JCO INTERVIEWS
Dr. Brandon Owen on Custom Labial Braces
In our interview, Dr. Owen, a private-practice orthodontist, founder of KLOwen* braces, and recipient of the first-ever AAO Ortho Innovator Award in 2019, shares his unique insights into custom labial braces and digital treatment planning. He describes the KLOwen digital system and the differences between KLOwen and past and current customized bracket systems; explores the challenges involved in producing high-quality prospective clinical studies; and explains how orthodontists can incorporate this new technology in their offices.
NEAL D. KRAVITZ, DMD, MS
DR. KRAVITZ Dr. Owen, it is a pleasure to interview you for JCO. I was fortunate to be on the AAO Committee on Technology when you received the first-ever AAO Ortho Innovator Award for KLOwen custom brackets. To begin, can you describe how the customization works?
DR. OWEN KLOwen are labial braces, bonded indirectly, that combine premanufactured brackets with customized composite bases (Fig. 1). The customization involves the following process: First, our laboratory sets the patient’s teeth in the ideal positions on a digital model. Second, the orthodontist makes any necessary modifications to the digital model and approves the case. Third, our laboratory reverse-engineers the best-fit bracket for each tooth and fabricates an indirect bonding (IDB) tray that holds each bracket in the correct position so that a custom composite base can be formed at the bonding appointment.
Similar articles from the archive:
- Introduction to LightForce Part 1: 3D-Printing the Next Generation of Fixed Appliances September 2023
- JCO INTERVIEWS Mr. Joseph Hogan on Align Technology February 2017
- JCO INTERVIEWS Dwight Damon, DDS, MSD November 2012
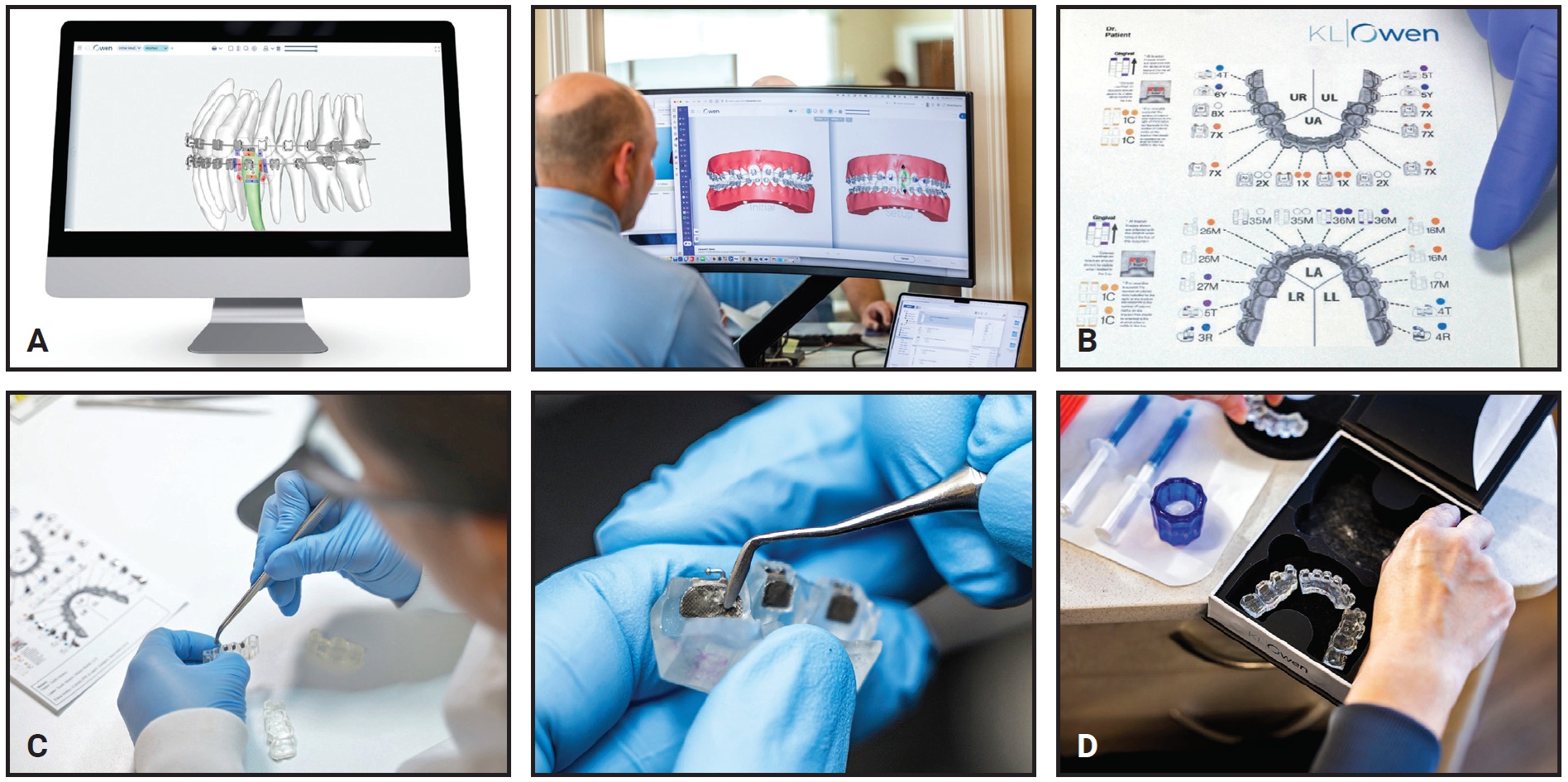
Fig. 1 Customized prescription process for KLOwen* system. A. Digital model modified and approved by practitioner. B. Customized bracket prescriptions. C. Brackets loaded into customized trays for indirect bonding. D. Prepared tray.
We consider KLOwen a “100% custom” system. Most of the customization is in the bracket shape and prescription. We use premanufactured brackets with various thicknesses and torques to lower costs and manufacturing time compared to other custom options. There are six bracket shapes for the maxillary incisors, 12 for the mandibular incisors, nine for all canines and premolars, six for all first molars, and eight for all second molars. These 41 bracket shapes produce 6.1 × 1021 different prescription options.
The remainder of the customization happens during bonding. The IDB tray holds each bracket in the precise orientation required for the ideal 1st, 2nd, and 3rd-order prescription for each tooth (Fig. 2). The composite added for the digital IDB process can be up to .1mm thick and provides the final few degrees of torque, if needed. With IDB, the potential prescriptions are virtually infinite, but even with direct bonding, the custom brackets mean that 6.1 × 1021 prescriptions are possible.

Fig. 2 Additional customization performed during indirect bonding of brackets.
DR. KRAVITZ What is the advantage of the KLOwen system over IDB with conventional stock brackets?
DR. OWEN The most significant difference is that reverse engineering of the custom bracket enables the use of full-size archwires. Generally speaking, bracket prescriptions vary significantly from one patient to the next—and even from the right to left side of the same patient. With conventional brackets, orthodontists typically address these variations by finishing in undersize final archwires with about 20° of slop; with custom brackets, the archwire can fill the slot (Fig. 3).
DR. KRAVITZ Do you have a preference for wire sequencing with KLOwen brackets?
DR. OWEN With twin brackets, my wire sequence for nonextraction cases is .014" nickel titanium, .018" × .018" nickel titanium, and .019" × .025" nickel titanium, though as a pearl, I suggest finishing the lower arch in an .017" × .025" TMA** wire instead. For extraction cases with twin brackets, my sequence is .014" nickel titanium, .018" × .018" nickel titanium, .017" × .025" stainless steel with an additional 10° of torque on the incisors, and .019" × .025" nickel titanium. When using self-ligating brackets, I replace the .018" × .018" nickel titanium wire with .014" × .025" nickel titanium.
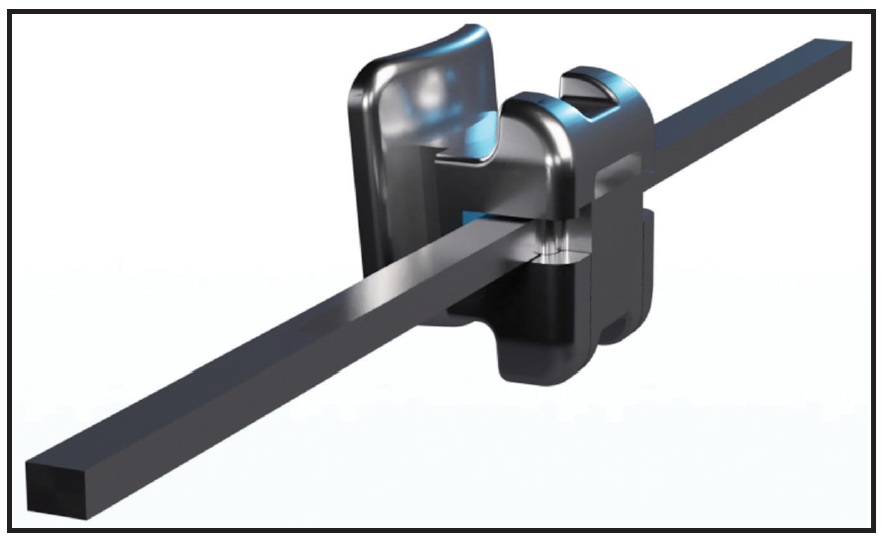
Fig. 3 Customized bracket enables use of full-size archwire that fills slot completely (shown with metal self-ligating bracket option).
DR. KRAVITZ What happens if a patient breaks or loses a bracket?
DR. OWEN If the patient still has the broken bracket, it can be microetched and rebonded. There are two ways to do this: the first is to use a sectioned piece of the original IDB tray, and the second is to directly bond the bracket to the tooth. Using the sectioned tray is better, because the custom composite base can be reapplied. If the original tray is not available, an empty replacement tray can be ordered. Offices using the KLOwen system will have an inventory of all available bracket shapes and torques, so lost brackets can be replaced at the same visit.
DR. KRAVITZ Where are the KLOwen brackets and wires manufactured?
DR. OWEN Most of our brackets are manufactured in the U.S., and currently all of the IDB trays are manufactured at our headquarters in Richardson, Texas. Recently, we have partnered with high-quality manufacturers outside the United States. Wires with our specific bracket-slot dimensions can be ordered through G&H Orthodontics,*** and we are working to validate other suppliers as well. The precision of the bracket slot and finishing archwires is critical for maximizing the efficiency of all custom fixed appliance systems.
DR. KRAVITZ How is the KLOwen system different from Ormco’s Insignia,** which was developed in the early 2000s?
DR. OWEN KLOwen and Insignia are vastly different. When Insignia entered the market, it used twin-bracket blanks, and the torque and 1st-order prescriptions were customized by milling the slots. Later, the system changed to a noncustomized solution combining variable torque prescriptions with passive self-ligating brackets. This reduced turnaround time and manufacturing costs but eliminated the customization that had made Insignia unique.
DR. KRAVITZ Currently, KLOwen and LightForce† are the two most popular custom labial systems in the United States. Can you describe the differences between them?
DR. OWEN LightForce uses three-dimensionally printed ceramic twin brackets, whereas KLOwen uses premade brackets with custom composite bases created during IDB. This enables KLOwen to provide both metal and clear twin and self-ligating bracket options (Fig. 4). It also keeps the price point lower compared to other brands. An advantage of LightForce and other custom systems such as Incognito‡ and Brius†† is that they also include customized bracket bases, allowing for uniform composite thickness.
DR. KRAVITZ Why should an orthodontist invest $500 or more to prescribe custom labial braces?
DR. OWEN Not every orthodontist should. To make custom braces worth the investment, offices must be able to implement systems that will save at least three or four visits per patient. This will increase income while reducing days in the office. Properly implemented, custom braces allow the practice to grow without hiring new associates or adding working days, making a better work-life balance possible. Furthermore, the KLOwen system can provide more consistent case finishes, particularly in busy practices with multiple doctors.

Fig. 4 Typodont demonstrating metal and clear twin-bracket options.
DR. KRAVITZ Does saving three or four visits also reduce treatment time?
DR. OWEN In practice, the average treatment time for comprehensive cases with custom braces can be less than 14 months, and my own average with the KLOwen system is less than a year, but I do not necessarily recommend shortening treatment times as a goal, at least at first. Initially, it makes more sense to keep treatment times relatively similar and instead focus on increasing efficiency and revenue per visit by reducing the number of appointments. After a few years, once doctors master use of the appliances—and address the common patient assumption that the length of the payment plan will match the treatment time—the practice can decide whether it makes sense to shift to shorter treatment times.
DR. KRAVITZ How would you describe the current literature on custom fixed appliances?
DR. OWEN Most of the research on custom appliances has been retrospective.1-8 All studies have found reduced treatment times with custom appliances. Most also evaluated outcomes, and they found that the ABO Cast-Radiograph Evaluation (ABO CRE) and Peer Assessment Rating (PAR) scores in the custom-appliance group were better than or equal to those in the conventional-bracket group. These types of studies require careful interpretation, because there is judgment involved in determining when a case is finished and the patient is ready to be debonded. I could use an .018" nickel titanium archwire, debond the case a little early to prove my results, and market it as a magic wire.
Clinical research on KLOwen specifically is sparse. Our best data is from our white paper, a 2022 multicenter, retrospective study of 138 patients treated with traditional labial brackets and 269 treated with KLOwen brackets.9 (Patients undergoing limited treatment, such as single-arch treatment or simple retreatment, were excluded.) The KLOwen group showed a 31% mean reduction in treatment time and 7.1 fewer office visits. This was a preliminary study, so orthodontists should exercise caution when interpreting the evidence.
DR. KRAVITZ What are some of the challenges a new company faces when conducting prospective clinical studies?
DR. OWEN We have attempted to conduct prospective clinical trials at orthodontic residencies, but we have not had much success, given the difficulty in maintaining stringent research protocols with an ever-changing pool of residents and faculty. You can imagine that this is incredibly frustrating, as years of research and donated products have been wasted. Nevertheless, we will continue pushing for independent prospective clinical trials. We hope to back up our anecdotal claims of increased efficacy with clinical data.
DR. KRAVITZ How can a practice start using the KLOwen system?
DR. OWEN Our team will conduct training sessions to teach the staff how to submit cases. A training team will also hold a virtual session with the orthodontist to provide an introduction to the software and help set up treatment preferences. Next, our clinical trainer will come to the office to assist the team while the first few cases are bonded; we will be by your side throughout the process. For additional information, I encourage orthodontists and their teams to attend lectures or webinars and subscribe to our social-media pages.
DR. KRAVITZ What does the future hold for the KLOwen system?
DR. OWEN For the past five years, our primary focus was on designing the various bracket types (metal twin, clear twin, metal self-ligating, and clear self-ligating), but now our attention is on enhancing the software, which will likely have a big impact. In the short term, we are excited for cone-beam computed tomography integration and automated ABO CRE scoring. In the near future, we want to use artificial intelligence to increase the efficiency of case setups. Undoubtedly, orthodontists will soon be able to provide same-day custom IDB using in-office 3D printing.
DR. KRAVITZ Thank you, Dr. Owen, for your insights into the KLOwen system. I know our JCO readers are looking forward to reading future case reports using KLOwen brackets.
FOOTNOTES
- *KLOwen Orthodontics, Richardson, TX; www.klowenortho.com.
- **Ormco Corporation, Brea, CA; www.ormco.com.
- ***G&H Orthodontics, Franklin, IN; www.ghorthodontics.com.
- †LightForce Orthodontics, Burlington, MA; www.lightforceorthodontics.com.
- ‡Solventum, St. Paul, MN; www.solventum.com.
- ††Brius Technologies, Carrollton, TX; www.brius.com.
REFERENCES
- 1. Saxe, A.K.; Louie, L.J.; and Mah, J.: Efficiency and effectiveness of SureSmile, World J. Orthod. 11:16-22, 2010.
- 2. Sachdeva, R.; Frugé, J.F.; Frugé, A.M.; Ingraham, R.; Petty, W.D.; Bielik, K.L.; Chadha, J.; Nguyen, P.; Hutta, J.L.; and White, L.: SureSmile: A report of clinical findings, J. Clin. Orthod. 39:297-314, 2005.
- 3. Brown, M.W.; Koroluk, L.; Ko, C.C.; Zhang, K.; Chen, M.; and Nguyen, T.: Effectiveness and efficiency of a CAD/CAM orthodontic bracket system, Am. J. Orthod. 148:1067-1074, 2015.
- 4. Weber, D.J. 2nd; Koroluk, L.D.; Phillips, C.; Nguyen, T.; and Proffit, W.R.: Clinical effectiveness and efficiency of customized vs. conventional preadjusted bracket systems, J. Clin. Orthod. 47:261-266, 2013.
- 5. Penning, E.W.; Peerlings, R.H.J.; Govers, J.D.M.; Rischen, R.J.; Zinad, K.; Bronkhorst, E.M.; Breuning, K.H.; and Kuijpers-Jagtman, A.M.: Orthodontics with customized versus noncustomized appliances: A randomized controlled clinical trial, J. Dent. Res. 96:1498-1504, 2017.
- 6. Groth, C.: Compare the quality of occlusal finish between SureSmile and conventional, thesis, University of Michigan, Ann Arbor, MI.
- 7. Rangwala, T.: Treatment outcome assessment of SureSmile compared to conventional orthodontic treatment using the American Board of Orthodontics grading system, thesis, Albert Einstein College of Medicine, Bronx, New York, 2012.
- 8. Alford, T.J.; Roberts, W.E.; Hartsfield, J.K. Jr.; Eckert, G.J.; and Snyder, R.J.: Clinical outcomes for patients finished with the SureSmile method compared with conventional fixed orthodontic therapy, Angle Orthod. 81:383-388, 2011.
- 9. Owen, B.; Brady, P.; Gianquinto, J.; Milnor, L.; and Richter, D.: Efficiency of digital custom braces vs. conventional braces in 4 orthodontic practices, white paper, www.klowenortho.com/white-paper, 2022.
-
 DR. OWEN
DR. OWEN -
 DR. KRAVITZ
DR. KRAVITZ
Brandon Owen, DDS, MS, is the president and founder of KLOwen Braces, Inc., and in the private practice of orthodontics, 3503 Wild Cherry Drive, Building 15, Lakeway, TX 78738; email: brandon@klowenortho.com. Neal D. Kravitz, DMD, MS, is the Editor-in-Chief of the Journal of Clinical Orthodontics, an Assistant Professor at the Harvard School of Dental Medicine, and in the private practice of orthodontics in South Riding, VA.