place it in fairly crowded dentitions, and it has all the 1st-, 2nd-, and 3rd-order bends to finish the case. If the teeth are really out of alignment, I can order a wire with the bends reduced by 50%, or by any percentage I desire, for easier placement. After that wire has been used, I can order and place a wire with 100% of the necessary corrective bends.
In my opinion, however, the major advantage of SureSmile is that it is a dynamic system, which means it is adjustable at any point during treatment. In my long career, I have found that perfection is rarely attainable, and unexpected problems inevitably crop up. For example, I may miss a small discrepancy in tooth position while checking the setup in the computer. Bone density, root shape, or occlusal forces may prevent a tooth from moving exactly as I had planned. With SureSmile, I can go into the system, see the interferences (Fig. 3), make the required adjustments in the virtual world, and have a corrected wire within two weeks. Because the new wires include all the original bends, I am always building on my previous work. This gives me a degree of control that is not possible with manual wire bending. The predictability of the process greatly reduces my stress. Although the first SureSmile wire usually gets me close to the desired result, I often order a second wire to make minor corrections.
When I first started using SureSmile, I did little to modify my mechanics. The beauty of the system is that it is "nondenominational", by which I mean it can be used with any bracket system. I just continued doing everything pretty much the same way and used SureSmile only for finishing wires. As I became more comfortable with the system, I began placing the wires earlier and earlier in treatment. This has greatly reduced my treatment times: in more than 500 finished cases, the average treatment time is now 13.1 months.
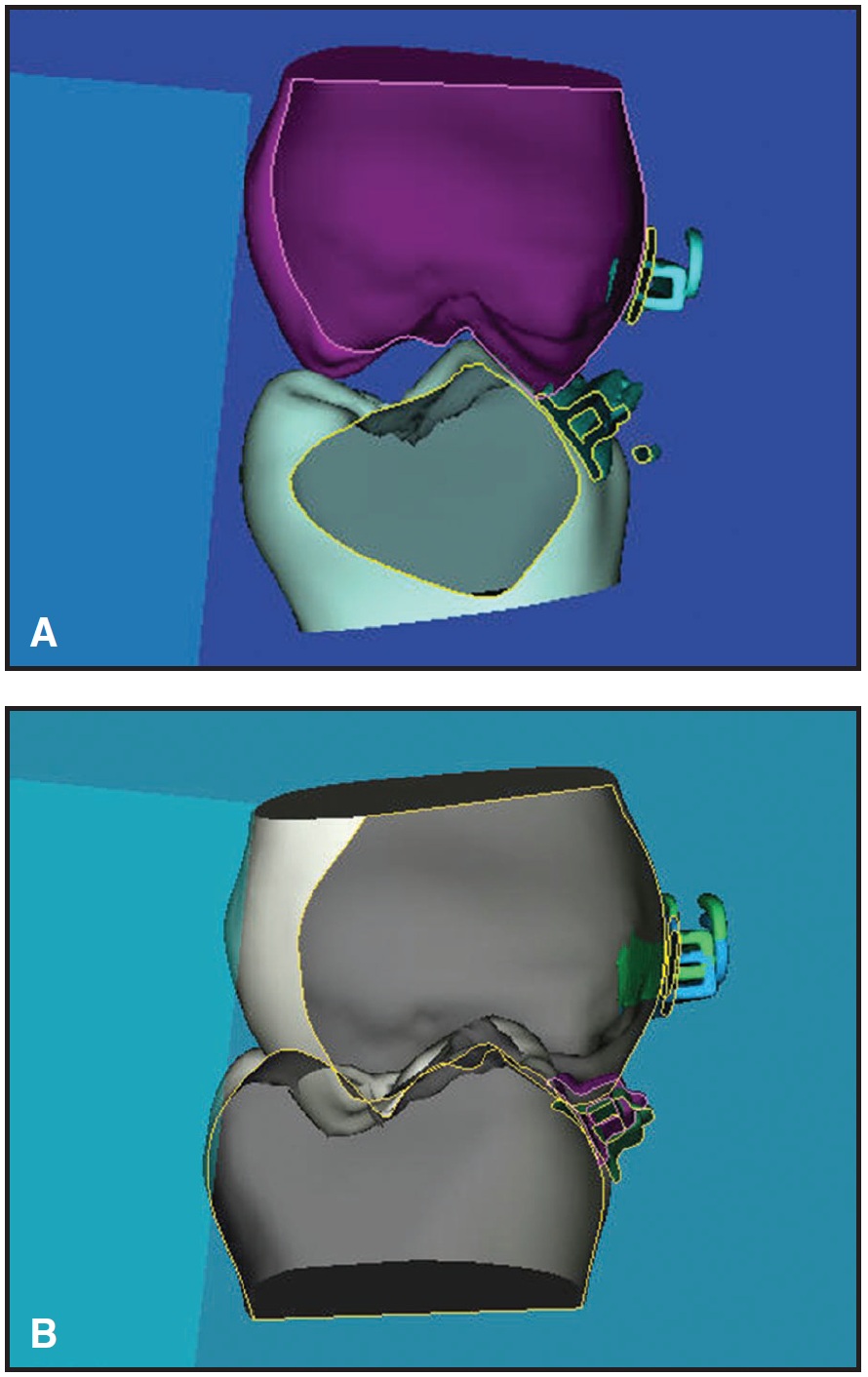
Fig. 3 Virtual teeth “sliced” to show interferences. A. Occlusal interference. B. Bracket interference.
The system provides me with the unanticipated benefit of feedback. Everything is in the computer--the diagnostic models, the setup models, all the modifications I have made, the final models, and even computerized scores using ABO parameters for each model. With a few clicks of the mouse, I can see what worked well and what did not. I must say this is humbling, but it's made me a much better orthodontist. Following are a couple of treatment examples.
Case 1: Extraction
An 11½-year-old female with a mesocephalic facial pattern presented with a Class I occlusion, severe crowding, lateral crossbites, and impacted maxillary canines (Fig. 4, Table 1).
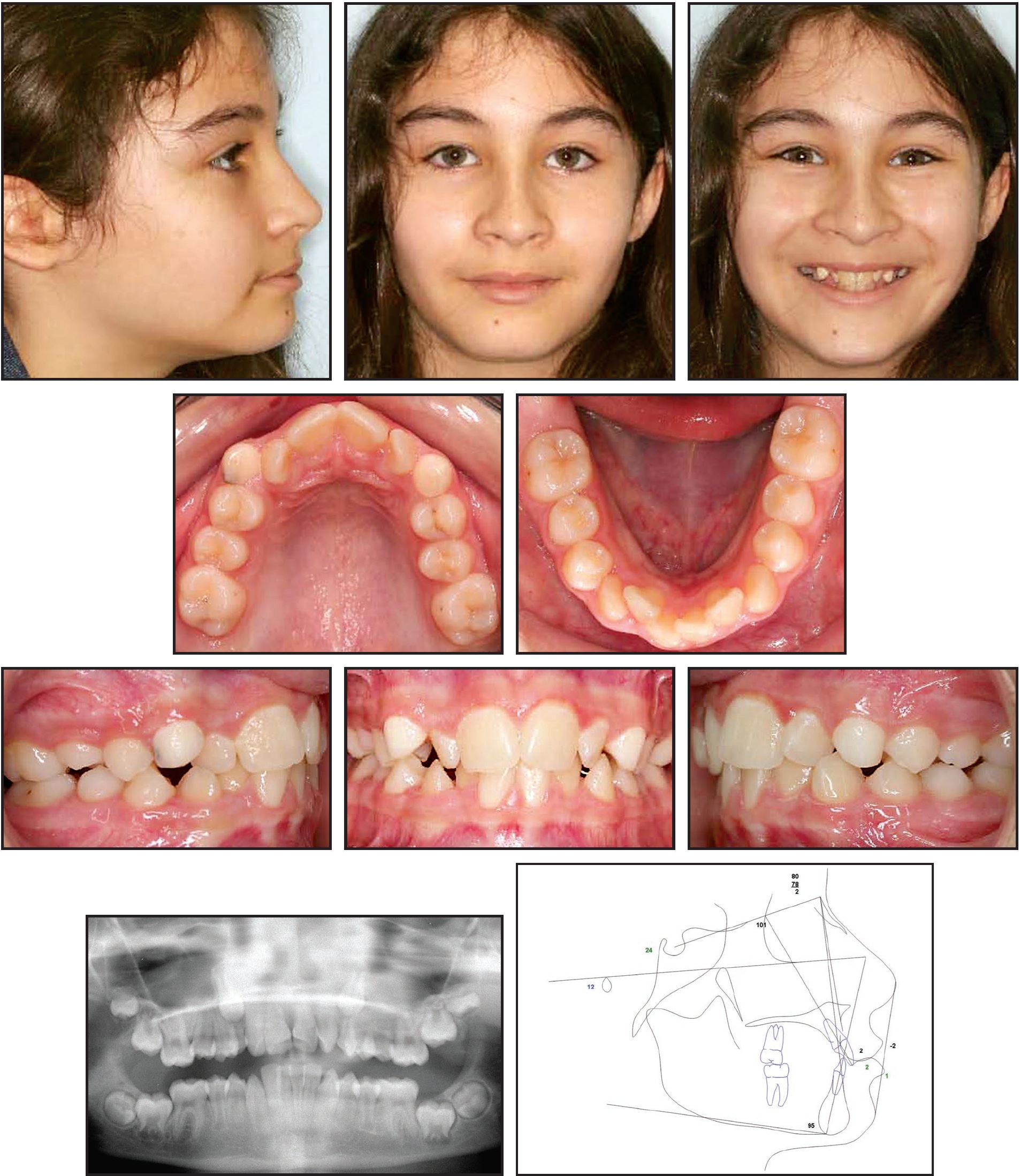
Fig. 4 Case 1. 11½-year-old female patient with Class I occlusion, severe crowding, lateral crossbites, and impacted maxillary canines before treatment.
This was a borderline case and could have been treated with or without extractions. The decision to extract was made because of the thin tissue over the mandibular central incisors and second molars, with the latter showing the potential to become impacted. The patient's records were scanned to create virtual diagnostic models (Fig. 5). The maxillary deciduous canines and maxillary and mandibular second premolars were then removed. Treatment was begun by placing .022" edgewise Orthos† brackets. Space closure was initiated using traditional edgewise closing mechanics with nickel titanium closing coils on .018" nickel titanium archwires.
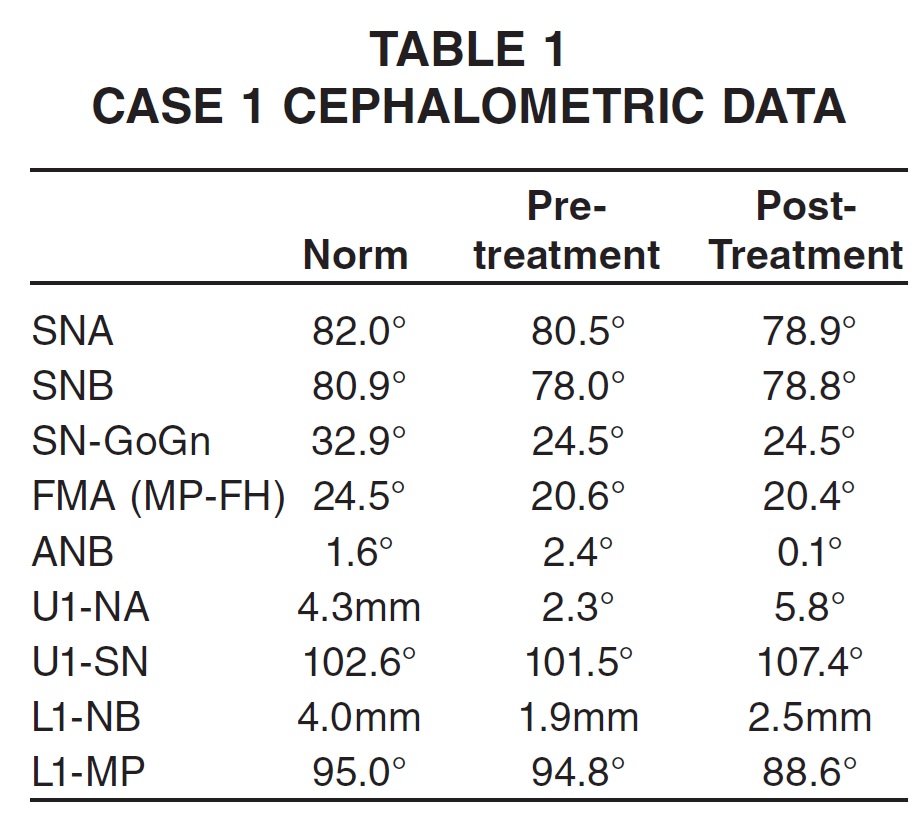

Fig. 5 Case 1. Pretreatment virtual diagnostic models. (Cases pictured in this article were treated before i-CAT compatibility allowed incorporation of roots in diagnostic images.)
Treatment progressed as planned. As the extraction spaces were closed, the maxillary canines and second molars erupted (Fig. 6).
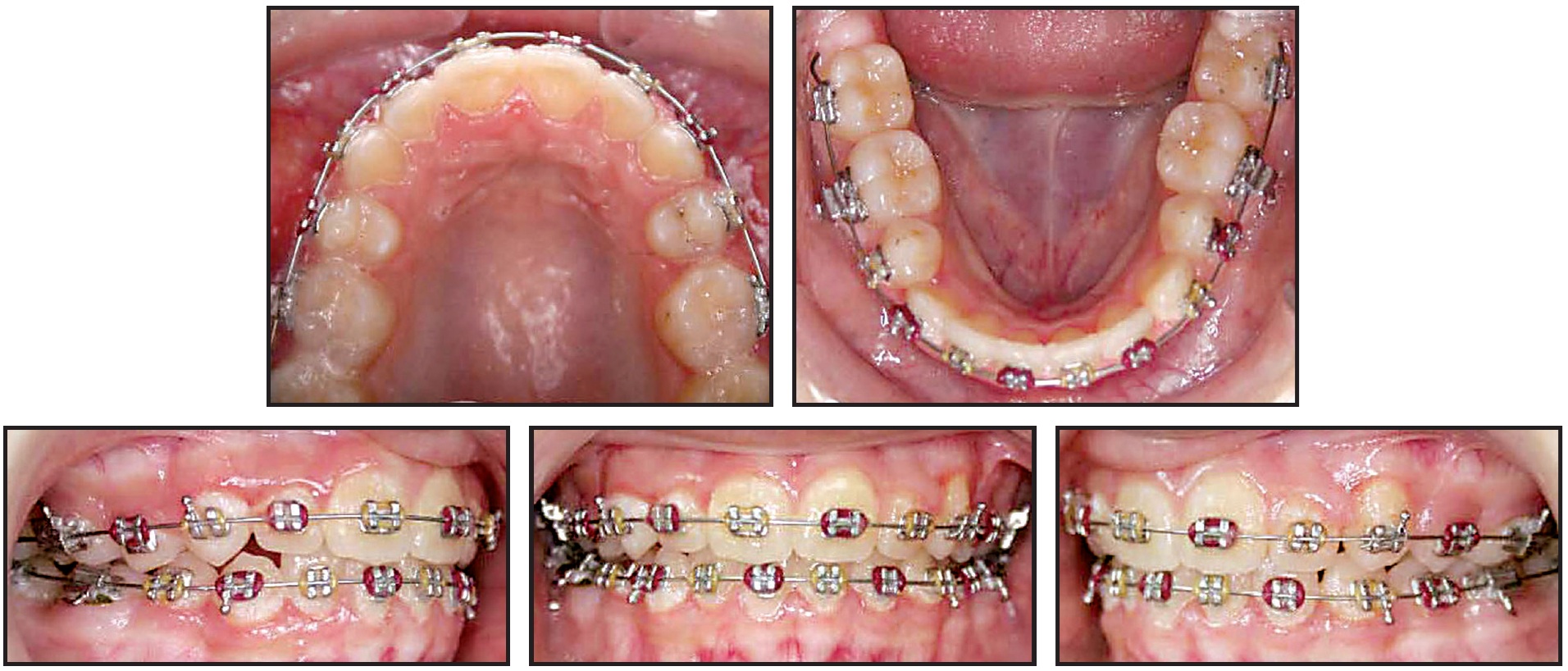
Fig. 6 Case 1. After 13 months of treatment, with extraction spaces closed and patient ready for SureSmile scanning to create therapeutic model.
After 13 months, it was time to scan the teeth with brackets to create a therapeutic model. At this point, significant finishing work remained to be done (Fig. 7).

Fig. 7 Case 1. Therapeutic model for setup.
Following my prescription, an OraMetrix laboratory technician produced an ideal setup, which I then checked and detailed (Fig. 8).
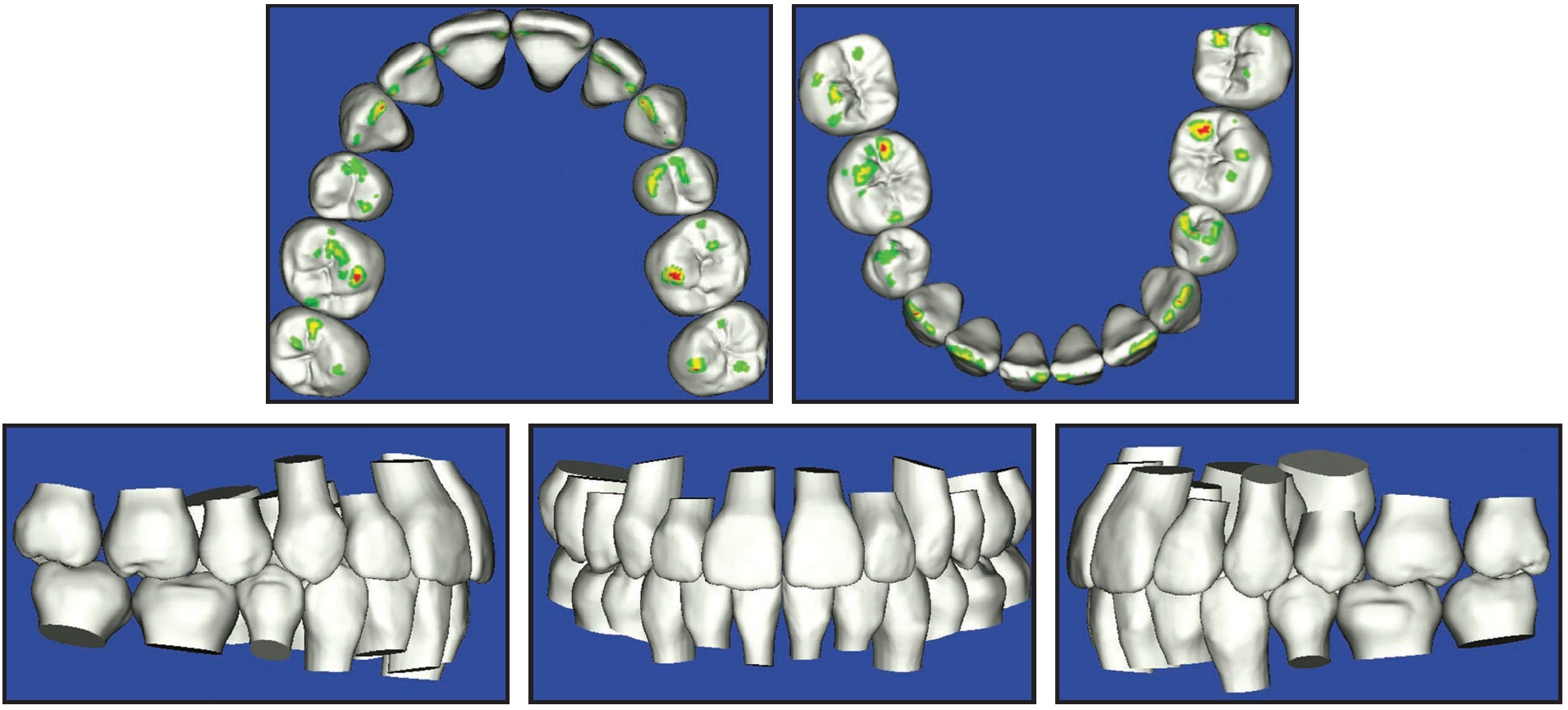
Fig. 8 Case 1. Virtual setup based on clinician’s prescription and detailing.
The computerized score based on ABO parameters is an excellent tool for evaluating the therapeutic setup (Fig. 9).
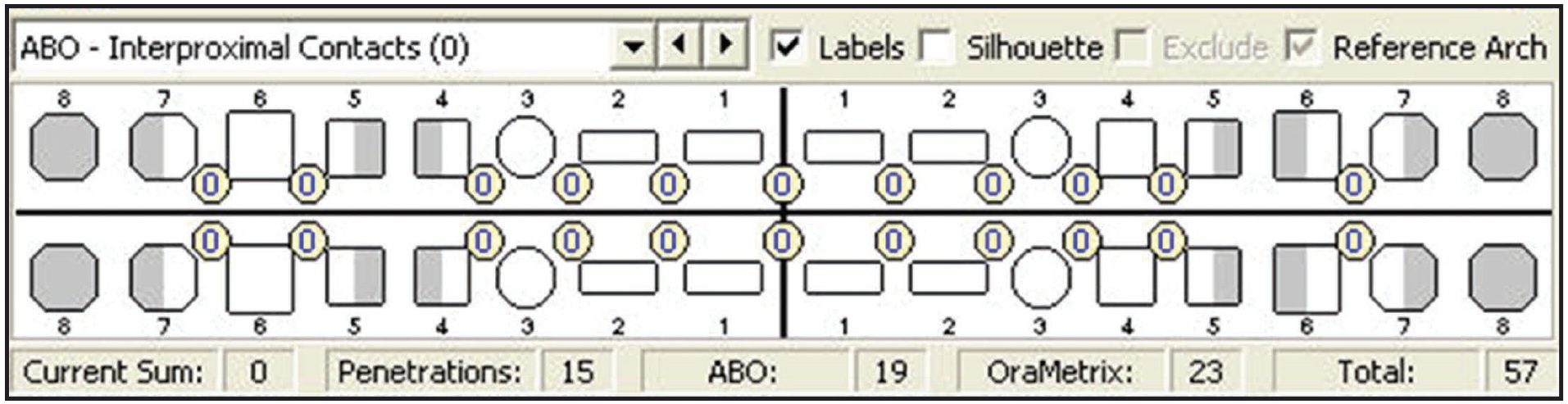
Fig. 9 Case 1. Computerized ABO-style score for quality check.
A robotically bent .019" x .025" copper nickel titanium archwire was placed along with Class II elastics about six weeks after the scanning (Fig. 10).
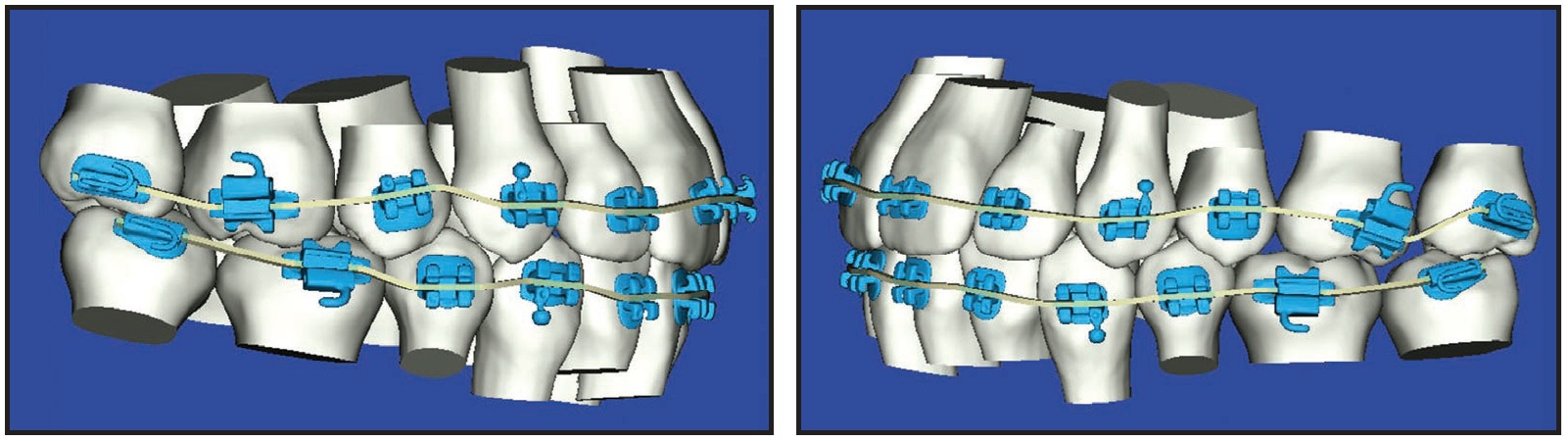
Fig. 10 Case 1. Initial archwires for perfected setup.
The patient was seen again seven weeks later, and a modified archwire was ordered with 6º of lingual crown torque added to the maxillary right second molar and .5mm of extrusion added to the left second molar (Fig. 11A); 8º of lingual root torque had been previously added to the maxillary incisors. In addition, 6º of buccal crown torque and .5mm of extrusion were added to the mandibular left second molar (Fig. 11B).
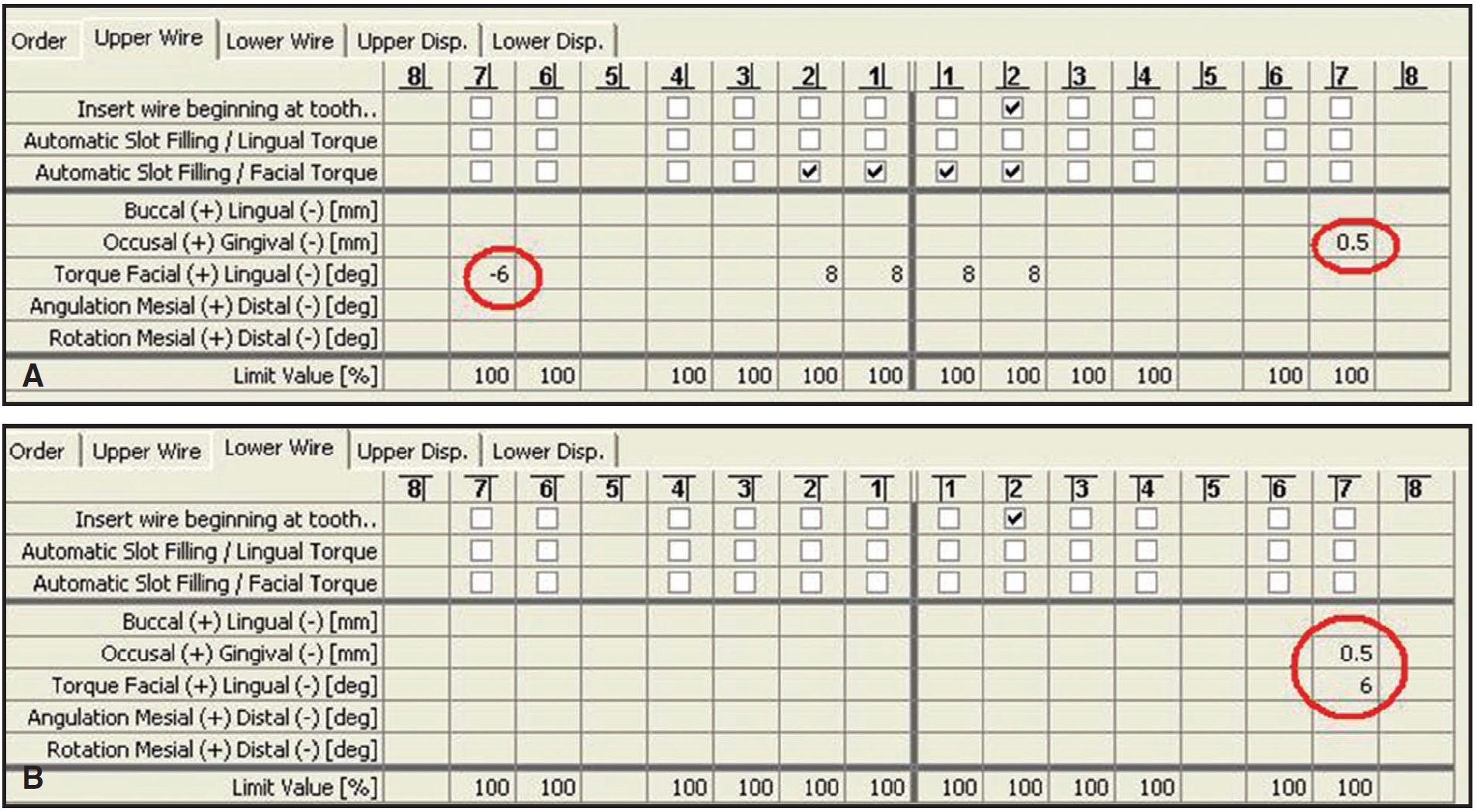
Fig. 11 Case 1. Wire modifications. A. Second maxillary archwire. B. Second mandibular archwire.
Eighteen months after the patient began treatment, the appliances were removed and final records obtained (Fig. 12, Table 1). When the records were scanned into the SureSmile system for evaluation, the computerized ABO score was 28 (zero would be a perfect score; 30 is considered a passing mark). SureSmile significantly shortened the finishing phase of treatment, with no loss of quality, while increasing the predictability of treatment. Not a single wire was bent by hand in the treatment of this case.
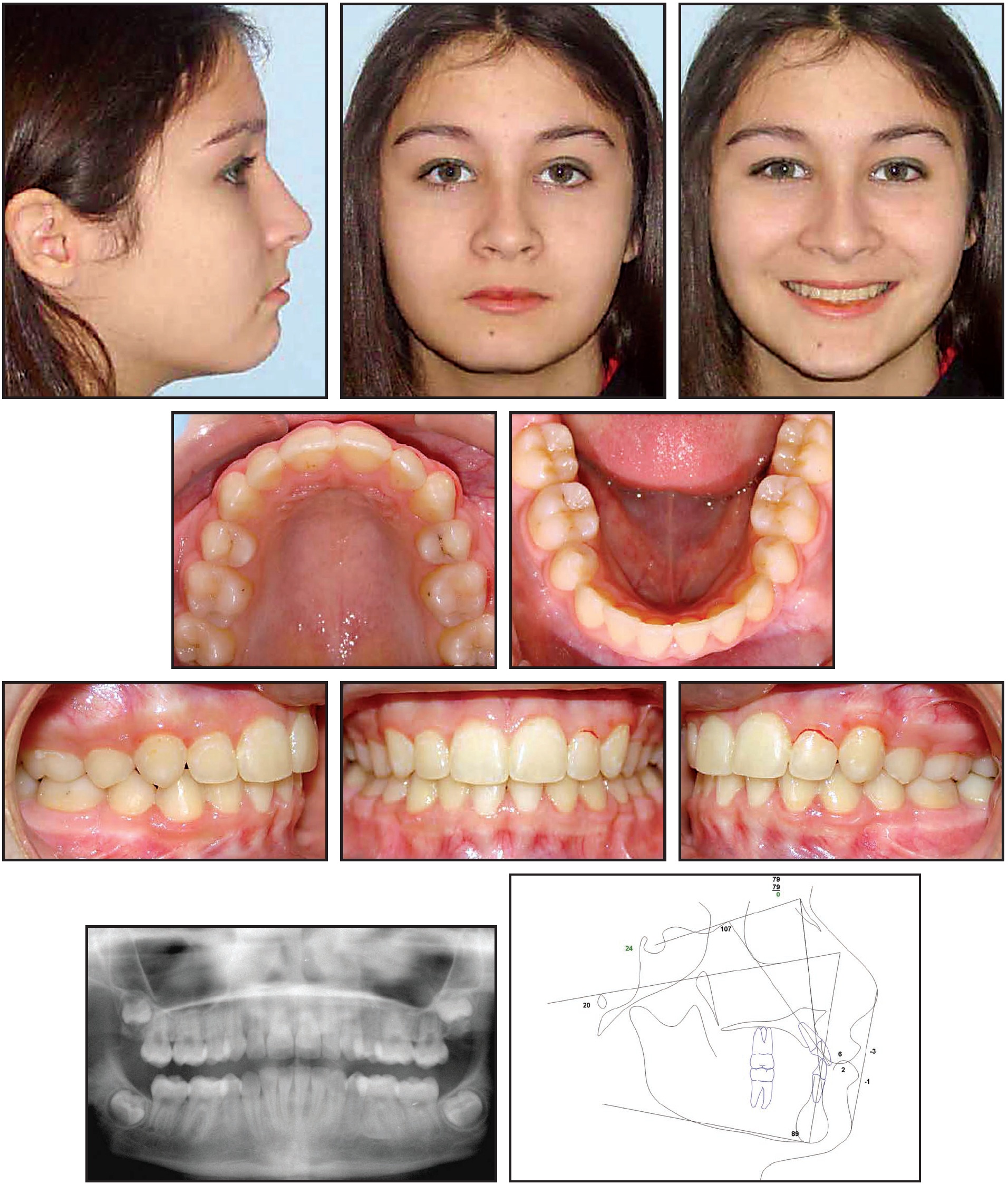
Fig. 12 Case 1. After 18 months of treatment with no wires bent by hand.
Case 2: Nonextraction with 0º Brackets
A 41-year-old female with a dolichocephalic facial pattern presented with maxillary protrusion, an open bite, and mandibular crowding (Fig. 13, Table 2).

Fig. 13 Case 2. 41-year-old female patient with maxillary protrusion, open bite, and mandibular crowding.
Her main complaints were the diastema and protrusion. She had an end-on Class I occlusion and a 4.5mm overjet. Nonextraction treatment was pursued because of the relatively straight profile.
The patient's records were scanned into the SureSmile system to create diagnostic models, which showed a Class II tendency (Fig. 14).
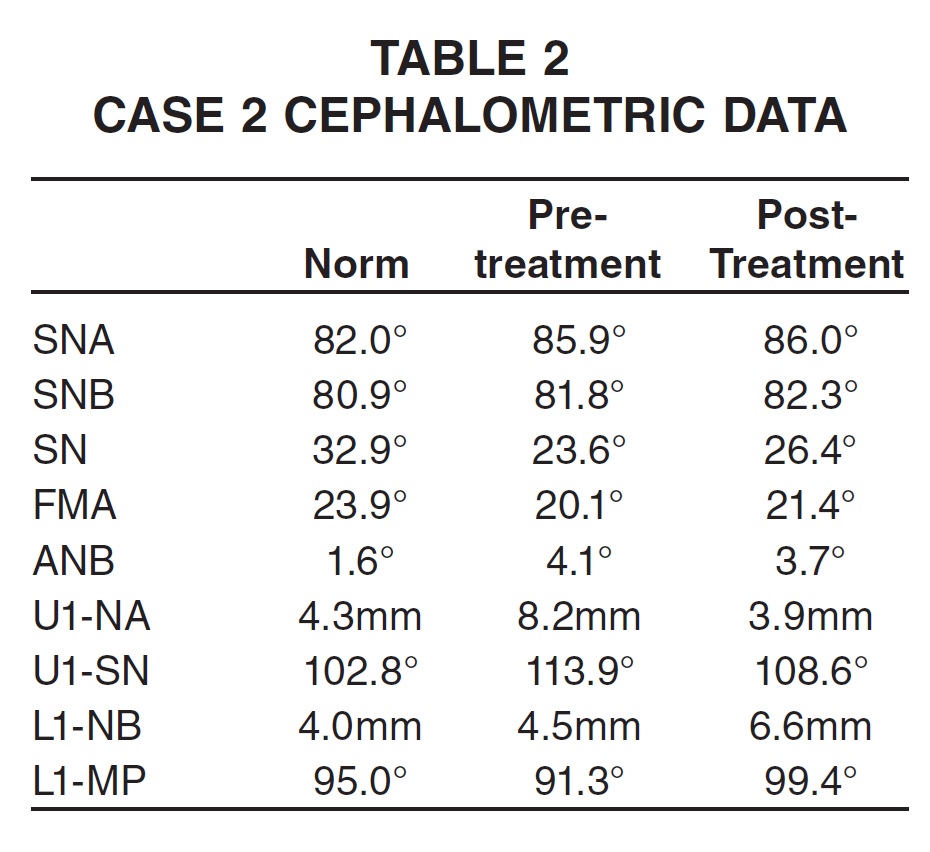

Fig. 14 Case 2. Pretreatment virtual diagnostic models.
Treatment began with the placement of generic 0º .018" edgewise brackets and .014" nickel titanium archwires. To promote expansion, crimpable splittube stops were placed mesial to the molars after the arches were fully engaged (Fig. 15).
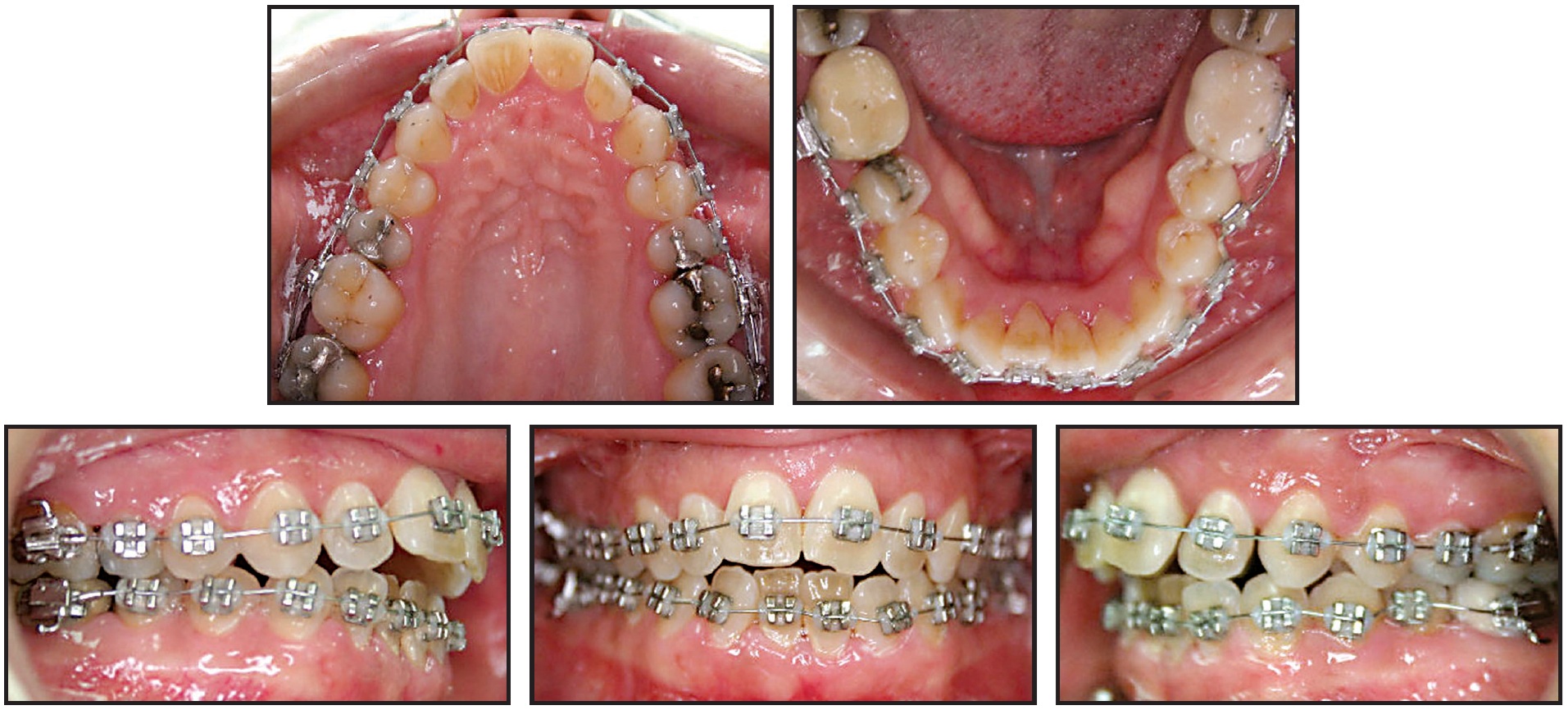
Fig. 15 Case 2. Generic 0° brackets and .014" nickel titanium archwires, with crimpable split-tube stops at molars for expansion.
Six weeks later, the teeth with brackets were scanned into the SureSmile system. As with Case 1, significant finishing work remained; the Class II malocclusion had actually increased (Fig. 16).

Fig. 16 Case 2. Therapeutic model for setup.
Following my prescription, the OraMetrix laboratory did the initial setup, which I then detailed (Fig. 17).
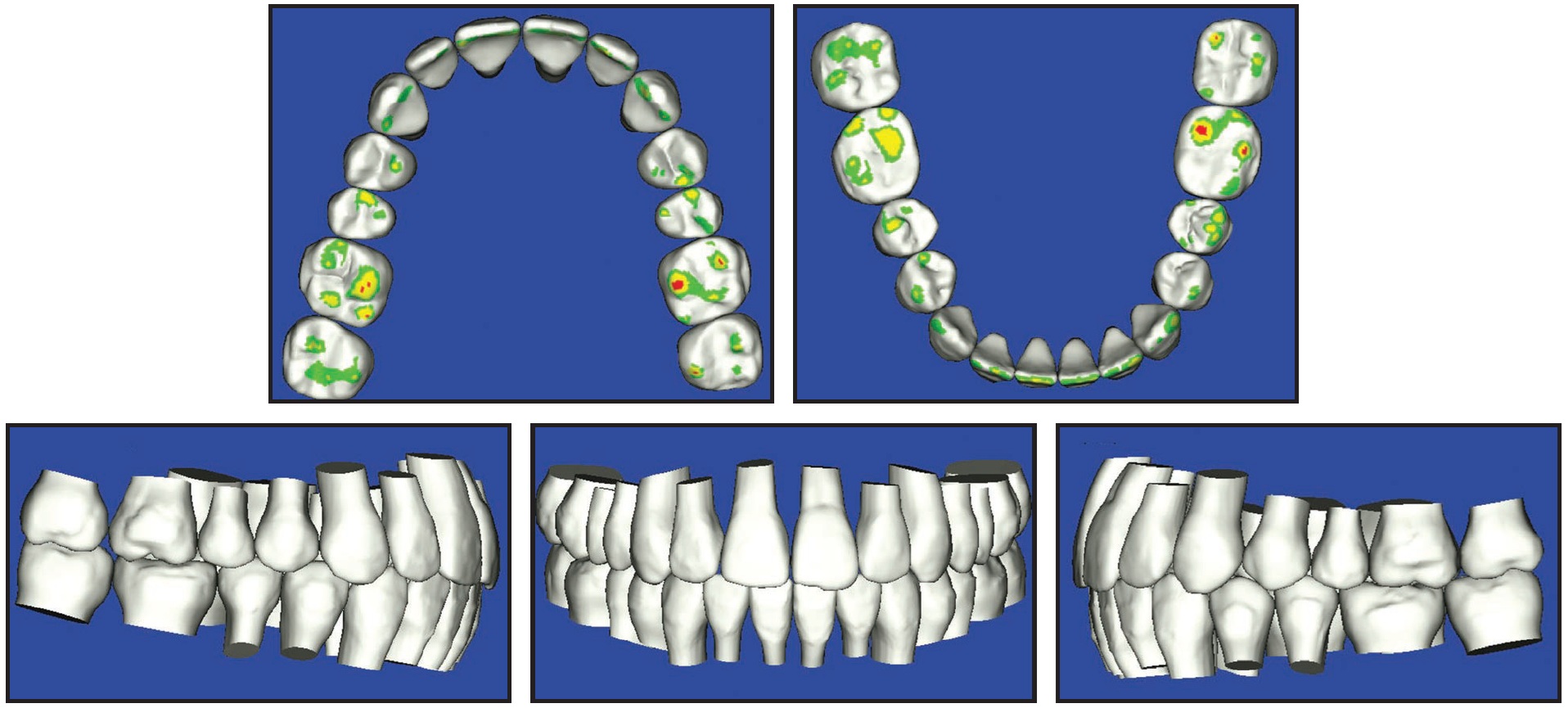
Fig. 17 Case 2. Virtual setup based on clinician’s prescription and detailing.
The computerized score using ABO parameters was 14 (Fig. 18).

Fig. 18 Case 2. Computerized ABO-style score for quality check.
From this setup, the lab produced robotically bent .017" x .025" upper and .016" x .022" lower copper nickel titanium archwires with increased curves of Spee to help prevent the bite from opening up, keeping the upper second molars slightly out of occlusion (Fig. 19).
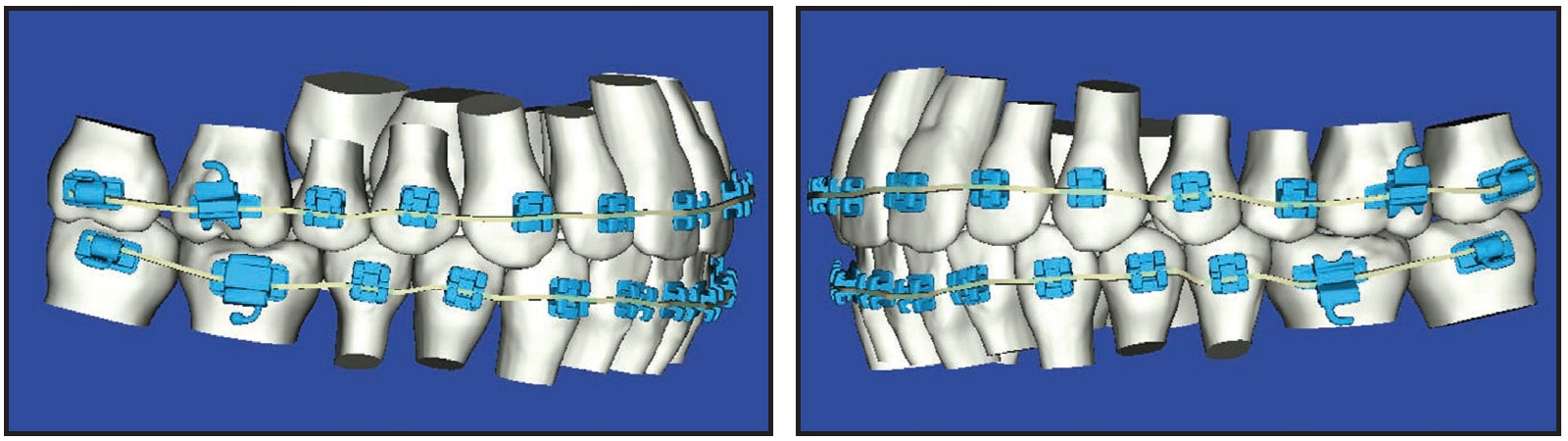
Fig. 19 Case 2. Initial archwires for perfected setup.
Six weeks after the intraoral scan, the wires were placed along with Class II triangular elastics. Eight weeks later, modified .017" x .025" copper nickel titanium archwires were ordered with increased forward angulation of the lower buccal segments and increased distal angulation of the upper buccal segments. Lingual root torque was added to the lower anterior teeth, and a few vertical adjustments were made on selected teeth (Fig. 20). These wires were placed two weeks later, and the triangular Class II elastics were continued.
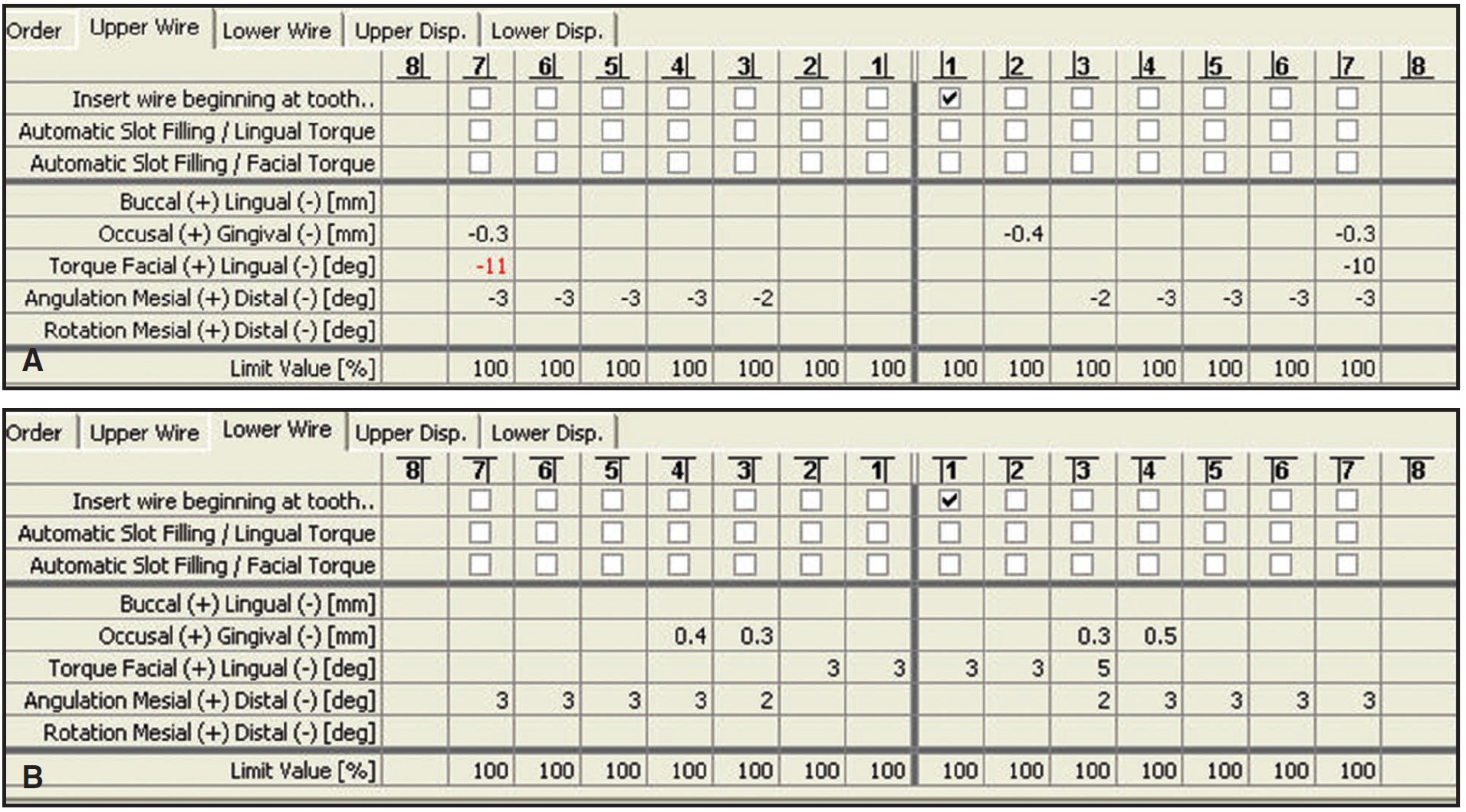
Fig. 20 Case 2. Wire modifications. A. Second maxillary archwire. B. Second mandibular archwire.
Eight months after the initial bonding and eight weeks after the final wires were placed, the patient was debonded (Fig. 21, Table 2). Final records were obtained and scanned into the SureSmile system. The computerized score for this patient was 32. Again, not a single wire was bent by hand to treat this patient.

Fig. 21 Case 2. After eight months of treatment using generic 0° brackets, with no wires bent by hand.
Discussion
SureSmile has worked out extremely well for my practice. It has added about 7% to our expenses, but we have experienced practice growth even in this difficult market. Initially, I offered it as an option to patients at an additional charge. After working with SureSmile for about a year and seeing the results, I decided I did not want to treat patients any other way, so I increased our fees to cover the additional expense. For the past three years, we have treated all fully bonded cases with SureSmile. Our patients and referring dentists are extremely happy with the results, and the word has spread. In my opinion, the combination of rapid treatment and high quality that we can not only see, but document, has been the key to this positive response. My decision to implement SureSmile has definitely paid off.
FOOTNOTES
- *Registered trademark of OraMetrix, Inc., 2350 Campbell Creek Blvd. #400, Richardson, TX 75082; www.orametrix.com. Dr. Moles is a lecturer for OraMetrix.
- **Registered trademark of Align Technology, Inc., 881 Martin Ave., Santa Clara, CA 95050; www.aligntech.com.
- ***Registered trademark of Imaging Sciences International, Inc., 1910 N. Penn Road, Hatfield, PA 19440; www.imagingsciences.com.
- †Trademark of Ormco/“A” Company, 1717 W. Collins Ave., Orange, CA 92867; www.ormco.com.
-
 DR. MOLES
DR. MOLES
Dr. Moles is in the private practice of orthodontics, 5801 Washington Ave., Racine, WI 53406. E-mail: rmoles@yahoo.com.