The High-Pull Palatal Gear (HPPG) Technique for Treating Hyperdivergent Class II Malocclusions
Common clinical findings in patients with skeletal Class II malocclusions and hyperdivergent growth patterns include excessive gingival display in smiling, lip incompetence, and elongated lower faces. To reduce gingival exposure and improve facial esthetics, treatment often involves double-jaw orthognathic surgery: a Le Fort I osteotomy with maxillary impaction and a mandibular bilateral sagittal split osteotomy. With recent advances in the use of skeletal anchorage, however, double-arch intrusion has become an alternative to surgery, producing a favorable counterclockwise rotation of the mandible and thus increasing chin projection and enhancing the profile.1
This article describes the high-pull palatal gear (HPPG) technique, a simple method that creates force vectors similar to those of traditional high-pull headgear, without the associated discomfort and possibility of noncompliance. In this approach, a single midpalatal miniscrew is used to intrude the entire maxillary dentition on a rigid archwire, with light forces applied directly to lingual buttons on the lateral incisors. In combination with lower-arch intrusion anchored by bilateral miniscrews, the HPPG technique can be an effective alternative to surgery in the treatment of hyperdivergent Class II malocclusions.
The HPPG Technique
The anterior palate is a favorable site for skeletal anchorage because of its optimal bone quality and low risk of root contact. While a number of appliances with palatal miniscrews have shown promise in achieving various tooth movements, their fabrication often requires sophisticated laboratory work.2,3 The HPPG technique instead uses a single palatal miniscrew, simplifying preparation and enabling more accurate force direction (Fig. 1A).
The precise position of the miniscrew and hence the line of force relative to the center of resistance of the upper dentition will depend on the depth of the overbite, the desired change in the upper occlusal plane, and the planned upper-incisor positions.4 To promote counterclockwise rotation of the upper occlusal plane, an intrusive force should be applied in front of the center of resistance of the maxillary dentition. This can be accomplished by inserting a miniscrew in the anterior portion of the T-Zone, just behind the palatal rugae, where the failure rate is reported to be only 2.1%.5
Similar articles from the archive:
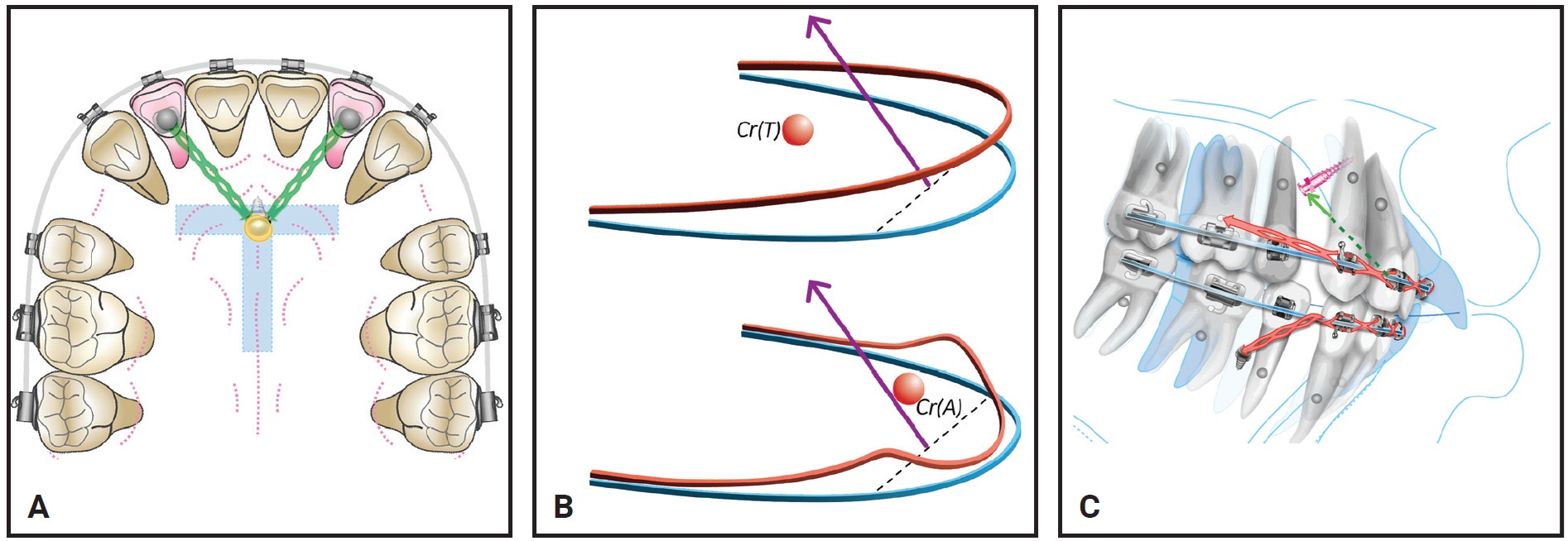
Fig. 1 High-pull palatal gear (HPPG) technique. A. Palatal miniscrew inserted in anterior portion of T-Zone and connected with elastomeric chains to lingual buttons on lateral incisors. B. Retracting lateral incisors on rigid archwire (above) transmits intrusion force to entire dentition; soft archwire (below) demonstrates side effects of force system (Cr(A) = center of resistance of anterior segment, Cr(T) = center of resistance of total arch). C. HPPG technique, with bilateral miniscrews inserted between lower first premolars and first molars, used for intrusion of both upper and lower dentitions.
Elastomeric chains are attached directly from the miniscrew to lingual buttons bonded to the lateral incisors, without extension arms, to deliver a reliable, vertically directed intrusive force. When a rigid archwire is inserted after space closure is nearly complete, this force can be transmitted to the whole arch, enabling intrusion and retraction of the entire maxillary dentition (Fig. 1B).
In a hyperdivergent Class II case, intrusion of the lower arch is often indicated to reduce lower facial height while preventing overintrusion of the upper incisors and avoiding anterior dental interferences. To promote clockwise rotation of the lower occlusal plane, more intrusion is needed in the anterior than the posterior region. Apically positioned lower miniscrews are inserted bilaterally to deliver intrusive forces in front of the center of resistance of the lower dentition (Fig. 1C).
Case Report
A 25-year-old male presented with the chief complaints of perioral protrusion and a gummy smile. Clinical examination showed a convex profile with a retrusive mandible and a long lower face, along with protrusive lips and an acute nasolabial angle (Fig. 2). The patient’s excessive gingival display in smiling and pronounced mentalis strain upon lip closure indicated significant vertical disharmony. A slight facial asymmetry was noted, with the maxillary dental midline deviated 1mm to the right of the facial midline and the mandibular midline 1mm to the right of the maxillary midline. The chin was also deviated 1.5mm to the right of the facial midline. A Class II canine relationship was present on the right side and a Class I canine relationship on the left, with bilateral Class I molar relationships. The overjet was 4mm, and the overbite was 2mm.
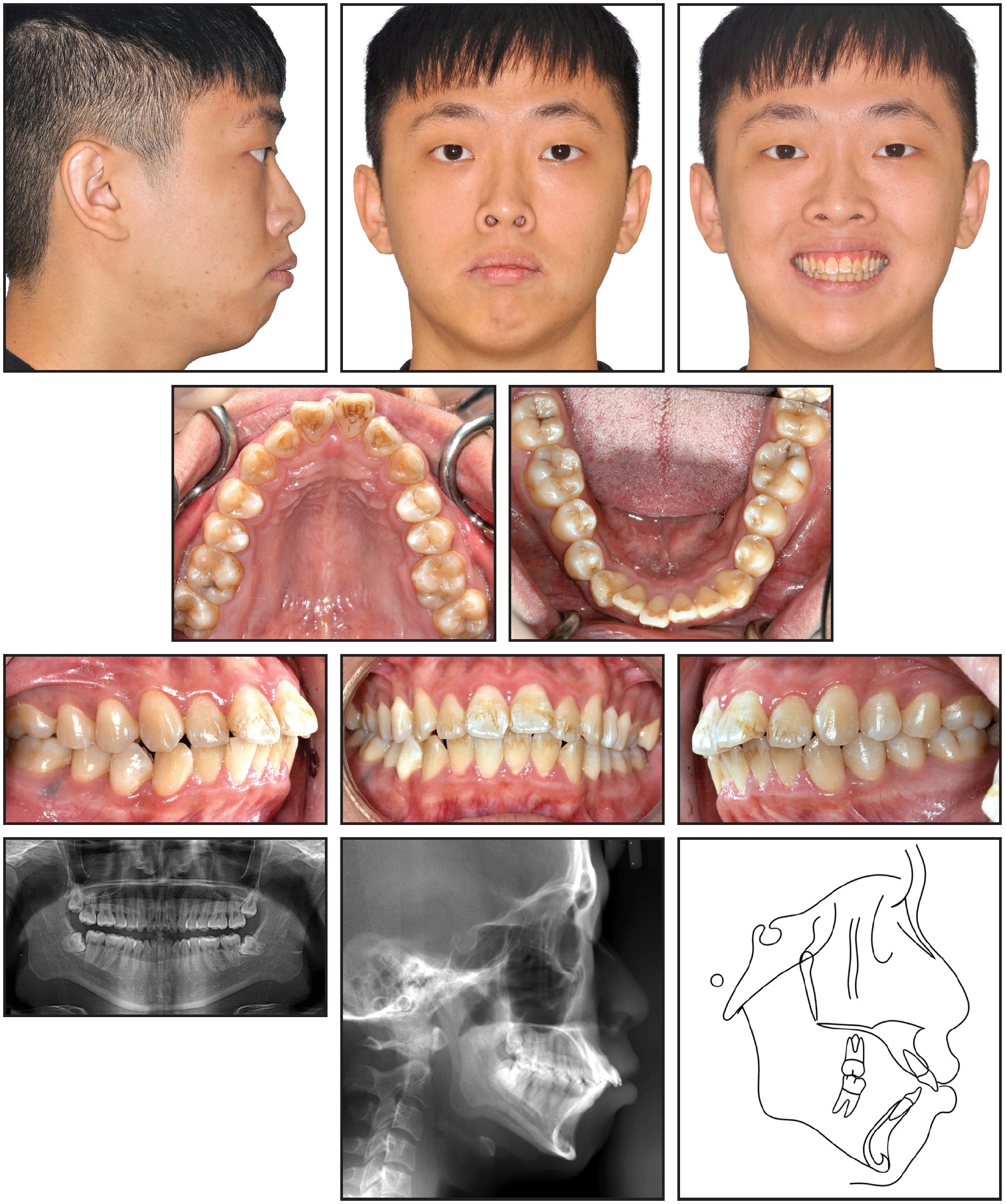
Fig. 2 25-year-old male patient with hyperdivergent Class II malocclusion, perioral protrusion, and excessive gingival display in smiling before treatment.
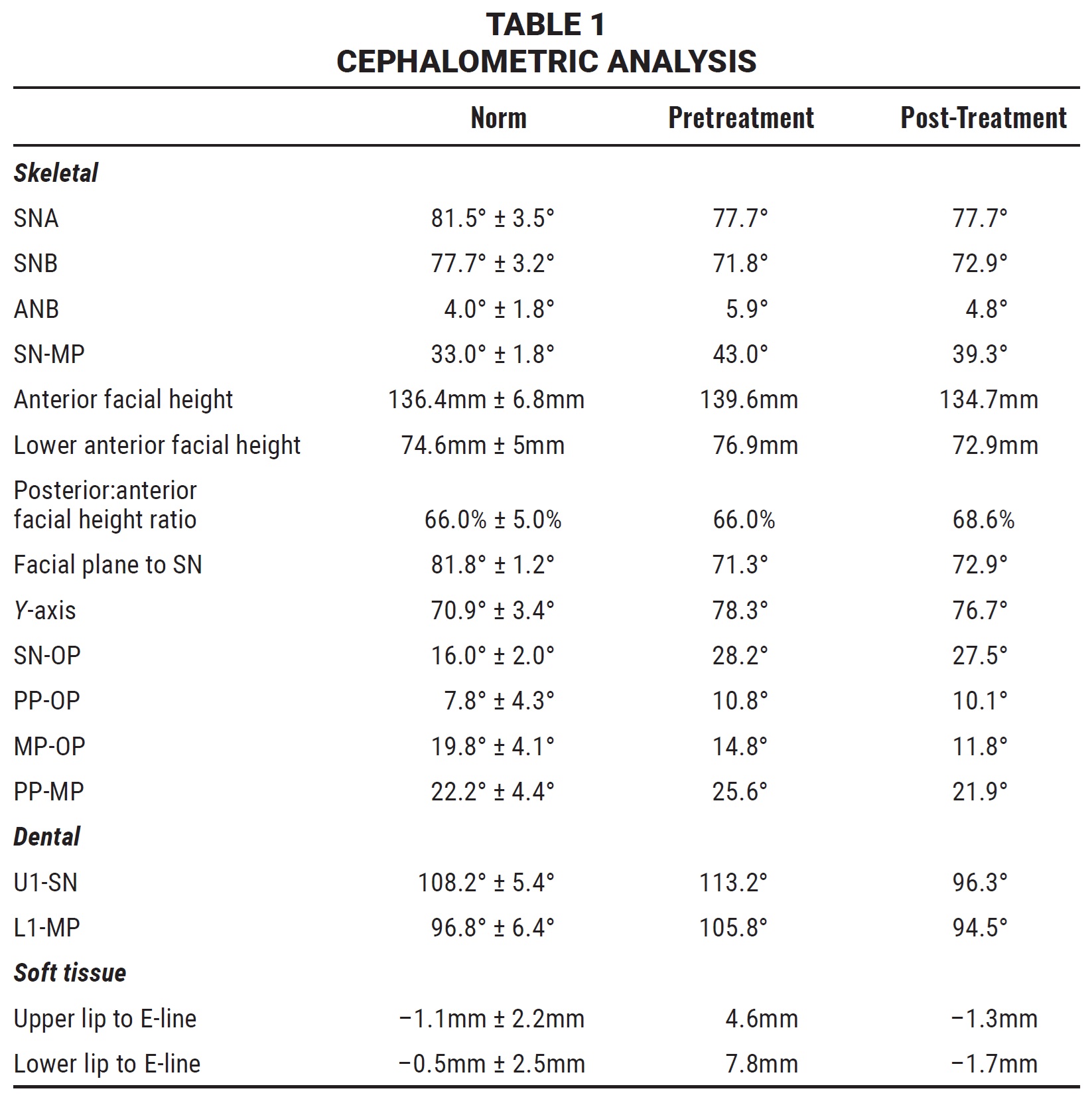
The panoramic radiograph revealed the impaction of all four third molars. The patient’s overall periodontal status was fair. Cephalometric analysis (Table 1) indicated a skeletal Class II malocclusion (SNA = 77.7°, SNB = 71.8°, ANB = 5.9°) with a high mandibular plane angle (SN-MP = 43°). The upper and lower incisors were proclined (U1-SN = 113.2°, L1-MP = 105.8°).
To improve the appearance of the profile, both the sagittal and vertical discrepancies would require correction. When the patient refused double-jaw orthognathic surgery, a nonsurgical approach was designed. The treatment plan involved extraction of the upper first and lower second premolars to make space for anterior retraction, as well as extraction of all third molars. The upper arch would be intruded with the HPPG technique, while bilateral miniscrews between the lower first premolars and first molars would anchor intrusion of the lower arch, thus promoting counterclockwise rotation of the upper occlusal and mandibular planes.
Treatment began with the bonding of .018" self-ligating brackets* in both arches for an initial stage of leveling and alignment with sequential nickel titanium wires. During this phase, the uprighting of the proclined upper incisors resulted in their relative extrusion and hence a steepening of the upper occlusal plane, necessitating more vertical control at a later stage.
After five months of leveling and alignment, the upper first and lower second premolars were extracted. Space closure began on .016" × .022" stainless steel wires in both arches, with an anti-bowing curve added to each wire to help prevent torque loss and keep the roots inside the alveolus, thus minimizing the risk of resorption.
After seven months of active treatment, a 1.5mm × 8mm midpalatal miniscrew** was inserted, and elastomeric chains were attached from the screw to lingual buttons bonded to the upper lateral incisors. Because the lateral incisors are near the center of resistance of the anterior segment, proper torque control and efficient intrusion of the upper anterior segment could be achieved during closure of the extraction spaces. The rate of space closure in each arch was coordinated to avoid producing anterior interferences. Over the course of treatment, a gradual improvement was observed in the gummy smile (Fig. 3).
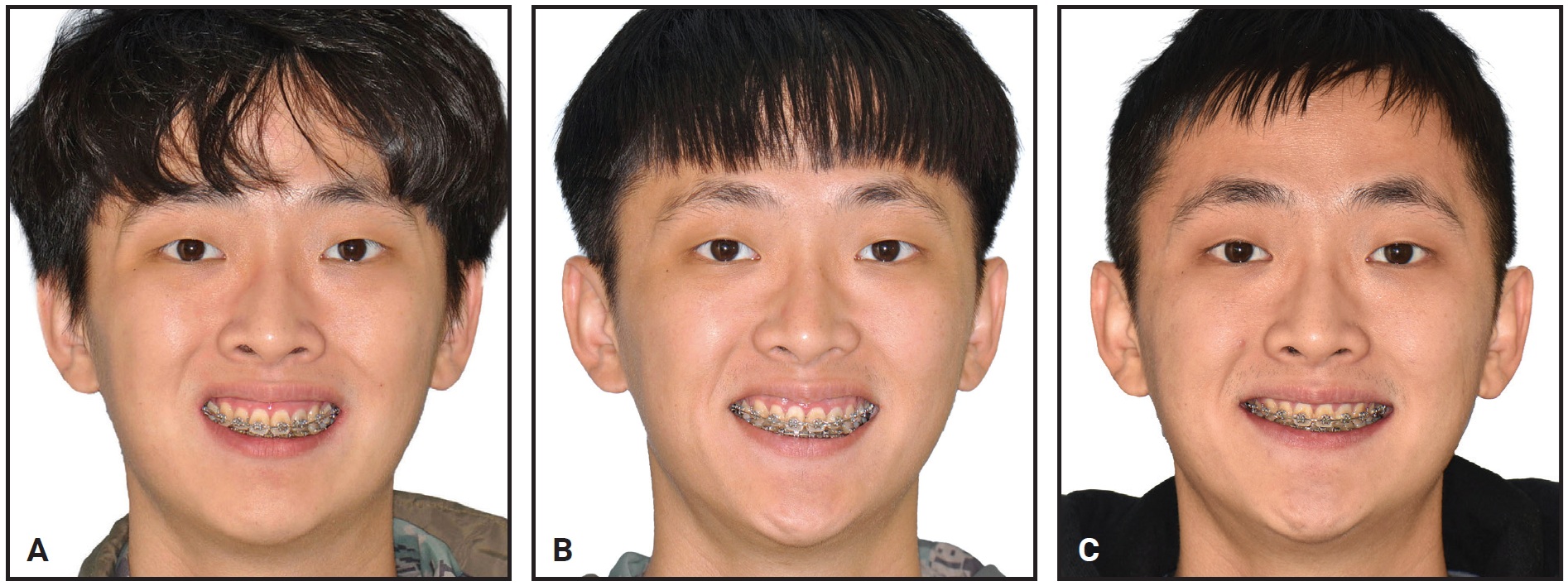
Fig. 3 Gradual reduction in gingival display in smiling. A. After eight months of active treatment. B. After 12 months. C. After 21 months.
After 22 months of treatment, the extraction spaces had almost closed. The upper archwire was changed to .017" × .025" stainless steel to reduce the play between the bracket slot and wire6 and to enable en-masse intrusion and distalization by the HPPG (Fig. 4). In the lower arch, tapered 1.4mm × 6mm bilateral miniscrews*** were inserted between the first premolars and first molars at the level of the mucogingival junction for delivery of an intrusive force; the lower archwire was also changed to .017" × .025" stainless steel to enhance en-masse intrusion with the miniscrew anchorage.
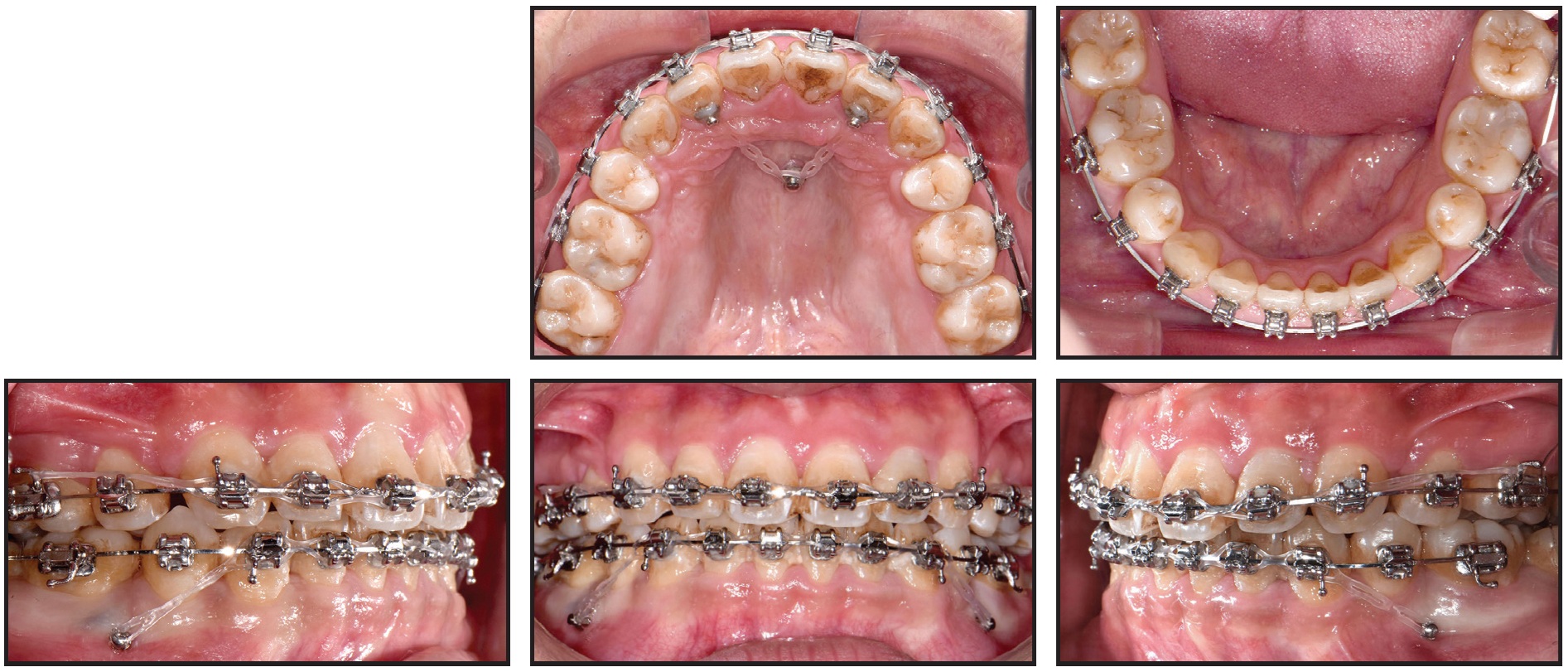
Fig. 4 After 23 months of treatment.
After a total 32 months of active treatment, all appliances were removed. Upper and lower Hawley retainers were delivered to be worn full-time for the first six months and then at night.
The patient expressed satisfaction with the treatment results (Fig. 5A). Class I canine and molar relationships were achieved on both sides. The lip protrusion and gingival display were reduced, and the chin projection improved considerably. The panoramic radiograph showed no obvious root resorption of the upper anterior teeth. Superimpositions of pre- and post-treatment cephalometric tracings confirmed intrusion of the entire maxillary and mandibular dentitions (Fig. 5B). The upper incisors were retracted 8mm and intruded 3.5mm, and the upper first molars were mesialized 1.5mm and intruded 1.5mm. The lower incisors were retracted 6mm and intruded 2mm, while the lower first molars were mesialized 1.5mm and intruded 1mm. Cephalometric analysis (Table 1) showed counterclockwise rotation of the mandible, with a 3.7° reduction in the mandibular plane angle (SN-MP = 39.3°). B point and pogonion moved upward and forward, while the ANB angle was reduced from 5.9° to 4.8°. The distances from the upper and lower lips to the E-line were brought into the normal range.
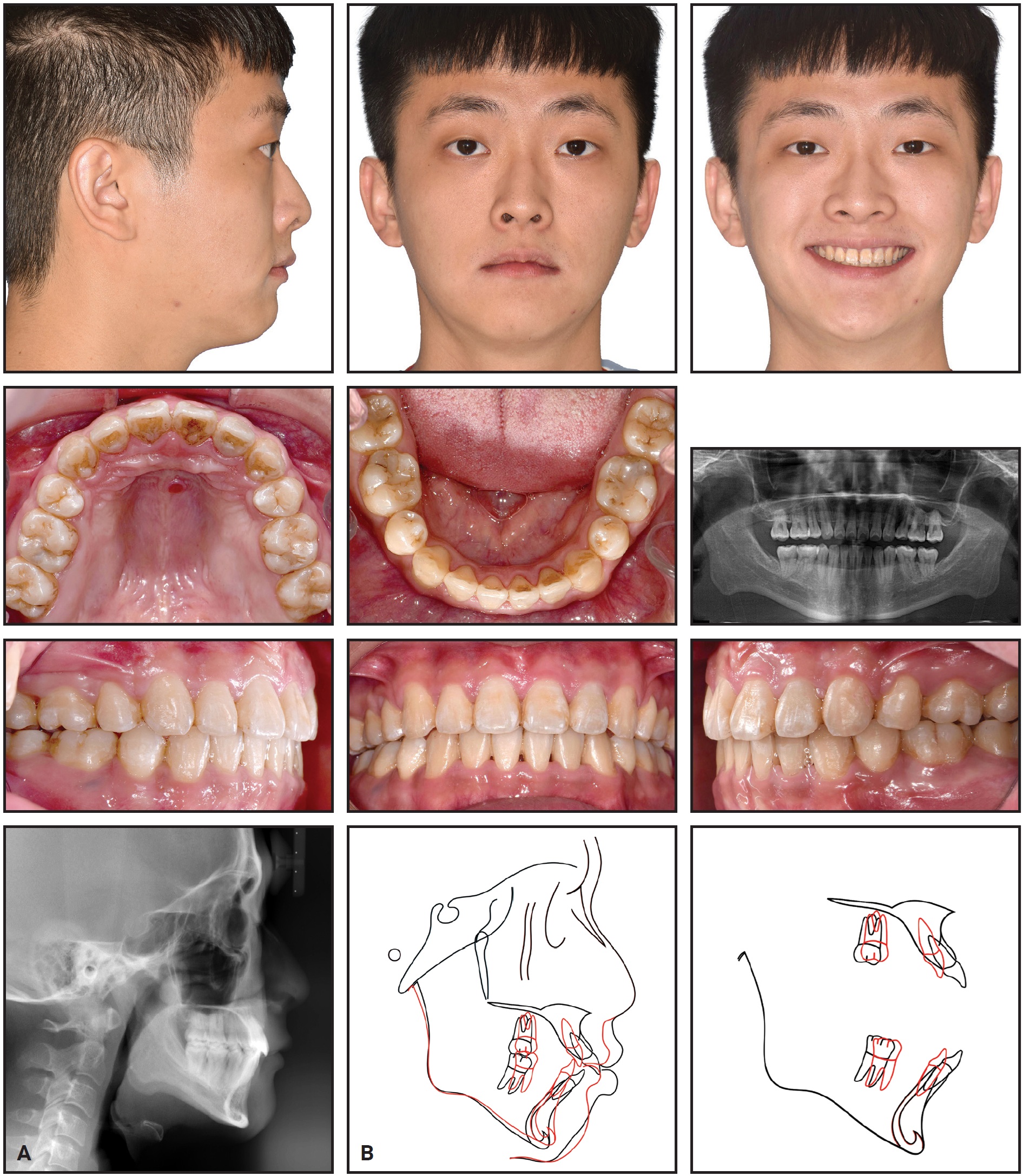
Fig. 5 A. Patient after 32 months of treatment. B. Superimposition of pretreatment (black) and post-treatment (red) cephalometric tracings.
The patient wore the retainers as directed, helping to preserve a harmonious facial profile and stable occlusion (Fig. 6).

Fig. 6 21 months after treatment, showing stable occlusion and preservation of facial profile.
Discussion
Vertical maxillary excess has been a common finding in multiethnic Asian skeletal Class II patients seeking orthognathic surgery, with a reported prevalence of 47%.7 Other than surgery, common methods for reducing the overjet and controlling the vertical dimension in hyperdivergent Class II cases include the use of fixed functional appliances, high-pull headgear, and premolar extractions. Heavy reliance on Class II elastics is contraindicated, since they can extrude the lower first molars, resulting in clockwise rotation of the mandible.
In recent years, the availability of skeletal anchorage has led to the proposal of various camouflage methods for treating hyperdivergent Class II cases by means of miniscrew-assisted upper-arch intrusion.1,8-11 Although interradicular buccal miniscrew placement is common, it increases the risk of root contact, which is the major cause of screw failure and consequent treatment interruption.12 Furthermore, with posterior positioning of buccal interradicular miniscrews, the line of force often passes below the center of resistance of the upper arch, resulting in clockwise rotation of the occlusal plane and hence extrusion of the anterior teeth and exacerbation of a gummy smile (Fig. 7A). Anterior interferences between the upper and lower incisors may also induce downward rotation of the mandible, worsening a retrusive chin. While the force system can be modified with additional anchorage in the incisor region, the resultant force can be unpredictable due to the differential forces and moments exerted by the anterior and posterior miniscrews (Fig. 7B). By contrast, the single screw used in the HPPG technique delivers a force closer to the center of resistance of the anterior segment, with more predictable results (Fig. 7C).
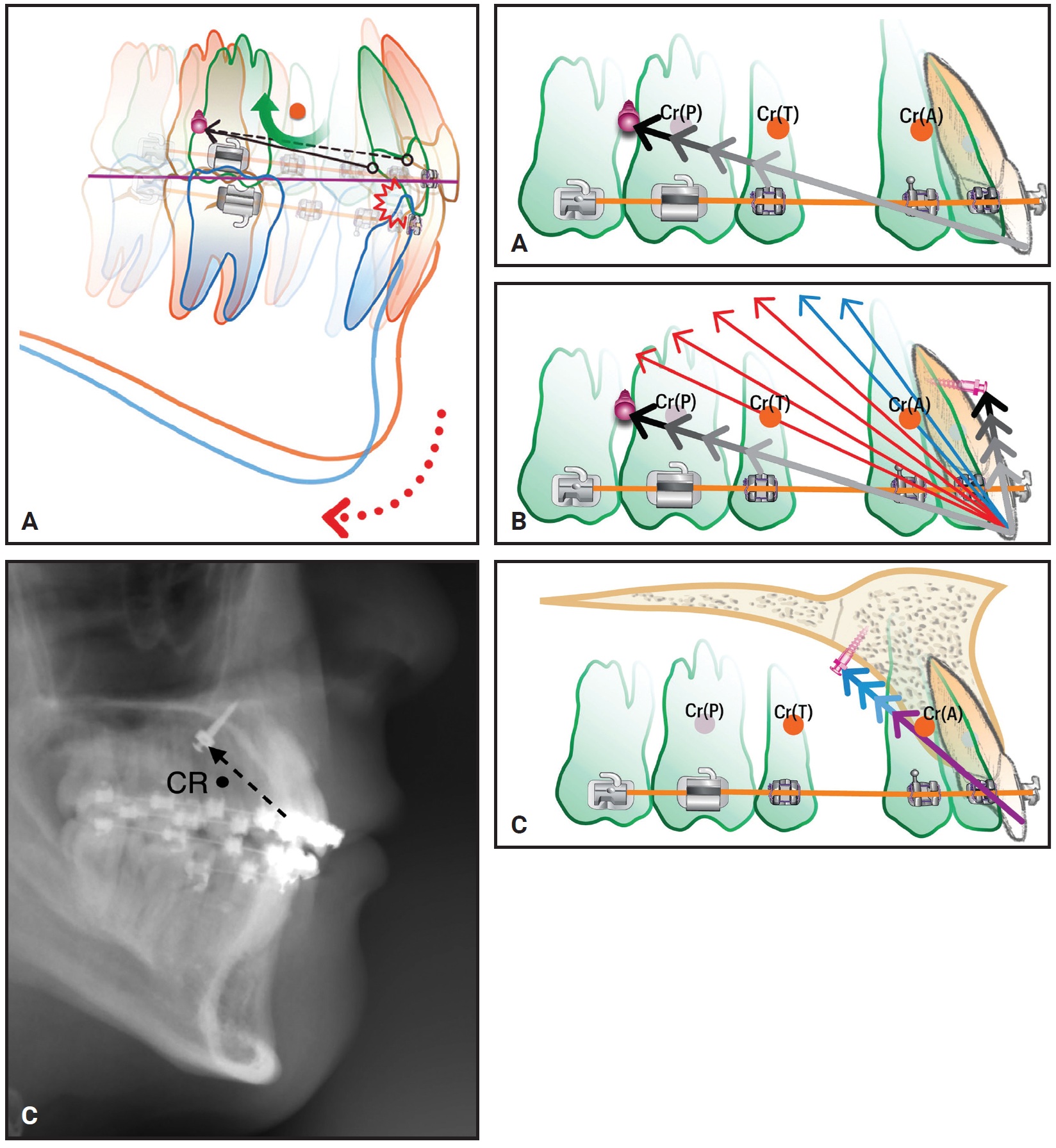
Fig. 7 Force systems created by different miniscrew positions (Cr(A) = center of resistance of anterior segment, Cr(P) = center of resistance of posterior segment, Cr(T) = center of resistance of total arch). A. Posterior buccal interradicular miniscrews can induce clockwise rotation of upper dentition and downward rotation of mandible due to occlusal interferences. B. Differential forces exerted by anterior and posterior miniscrews create unpredictable resultant force, which can be exerted in front of (blue arrows) or behind (red arrows) anterior segment’s center of resistance. C. HPPG technique exerts force closer to center of resistance of anterior segment, in front of center of resistance of entire maxillary dentition.
The center of resistance is not a fixed point; it moves during space closure. In a finite-element study by Song and colleagues, the upper incisors tended to extrude below the original occlusal plane during the initial closure of premolar-extraction spaces, promoting clockwise rotation of the upper occlusal plane regardless of screw position.13 Once the extraction spaces were nearly closed, however, a higher miniscrew position—as used in the HPPG technique—delivered the more vertically directed force needed for counterclockwise rotation of the upper occlusal plane. The entire maxillary arch can thus be intruded above the original occlusal plane, with more intrusion at the incisors and less in the molar regions.
By enabling careful control of sagittal and vertical movements, a combination of the HPPG technique and mandibular miniscrews can correct the pitch of the occlusal plane,14 producing a pleasant profile and improved smile esthetics in a hyperdivergent Class II patient.
FOOTNOTES
- *Clippy, Tomy, Inc., Tokyo, Japan; www.tomyinc.co.jp.
- **A1-P, Bioray Biotech Corporation, Taipei, Taiwan; www.dental-bio-ray.com.
- ***AbsoAnchor, Dentos Co., Daegu, Korea; www.dentos.co.kr.
REFERENCES
- 1. Paik, C.H.; Park, H.S.; and Ahn, H.W.: Treatment of vertical maxillary excess without open bite in a skeletal Class II hyperdivergent patient, Angle Orthod. 87:625-633, 2017.
- 2. Kwon, S.Y.; Ahn, H.W.; Kim, S.H.; Park, Y.G.; Chung, K.R.; Paik, C.H.; and Nelson, G.: Antero-posterior lingual sliding retraction system for orthodontic correction of hyperdivergent Class II protrusion, Head Face Med. 10:22, 2014.
- 3. Li, M.; Su, X.; Li, Y.; Li, X.; and Si, X.: Cone-beam computed tomography-guided three-dimensional evaluation of treatment effectiveness of the Frog appliance, Kor. J. Orthod. 49:161-169, 2019.
- 4. Heo, S.; Park, J.H.; Lee, M.Y.; Kim, J.S.; Jung, S.P.; and Chae, J.M.: Maxillary incisor position-based orthodontic treatment with miniscrews, Semin. Orthod. 28:123-135, 2022.
- 5. Wilmes, B.; Ludwig, B.; Vasudavan, S.; Nienkemper, M.; and Drescher, D.: The T-Zone: Median vs. paramedian insertion of palatal mini-implants, J. Clin. Orthod. 50:543-551, 2016.
- 6. Johnson, E.: Selecting custom torque prescriptions for the straight-wire appliance, Am. J. Orthod. 143:S161-S167, 2013.
- 7. Chew, M.T.: Spectrum and management of dentofacial deformities in a multiethnic Asian population, Angle Orthod. 76:806-809, 2006.
- 8. Noh, H.K. and Park, H.S.: Considerations for vertical control with microimplants in an idiopathic condylar resorption patient: A case report, J. Orthod. 48:172-182, 2021.
- 9. Park, J.H.; Kook, Y.A.; Kim, Y.; Ham, L.K.; and Lee, N.K.: Improved facial profile with non-extraction treatment of severe protrusion using TSADs, Semin. Orthod. 28:157- 163, 2022.
- 10. Liaw, J.J.L.; Wang, S.H.; and Tsai, B.M.Y.: An unusual extraction pattern for retreatment in a patient with dental protrusion and a deficient soft-tissue chin, Am. J. Orthod. 162:554-567, 2022.
- 11. Kim, S.J.; Kim, J.W.; Choi, T.H.; and Lee, K.J.: Combined use of miniscrews and continuous arch for intrusive root movement of incisors in Class II division 2 with gummy smile, Angle Orthod. 84:910-918, 2014.
- 12. Kuroda, S.; Yamada, K.; Deguchi, T.; Hashimoto, T.; Kyung, H.M.; and Takano-Yamamoto, T.: Root proximity is a major factor for screw failure in orthodontic anchorage, Am. J. Orthod. 131:S68-S73, 2007.
- 13. Song, J.W.; Lim, J.K.; Lee, K.J.; Sung, S.J.; Chun, Y.S.; and Mo, S.S.: Finite element analysis of maxillary incisor displacement during en-masse retraction according to orthodontic mini-implant position, Kor. J. Orthod. 46:242-252, 2016.
- 14. Ackerman, J.L.; Proffit, W.R.; Sarver, D.M.; Ackerman, M.B.; and Kean, M.R.: Pitch, roll, and yaw: Describing the spatial orientation of dentofacial traits, Am. J. Orthod. 131:305-310, 2007.
-
 DR. LIN
DR. LIN -
 DR. THAVARUNGKUL
DR. THAVARUNGKUL -
 DR. CHEN
DR. CHEN -
 DR. WANG
DR. WANG
Dr. Lin is a visiting staff member, Chinmei Dental Clinic, Zhubei, Taiwan. Dr. Thavarungkul is a visiting staff member, WeCare Dental Clinic, Bangkok, Thailand. Dr. Chen is the Director, Icon Dental Specialty Clinic, Taichung, Taiwan. Dr. Wang is a visiting staff member, Beauty Forever Orthodontic Clinic, 10F, No. 20, Changchun Road, Taipei 10450, Taiwan; e-mail: thinfe@hotmail.com.
