A New Appliance for Efficient Molar Distalization
An estimated 25-30% of all orthodontic patients can benefit from maxillary expansion, and 95% of Class II cases can be improved by molar rotation, distalization, and expansion.1 Therefore, Class II treatment usually involves distal movement of the upper molars to achieve Class I molar and canine relationships.
Headgear requires patient cooperation, and lack of cooperation will compromise results and increase the length of treatment.2-4 These problems inspired many clinicians to develop intraoral devices and techniques for distal molar movement. In 1992, Hilgers introduced the Pendulum* appliance for distalization without the need for patient compliance.5 Since then, other intraoral maxillary first-molar distalizers such as the Distal Jet,**6 Jones Jig,**7 and Frog appliance***8 have been developed.
According to Burstone’s principles, when designing an active orthodontic force system, the magnitude of forces and moments, moment-to-force ratio, constancy of forces and moments, bracket friction, and ease of use should all be considered.9 This article describes the design of a palatally based active force system, the Molar Thruster appliance, for molar distalization as part of a two-phase treatment sequence in Class II patients.
Appliance Design
Similar articles from the archive:
The first premolars and first molars are banded; banding of the second premolars is recommended for better anchorage. Palatal sheaths are welded to the upper first-molar bands (Fig. 1). The first and second premolars are attached with .040" wire to an acrylic covering that is in close contact with the palatal surface. If the overbite permits, this acrylic covering can be converted to an anterior biteplane to disclude the posterior teeth, thus enhancing molar distalization and deep-bite correction. Before polymerization, two .036" Begg buccal tubes are embedded in the acrylic near the distal margin, 5mm from the midline.
Two bayonets are constructed from .028" stainless steel wire. One end of each bayonet is attached to the palatal molar sheath; the other is inserted into the Begg buccal tube along with a nickel titanium open-coil spring. When the bayonet is placed, the spring is compressed to push the molar distally. To keep the spring from slipping over the distal arm of the bayonet, a piece of band material is welded at the junction of the bayonet’s distal and anterior arms.
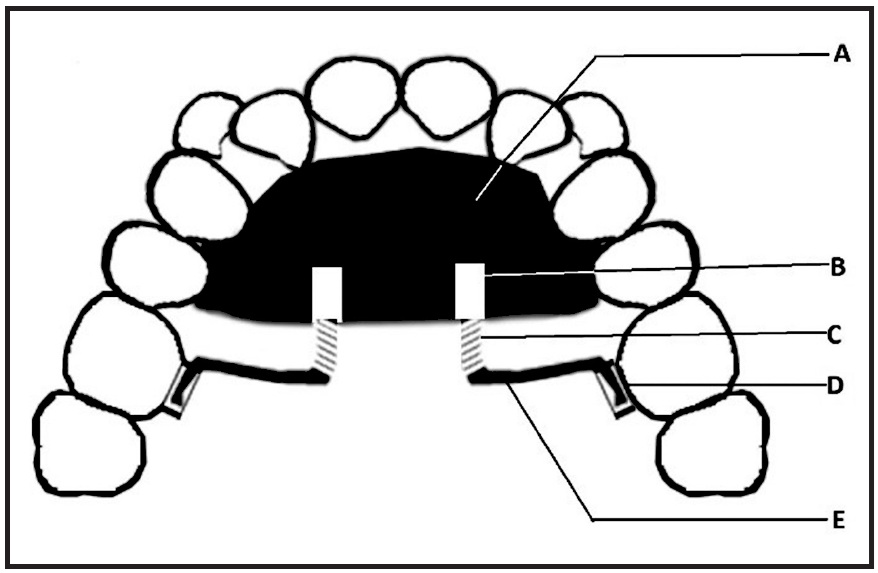
Fig. 1 Appliance design (A = acrylic covering over palatal surface; B = .036" Begg buccal tube embedded in acrylic; C = nickel titanium open-coil spring for force delivery; D = palatal molar sheath for attaching distal end of bayonet; E = bayonet made of .028" stainless steel wire).
The appliance generates 150-200g of force, optimal for distalization of both the first and second molars. Along with the distalization, however, this force system will produce some distal molar tipping. After observing the effects of the appliance, we devised the simple solution of placing a small bend in the bayonet wire near its attachment with the molar sheath. Reactivation can be accomplished by placing a new bayonet wire with a longer anterior arm and a longer nickel titanium spring.
Case 1
A 17-year-old female presented with high, buccally placed upper canines; retained upper deciduous canines and a retained lower left second deciduous molar; a congenitally missing lower left second premolar; a straight soft-tissue profile; and 11mm of crowding in the upper arch and 7mm in the lower (Fig. 2).
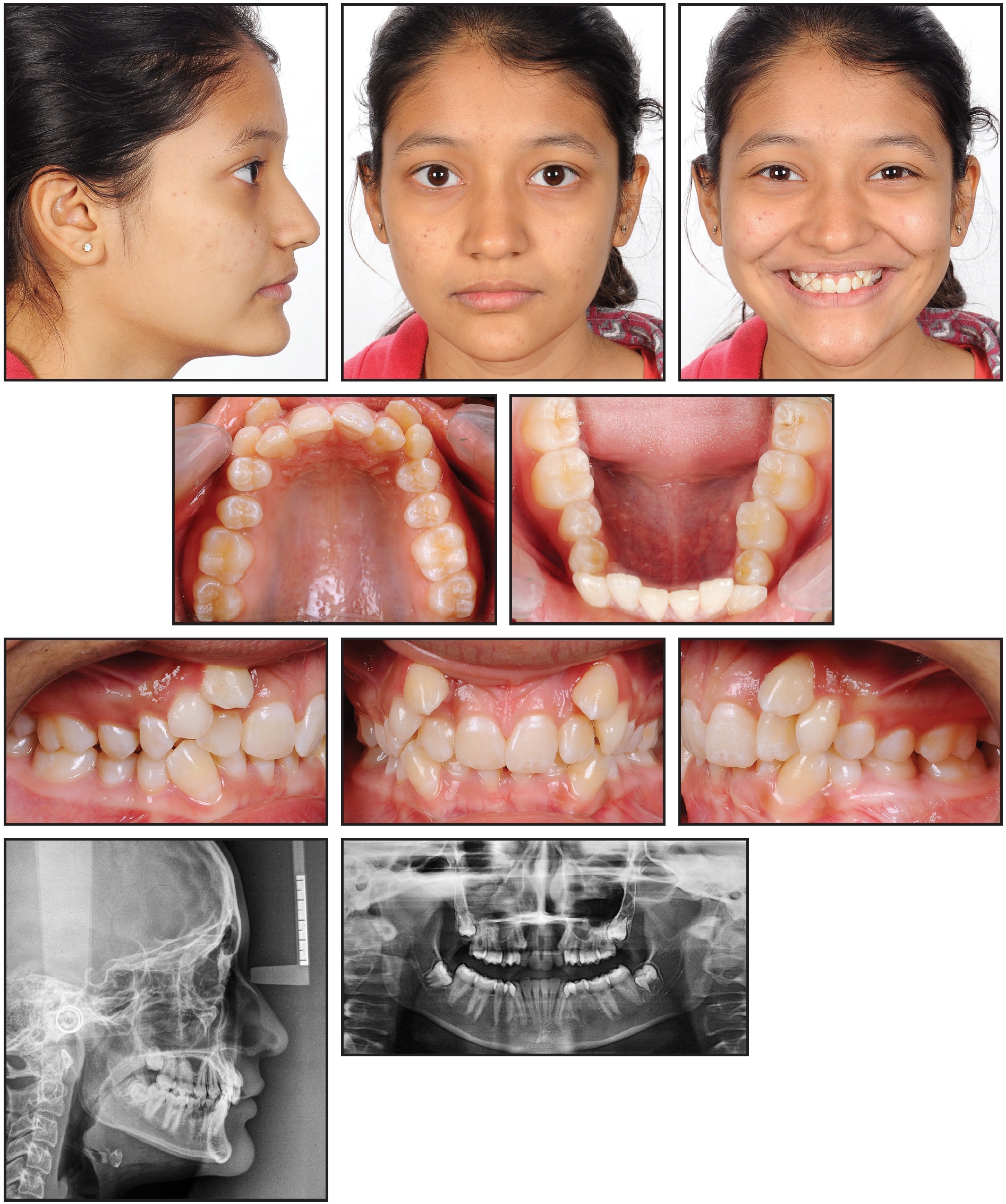
Fig. 2 Case 1. 17-year-old female patient with Class II molar relationship, horizontal growth pattern, retained upper deciduous canines and lower left second deciduous molar, and congenitally missing lower left second premolar before treatment.
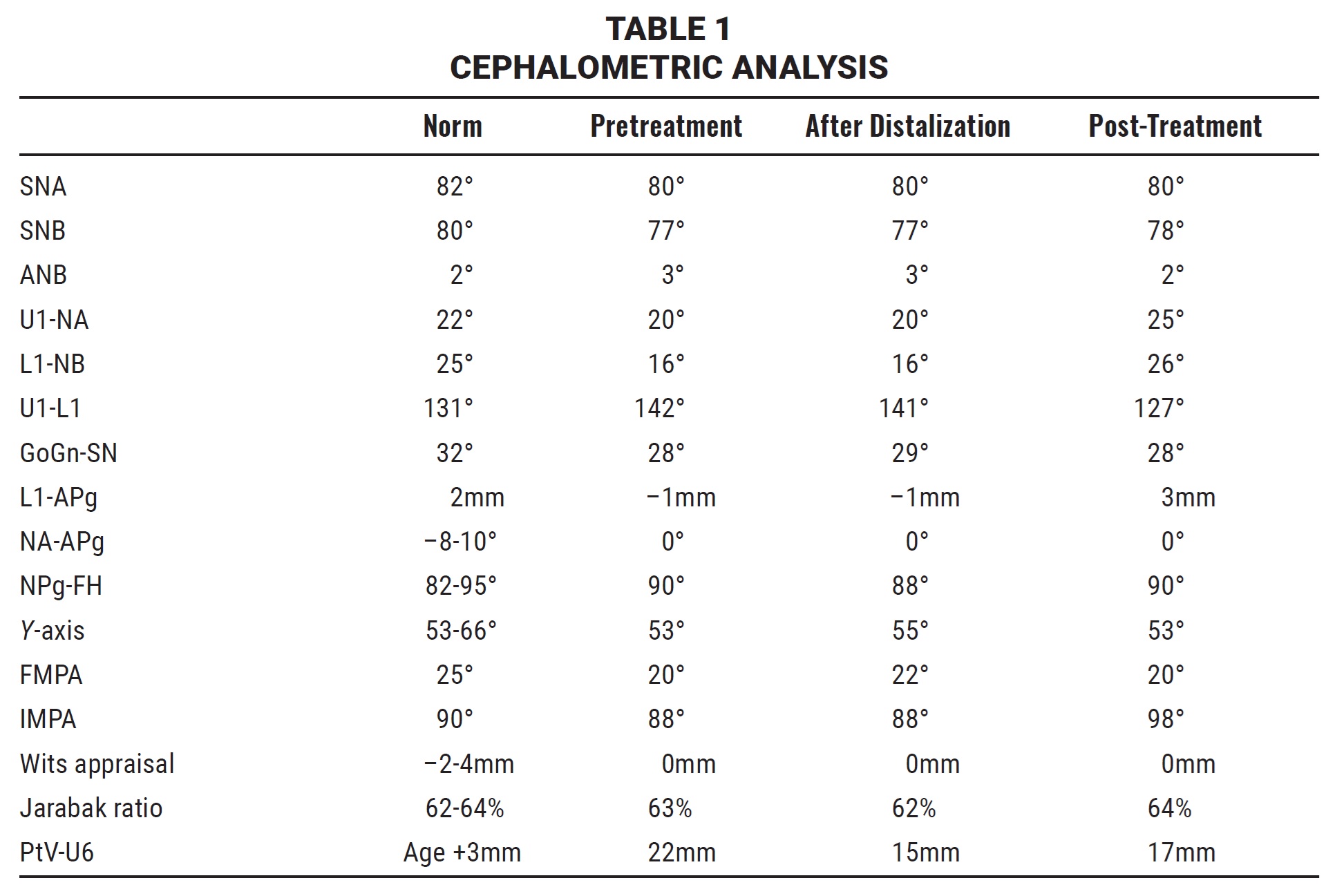
Cephalometric analysis indicated a Class II molar relationship over a skeletal Class I base, created by the combination of an orthognathic maxilla and a horizontal mandibular growth pattern (Table 1).
Before active distalization was started, the upper third molars were removed. To begin the first phase of treatment, the Molar Thruster appliance was placed with an active distalizing force; an anterior biteplane was incorporated to disclude the posterior teeth for faster movement (Fig. 3). The lower arch was bonded simultaneously to save overall treatment time, and an .014" nickel titanium archwire was inserted three months later. The pull of transseptal fibers had already caused some distalization of the upper second premolars. After six months of active upper-molar distalization, a bilateral super-Class I molar relationship had been achieved (Fig. 4).
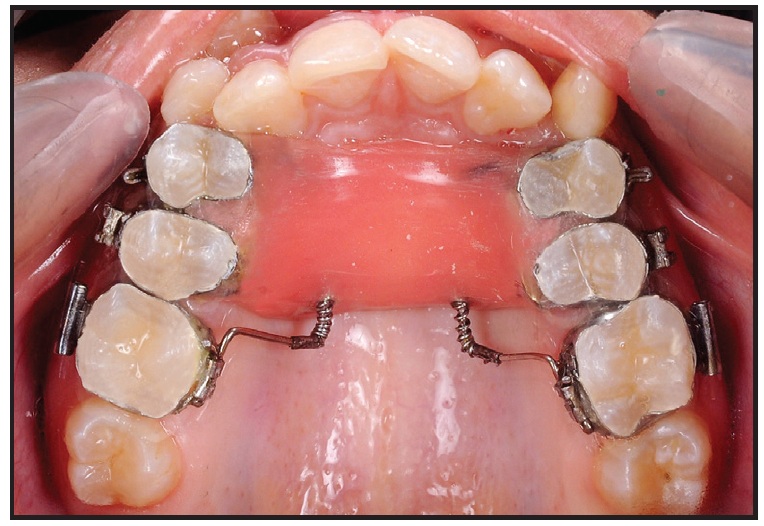
Fig. 3 Case 1. Distalization appliance and anterior biteplane in place.
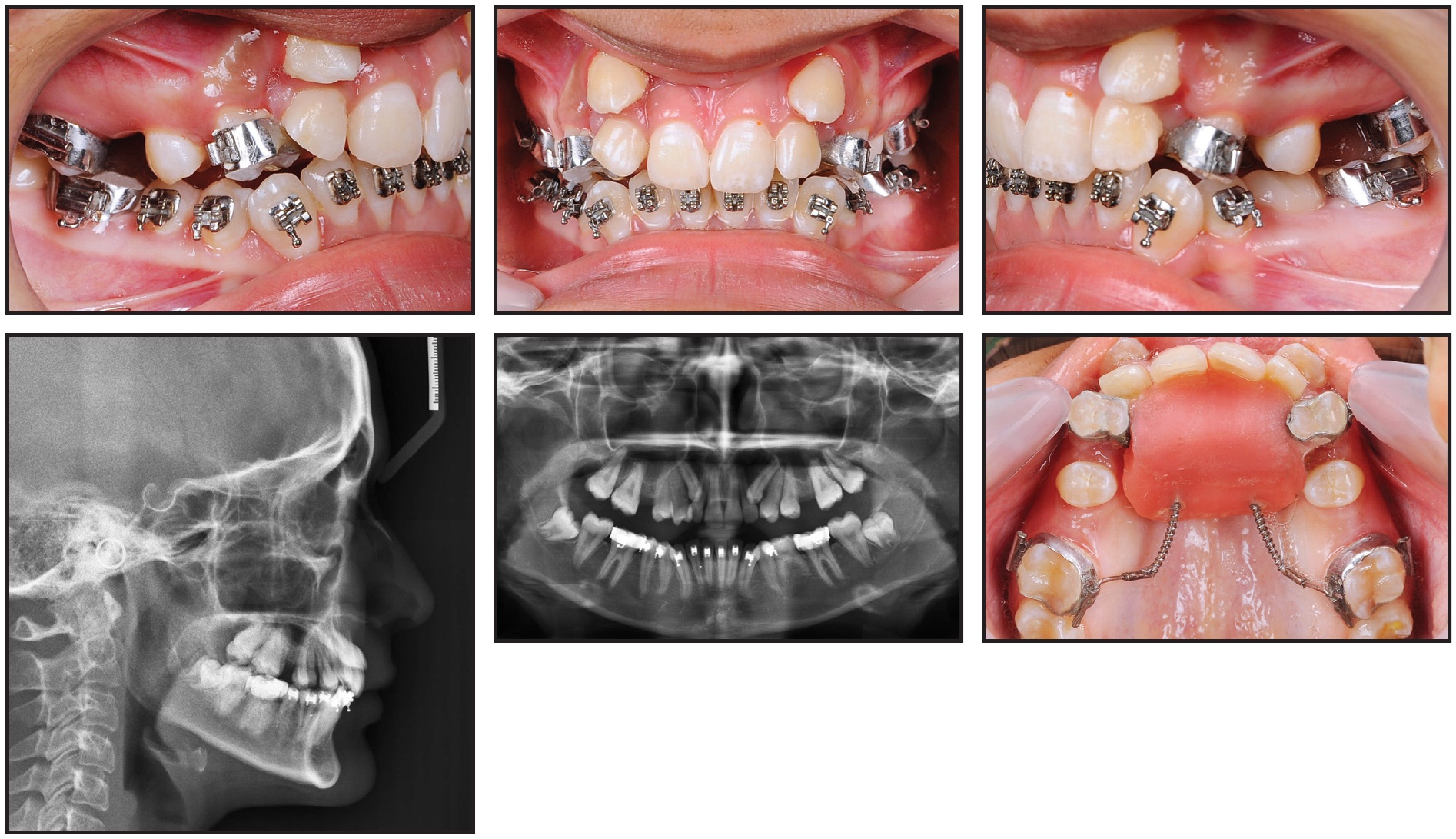
Fig. 4 Case 1. After six months of distalization.
Upon completion of Phase I, a Nance palatal button was placed to maintain the correction. Phase II was then initiated by bonding the upper arch except for the canines and inserting an .014" nickel titanium wire. The second premolars were distalized first, followed by the first premolars to prevent anchorage loss. Once enough space had been gained, the canines were bonded and actively pulled into the arch with a piggyback .014" nickel titanium wire. After archwires had progressed up to .019" × .025" stainless steel, +7° torque brackets were bonded to the upper canines to move their roots into the center of the buccal and palatal cortical plates. Clinical observation of similar cases has shown that buccally placed upper canines require positive torque because of their root positions. The upper arch was leveled and aligned in 13 months of Phase II treatment (Fig. 5, Table 1). After appliance removal, upper and lower 3-3 fixed lingual wires were bonded and upper and lower Hawley retainers were delivered.

Fig. 5 Case 1. Patient after 19 months of treatment.
Case 2
A 13-year-old female presented with highly placed, blocked-out upper canines, severe crowding in the upper arch and mild crowding in the lower, competent lips, a non-consonant smile arc, and a straight soft-tissue profile (Fig. 6).
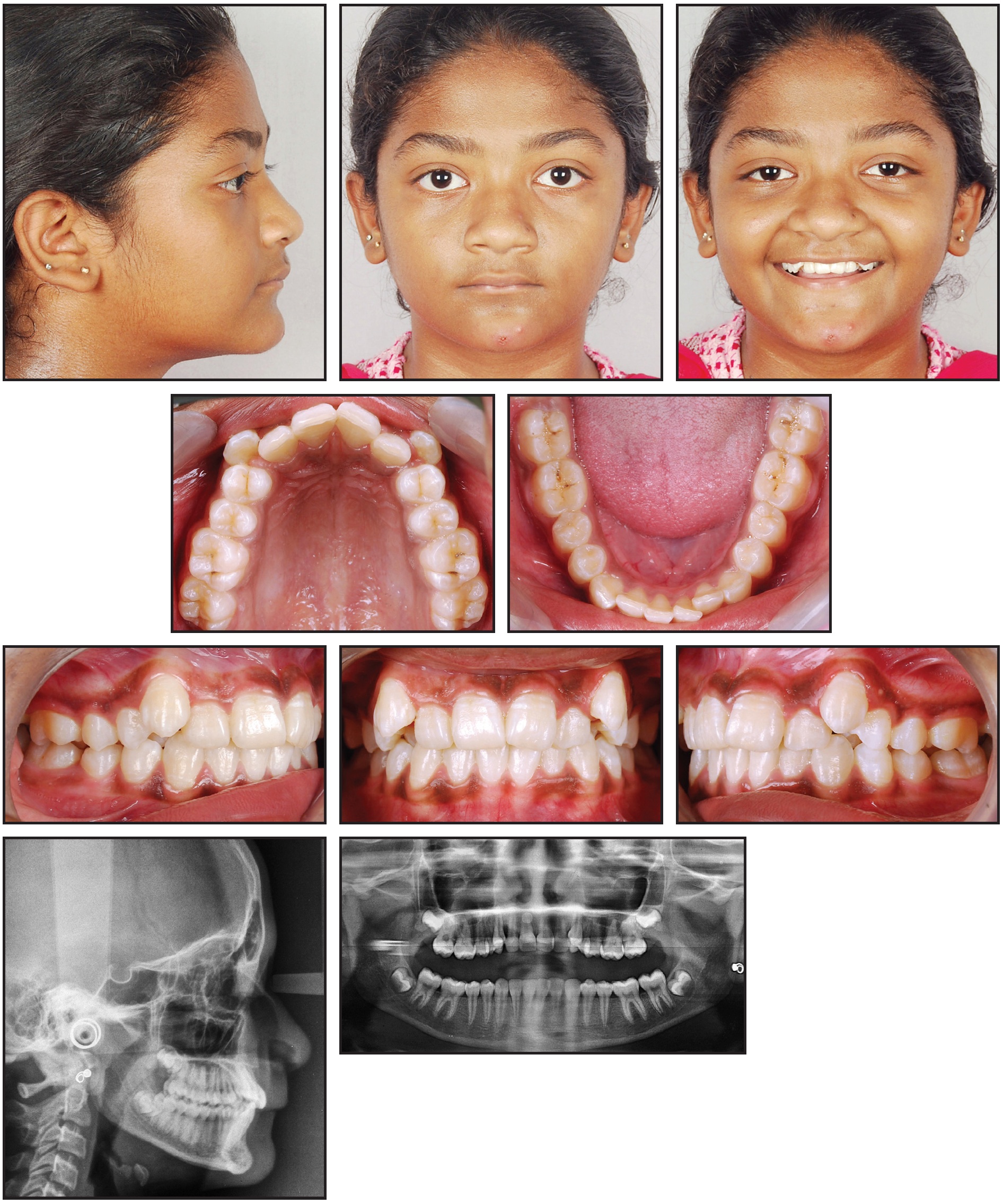
Fig. 6 Case 2. 13-year-old female patient with Class II molar relationship, blocked-out upper canines, severe upper crowding, and mild lower crowding before treatment.
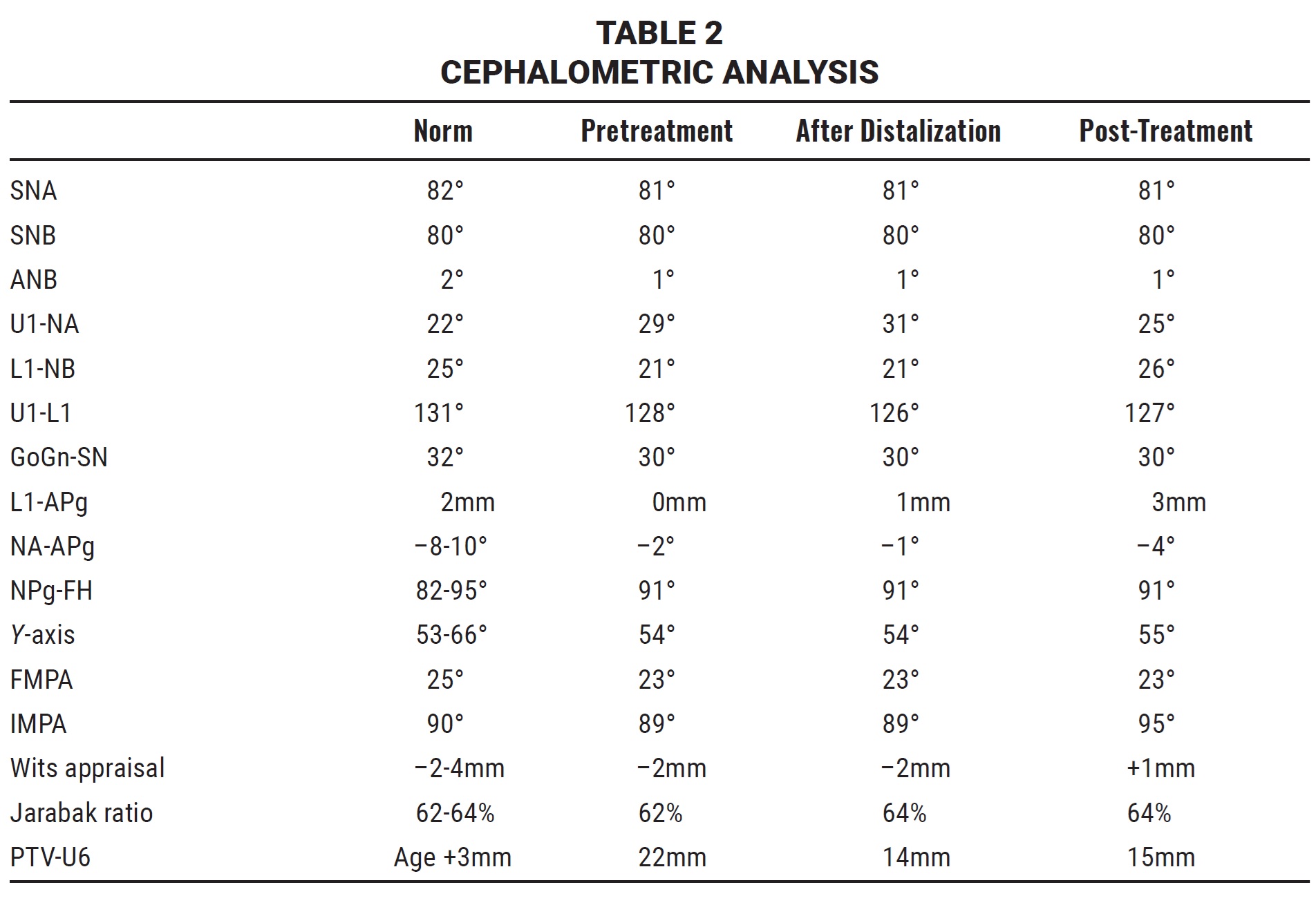
Cephalometric analysis showed a Class II molar relationship on a Class I skeletal base, owing to an orthognathic maxilla and an average mandibular growth pattern (Table 2).
The patient was treated as described in Case 1. After six months of Phase I distalization (Fig. 7), the upper arch was bonded and .014" nickel titanium archwires were inserted.
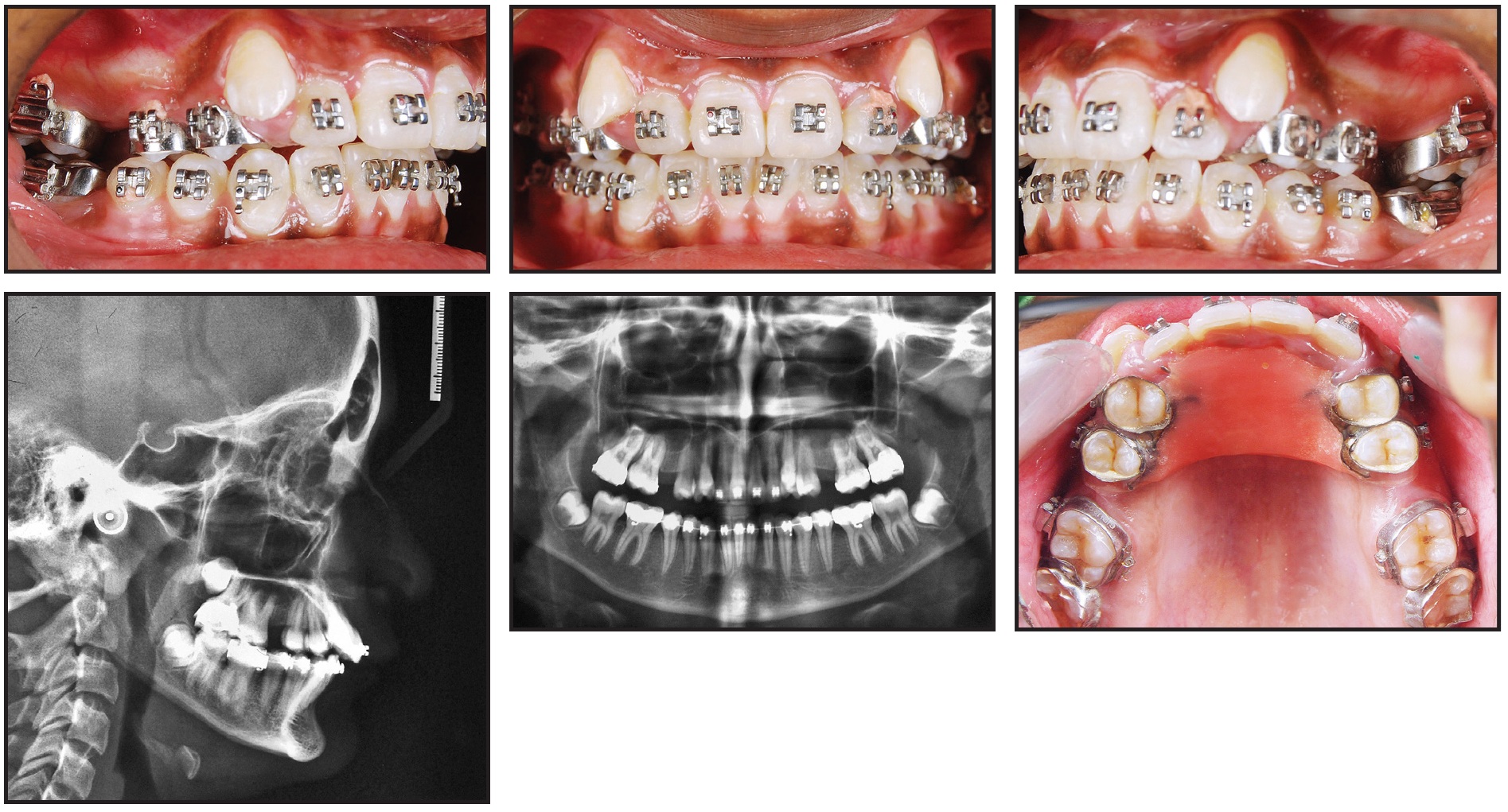
Fig. 7 Case 2. After six months of distalization.
Treatment continued over 14 months, finishing with .019" × .025" TMA† archwires and positive canine torquing.

Fig. 8 Case 2. Patient after 19 months of treatment.
Retention involved upper and lower 3-3 fixed lingual wires and upper and lower Hawley retainers. The results remained stable when evaluated 29 months after treatment (Fig. 9).

Fig. 9 Case 2. Patient 29 months after treatment.
Conclusion
This simple appliance is constructed using items that are readily available in an orthodontic practice. Our results suggest that the Molar Thruster can be an effective, convenient, and cost-effective palatally based molar distalizer for Class II non-compliance treatment. Further investigation is required to fully compare its results with those of other molar-distalizing appliances.
FOOTNOTES
- *Ormco Corporation, Orange, CA; www.ormco.com.
- **American Orthodontics, Sheboygan, WI; www.americanortho.com.
- ***Forestadent GmbH, Pforzheim, Germany; www.forestadent.com.
- †Registered trademark of Ormco Corporation, Orange, CA; www.ormco.com.
REFERENCES
- 1. Corbett, M.C.: Slow and continuous maxillary expansion, molar rotation, and molar distalization, J. Clin. Orthod. 31:253-263, 1997.
- 2. Poulton, D.R.: The influence of extraoral traction, Am. J. Orthod. 53:8-18, 1967.
- 3. Cangialosi, T.J.; Melstrell, M.E. Jr.; Leung, M.A.; and Ko, J.Y.: Cephalometric appraisal of edgewise Class II nonextraction treatment with extraoral force, Am. J. Orthod. 93:315-324, 1988.
- 4. Arvystas, M.G.: Nonextraction treatment of severe Class II, division 2 malocclusions: Part 2, Am. J. Orthod. 99:74-84, 1991.
- 5. Hilgers, J.J.: The Pendulum appliance for Class II non-compliance therapy, J. Clin. Orthod. 26:706-714, 1992.
- 6. Carano, A. and Testa, M.: The Distal Jet for upper molar distalization, J. Clin. Orthod. 30:374-380, 1996.
- 7. Brickman, C.D.; Sinha, P.K.; and Nanda, R.S.: Evaluation of the Jones Jig appliance for distal molar movement, Am. J. Orthod. 118:526-534, 2000.
- 8. Bayram, M.; Nur, M.; and Kilkis, D.: The Frog appliance for upper molar distalization: A case report, Kor. J. Orthod. 40:50-60, 2010.
- 9. Kalra, V.: The K-Loop molar distalizing appliance, J. Clin. Orthod. 26:60-61, 1995.
-
 DR. GANDHI
DR. GANDHI -
 DR. MEHTA
DR. MEHTA -
 DR. PAREKH
DR. PAREKH -
 DR. AGRAWAL
DR. AGRAWAL
Drs. Gandhi and Agrawal are third-year postgraduate students, Dr. Mehta is Head, and Dr. Parekh is a tutor, Department of Orthodontics, Government Dental College and Hospital, Civil Hospital Road, Asarwa, Ahmedabad, Gujarat 380016, India. E-mail Dr. Gandhi at smiledesigner1988@gmail.com.
