Effects of the Ricketts Z Sectional Arch in Producing En-Masse Maxillary Distalization in Adult Class II Patients
Compensatory treatment of Class II malocclusion by distalization of the maxillary posterior teeth is indicated for patients with no further growth potential.1 Although a variety of intraoral distalizers have been used in orthodontic therapy,2-4 all mechanical systems except headgear traction have been shown to produce reciprocal mesialization of the anchor teeth, resulting in undesirable side effects and longer treatment.2,5 This approach therefore requires molar overcorrection into a Class III relationship.1 En-masse distalization can be performed with skeletal anchorage from miniplates or miniscrews,1,6 but that comes with the risks of surgical complications and patient discomfort.7
Intermaxillary elastics are commonly combined with continuous archwires for distalization of maxillary teeth in Class II cases. To mitigate the usual side effects—clockwise rotation of the facial axis,8 extrusion of the lower molars and upper incisors, and loss of anchorage of the lower molars8,9—the maxillary archwire can be segmented with Z-shaped sections between the molars and the canines, as proposed by Ricketts (Fig. 1).8 Six activations are incorporated into this modified wire, enabling en-masse distalization of the maxillary posterior teeth in a single operational step, without the side effects of other distalization devices.8 Despite the advantages of the Z sectional arch, it has been described only in case reports8 and therefore lacks a retrospective assessment of treatment outcomes.
Our study hypothesis was that the Ricketts Z sectional arch, combined with Class II elastics, would be effective in achieving en-masse distalization of the maxillary posterior teeth (canine, first and second premolars, and first and second molars) without producing significant changes in the clockwise rotation of the mandible or losing lower-molar anchorage. Hence, this study aimed to determine the cephalometric and dimensional effects of the Ricketts Z sectional arch on dental Class II malocclusions in adult patients.
Materials and Methods
Our retrospective study involved nongrowing patients treated with the Ricketts Z sectional arch and Class II elastics. The minimum sample size (N = 30) was calculated from a pilot study (N = 8), based on a 5% significance level and 80% test power to detect the average effect between baseline and post-treatment outcomes.10,11 The university ethics committee approved this study (No. 94422218.7.0000.5385).
Similar articles from the archive:
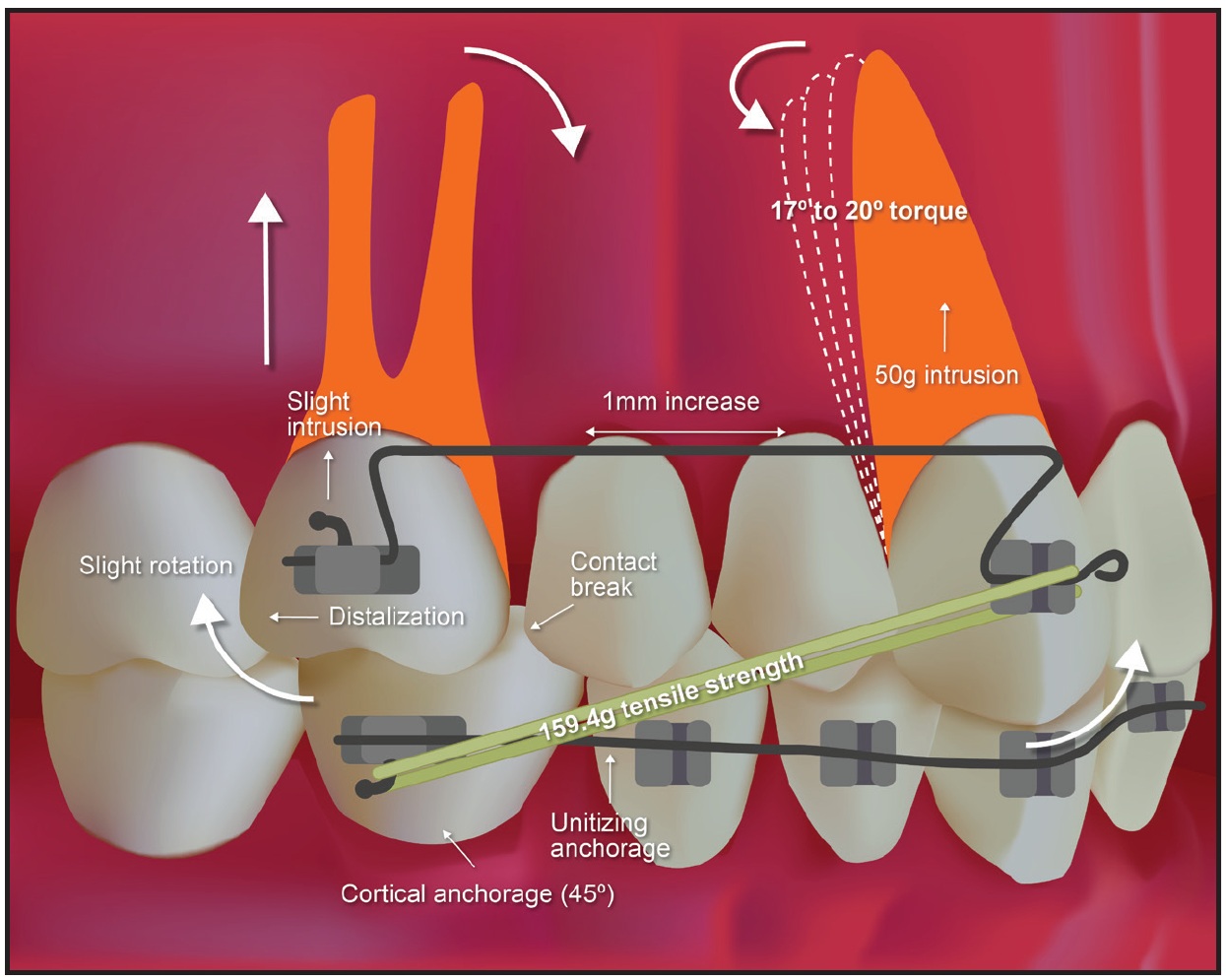
Fig. 1 Biomechanics of Ricketts Z sectional arch.
Eligibility criteria included a dental Class II malocclusion, either complete (N = 17) or three-quarter (N = 13); a skeletal Class I relationship (ANB = 0-4º) or mild skeletal Class II relationship (ANB > 5º); the presence of all permanent teeth in occlusion, except for third molars; completion of pubertal growth; and an SN-GoGn angle greater than 37º. The 30 patients were between the ages of 18 and 42 at the initiation of treatment, with a mean age of 27.4. Baseline and post-treatment lateral cephalograms and study casts were obtained and scanned for subsequent analysis.
The treatment protocol, as described by Ricketts,8 involved maxillary Z-shaped utility segments of .016" × .016" blue Elgiloy thread between the molars and canines (Fig. 2). Brackets with .018" × .030" slots were used. Each Z sectional arch supported six activations (Fig. 3) and was worn with a latex intermaxillary elastic*** exerting an average 159.4g of force, as measured by a dynamometer.† Lower cortical anchorage was obtained initially from a utility arch12 and later from an ideal arch, promoting unified anchorage.13 Distalization was performed on one side at a time; after a Class I molar relationship was obtained on the right side, the contralateral distalization was begun. The patient was instructed to remove the elastic only during meals and to replace it with a new one every 24 hours.
Baseline and post-treatment lateral cephalograms were scanned on a Microtek ScanMaker i800 Plus‡ with a minimum resolution of 300dpi and transferred to the Dolphin Imaging Premium†† 11.95 program. The same operator traced all the cephalometric points.
Both angular and linear measurements were used to evaluate skeletal and soft-tissue changes (Fig. 4A).3 The centroids of the posterior teeth and the incisal borders of the upper and lower central incisors were used as dental reference points.3 Horizontal measurements were made perpendicular to the pterygoid vertical plane; vertical measurements were made perpendicular to the palatal plane (Fig. 4B).3 Angular changes were determined by the inclination of the long axes of the teeth to the SN plane. The long axis of a molar or premolar was based on the centroid perpendicular to the line connecting the greatest mesial and distal convexity of the crown. The long axis of a central incisor was the line between the incisal edge and the root apex (Fig. 4C).
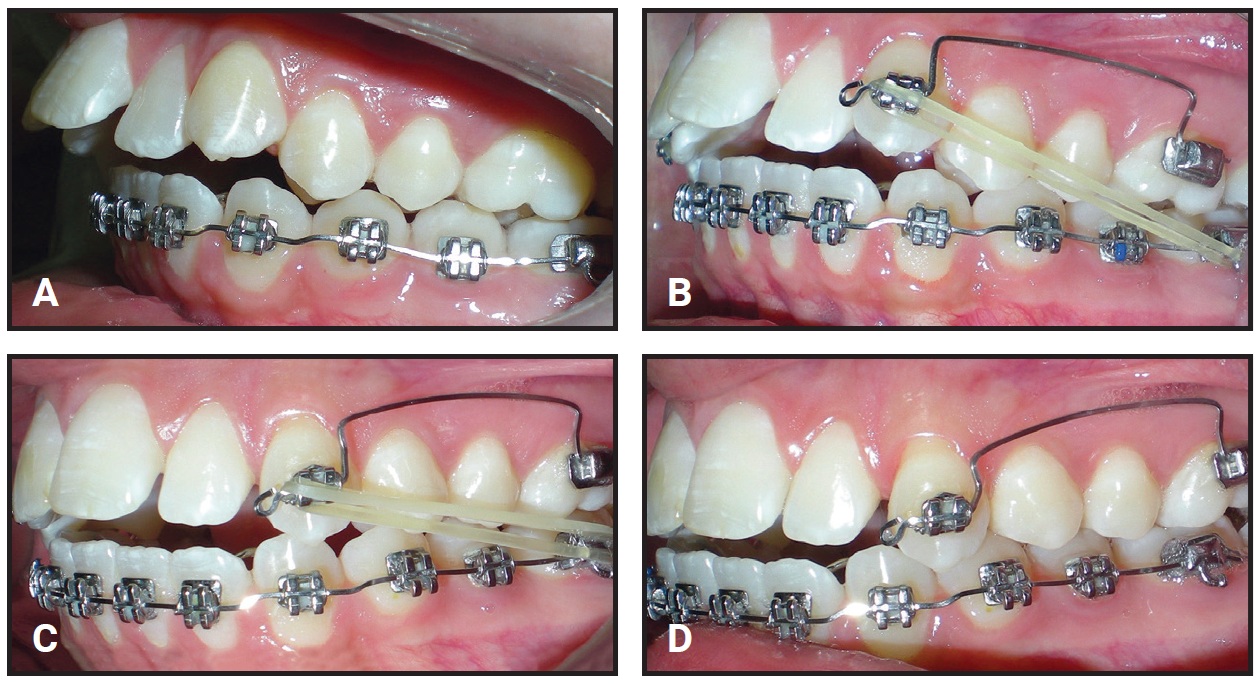
Fig. 2 Clinical sequence of Ricketts Z sectional arch. A. Anchorage. B. Class II elastics exerting 150g of force. C. Intermediate phase. D. Conclusion of treatment.
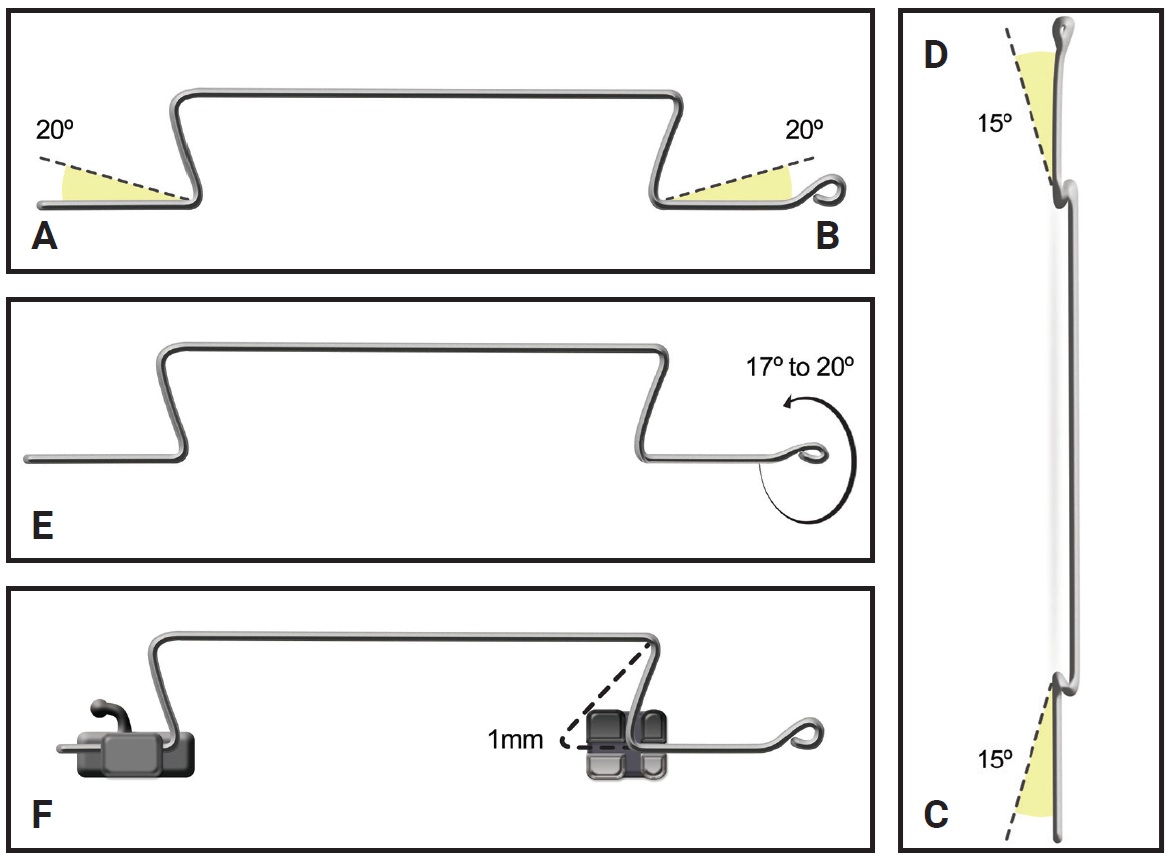
Fig. 3 Six activations of Ricketts Z sectional arch. A. Caudal angulation of 20° in molar region. B. Caudal angulation of 20° in canine region. C. Caudal deviation of 15° in molar region. D. Caudal deviation of 15° in canine region. E. Twist in wire of 17-20° in canine region. F. 1mm increase in sectional arch length.
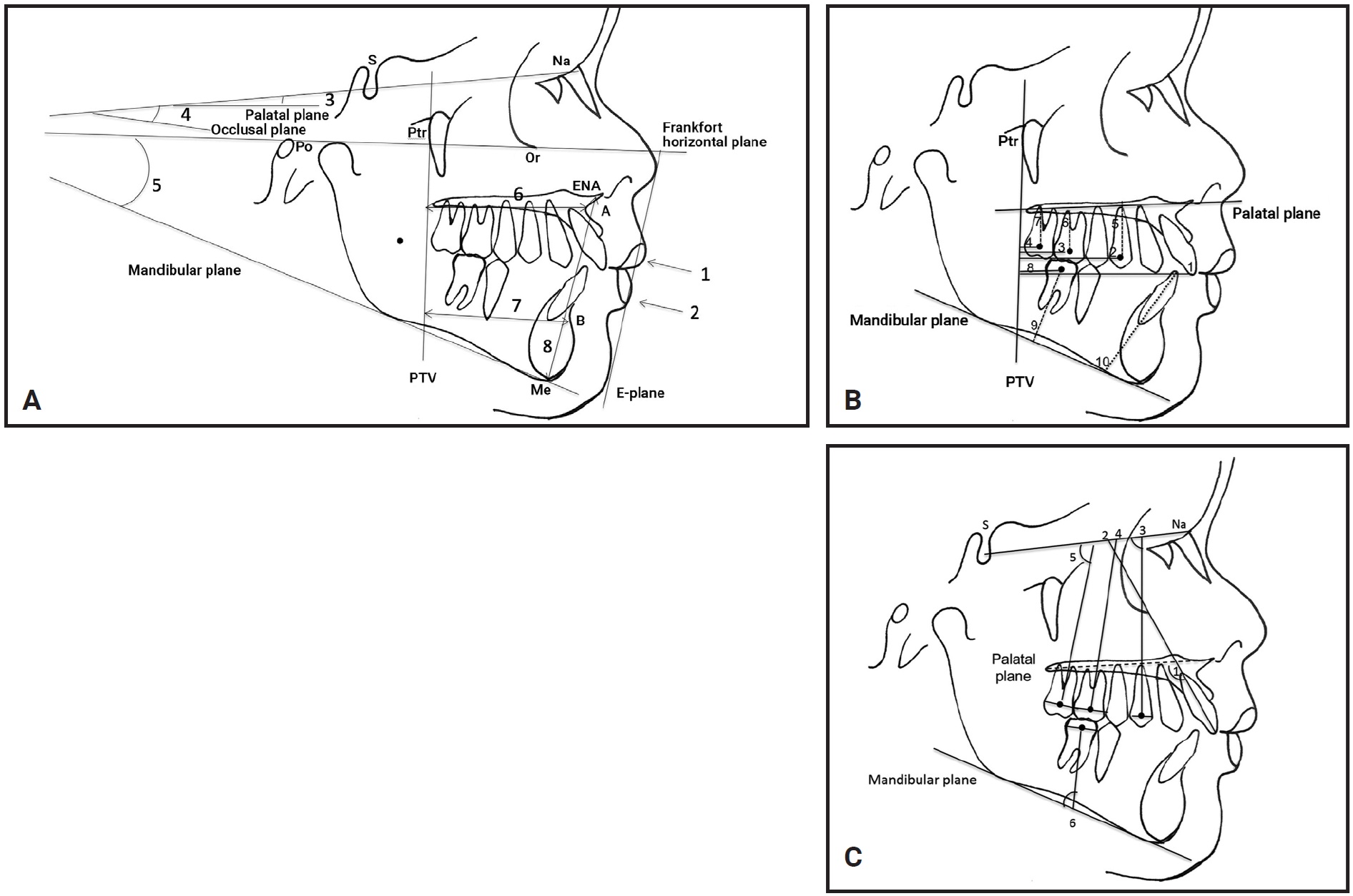
Fig. 4 A. Skeletal cephalometric measurements. 1. Upper lip to E-plane; 2. Lower lip to E-plane; 3. Angle between SN plane and palatal plane; 4. Angle between SN plane and occlusal plane; 5. Angle between mandibular plane and Frankfort plane; 6. Point A to PTV; 7. Point B to PTV; 8. ENA to Me. B. Linear dental measurements. Maxillary anteroposterior: 1. PTV to incisor tip; 2. PTV to centroid of first premolar; 3. PTV to centroid of first molar; 4. PTV to centroid of second molar. Maxillary vertical: 5. PP to centroid of first premolar; 6. PP to centroid of first molar; 7. PP to centroid of second molar. Mandibular anteroposterior: 8. PTV to centroid of first molar. Mandibular vertical: 9. MP to centroid of first molar; 10. MP to incisor and IMPA. C. Angular dental measurements. Maxillary: 1. PP to incisor; 2. SNA to incisor; 3. SNA to first premolar; 4. SNA to first molar; 5. SNA to second molar. Mandibular: 6. MP to first molar.
Points and lines were marked directly on the baseline and post-treatment study casts3 using a .5mm graphite pencil. The most prominent rugae near the midline and the tips of the incisors, premolars, and molar cusps were also marked. The rugae plane (RP) and medial palatine suture (MPS) plane were drawn as references to evaluate molar, premolar, and incisor changes in the sagittal dimension, molar movement in the transverse dimension, and molar rotation (Fig. 5). The Microtek ScanMaker i800 Plus was used to scan the marked casts. Measurements were made separately for the maxillary left and right teeth, using Dolphin Imaging Premium, and were then averaged for statistical analysis.
The same examiner repeated all measurements in the entire sample within 30 days. The Dahlberg formula was used to calculate the casual error; the results, ≥ 1mm for linear measurements and ≥ 1.5º for angular measurements, are considered acceptable. The Bland-Altman analysis was used to calculate systematic errors, with 95% confidence limits, and indicated excellent reproducibility. Because the data had a parametric distribution, the baseline and post-treatment measurements were compared using paired t-tests. The statistical analysis was performed with the R program,‡‡ based on a 5% significance level.
Results
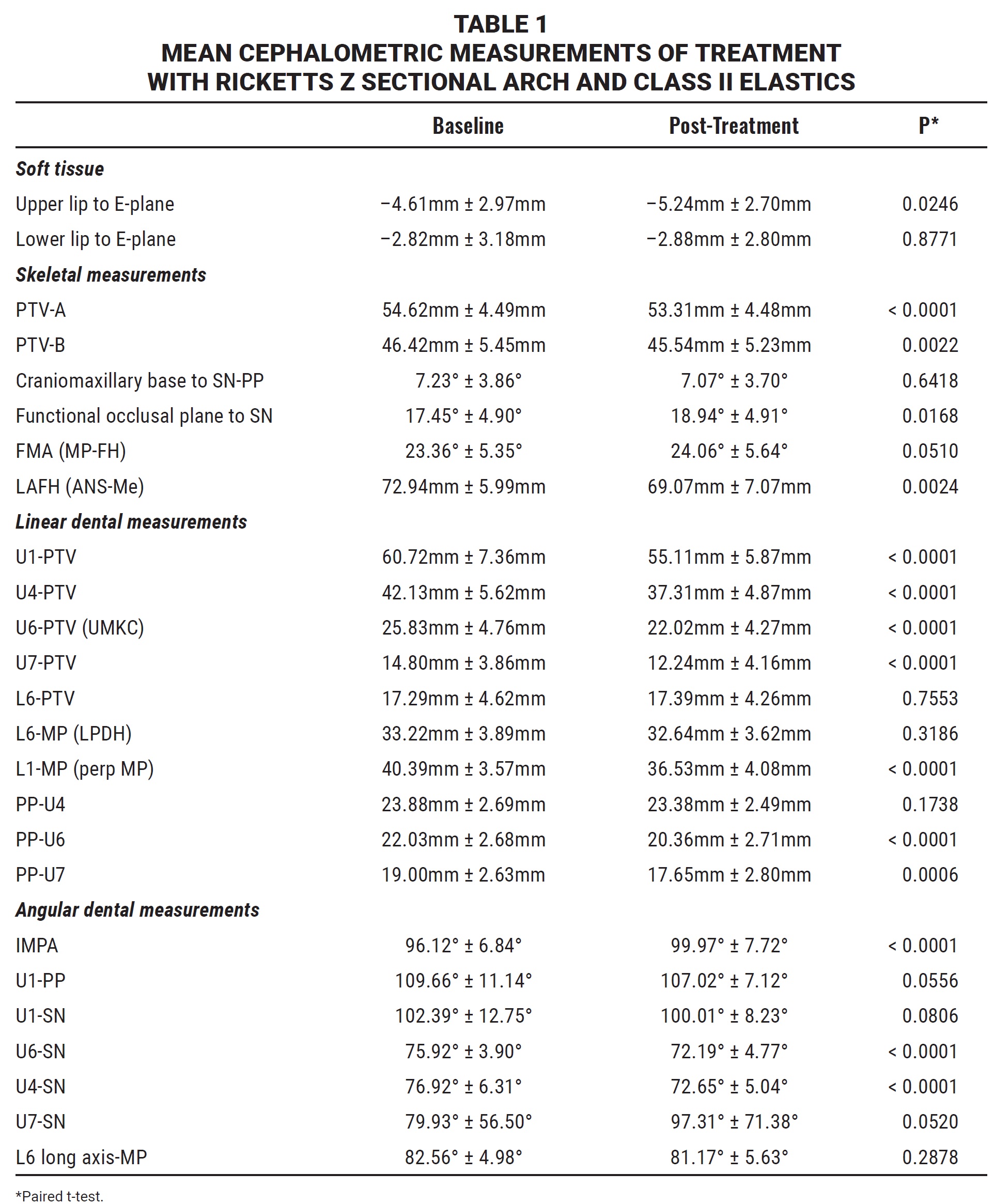
The corrective orthodontic treatment produced Class I molar relationships through en-masse distalization of the maxillary teeth in an average 6.2 months (Table 1). Skeletally, there was a significant reduction in PTV-A and functional occlusal plane to SN (p = .0168). Among the linear dental variables, there were highly significant decreases in U1-PTV, U6-PTV, U7-PTV, L1-MP, and PP-U6 (p < .0001). The overall en-masse distalization was 4.82mm (p < .0001), according to the U4-PTV measurement. The angular dental measurements IMPA, U6-SN, and U4-SN showed highly significant changes (p < .0001), but no significant effects were seen in the soft-tissue variables.
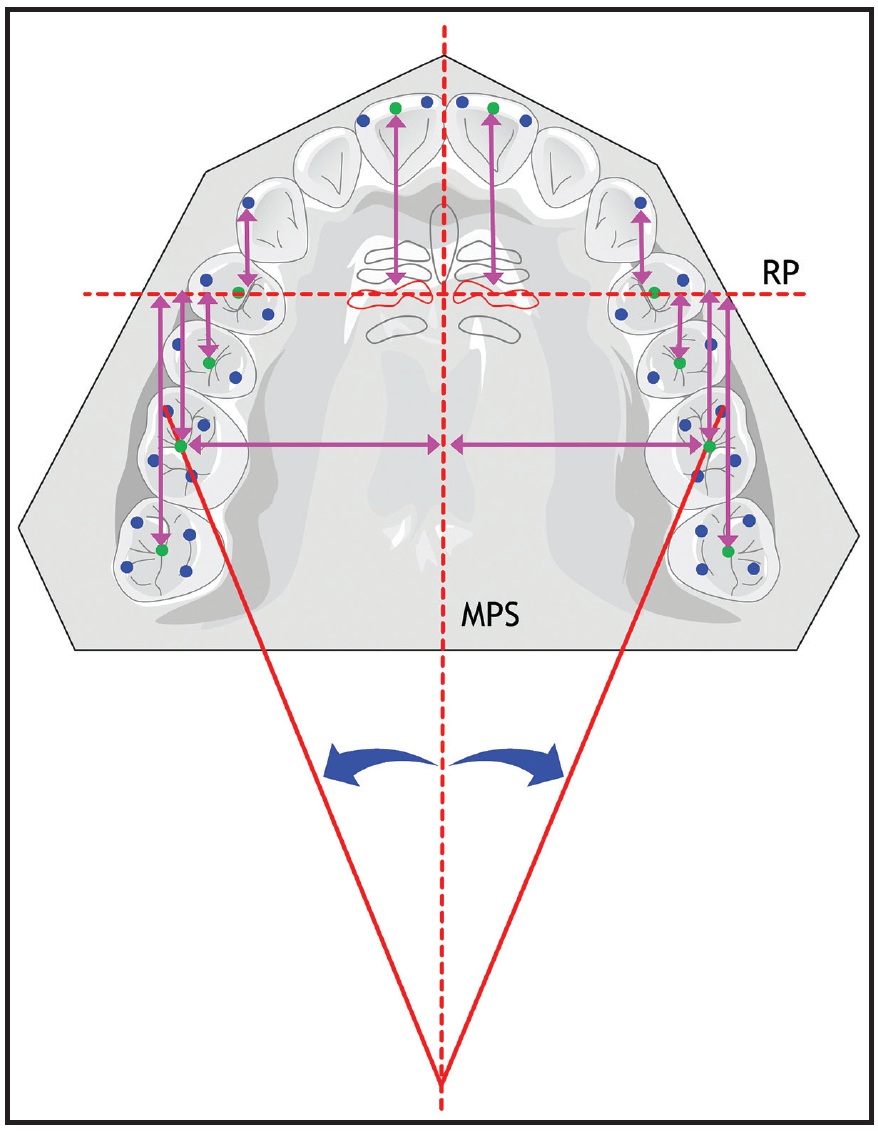
Fig. 5 Study cast measurements. Sagittal: distalization of molars, premolars, and canines and retrusion of upper incisors measured from rugae plane (RP), perpendicular to medial palatine suture (MPS) plane (1-RP, 3-RP, 4-RP, 5-RP, 6-RP, 7-RP). Transverse: 6-MPS. Molar rotation: angulation between line passing through mesiobuccal and distopalatal cusps and MPS.
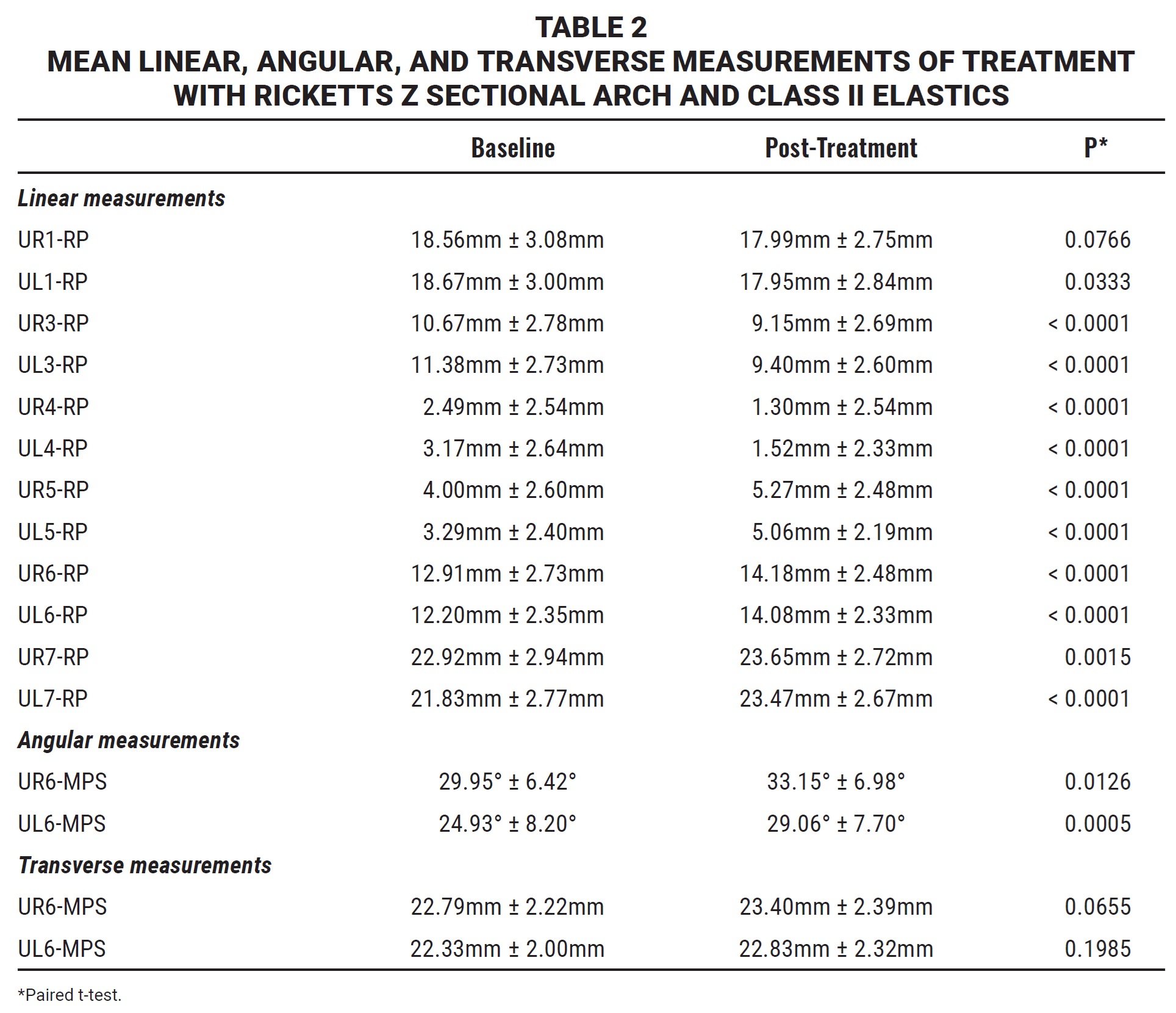
Use of the Ricketts Z sectional arch significantly reduced the linear distances of the upper left central incisor, upper right canine, upper left canine, upper right first premolar, and upper left first premolar to RP (p < .05). On the other hand, the linear and angular measurements of the second premolars and the first and second molars all increased (Table 2). The first molars exhibited an average distalization of 1.27mm (p < .0001) on the right side, compared to 1.87mm on the left (p < .0001); the second molars showed an average distalization of .73mm (p = .0015) on the right and 1.64mm (p < .0001) on the left.
Discussion
Our hypothesis was that the Z sectional arch, combined with Class II elastics, can achieve en-masse distalization of the maxillary posterior teeth without significant sagittal changes or loss of anchorage of the lower molars. Based on our results, this hypothesis was accepted.
Our findings showed that the caudal angulation of the Z sectional arch in the molar region produced an intrusive force of about 50g on the canine, neutralizing the vertical vector of the elastic traction (159.4g). The resulting intermaxillary traction force was 109.4g toward the distal—sufficient for en-masse movement of the posterior teeth.8,14 The molars received forces from four directions: backward tilt, distalization, rotation, and slight intrusion. The torque in the canine region, added to the caudal deviation at the molar, positioned the canine within the cancellous bone, thus facilitating orthodontic movement. The premolars were spontaneously distalized by the molars’ intraseptal fibers15 and by contact with the distal surfaces of the canines.8
The average en-masse distalization in our study was 4.82mm, or .77mm per month. A similar study measuring en-masse distalization with zygomatic-crest anchorage and nickel titanium springs reported monthly distalization rates of .44mm and .47mm from forces of 120g and 180g, respectively.14 Another study reported an average 1.64mm distalization in 12.3 ± 5.7 months from nickel titanium springs (200g) with miniscrew anchorage.5 In our study, the Z sectional arch provided more en-masse distalization with less force, despite its reliance on patient cooperation with elastic wear.
An important detail to consider is that the distalization in our protocol was performed on one side at a time. While light Class II elastics were being worn to one side of the lower arch to control anchorage, the other side was stabilized by cortical anchorage, with no intermaxillary traction force in the mesial direction.12 The Z sectional arch produced a bilateral Class I molar relationship in an average 6.2 months—similar to other studies in which all posterior teeth were distalized simultaneously.3,13,14 The sectional mechanics allowed the upper incisors to be retracted by the labial musculature while promoting distalization in each posterior segment,8 thus reducing the overall treatment time. The Z sectional arch also has the advantage of eliminating friction between the brackets and archwire.16 The average treatment time in our study was one-third less than that associated with the modified C-palatal plate17 and about half that for zygomatic-bone anchorage.18,19 The magnitude of the distalization forces employed in these methods were twice as high with the C-palatal plate20 and three times as high with the zygomatic anchorage.19 The second molars in our study did show a greater distal inclination after treatment, probably because they were not connected to the Z sectional arches, which could have controlled their inclination during distalization.
In the present study, the first premolars were distalized by 4.82mm and intruded by .5mm—similar to the results reported for zygomatic-bone anchorage,19 but greater than the amounts found with miniscrew anchorage.5 Our data thus demonstrated a spontaneous distalization of the premolars.15 In addition, the stability of our L6-PTV and lower-lip to E-plane measurements confirmed the effectiveness of the lower anchorage for the light unilateral elastic traction. The reduction in L6-MP, indicating molar intrusion and uprighting, and the increase in IMPA, indicating lower-incisor intrusion, were attributable to the mechanics (Fig. 6).
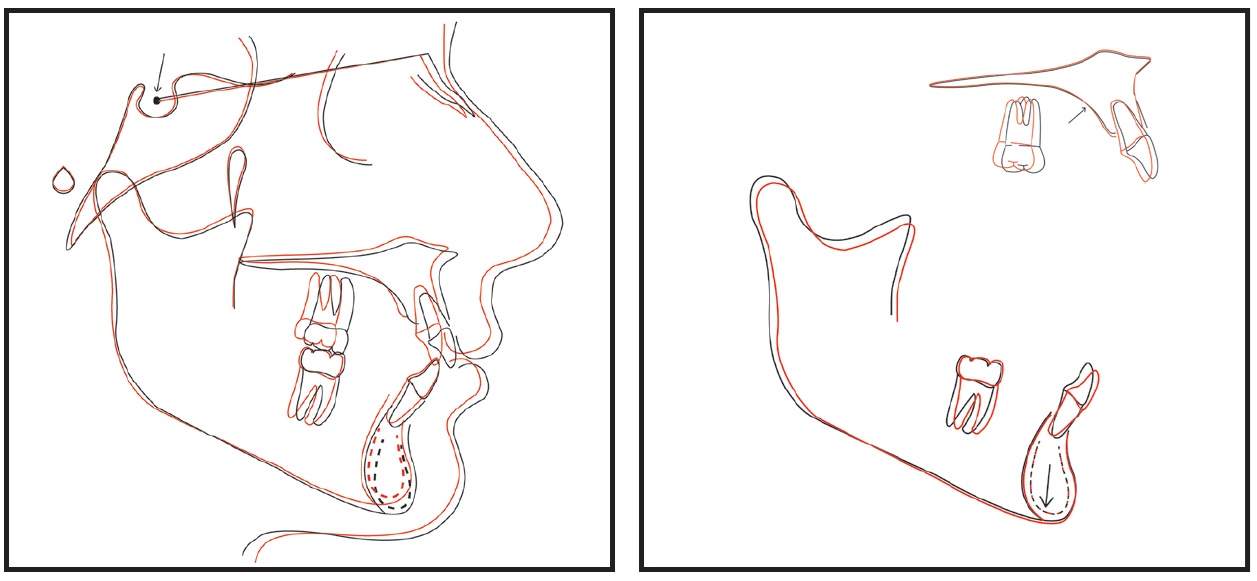
Fig. 6 Superimposition of means (N = 30) of pre- and post-treatment cephalometric tracings.
During distalization, the first premolars, first molars, and second molars were intruded by .5mm, 1.67mm, and 1.35mm, respectively, as confirmed by significant changes in FMA and LAFH (ANS-Me). The uprighting and intrusion of the lower molars could have affected the stability of the FMA angle, or the patients’ growth patterns (meso- or brachyfacial) could have contributed to these vertical effects. It should be noted that only the upper molars and canines were subject to the extrusive forces of intermaxillary traction applied to the entire lower arch. Our results also showed significant reductions in the measurements of the upper lip (upper lip to E-plane = –.63mm) and point A (PTV-A = –1.31mm), corroborating a previous study.19 The differences between these findings and those of other studies5,21 can be attributed to our sample criteria of complete or three-quarter Class II malocclusions, allowing a more significant retraction of anterior teeth.
In our study, the Ricketts Z sectional arch and Class II elastics significantly increased the clockwise rotation of the occlusal plane (functional occlusal plane to SN)—probably not because of a clockwise rotation of the mandible itself, but because of the intrusion of the lower incisors to correct the curve of Spee.22 This interpretation is consistent with our vertical measurements, which did not show any significant alterations.
The limitations of this study included the absence of a nontreated sample for comparison, a lack of quantitative evaluation immediately after distalization, and the dependence on patient collaboration for the success and duration of treatment. The study would have been strengthened by a longitudinal follow-up to assess the long-term stability of these orthodontic corrections. Nevertheless, the Ricketts Z sectional arch and Class II intermaxillary elastics were found to be effective in the treatment of Class II malocclusion, promoting en-masse distalization of the upper posterior teeth with no loss of lower anchorage. Such an approach avoids the need for extractions and provides beneficial vertical and anteroposterior effects at both the dental and skeletal levels.
FOOTNOTES
- *Registered trademark of Rocky Mountain Orthodontics, Denver, CO; www.rmortho.com.
- **Registered trademark of Henry Schein Orthodontics, Melville, NY; www.henryscheinortho.com.
- ***Morelli, Sorocaba, Brazil; www.morelli.com.br.
- †Haag-Streit Diagnostics, Köniz, Switzerland; www.haag-streit.com.
- ‡Registered trademark of Microtek International, Inc., Hsinchu, Taiwan; microtek.com.
- ††Trademark of Dolphin Imaging & Management Solutions, Chatsworth, CA; www.dolphinimaging.com.
- ‡‡Registered trademark of R Foundation for Statistical Computing, Vienna, Austria; r-project.org.
REFERENCES
- 1. Bechtold, T.E.; Kim, J.W.; Choi, T.H.; Park, Y.C.; and Lee, K.J.: Distalization pattern of the maxillary arch depending on the number of orthodontic miniscrews, Angle Orthod. 83:266-273, 2013.
- 2. Vilanova, L.; Henriques, J.F.C.; Janson, G.; Patel, M.P.; Reis, R.S.; and Aliaga del Castillo, A.: Class II malocclusion treatment effects with Jones Jig and Distal Jet followed by fixed appliances, Angle Orthod. 88:10-19, 2018.
- 3. Papadopoulos, M.A.; Melkos, A.B.; and Athanasiou, A.E.: Noncompliance maxillary molar distalization with the first class appliance: A randomized controlled trial, Am. J. Orthod. 137:586e1-e13, 2010.
- 4. Areepong, D.; Kim, K.B.; Oliver, D.R.; and Ueno, H.: The Class II Carriere Motion appliance, Angle Orthod. 90:491-499, 2020.
- 5. Park, H.S.; Lee, S.K.; and Kwon, O.W.: En-masse distal movement of teeth using microscrew implant anchorage, Angle Orthod. 75:602-609, 2005.
- 6. Chang, C.H.; Lin, J.S.; and Roberts, W.E.: Failure rates for stainless steel versus titanium alloy infrazygomatic crest bone screws: A single-center, randomized double-blind clinical trial, Angle Orthod. 89:40-46, 2019.
- 7. Uesugi, S.; Kokai, S.; Kanno, Z.; and Ono, T.: Prognosis of primary and secondary insertions of orthodontic miniscrews: What we have learned from 500 implants, Am. J. Orthod. 152:224-231, 2017.
-
8.
Ricketts, R.M.:
[in Portuguese], Editora Kelps, Goiânia, Brazil, 1998. - 9. Janson, G.; Sathler, R.; Fernandes, T.M.; Branco, N.C.; and Freitas, M.R.: Correction of Class II malocclusion with Class II elastics: A systematic review, Am. J. Orthod. 143:383-392, 2013.
- 10. Cohen, J.: Statistical Power Analysis for the Behavioral Sciences, 2nd ed., Lawrence Erlbaum Associates Publishers, Hillsdale, NJ, 1988.
- 11. Cohen, J.: A power primer, Psychol. Bull. 112:155-159, 1992.
- 12. Urias, D. and Mustafa, F.: Anchorage control in bioprogressive vs straight-wire treatment, Angle Orthod. 75:987-992, 2005.
- 13. Mavropoulos, A.; Sayinsu, K.; Allaf, F.; Kiliaridis, S.; Papadopoulos, M.A.; and Keles, A.O.: Noncompliance unilateral maxillary molar distalization: A three-dimensional tooth movement analysis, Angle Orthod. 76:382-387, 2006.
- 14. Limsiriwong, S.; Khemaleelakul, W.; Sirabanchongkran, S.; Pothacharoen, P.; Kongtawelert, P.; Ongchai, S.; and Jotikasthira, D.: Biochemical and clinical comparisons of segmental maxillary posterior tooth distal movement between two different force magnitudes, Eur. J. Orthod. 40:496-503, 2018.
- 15. Grec, R.H.; Janson, G.; Branco, N.C.; Moura-Grec, P.G.; Patel, M.P.; and Henriques, J.F.: Intraoral distalizer effects with conventional and skeletal anchorage: A meta-analysis, Am. J. Orthod. 143:602-615, 2013.
- 16. Yanase, Y.; Loi, H.; Nishioka, M.; and Takahashi, I.: Effects of sliding velocity on friction: An in vitro study at extremely low sliding velocity approximating orthodontic tooth movement, Angle Orthod. 84:451-458, 2014.
- 17. Park, C.O.; Sa’aed, N.L.; Bayome, M.; Park, J.H.; Kook, Y.A.; Park, Y.S.; and Han, S.H.: Comparison of treatment effects between the modified C-palatal plate and cervical pull headgear for total arch distalization in adults, Kor. J. Orthod. 47:375-383, 2017.
- 18. Sugawara, J.; Kanzaki, R.; Takahashi, I.; Nagasaka, H.; and Nanda, R.: Distal movement of maxillary molars in non-growing patients with the skeletal anchorage system, Am. J. Orthod. 129:723-733, 2006.
- 19. Kaya, B.; Arman, A.; Uçkan, S.; and Yacizi, A.C.: Comparison of the zygoma anchorage system with cervical headgear in buccal segment distalization, Eur. J. Orthod. 31:417-424, 2009.
- 20. Lee, S.K.; Abbas, N.H.; Bayome, M.; Baik, U.B.; Kook, Y.A.; Hong, M.; and Park, J.H.: A comparison of treatment effects of total arch distalization using modified C-palatal plate vs buccal miniscrews, Angle Orthod. 88:45-51, 2018.
- 21. Kilkis, D.; Celikoglu, M.; Nur, M.; Bayram, M.; and Candirli, C.: Effects of zygoma-gear appliance for unilateral maxillary molar distalization: A prospective clinical study, Am. J. Orthod. 150:989-996, 2016.
- 22. Chhibber, A.; Upadhyay, M.; Uribe, F.; and Nanda, R.: Mechanism of Class II correction in prepubertal and postpubertal patients with Twin Force Bite Corrector, Angle Orthod. 83:718-727, 2013.
-
 DR. VASCONCELOS
DR. VASCONCELOS -
 DR. VEDOVELLO-FILHO
DR. VEDOVELLO-FILHO -
 DR. CARMO DE MENEZES
DR. CARMO DE MENEZES -
 DR. SANTAMARIA-JR
DR. SANTAMARIA-JR -
 DR. VEDOVELLO
DR. VEDOVELLO
Dr. Vasconcelos is a student, and Drs. Vedovello-Filho, Carmo de Menezes, Santamaria-Jr, and Vedovello are Professors, Department of Orthodontics, Araras Dental School, University Center of Hermínio Ometto Foundation, Dr. Maximiliano Baruto Av. 500, Jardim Universitário, Araras, São Paulo 13607-339, Brazil. E-mail Dr. Vedovello at silviavedovello@gmail.com.
