ALIGNER CORNER
Management of Impacted Canines Using Clear Aligners
This JCO column is compiled by Contributing Editor William V. Gierie, DDS, MS. In each edition, Dr. Gierie will introduce a pertinent article related to clear aligner therapy. Your suggestions for future topics or authors are welcome.
In the current edition of the Aligner Corner, the authors present three cases showing the effective treatment of impacted canines with Invisalign.* These three patients—one with bilateral and two with unilateral impactions—illustrate the kind of ingenuity needed to manage impacted-canine cases with clear aligners. The authors tailored their strategies to the complexity of the required movements, achieving the more difficult movements with lingual Caplin hooks, buccal composite buttons, and, in one case, a segment of lingual brackets. The treatment times ranged from 30 to 36 months.
The techniques the authors describe were successful, and the cases were well treated. Still, we should all be thankful that impacted canines represent only 1-2.5% of orthodontic cases, since they are among the most challenging conditions to treat.
WVG
Management of Impacted Canines Using Clear Aligners
Over the past decade, an increasing number of adolescent and preadolescent patients have requested treatment with clear aligners. A recent study comparing the experiences of adolescents treated with fixed appliances to those treated with aligners concluded that while the overall reported quality of life was similar, those who used clear aligners adapted to treatment more quickly, felt more confident, and experienced less difficulty in eating.1
Along with this surge in popularity, the complexity of cases treated with clear aligners has increased, with a significant expansion in the range of potential indications.2,3 Despite many technological improvements, however, notable differences have still been observed between planned and achieved tooth movements,2,4 and a recent survey found that most practitioners will avoid using clear aligners to treat complex cases.5 In particular, only 10% of orthodontists expressed confidence about managing canine impactions with aligners.5
Similar articles from the archive:
- Pink Esthetic Score Evaluation of Gingival Esthetics after Clear Aligner Treatment of Palatally Impacted Canines July 2024
- CASE REPORT Upper Canine Extrusion Using Temporary Anchorage Devices and Clear Aligners January 2023
- Aligner Treatment of Transposed Maxillary Canines and Lateral Incisors January 2021
Impaction or ectopic eruption of a canine is found in 1-2.5% of orthodontic patients6,7 and is most commonly treated with surgical exposure followed by forced eruption. To ensure a successful outcome, the extrusive force must be applied with the proper vector and magnitude, and appropriate anchorage preparation is crucial. Extrusion and root movement5,8 are particularly challenging to accomplish predictably with clear aligners due to the inherent limitations of the material, which can prevent the aligner from applying adequate force or sufficiently adhering to the teeth.9-11 While recent advances in aligner biomaterials, design, and manufacturing processes have overcome some limitations,10 auxiliaries such as buccal or palatal attachments, elastics, temporary anchorage devices, fixed sectional appliances, and cantilevers can add further biomechanical advantages to enhance the reliability of extrusion.10,12,13
This case series demonstrates the use of auxiliaries to overcome the biomechanical limitations of clear aligners in the treatment of impacted canines. Three patients with unilateral or bilateral impacted upper canines were treated successfully with a hybrid approach combining Invisalign with elastics, buttons, and sectional fixed appliances.
Case 1: Applying an Extrusive Traction Force
A 22-year-old female was referred by her general dentist for treatment of retained upper deciduous canines (Fig. 1A). She had a mildly convex soft-tissue profile, excessive lower anterior facial height, and an obtuse nasolabial angle. The smile arc was consonant, with 90% gingival display, but some lip incompetence was noted. The lower midline was deviated to the left of the facial midline. The overjet was 4mm, and the overbite less than 1mm. Mild Class II molar relationships were present on both sides.

Fig. 1 Case 1. 22-year-old female patient with bilaterally impacted upper canines before treatment (continued in next image).
The panoramic radiograph showed that both upper canines were impacted and slightly overlapping the roots of the lateral incisors. Cone-beam computed tomography (CBCT) evaluation revealed a palatal position of the left canine and a mid-crestal position of the right canine (Fig. 1B).
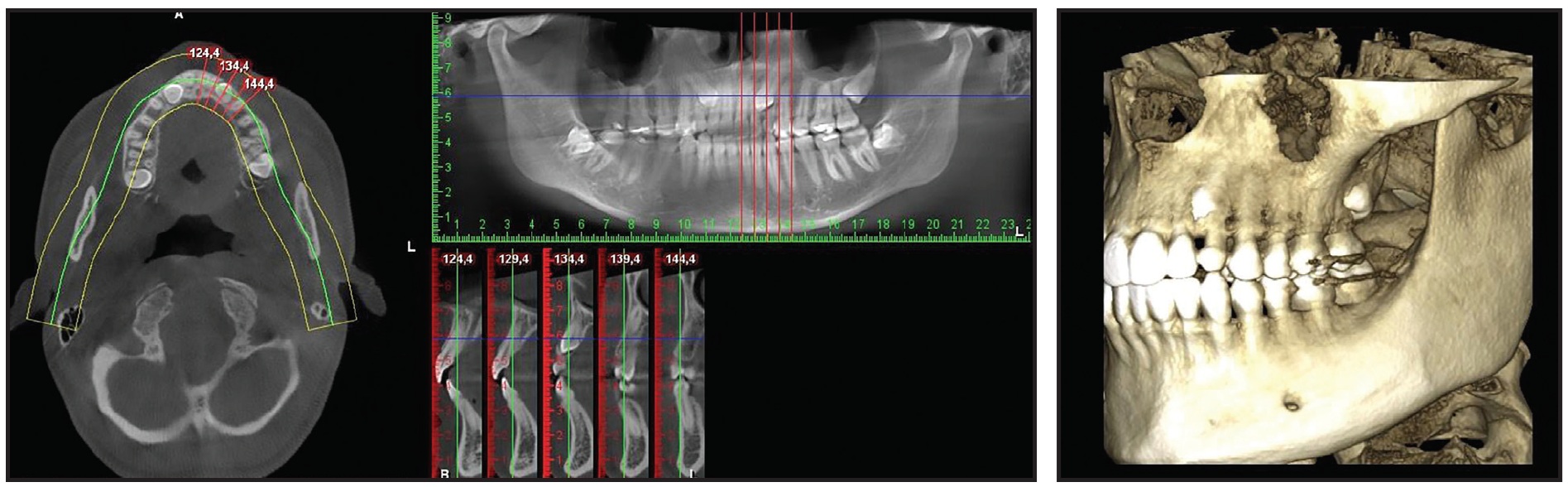
Fig. 1 (cont.) Case 1. 22-year-old female patient with bilaterally impacted upper canines before treatment.
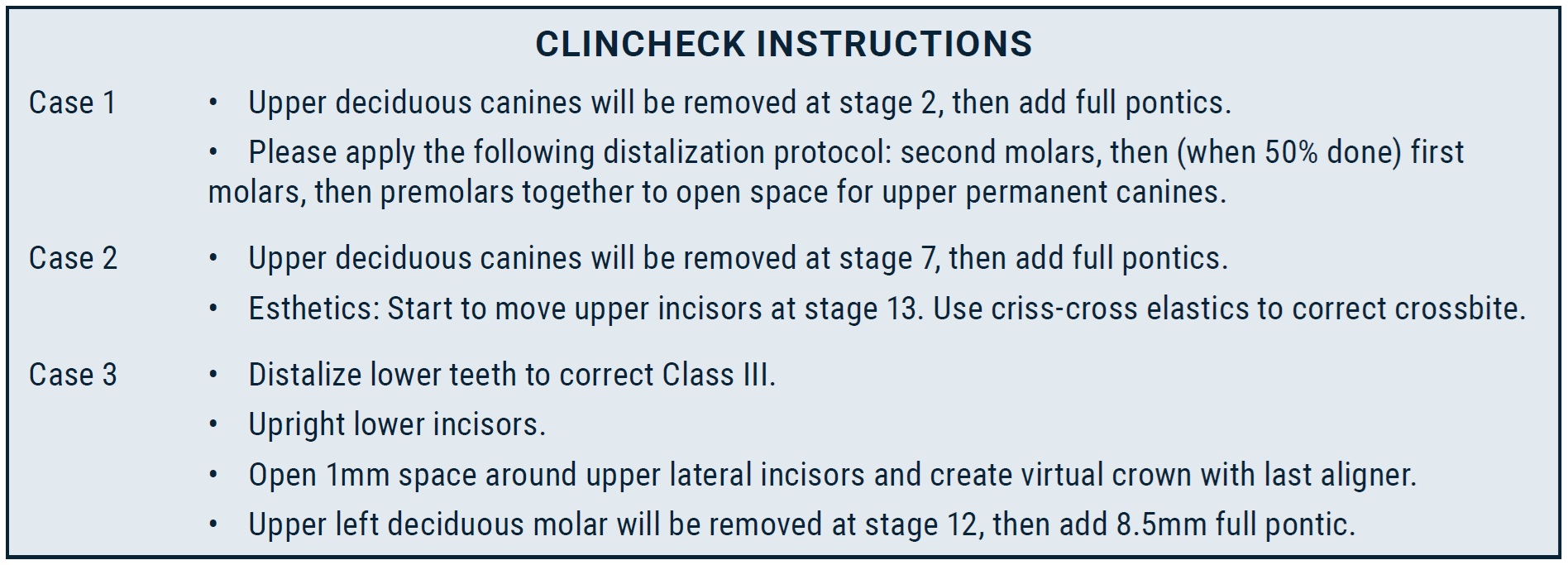
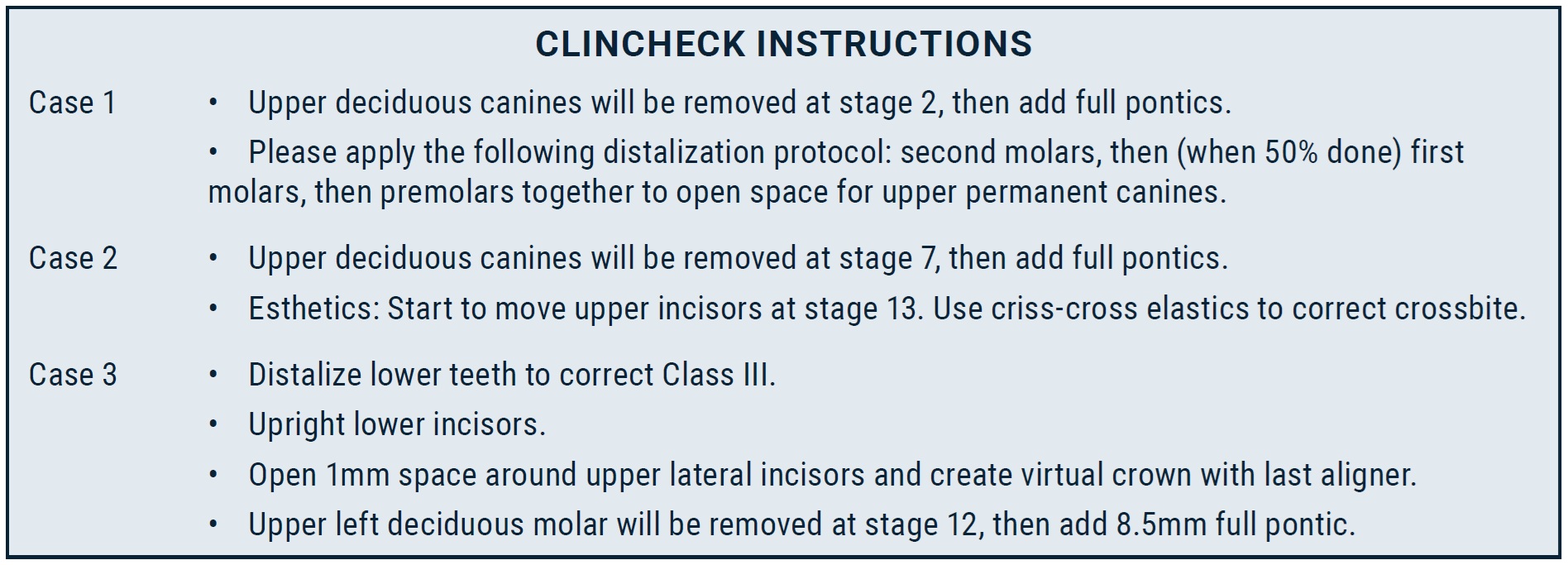
Considering the patient’s age and the locations of the impacted canines,14 the best treatment option was determined to be surgical exposure followed by orthodontic traction to bring the teeth into the arch. Invisalign clear aligners were selected to meet the patient’s preference for esthetic treatment. Additional objectives were to align the teeth and correct the Class II relationship and midline deviation. Sequential distalization would be performed in the maxillary arch (3mm on the right side and 4mm on the left), and Class II elastics would be used to prepare space for the canine and correct the Class II relationship (Fig. 2).
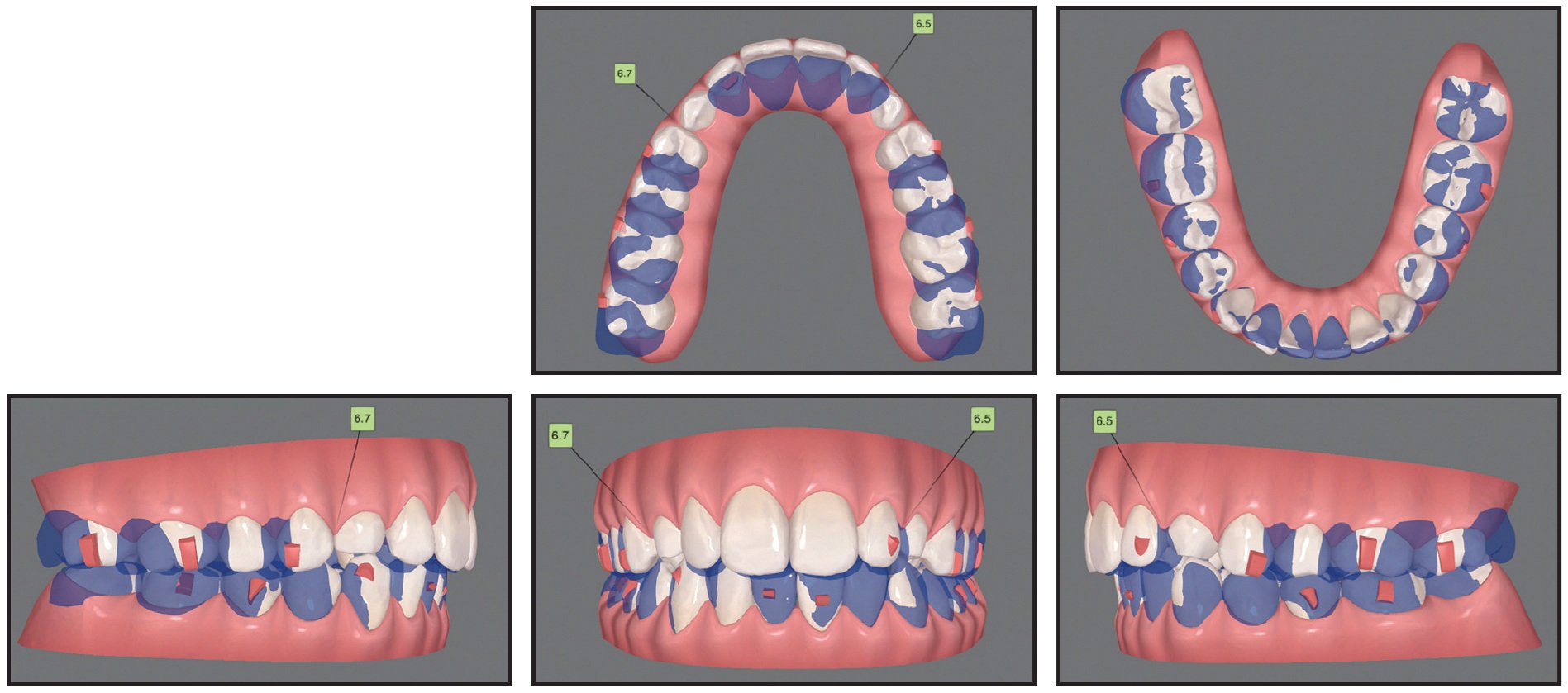
Fig. 2 Case 1. ClinCheck* superimposition of initial (white) and planned (purple) tooth positions for correction of Class II relationships using sequential distalization and Class II elastics.
At the beginning of treatment, the upper deciduous canines were extracted and temporarily replaced with pontics added to the aligner trays by filling the labial aspects with composite (see box).
After the attachments were bonded, the patient was referred for surgical exposure of the canines. An open-exposure procedure was performed on the upper left canine, and traction began immediately. To move the canine distally, away from the lateral-incisor root, an elastomeric module was tied from a ligature wire extending out of the tissue to a lingual button on the first molar. Two months later, the right canine was exposed, and the same treatment protocol was followed.
Three to four months later, the direction of force application was changed from distal to vertical (Fig. 3). During this stage, precision cutouts were incorporated in the labial canine areas of the aligners. To apply extrusive and Class II forces simultaneously, the patient was instructed to wear elastics (3⁄16", 3.5oz) from the cutouts to lingual hooks on the canines during the day and from the hooks to the lower first and second premolars at night.

Fig. 3 Case 1. Elastics attached from lingual hooks to labial cutouts on trays to exert vertical force on impacted canines.
After three stages of treatment with 118 sets of aligners, changed weekly, the canines had partially erupted, and the first refinement stage began. Twenty-six sets of aligners, changed every week, were used for this phase. Esthetic buttons were bonded to the labial sides of the impacted canines, and traction continued with elastics (3⁄16", 3.5oz) worn from the upper canines to the lower canines and first premolars and from the upper canines to the second molars (Fig. 4A). Vertical rectangular attachments were added to the lingual surfaces of the canines to correct their rotations during extrusion (Fig. 4B).

Fig. 4 Case 1. A. Application of vertical force using elastics attached from impacted canines to lower canines and first premolars, and from upper canines to second molars (continued in next image).
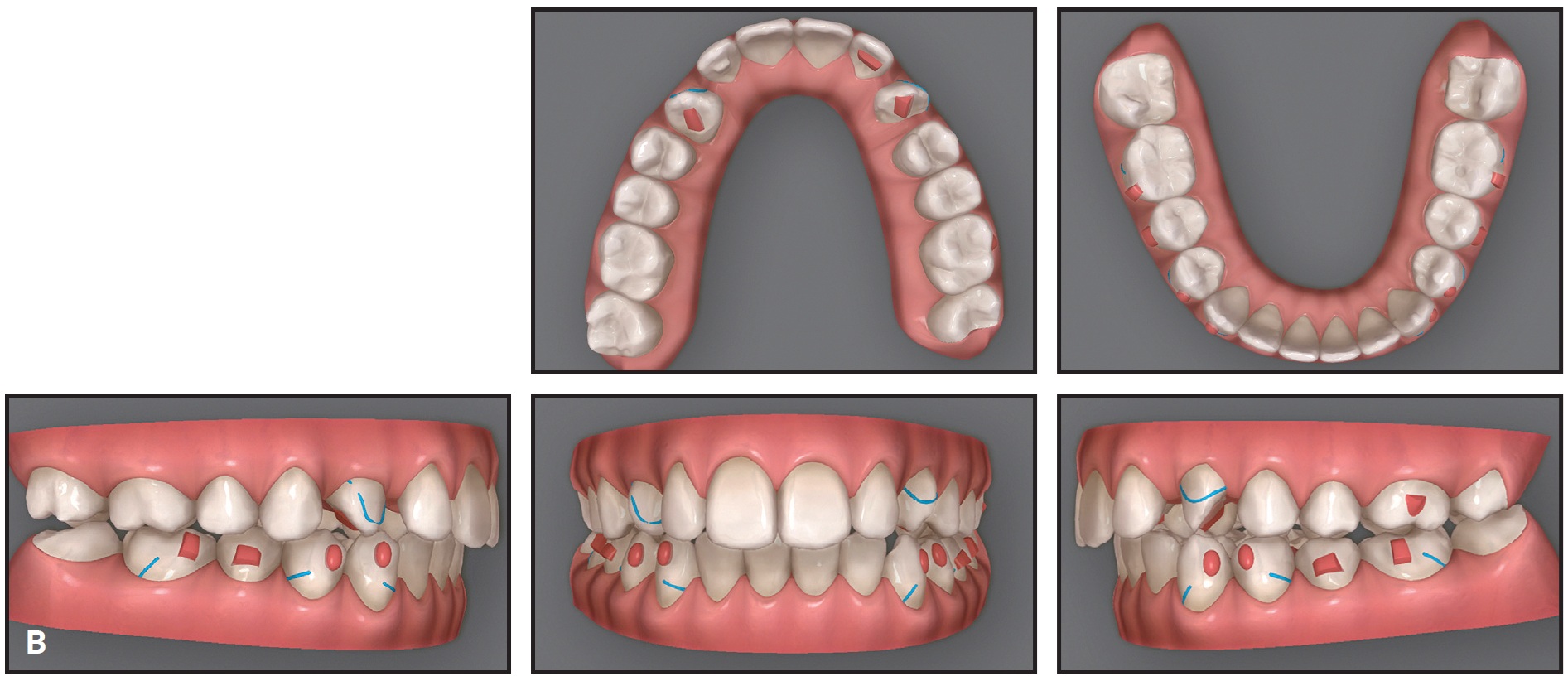
Fig. 4 (cont.) Case 1. B. ClinCheck plan of first refinement stage, showing use of lingual attachments on canines to improve aligner retention during extrusion and rotation.
In the final refinement phase, involving 34 sets of aligners, changed weekly, bilateral vertical cross-elastics (1⁄8", 4.5oz) were used to apply a counterclockwise moment and improve the torque of the canines while they were extruded into the arch (Fig. 5).
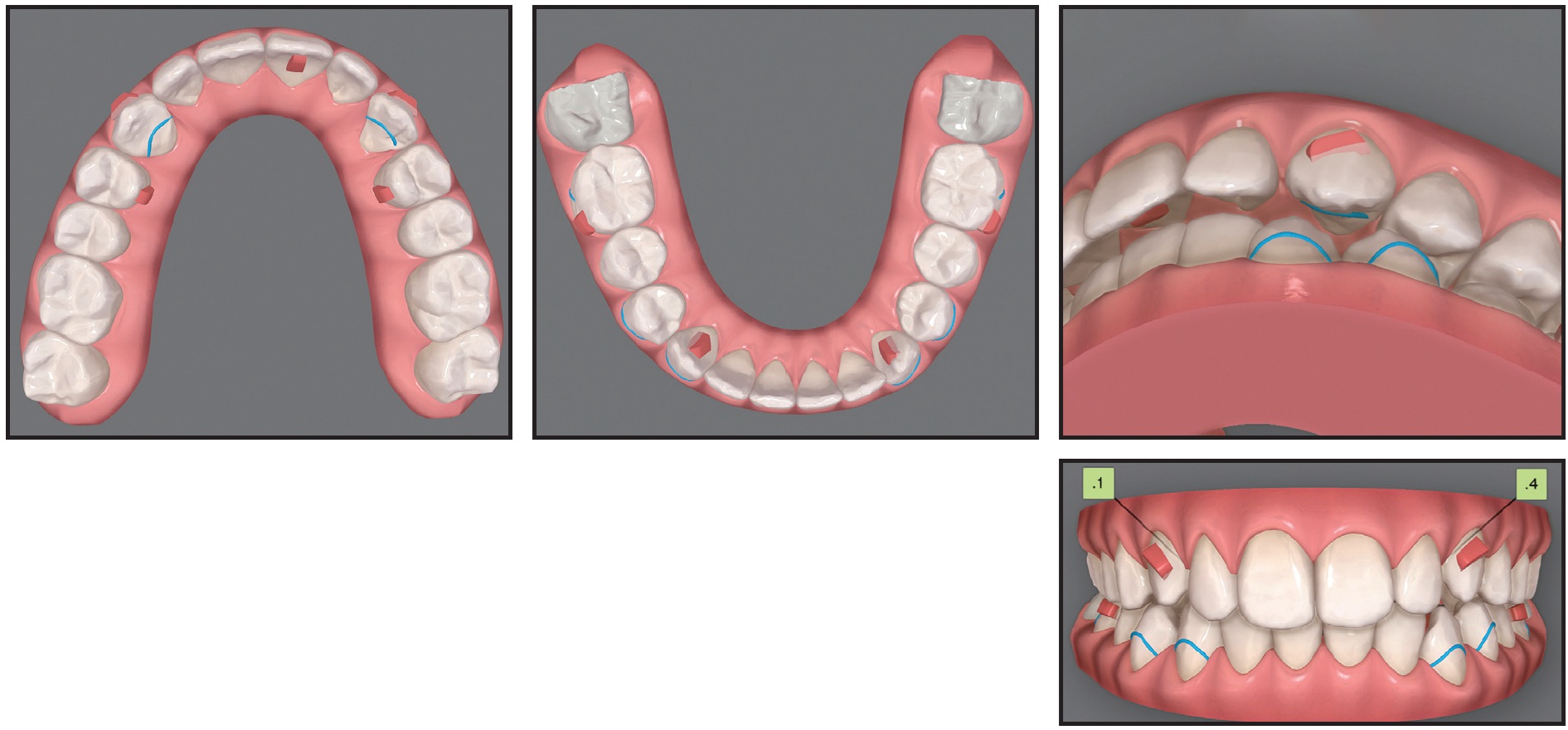
Fig. 5 Case 1. ClinCheck plan of final refinement stage, with vertical cross-elastics attached from lingual sides of canines to buccal sides of lower premolars to apply lingual root torque.
After a total 36 months of treatment, the alignment and torque of the canines were corrected, with both sides in occlusion (Fig. 6). Gingivectomies of both canines were performed to obtain even gingival margins.
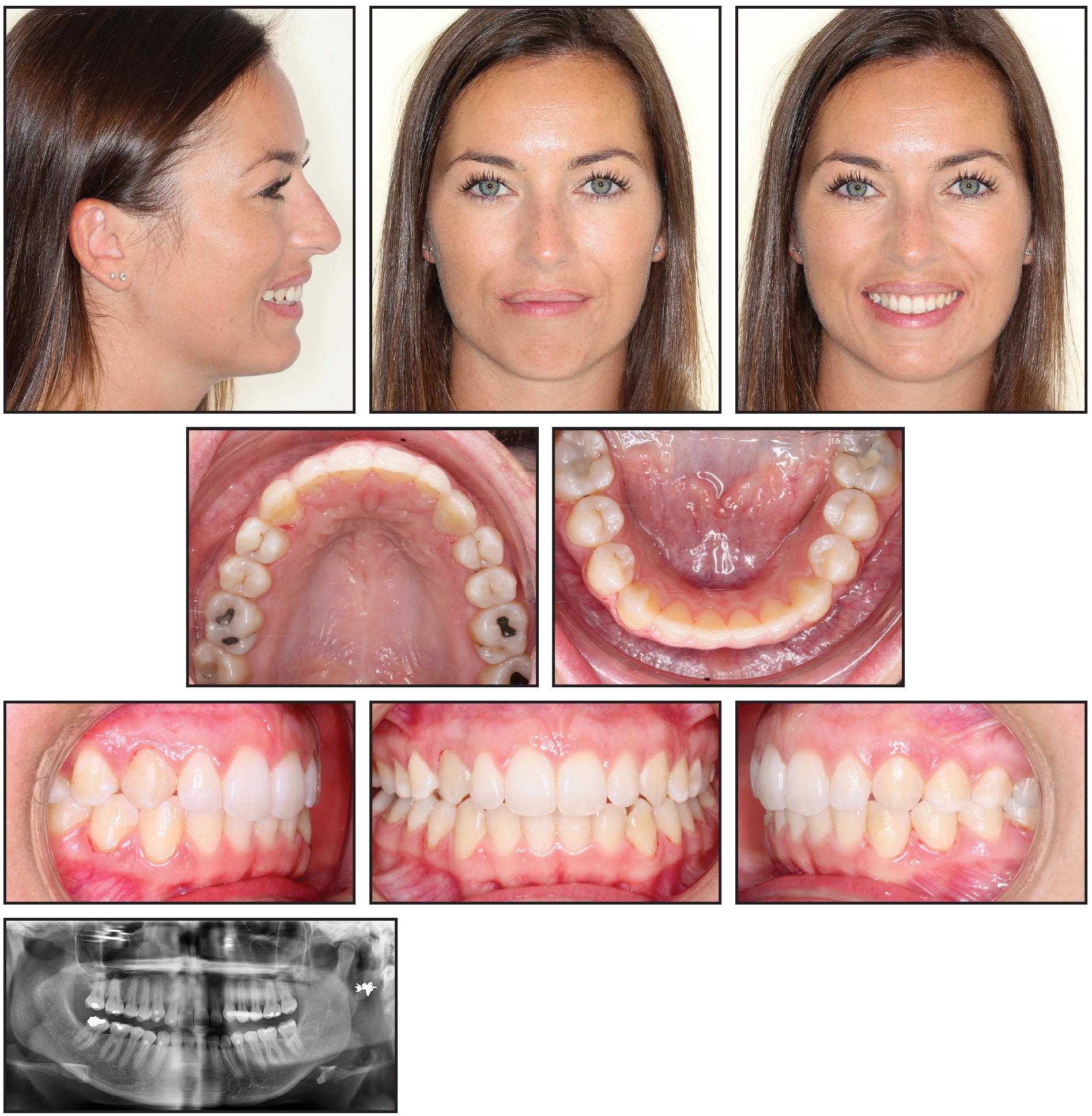
Fig. 6 Case 1. Patient after three years of treatment, showing well-aligned canines.
Case 2: Using Fixed Appliances as Auxiliaries
A 19-year-old female presented with the chief complaint of irregular anterior teeth (Fig. 7). The patient had a balanced, well-proportioned soft-tissue profile. The smile arc was non-consonant, with more gingival display on the right posterior side than on the left. The upper right deciduous canine was retained, and the upper second premolars were palatally displaced on both sides. The maxillary arch was constricted and V-shaped; a bilateral posterior lingual crossbite and excessive overjet were noted.
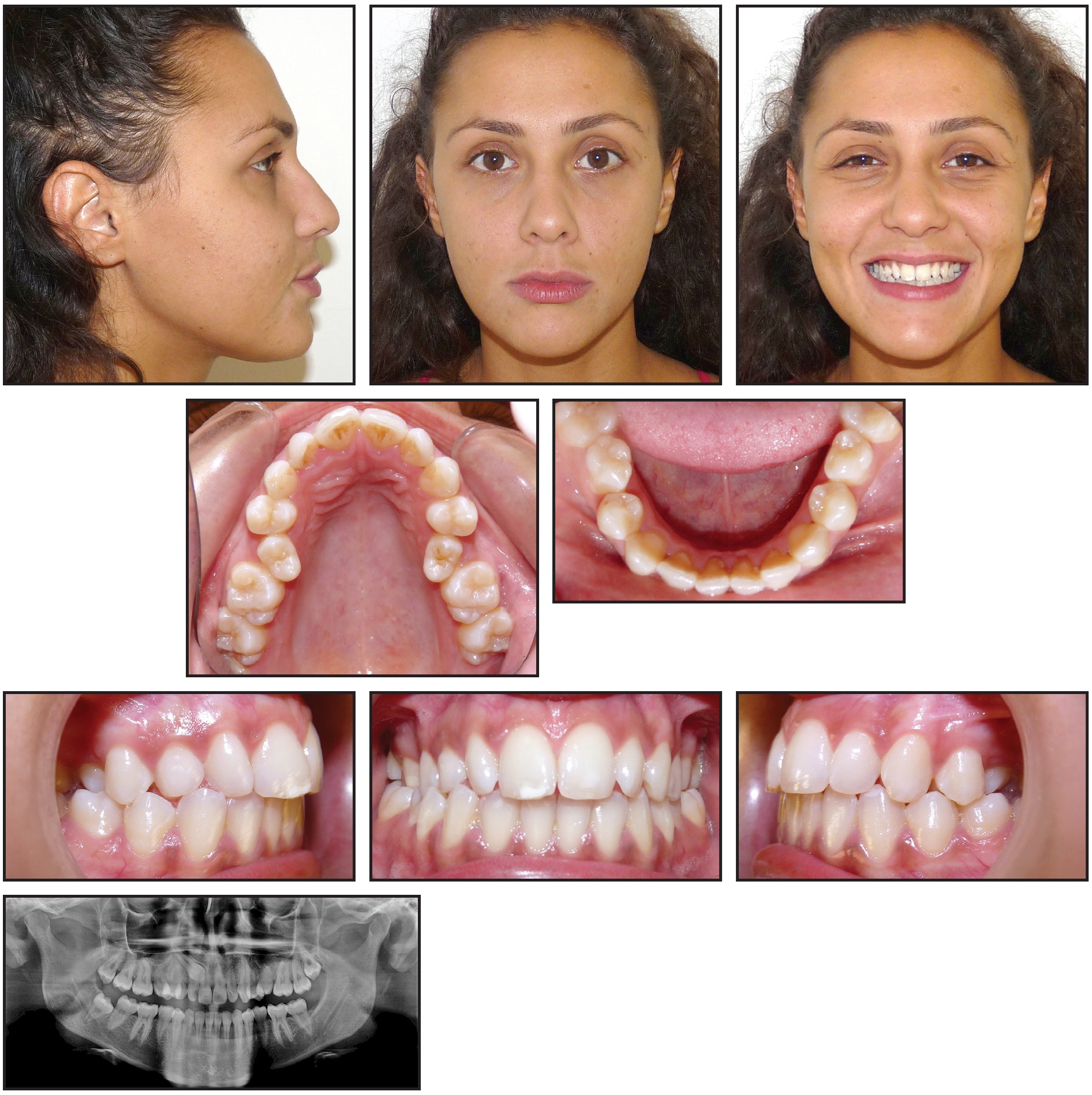
Fig. 7 Case 2. 19-year-old female patient with impacted upper right canine, constricted maxillary arch with bilateral posterior crossbite, and excessive overjet before treatment.
The panoramic radiograph revealed an impacted upper right canine overlapping the roots of the lateral and central incisors.
The treatment objectives were to alleviate the crowding, bring the upper right canine and both upper premolars into the arch, expand the maxillary arch to correct the crossbite, and achieve proper overjet and overbite. Clear aligners would be used, with fixed appliances as auxiliaries.
The treatment plan was divided into two stages (see box). The first, involving arch expansion and space preparation for the canine, would require 44 sets of aligners, changed weekly. In the second stage, which would involve 32 sets of aligners changed every two weeks, the canine would be exposed, and traction would be performed.
The first set of aligners was designed to expand the maxillary arch and prepare space for the upper premolars with sequential molar distalization (Fig. 8). Class II elastics (3⁄16", 4.5oz) were worn from the first premolars to the lower molars to prevent labial movement of the premolars. Next, the premolars were derotated and moved buccally into the arch. Using the contralateral canine’s mesiodistal width as a guide, about 7.5mm of space was prepared for the impacted canine.
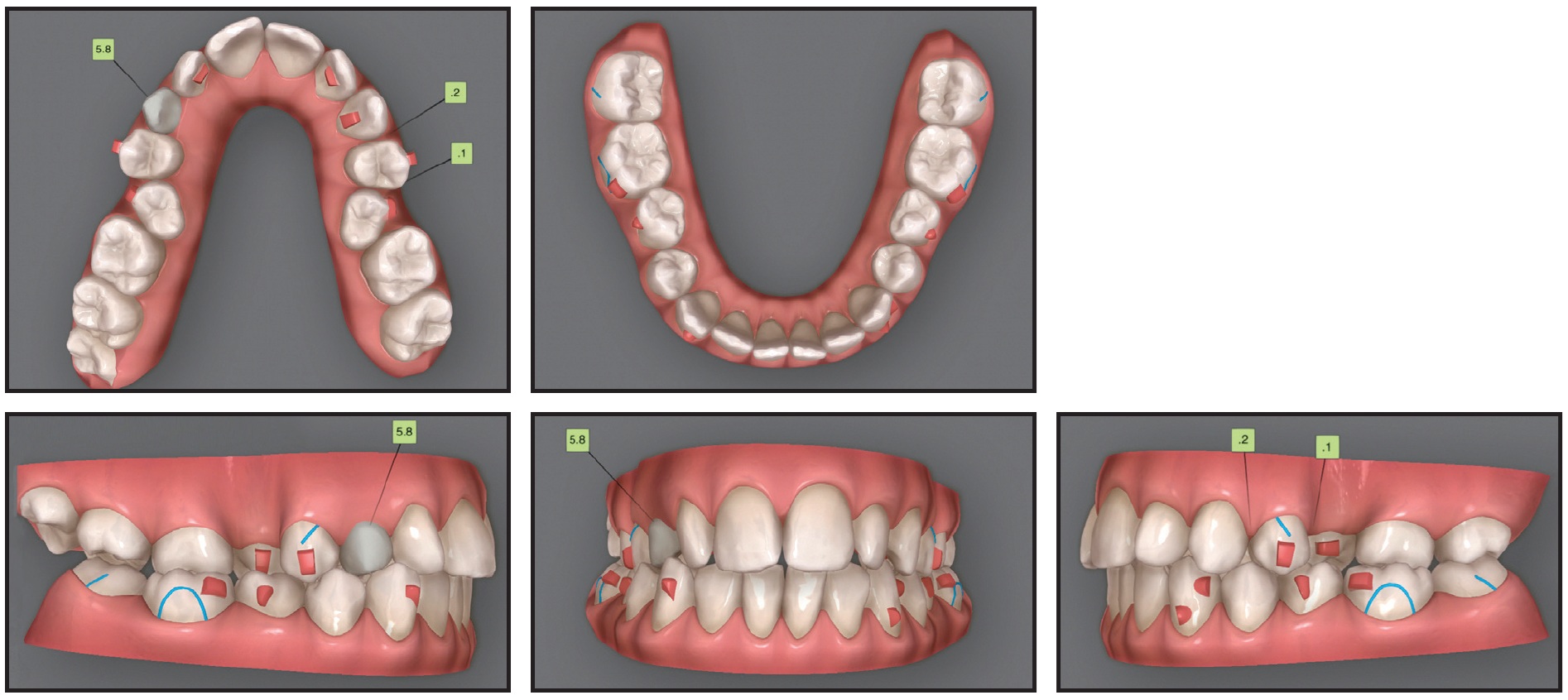
Fig. 8 Case 2. ClinCheck plan of first treatment stage, involving expansion of maxillary arch and preparation of space for impacted canine.
After two months, the canine was surgically exposed. A button was bonded to the labial side of the upper right first molar, and elastic thread was used to apply a distobuccal force vector, with the primary objective of moving the canine away from the incisor roots.
After the first stage of treatment, the canine was partially visible and had moved buccally into the arch. Because 30° of derotation would be required for alignment, in addition to extrusion and buccal root-torquing movements, a lingual fixed appliance would be used as an auxiliary; the ClinCheck* plan was modified accordingly (Fig. 9). Lingual .022" Victory** lower-incisor twin brackets were bonded from the upper right central incisor to the second premolar, and an .016" nickel titanium lingual archwire was engaged to correct the rotation. At the same time, clear aligners were used to extrude the upper right canine, with elastics (3⁄16", 3.5oz) worn from the canine hook to cutouts on the labial sides of the canine and first premolar.
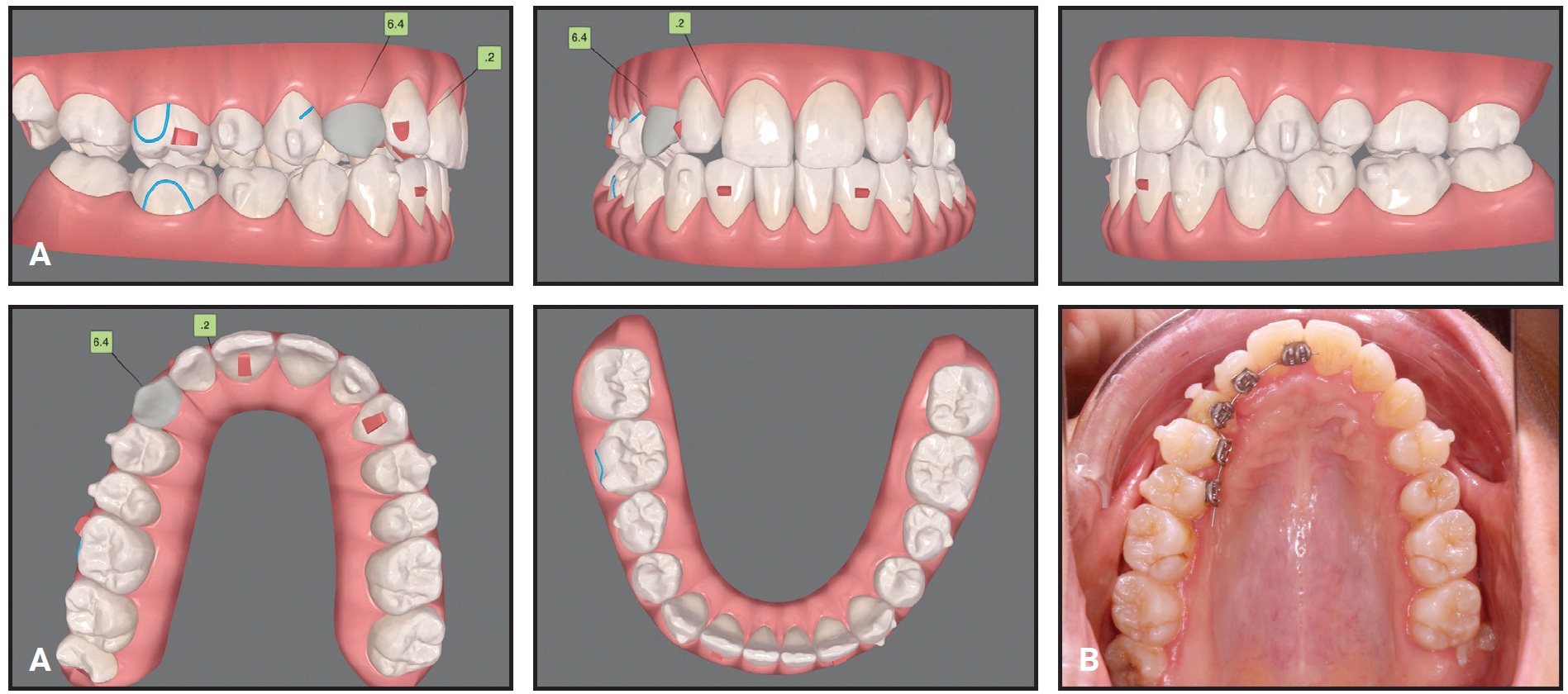
Fig. 9 Case 2. A. ClinCheck plan of first refinement stage, showing modifications to account for use of sectional fixed appliance on lingual side of upper right segment. B. Fixed lingual appliance used as auxiliary during first refinement stage.
Four months later, buccal root torque was applied to the canine with an .016" × .022" rectangular TMA*** lingual archwire. During the detailing phase, the fixed lingual appliance was removed, and treatment continued with 12 sets of clear aligners, changed weekly. To reduce the visibility of the attachments, they were placed on the lingual sides of all upper anterior teeth except the right canine.
After 30 months of active treatment, the maxillary and mandibular arches were well aligned, the posterior crossbite was corrected, the overjet and overbite were within normal ranges, and bilateral Class I canine and molar relationships were obtained (Fig. 10). At the end of treatment, a gingivectomy of the canine was performed to align its soft-tissue contours with those of the adjacent teeth.
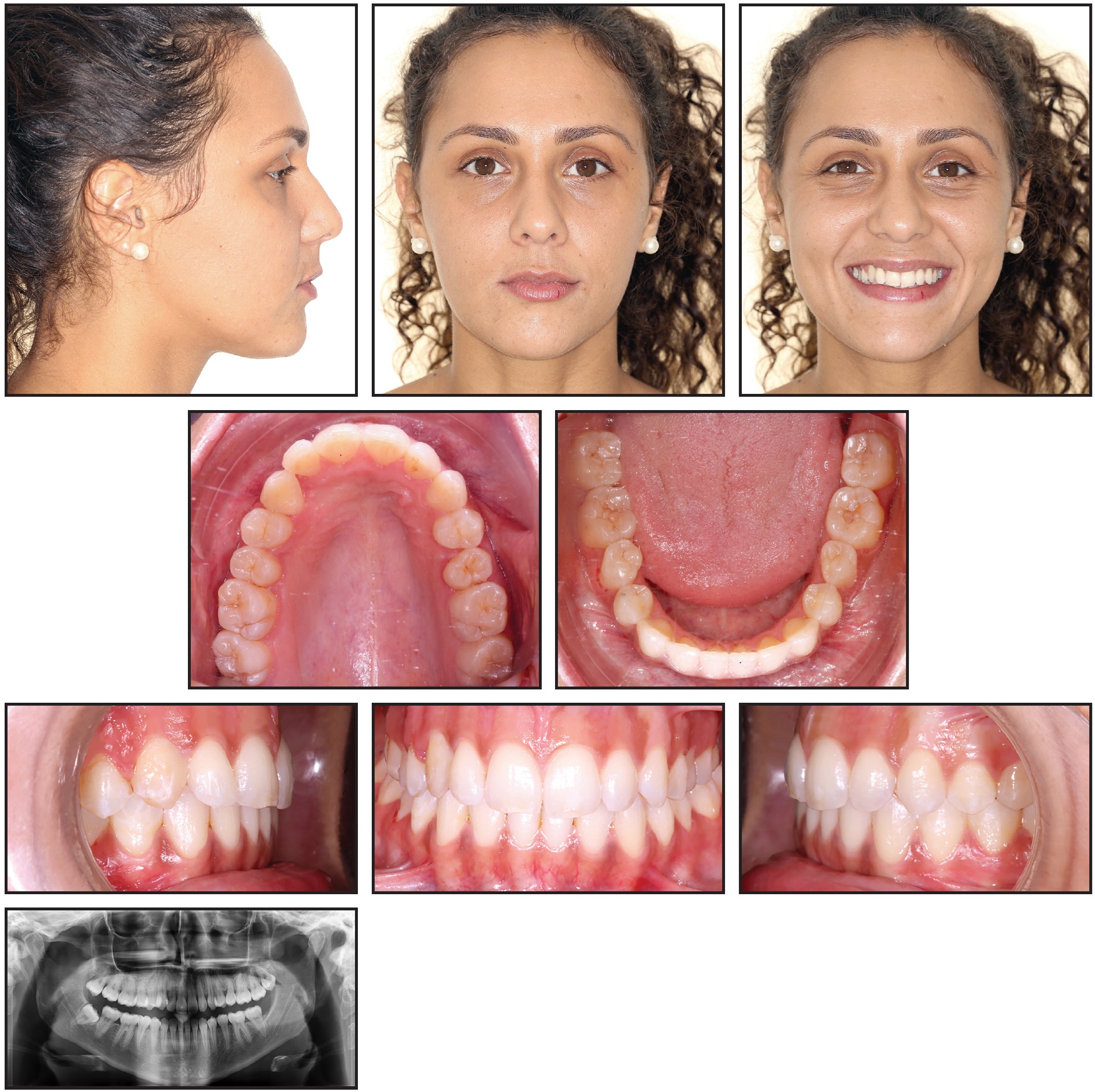
Fig. 10 Case 2. Patient after 30 months of treatment, showing alignment of impacted upper right canine, correction of posterior crossbite, and normalization of overjet and overbite.
Case 3: Applying Traction Forces with Different Vectors
A 29-year-old male presented with the chief complaint of a gap between his upper front teeth (Fig. 11). The soft-tissue profile was straight, with mildly retrusive upper and lower lips, 50% incisor display in smiling, and a flat smile arc. The mandibular midline was deviated 3mm to the left of the facial midline, and there was a 2mm diastema between the upper central incisors; the overbite was 1-2mm. Class III molar and canine relationships were present on the right side, and Class I relationships on the left. The maxillary arch was constricted compared to the mandibular arch, with a crossbite from the left canine to the left second molar. The lower left deciduous canine was retained, and mild crowding was noted in the mandibular arch. The upper right lateral incisor was in an edge-to-edge relationship with the lower right canine, while the upper left incisor was in an anterior crossbite. Bolton analysis indicated a 2.07mm mandibular excess due to the narrow mesiodistal width of the upper lateral incisors (6mm each).
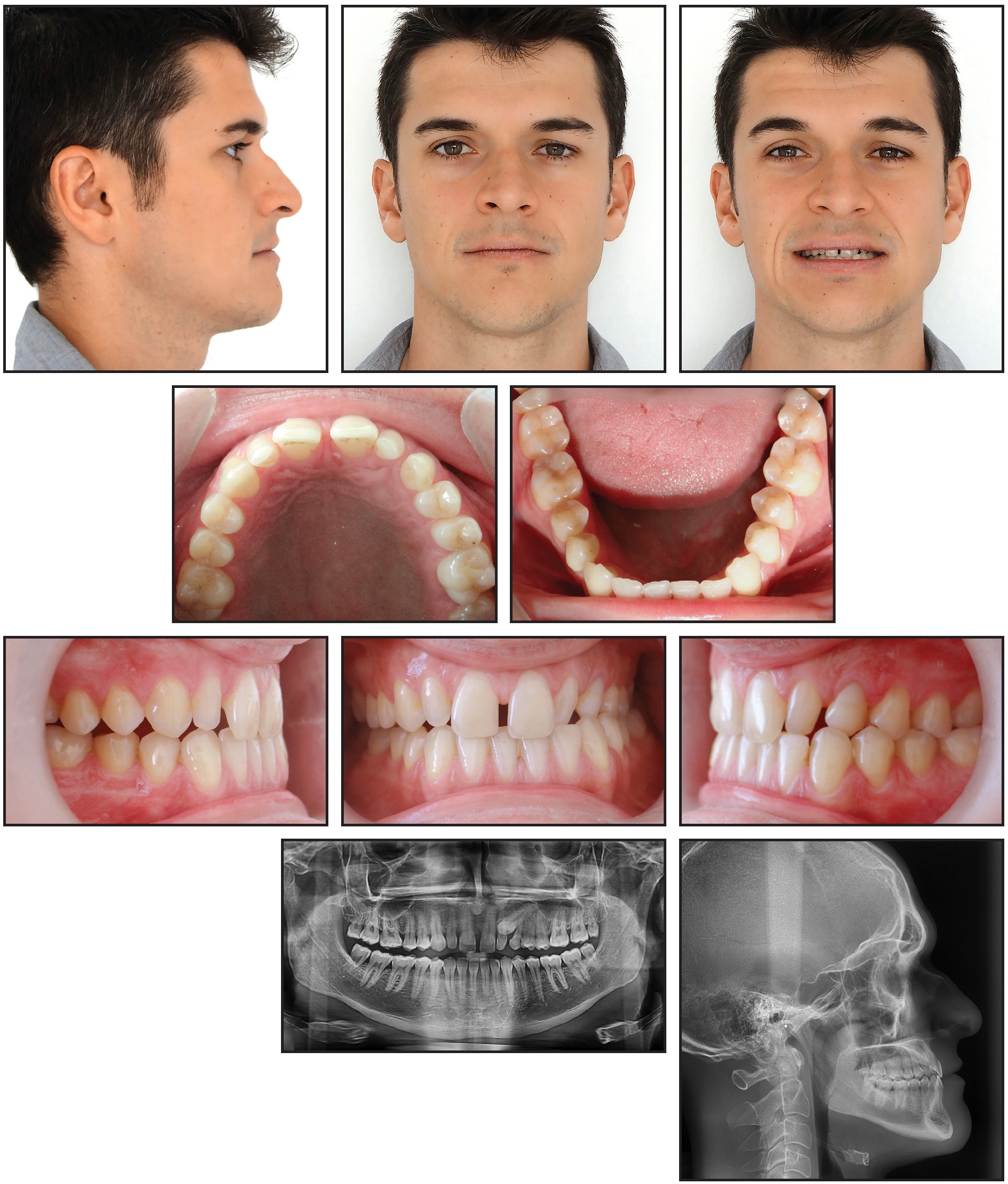
Fig. 11 Case 3. 29-year-old male patient with horizontally impacted upper left canine, diastema between upper central incisors, Class III molar and canine relationships on right side, left buccal crossbite, and Bolton discrepancy before treatment.
The panoramic radiograph revealed that the upper left canine was horizontally impacted, overlapping the root of the upper left lateral incisor. Cephalometric analysis indicated a Class III skeletal relationship (ANB = –1°, Wits appraisal = –3mm) with a normal vertical dimension (MPA = 34°). Both the upper and lower incisors were retroclined.
Treatment objectives were to bring the impacted canine into the arch and obtain Class I molar and canine relationships, along with a normal overjet and overbite. The Bolton discrepancy would be addressed with porcelain veneers on the upper lateral incisors. The goals of clear aligner treatment (see box) were to expand the maxillary arch, procline the incisors, close the space between the upper central incisors, prepare space in the arch for the impacted canine, and correct the Class III relationship and midline deviation, using Class III elastics for bite stimulation (Fig. 12).
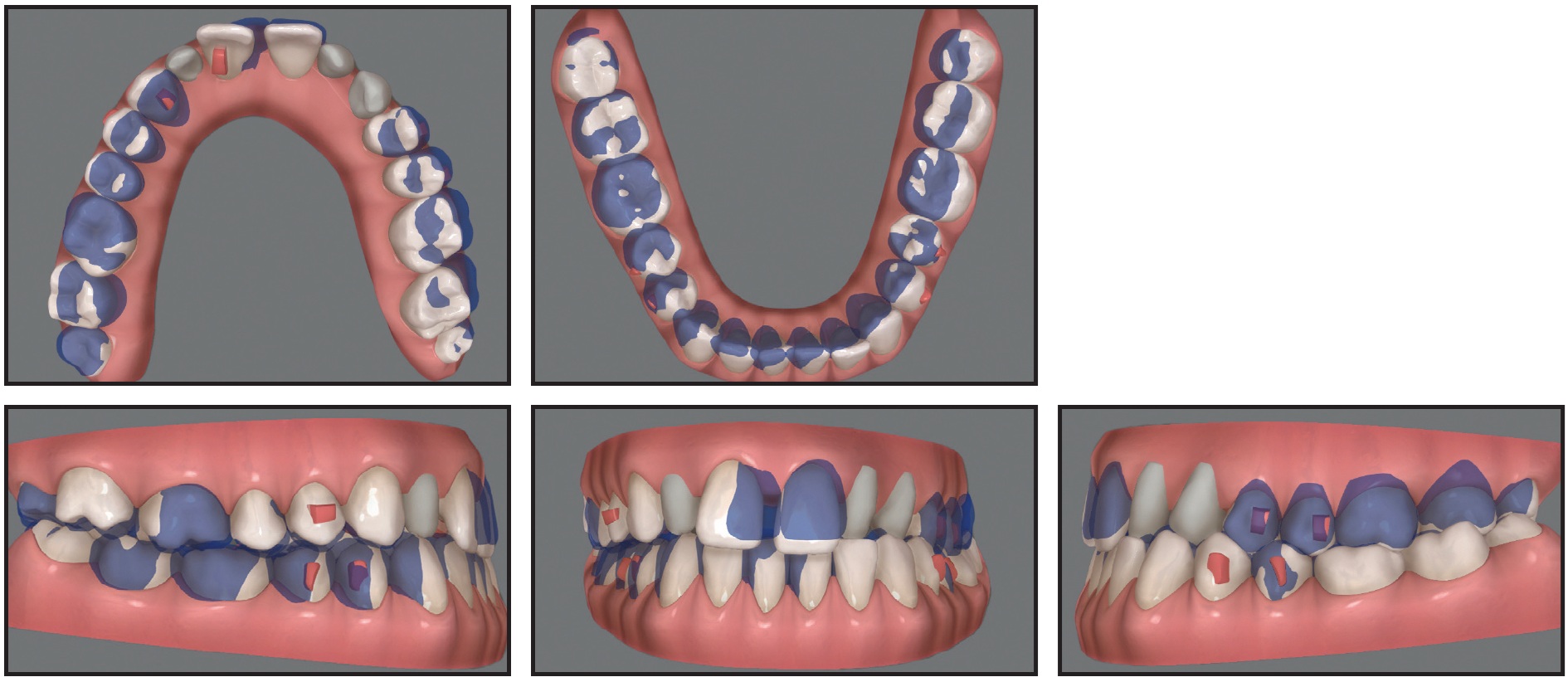
Fig. 12 Case 3. ClinCheck superimposition of initial (white) and planned (purple) tooth movements for first set of aligners.
The impacted canine was exposed using the closed surgical technique, and a distal force vector was applied immediately to upright the tooth while moving it away from the lateral incisor (Fig. 13).
Four months after traction began, the canine crown had erupted into the arch. A vertical force vector was applied using 3⁄16", 4.5oz vertical elastics, worn at night from a lingual button on the canine to an undercut on the labial side, and 1⁄8", 4.5oz elastics, worn during the day from the button to the opposite arch.
After 14 months of treatment, three-quarters of the canine was exposed. Refinement trays were delivered to begin the derotation. The lingual button was then removed, and a lingual vertical attachment was bonded for aligner retention (Fig. 14).

Fig. 13 Case 3. Elastomeric chain tied from impacted canine to first molar to apply distal force vector.
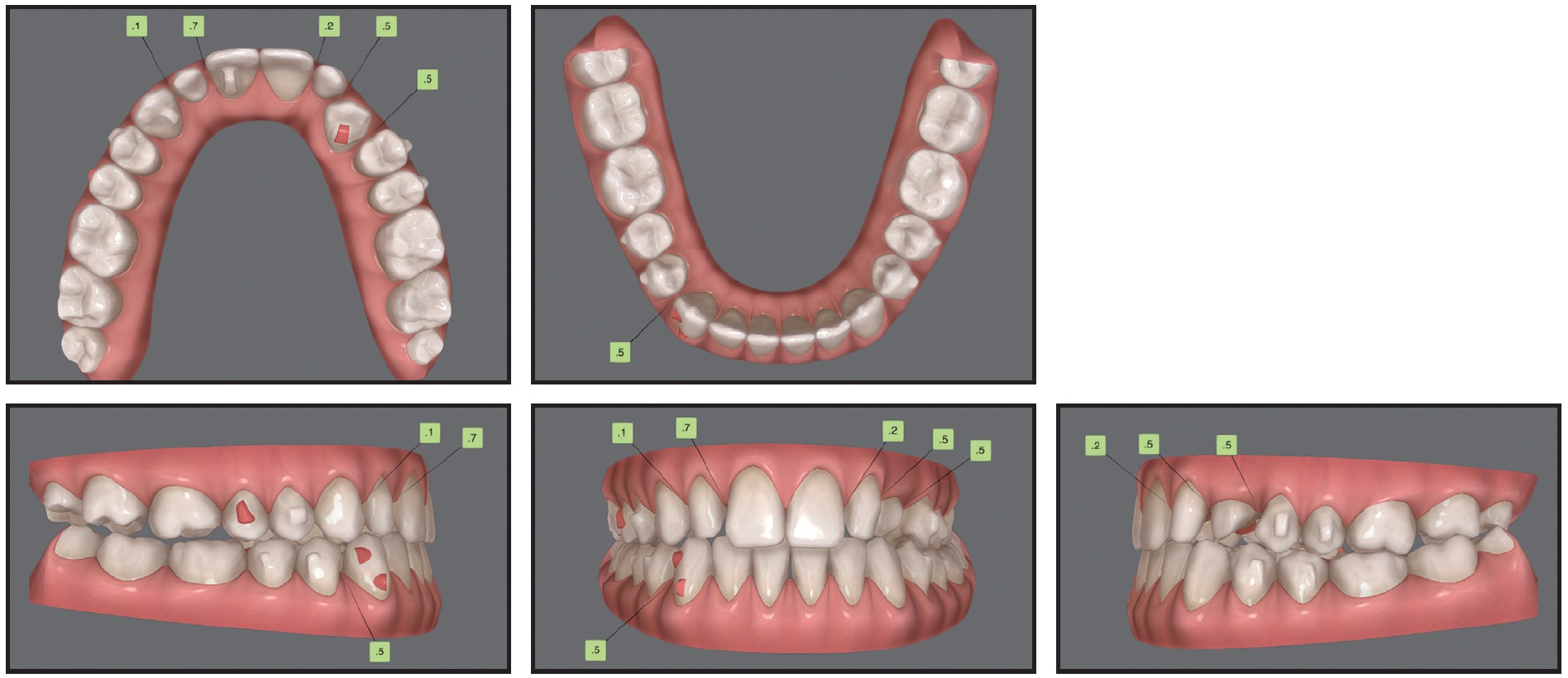
Fig. 14 Case 3. ClinCheck plan of refinement stage, with lingual attachment used to derotate canine.
After 30 months of treatment, involving 27 sets of aligners for the initial treatment and five sets for refinement, changed every two weeks, the left canine was fully aligned, and proper torque and root parallelism were obtained, with no signs of root resorption noted on the panoramic radiograph (Fig. 15). The upper lateral incisors were restored with porcelain veneers. The appearance of the smile had improved, with increased incisor display. The lower midline was coincident with the facial midline, and Class I canine and molar relationships were achieved.
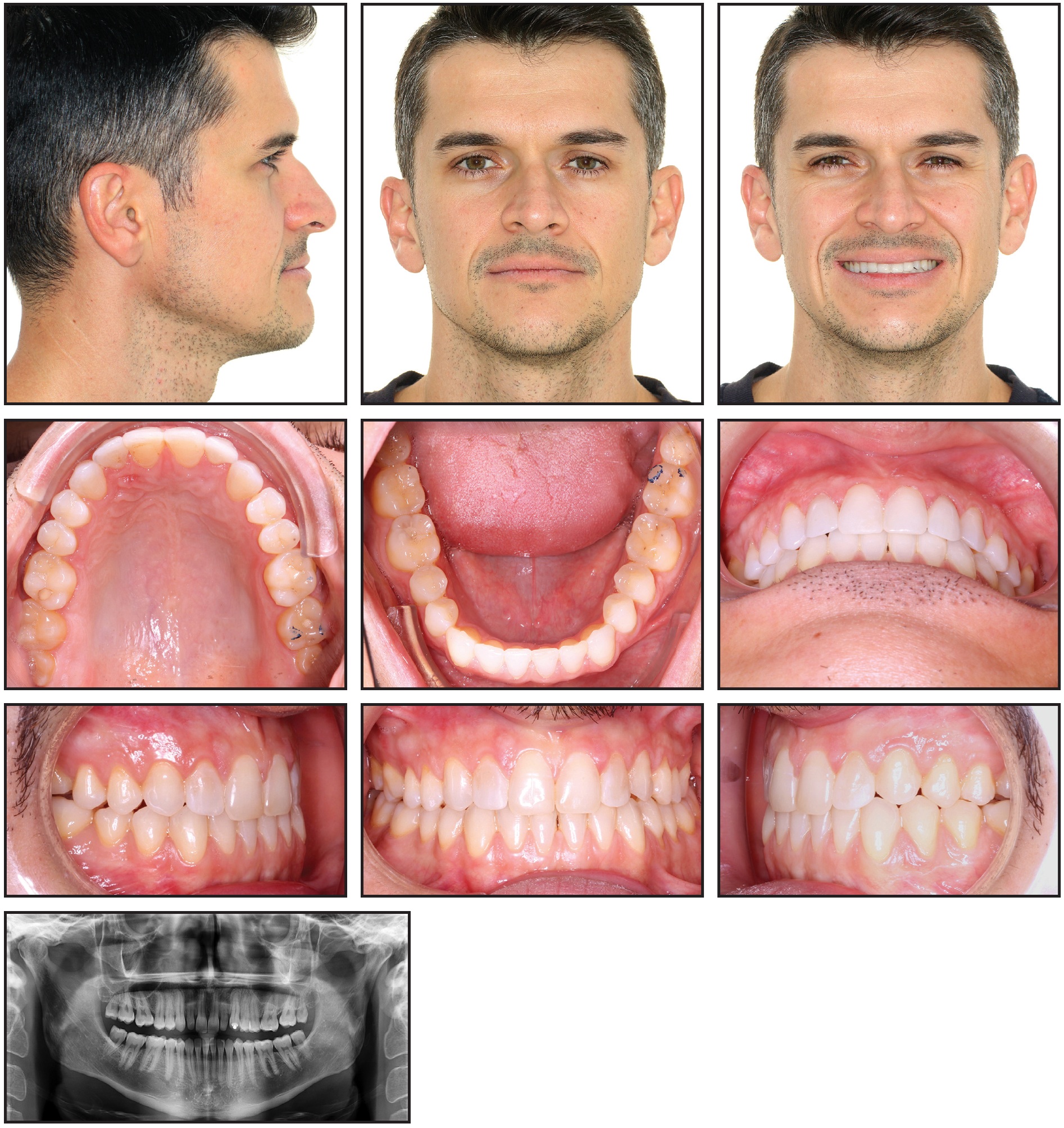
Fig. 15 Case 3. Patient after 30 months of treatment, showing aligned upper left canine, Class I canine and molar relationships, and improved smile appearance.
Discussion
Multiple factors can influence the success and duration of impacted-canine treatment. While the location and angulation of the canine will significantly affect treatment time,14,15 there are other factors under the orthodontist’s control, including the amount of space preparation, the magnitude and direction of the traction force, and the type and amount of anchorage.15
When fixed appliances are utilized, the surgical exposure and traction of the impacted canine are usually postponed until after alignment and space preparation, so that any crowding can be resolved and a full-size archwire engaged.16 By contrast, clear aligners allow canine traction to begin much earlier, often at the same time as alignment.16
In the three cases discussed above, tooth movement was divided into three stages: early traction of the impacted canine; distal tipping of the canine from the roots of the adjacent teeth; and uprighting of the crown by application of an occlusal and distal force vector, usually by means of elastomeric modules attached from the canine to the molar.
Anchorage preparation is critical to successful canine traction. To prevent uncontrolled movement of the anchorage teeth, multiple attachments can be added, Class II elastics can be worn to counteract the mesial force exerted on the anchorage unit, and the duration of the stage can be limited to three or four months.
During the second stage, the elastic patterns are alternated between day and night wear to apply the traction force, mainly in a vertical direction. In the first pattern, the elastics are attached from one side of the canine to a gingival undercut or precision cut on the other side of the same tooth, like a hammock. In the other, the elastics are attached to buttons on the opposing teeth, which provide anchorage. We strongly recommend limiting canine movement to extrusion during this stage. Considering the unpredictable nature of rotational movements,8 an attempt to derotate the tooth at this point might reduce the effectiveness of treatment or create non-tracking problems.
After about three-quarters of the crown is exposed, refinement can begin. This stage focuses on rotational correction, extrusion, and labial or palatal movement. Attachments and elastics or sectional fixed appliances can be used to improve both the efficiency and predictability of treatment. In some cases, lingual attachments and labial buttons can be used used to reliably perform simultaneous extrusion and derotation. When multiple types of tooth movement are required to align the impacted tooth, predictability can be increased by staging the treatment into separate phases of extrusion and rotation or incorporating sectional fixed appliances to carry out the rotational movement. For example, in our second case, a lingual sectional fixed appliance facilitated the rotational and torque correction without compromising esthetics.
Finally, it is essential to optimize anchorage control throughout the course of canine traction. In a finite-element analysis comparing clear aligners with fixed appliances for the treatment of labially impacted canines, Xia and colleagues noted that the initial magnitude and distribution of stress on the periodontal ligament of the canine and its subsequent displacement were similar regardless of treatment method.16 The main biomechanical difference between the two modalities was that clear aligners subjected the anchorage teeth to greater and more variable levels of stress, potentially resulting in uncontrolled movement. In the three cases shown here, we limited undesirable displacement of the anchorage teeth by adding attachments,17 by using the opposing arch to reinforce anchorage, or by splinting the anchorage units with sectional fixed appliances and archwires.
FOOTNOTES
- *Registered trademark of Align Technology, Inc., San Jose, CA; www.aligntech.com.
- **Registered trademark of Solventum, St. Paul, MN; www.solventum.com.
- ***Registered trademark of Ormco Corporation, Brea, CA; www.ormco.com.
REFERENCES
- 1. Sharma, R.; Drummond, R.; Wiltshire, W.; Schroth, R.; Lekic, M.; Bertone, M.; and Tate, R.: Quality of life in an adolescent orthodontic population, Angle Orthod. 91:718-724, 2021.
- 2. Jaber, S.T.; Hajeer, M.Y.; and Sultan, K.: Treatment effectiveness of clear aligners in correcting complicated and severe malocclusion cases compared to fixed orthodontic appliances: A systematic review, Cureus 15:e38311, 2023.
- 3. Bilello, G.; Fazio, M.; Amato, E.; Crivello, L.; Galvano, A.; and Currò, G.: Accuracy evaluation of orthodontic movements with aligners: A prospective observational study, Prog. Orthod. 23:12, 2022.
- 4. D’Apuzzo, F.; Perillo, L.; Carrico, C.K.; Castroflorio, T.; Grassia, V.; Lindauer, S.J.; and Shroff, B.: Clear aligner treatment: Different perspectives between orthodontists and general dentists, Prog. Orthod. 20:10, 2019.
- 5. Abu-Arqub, S.; Ahmida, A.; Da Cunha Godoy, L.; Kuo, C.L.; Upadhyay, M.; and Yadav, S.: Insight into clear aligner therapy protocols and preferences among members of the American Association of Orthodontists in the United States and Canada, Angle Orthod. 93:417-426, 2023.
- 6. Ericson, S. and Kurol, J.: Radiographic examination of ectopically erupting maxillary canines, Am. J. Orthod. 91:483-492, 1987.
- 7. Chapokas, A.R.; Almas, K.; and Schincaglia, G.P.: The impacted maxillary canine: A proposed classification for surgical exposure, Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 113:222-228, 2012.
- 8. Castroflorio, T.; Sedran, A.; Parrini, S.; Garino, F.; Reverdito, M.; Capuozzo, R.; Mutinelli, S.; Grybauskas, S.; Vaitiekūnas, M.; and Deregibus, A.: Predictability of orthodontic tooth movement with aligners: Effect of treatment design, Prog. Orthod. 24:2, 2023.
- 9. Bichu, Y.M.; Alwafi, A.; Liu, X.; Andrews, J.; Ludwig, B.; Bichu, A.Y.; and Zou, B.: Advances in orthodontic clear aligner materials, Bioact. Mater. 22:384-403, 2022.
- 10. Nucera, R.; Dolci, C.; Bellocchio, A.M.; Costa, S.; Barbera, S.; Rustico, L.; Farronato, M.; Militi, A.; and Portelli, M.: Effects of composite attachments on orthodontic clear aligners therapy: A systematic review, Mater. (Basel) 15:533, 2022.
- 11. Rossini, G.; Parrini, S.; Castroflorio, T.; Deregibus, A.; and Debernardi, C.L.: Efficacy of clear aligners in controlling orthodontic tooth movement: A systematic review, Angle Orthod. 85:881-889, 2015.
- 12. Dai, F.F.; Xu, T.M.; and Shu, G.: Comparison of achieved and predicted tooth movement of maxillary first molars and central incisors: First premolar extraction treatment with Invisalign, Angle Orthod. 89:679-687, 2019.
- 13. Savignano, R.; Valentino, R.; Razionale, A.V.; Michelotti, A.; Barone, S.; and D’Antò, V.: Biomechanical effects of different auxiliary-aligner designs for the extrusion of an upper central incisor: A finite element analysis, J. Healthc. Eng. 2019:9687127, 2019.
- 14. Grisar, K.; Luyten, J.; Preda, F.; Martin, C.; Hoppenreijs, T.; Politis, C.; and Jacobs, R.: Interventions for impacted maxillary canines: A systematic review of the relationship between initial canine position and treatment outcome, Orthod. Craniofac. Res. 24:180-193, 2021.
- 15. Arriola-Guillén, L.E.; Aliaga-Del Castillo, A.; Ruíz-Mora, G.A.; Rodríguez-Cárdenas, Y.A.; and Dias-Da Silveira, H.L.: Influence of maxillary canine impaction characteristics and factors associated with orthodontic treatment on the duration of active orthodontic traction, Am. J. Orthod. 156:391-400, 2019.
- 16. Xia, Q.; He, Y.; Jia, L.; Wang, C.; Wang, W.; Wang, C.; Song, J.; and Fan, Y.: Assessment of labially impacted canines traction mode with clear aligners vs. fixed appliance: A comparative study based on 3D finite element analysis, Front. Bioeng. Biotechnol. 10:1004223, 2022.
- 17. Gomez, J.P.; Peña, F.M.; Martínez, V.; Giraldo, D.C.; and Cardona, C.I.: Initial force systems during bodily tooth movement with plastic aligners and composite attachments: A three-dimensional finite element analysis, Angle Orthod. 85:454-460, 2015.
-
 DR. SABOUNI
DR. SABOUNI -
 DR. AZAMI
DR. AZAMI -
 DR. NANDA
DR. NANDA
Dr. Sabouni is an orthodontist consultant in the United Arab Emirates and France and a part-time lecturer, University of Dijon, France. He often lectures for Align Technology. Dr. Azami is the Program Director, Department of Orthodontics, School of Dental Medicine, UConn Health, Farmington, CT. Dr. Nanda is an Associate Editor of the Journal of Clinical Orthodontics; an Adjunct Professor, ADA Forsyth Institute, Cambridge, MA; and Professor Emeritus, Department of Orthodontics, School of Dental Medicine, University of Connecticut, 263 Farmington Ave., Farmington, CT 06030; e-mail: nanda@uchc.edu.
