Dual Action Vertical Intra-Arch Technique
Open bite is one of the most difficult malocclusions to treat because its etiology is multifactorial, involving both genetic and environmental factors.1-6 Dental open bite, generally restricted to the canines and incisors, is associated with a balanced facial pattern, undererupted anterior teeth, normal or slightly excessive molar height, and sucking habits.2,6 Skeletal open bite is often characterized by excessive lower anterior facial height and upper molar height, divergence between the palatal and mandibular planes and the maxillary and mandibular occlusal planes, clockwise mandibular rotation, an excessive mandibular-plane angle, and mesial angulation of the posterior teeth.2,6-10 Most open-bite patients present some degree of dental and skeletal imbalance.4-6,8,11
The choice of an orthodontic treatment modality for open-bite correction depends on the causative factors, the degree of dental and skeletal involvement, the patient’s growth potential, the patient’s self-perception and expectations, the anticipated compliance level, the biological and financial costs of treatment, and the clinician’s skill.2,5,6,12,13 Nonsurgical options for late adolescent and adult patients include vertical anterior elastics, designed to achieve anterior extrusion, maxillary incisor uprighting, and some uprighting of the mandibular posterior teeth2,3,5,14-21; the multiloop edgewise archwire (MEAW) technique, which produces posterior uprighting, occlusal-plane rotation, anterior extrusion, and some posterior intrusion5,19,20; an extrusion arch for anterior extrusion and mesial tipping of the posterior teeth22; or skeletal anchorage from mini-implants or miniplates, aimed at molar intrusion and occlusal-plane alteration.12,23-29 The dentoalveolar effects of these protocols cannot be calibrated, however, to suit a particular patient’s needs. Moreover, patient compliance is critical when vertical anterior elastics or removable appliances such as high-pull headgear or active vertical correctors are used.7,27,30-32
The Dual Action Vertical Intra-Arch Technique (DAVIT) was designed to simultaneously produce posterior intrusion and anterior extrusion in open-bite treatment, without the need for patient cooperation. A “davit” is a small crane-like device with a pair of power arms for suspending or lowering loads on ships, corresponding to the design and action of this new orthodontic appliance (Fig. 1).
The DAVIT is fabricated by making six right-angle bends in an .017" × .025" TMA wire, resulting in a horizontal anchorage segment, two vertical extensions, and two horizontal power arms with vertical plugs at the ends (Fig. 2A). The horizontal anchorage segment is fitted into the slot of a bracket-head mini-implant, while the vertical plugs of the horizontal power arms are inserted into the vertical slots of orthodontic cross-tubes positioned between the lateral incisor and canine and the first and second molars (Fig. 2B).
Similar articles from the archive:
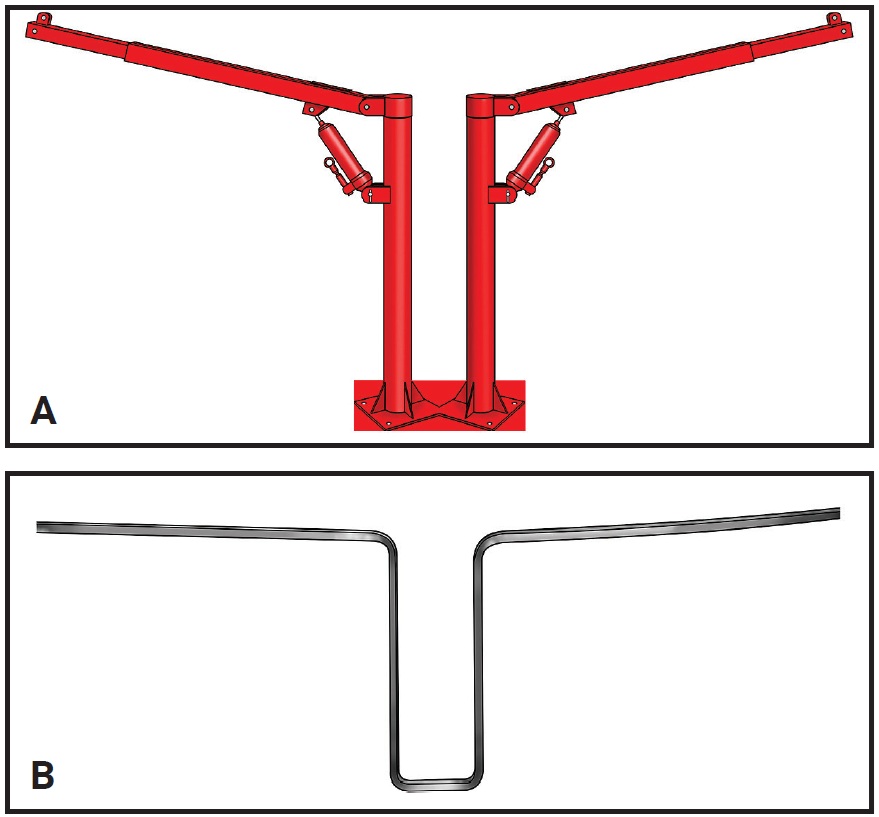
Fig. 1 A. Davit: small, crane-like device for suspending or lowering loads. B. Dual Action Vertical Intra-Arch Technique (DAVIT) appliance used to intrude or extrude teeth.
Before beginning vertical mechanics with the DAVIT, all teeth should be aligned and the interproximal contacts closed, with an .019" × .025" stainless steel archwire in place. The DAVIT is initially inserted into the slot of the mini-implant head to program its clinical action. If the horizontal arms are level with the archwire, the device is considered passive (Fig. 3A). If either arm is apical to the archwire, it is activated for intrusion in this segment (Fig. 3B). If an arm is occlusal to the archwire, it is activated for extrusion.
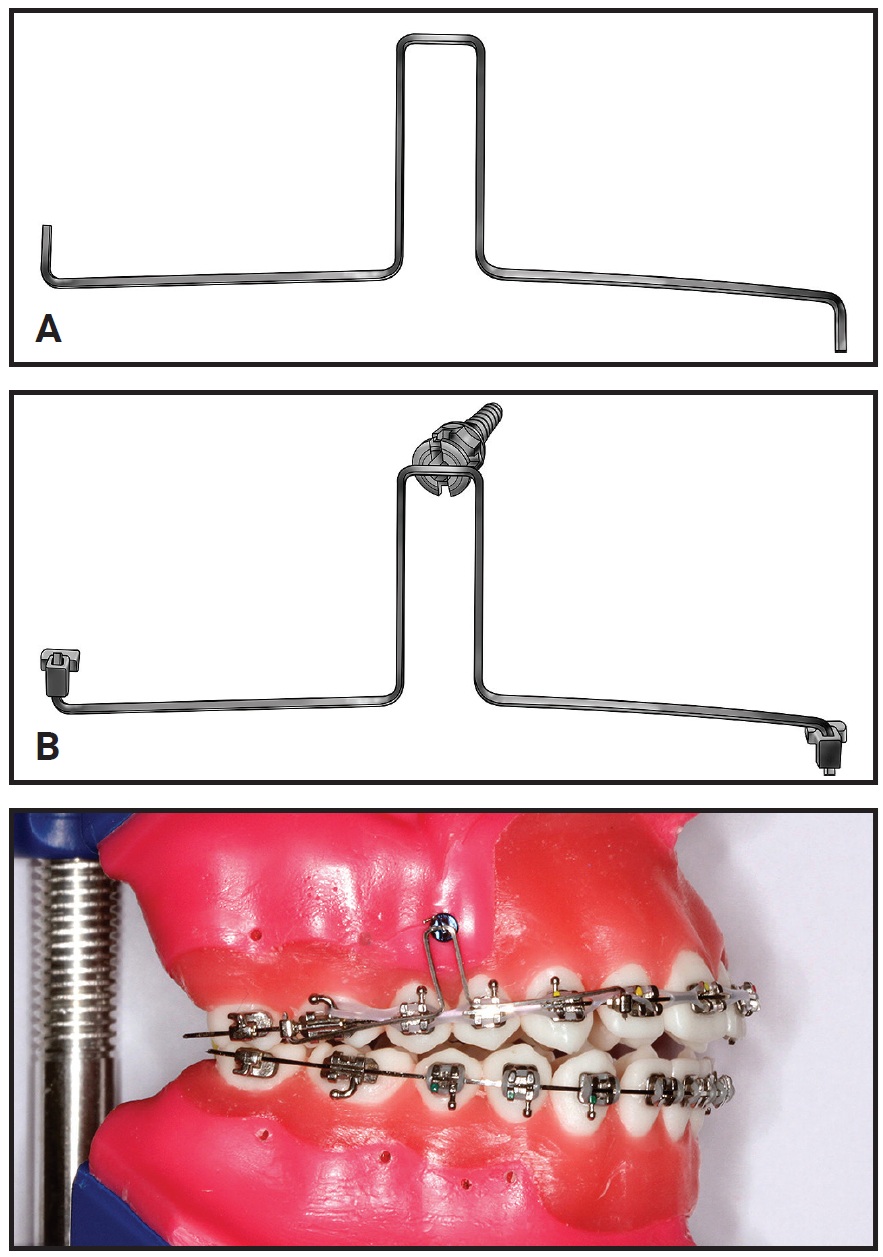
Fig. 2 A. DAVIT appliance fabricated from .017" × .025" TMA* wire. B. Horizontal anchorage segment fitted to bracket-head mini-implant; vertical plugs inserted in cross-tubes positioned in anterior and posterior segments.
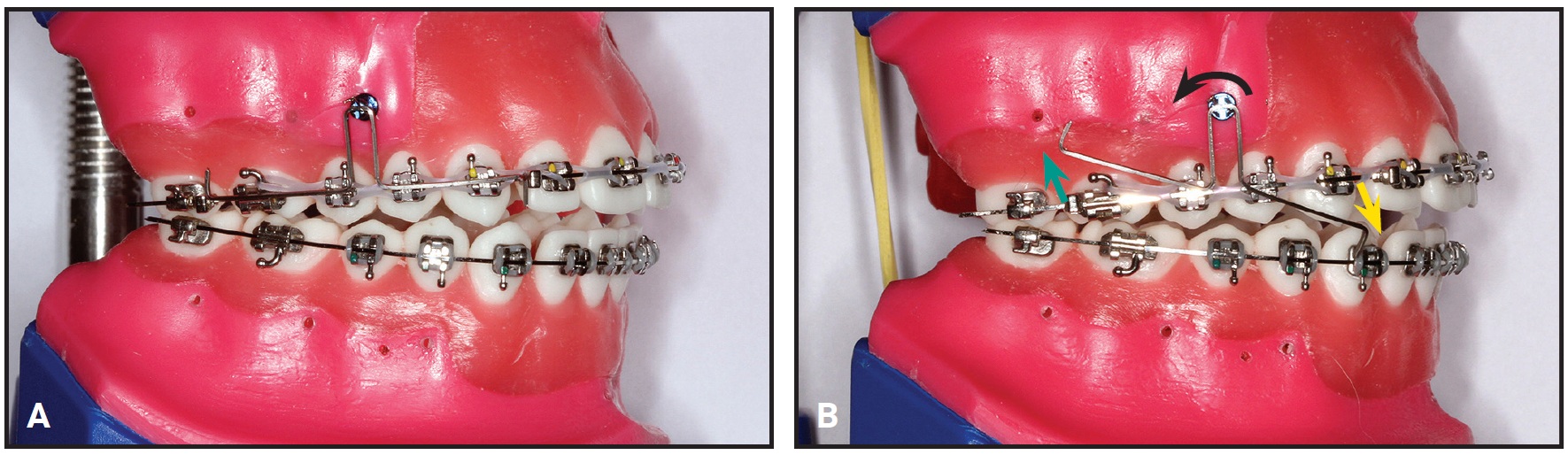
Fig. 3 A. Horizontal power arms level with archwire, indicating passive position of DAVIT. B. DAVIT appliance activated to intrude posterior segment (green arrow) and extrude anterior segment (yellow arrow).
Thus, equal or opposite tooth-movement directions can be obtained in each DAVIT segment, allowing different rates of vertical movement (intrusion or extrusion) to meet the patient’s specific needs. An open bite can be closed with predominantly posterior or predominantly anterior extrusion, or with a balanced combination of the two. This dual vertical action seems to greatly improve the efficiency of open-bite correction. In addition, the DAVIT can be used in both arches—especially in more severe open-bite cases—to further enhance its efficiency, since posterior intrusion and anterior extrusion can be performed simultaneously in both arches (Fig. 4).
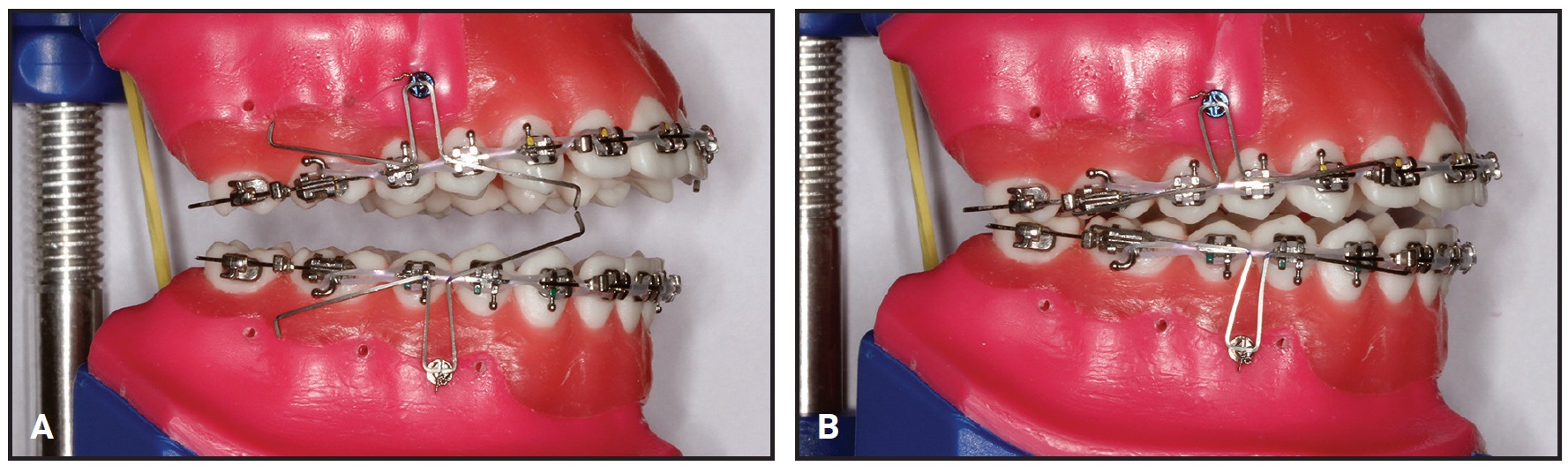
Fig. 4 A. DAVIT appliance activated for posterior intrusion and anterior extrusion in both arches. B. Dual action (intrusion and extrusion) can further improve efficiency of open-bite correction.
The mini-implant is positioned between the premolars and about 12mm apical to the occlusal plane, close to the center of resistance of the dental arch.33 When posterior intrusive and anterior extrusive forces are simultaneously applied from this point, a moment is created to rotate the arch around its center of resistance.33,34 This is because a group of teeth joined together by a stiff archwire will rotate around a point approximating the combined center of resistance.33 Anterior extrusion, posterior intrusion, occlusal-plane rotation, and posterior uprighting occur simultaneously, without unwanted dental side effects (Fig. 5).5,10,16,19,27
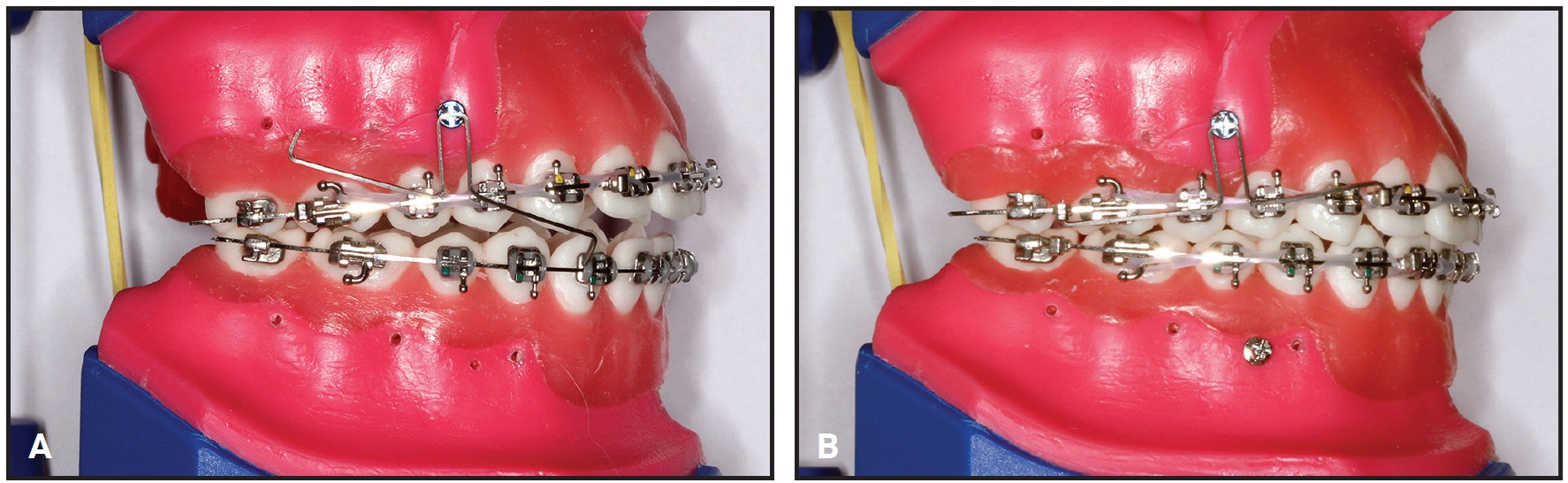
Fig. 5 A. DAVIT appliance activated for posterior intrusion and anterior extrusion in upper arch only. B. Post-treatment setup indicates posterior intrusion, anterior extrusion, clockwise occlusal-plane rotation, and posterior uprighting.
Rotational forces are known to cause mini-implant failure, especially when immediate loading is performed.35 The DAVIT’s dual vertical action produces a counterclockwise rotation moment on the upper right mini-implant and a clockwise rotation moment on the upper left mini-implant. Therefore, counterclockwise and clockwise mini-implant thread directions are imperative to ensure miniscrew stability on the right and left sides, respectively. When the DAVIT is used in the lower arch for open-bite closure, the opposite scenario applies, requiring a clockwise thread on the right side and a counterclockwise thread on the left.
Case Report
A 13-year-old female presented with the chief complaint of an anterior open bite (Fig. 6).
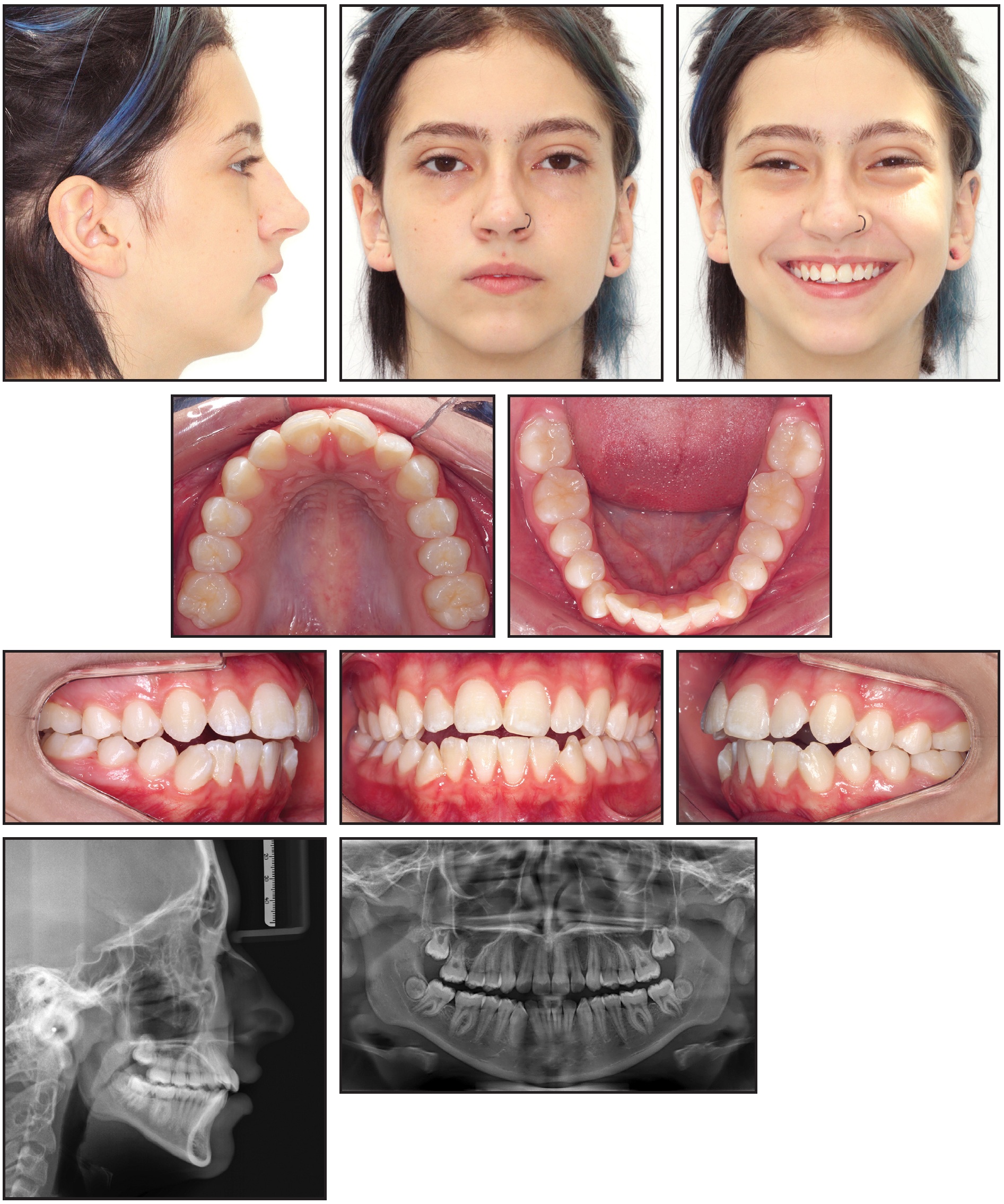
Fig. 6 13-year-old female patient with bilateral Class I molar relationship, anterior open bite, moderate lower anterior crowding, and excessive overjet before treatment (continued in next image).
Clinical examination confirmed an anterior open bite extending from first premolar to first premolar, a bilateral Class I molar relationship, moderate lower anterior crowding, and excessive overjet. The panoramic radiograph revealed the presence of unerupted upper second and lower third molars and agenesis of the upper third molars. The upper second molars were favorably positioned for later eruption,36 with incomplete rhizogenesis (Fig. 6B). There was no deviation between centric occlusion and centric relation, and there were no signs of TMD. Cephalometric analysis found an anteroposterior maxillomandibular discrepancy with mandibular deficiency, a slightly vertical growth pattern with an excessive mandibular-plane angle, and a convex skeletal profile. The upper incisors were slightly protrusive, but the lower incisors were well positioned.
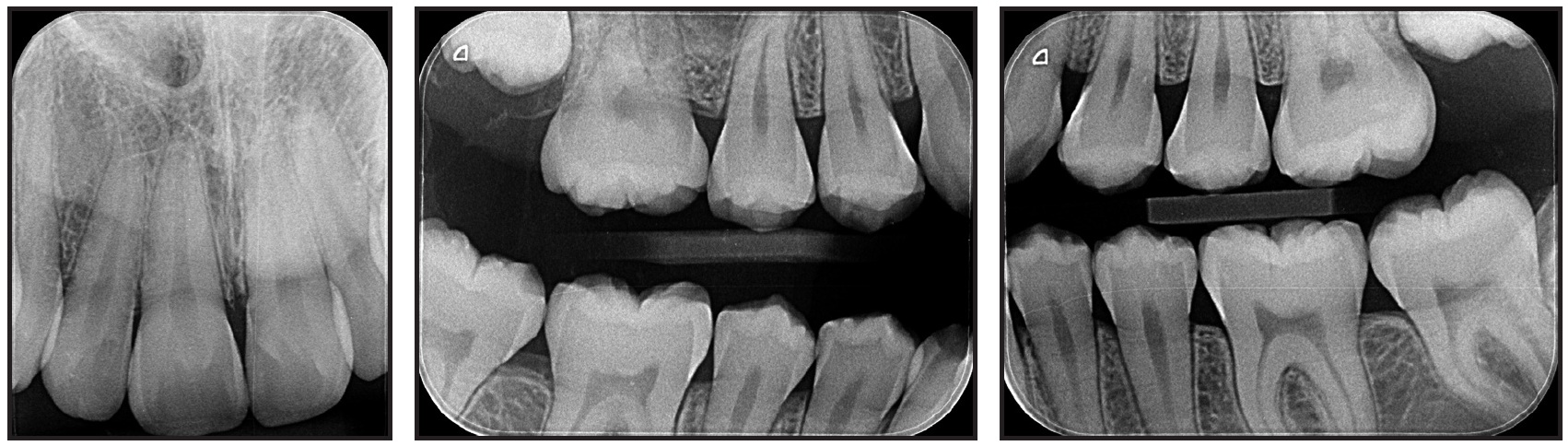
Fig. 6 (cont.) 13-year-old female patient with bilateral Class I molar relationship, anterior open bite, moderate lower anterior crowding, and excessive overjet before treatment.
The DAVIT device was chosen for treatment because the patient’s vertical facial pattern and smile esthetics were favorable for open-bite closure by simultaneous posterior intrusion and anterior extrusion, and because compliance with removable appliances was unpredictable.37
Full .022" × .028" preadjusted appliances were placed in both arches. Leveling and alignment began on .012" and .014" nickel titanium archwires, followed by .016", .018", .020", and .019" × .025" stainless steel.
After seven months of treatment, the initial alignment was complete. A bracket-head mini-implant (1.5mm × 8mm, with a 1mm transmucosal collar) was inserted on each side between the upper premolars to provide skeletal anchorage for the DAVIT device (Fig. 7). The right and left mini-implants had counterclockwise and clockwise thread directions, respectively, to prevent screw failure due to the rotational force load.35 The posterior power arms of the DAVIT were activated above the .019" × .025" alignment archwire to produce a posterior intrusive force of about 300g per side. The anterior power arms were activated below the archwire to produce an anterior extrusive force of about 150g on each side, for a total 300g of anterior extrusive force. The horizontal anchorage segments of the DAVIT were tied into the mini-implant bracket slots with .008" stainless steel ligature wire. Finally, the activated vertical plugs at the ends of the horizontal power arms were inserted into the vertical slots of orthodontic cross-tubes positioned between the lateral incisor and canine and between the second premolar and first molar on each side of the maxillary arch.

Fig. 7 After seven months of alignment, mini-implants inserted between upper premolars, and DAVIT appliances activated to correct open bite by posterior intrusion and anterior extrusion.
After two months of treatment with the DAVIT appliance, the open bite was completely closed and interocclusal contact between the premolars had substantially increased (Fig. 8).

Fig. 8 After two months of DAVIT treatment, open bite closed and vertical relationship between premolars substantially improved.
To minimize the possibility of post-treatment relapse,38 however, the DAVIT was reactivated using the same protocol. Two months later, the desired overcorrection had been achieved (Fig. 9).

Fig. 9 After four months of DAVIT treatment, overcorrection of open bite obtained.
The DAVIT device was then kept passively in place for another two months to stabilize the dentoalveolar changes (Fig. 10).

Fig. 10 After two months of passive retention with DAVIT to stabilize changes.
Intermaxillary elastics were not prescribed to improve the overbite, posterior intercuspation, or anteroposterior relationship during the finishing phase. The fixed appliances and mini-implants were removed, and an upper Hawley and lower 3-3 fixed lingual retainer were placed for retention.
Total treatment time was 13 months (Fig. 11A).
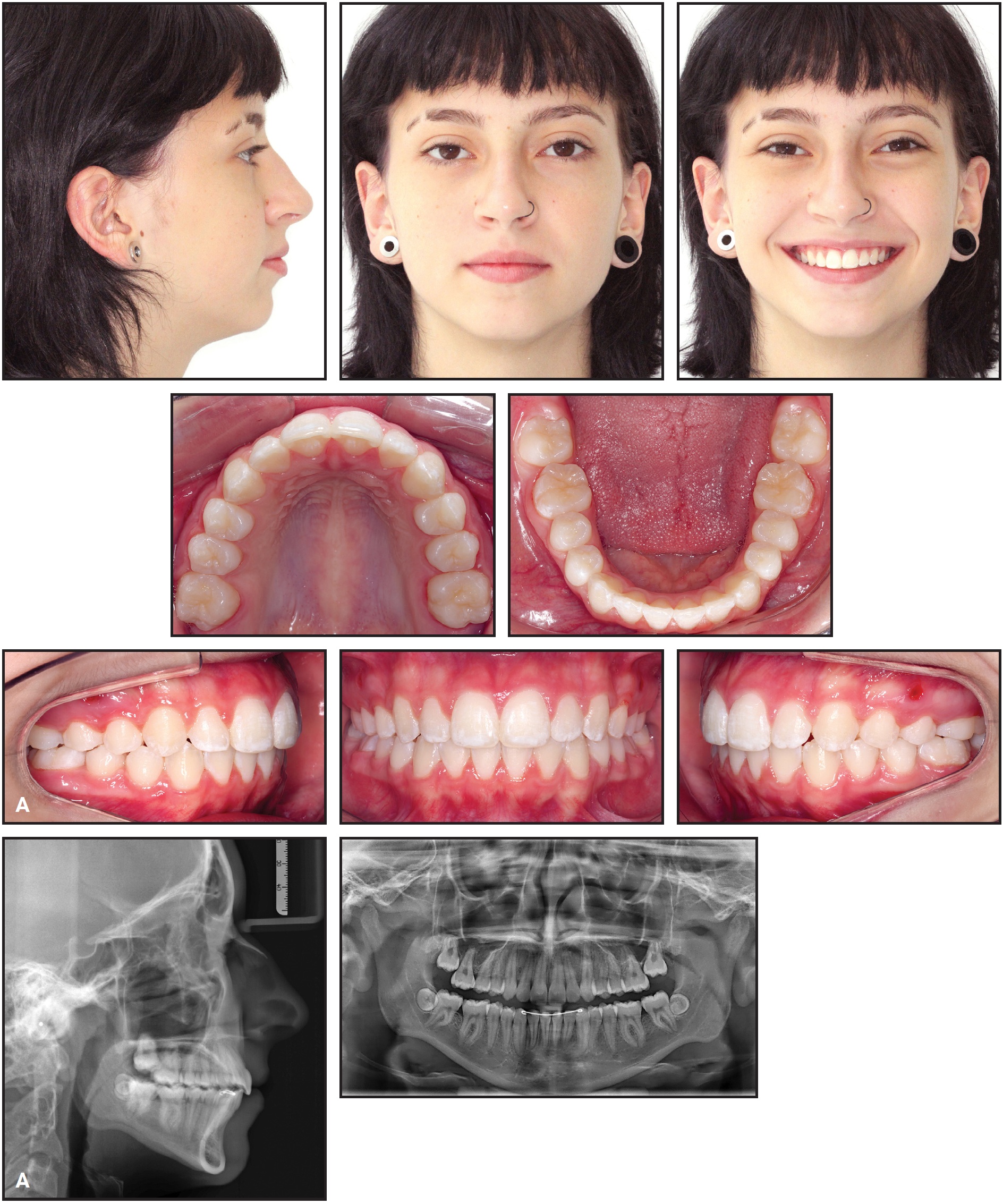
Fig. 11 A. Patient after 13 months of treatment (continued in next image).
Excellent smile esthetics and a static and functional occlusion were obtained. The upper incisors were extruded and palatally tipped, while the upper molars were intruded. The occlusal plane underwent clockwise rotation, and the upper posterior teeth were uprighted. Consequently, the anterior open bite was closed, the overbite was overcorrected, and occlusal contact was established between the premolars. The Class I molar relationship and the posterior transverse relationship were maintained. The lower incisors were protruded to resolve the anterior crowding. External apical root resorption involved no more than slight rounding, which is considered clinically acceptable.39 The upper second molars were erupting toward the occlusal plane, but the left second molar showed a less favorable eruption axis; therefore, the patient was kept under observation to evaluate whether surgical intervention would be required (Fig. 11B).
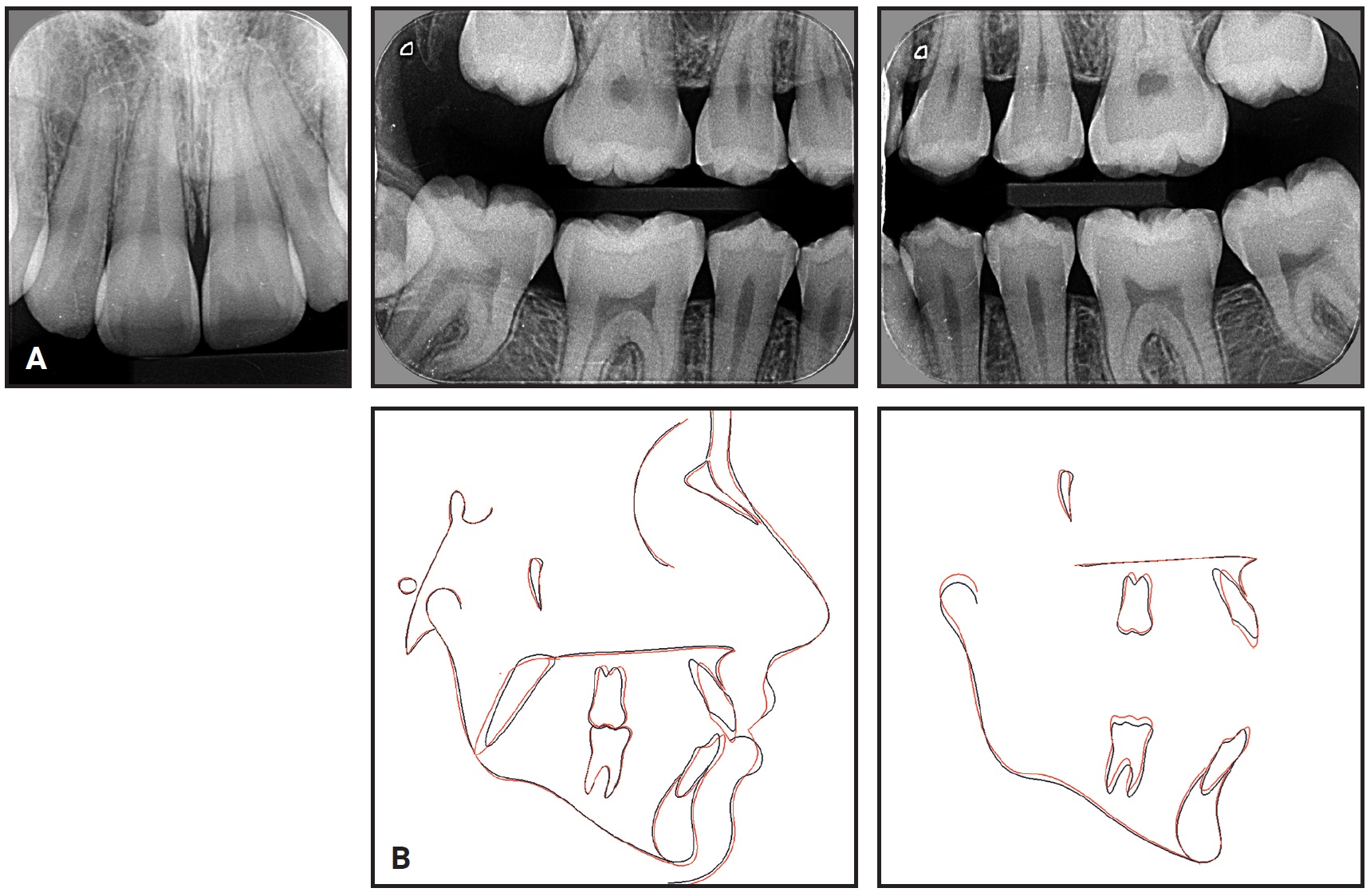
Fig. 11 (cont.) A. Patient after 13 months of treatment. B. Superimposition of pretreatment (black) and post-treatment (red) cephalometric tracings.
Discussion
Extrusion of anterior teeth is a common objective in treating dental open bite, while skeletal open bite may require posterior intrusion. Considering the wide variety of skeletal open-bite characteristics and the frequent mixture of skeletal and dental factors, however, anterior extrusion may be carried out in many skeletal open-bite patients without compromising smile esthetics.4-6,8 While vertical anterior elastics and extrusion arches have been widely used for anterior extrusion in such cases,22 an attempt to close an open bite by anterior extrusion alone may require more vertical movement of the incisors than the patient’s smile esthetics allow.40,41 Vertical anterior elastics have some uprighting effect on the mandibular posterior teeth,16 but they cannot intrude the posterior teeth. In addition, the success of vertical anterior elastics depends on patient compliance.5,7,19,22,31 Extrusion arches are not compliance-dependent, but they tend to cause mesial tipping of the posterior teeth.10,22
The DAVIT appliance is an excellent alternative to orthodontic mechanics based only on incisor extrusion. Extrusion of the upper incisors through palatal tipping is another DAVIT effect that contributes greatly to anterior open-bite correction by means of the “drawbridge effect.”2 Although this effect will be more evident in extraction cases, the patient’s soft-tissue profile may contraindicate such treatment, as in the case described here.
The MEAW technique can produce similar dentoalveolar effects to the DAVIT,5,19,20 but it still depends on patient compliance with vertical anterior elastics. Poor patient cooperation can lead to unwanted tooth movements such as anterior intrusion and proclination.5,7,19,31,42,43 MEAW also requires special training on the part of the clinician, and it does not allow the rate of posterior intrusion and anterior extrusion to be planned according to the specific needs of the patient.5,31,42,43 In the present case, the DAVIT was used to correct the open bite primarily by anterior extrusion, since it was not detrimental to the smile esthetics. Incisor extrusion is more easily obtained than molar intrusion, and extrusion is about four times less likely than intrusion to cause external apical root resorption.44,45
Considerable posterior intrusion can be achieved with mini-implant or miniplate anchorage, potentially avoiding surgery in nongrowing patients with severe skeletal open bites.23,24,27,28 In these situations, the DAVIT appliance can be activated to produce maximum posterior intrusion. If extrusion of the upper incisors will have a negative effect on the level of gingival exposure, the anterior power arms of the DAVIT should be activated to prevent this anterior extrusion during posterior intrusion.5,34 The DAVIT can also be used in the mandibular arch to obtain maximum posterior intrusion and anterior extrusion while preserving smile esthetics.26,34 Other appliances are available for active molar intrusion—including magnetic bite blocks, rapid molar intruders, and high-pull headgear—but they are used mainly in the late mixed or early permanent dentition, and many are removable, requiring a high level of patient compliance.32,46-48
Although the dual action of the DAVIT promotes uprighting of the posterior teeth and occlusal-plane rotation, which are beneficial in open-bite cases, there is about a .5mm change in the sagittal occlusal relationship for each degree of occlusal-plane rotation in either the downward and backward or upward and forward directions.33 Therefore, the initial sagittal occlusal relationship should be considered when planning open-bite correction. When the DAVIT appliance is used in the mandibular arch, it produces a counterclockwise rotation of the occlusal plane that can be helpful in correcting Class III occlusal relationships.33,34,49,50 Conversely, when the DAVIT is applied in the maxillary arch, it creates a clockwise rotation of the occlusal plane that can be beneficial in Class II correction.33 The vertical effect of the occlusal-plane rotation on smile esthetics should be carefully evaluated to determine whether anterior extrusion should be restrained by the anterior power arm of the DAVIT, modifying the center of rotation of the dental arch.
Although the DAVIT appliance was conceived primarily for anterior open-bite treatment, we believe it can also be successful in correcting a deep bite if the activation is modified to obtain anterior intrusion and/or posterior extrusion, according to the patient’s needs (Fig. 12). Further studies are underway to evaluate the effects of DAVIT in the correction of different vertical malocclusions.
FOOTNOTES
- *Trademark of Ormco Corporation, Orange, CA; www.ormco.com.
REFERENCES
- 1. Baek, M.S.; Choi, Y.J.; Yu, H.S.; Lee, K.J.; Kwak, J.; and Park, Y.C.: Long-term stability of anterior open-bite treatment by intrusion of maxillary posterior teeth, Am. J. Orthod. 138:396 e1-e9, 2010.
- 2. Beane, R.A. Jr.: Nonsurgical management of the anterior open bite: A review of the options, Semin. Orthod. 5:275-283, 1999.
- 3. Rinchuse, D.J.: Vertical elastics for correction of anterior open bite, J. Clin. Orthod. 28:284, 1994.
- 4. Rosa, M.; Quinzi, V.; and Marzo, G.: Paediatric orthodontics, Part 1: Anterior open bite in the mixed dentition, Eur. J. Paediat. Dent. 20:80-82, 2019.
- 5. Cruz-Escalante, M.A.; Aliaga-Del Castillo, A.; Soldevilla, L.; Janson, G.; Yatabe, M.; and Zuazola, R.V.: Extreme skeletal open bite correction with vertical elastics, Angle Orthod. 87:911-923, 2017.
- 6. Lin, L.; Huang, G.; and Chen, C.: Etiology and treatment modalities of anterior open bite malocclusion, J. Exp. Clin. Med. 5:1-4, 2013.
- 7. Kim, Y.H.: Anterior openbite and its treatment with multiloop edgewise archwire, Angle Orthod. 57:290-321, 1987.
- 8. Cangialosi, T.J.: Skeletal morphologic features of anterior open bite, Am. J. Orthod. 85:28-36, 1984.
- 9. Ngan, P. and Fields, H.W.: Open bite: A review of etiology and management, Pediat. Dent. 19:91-98, 1997.
- 10. Janson, G.; Laranjeira, V.; Rizzo, M.; and Garib, D.: Posterior tooth angulations in patients with anterior open bite and normal occlusion, Am. J. Orthod. 150:71-77, 2016.
- 11. Hotokezaka, H.; Matsuo, T.; Nakagawa, M.; Mizuno, A.; and Kobayashi, K.: Severe dental open bite malocclusion with tongue reduction after orthodontic treatment, Angle Orthod. 71:228-236, 2001.
- 12. Alsafadi, A.S.; Alabdullah, M.M.; Saltaji, H.; Abdo, A.; and Youssef, M.: Effect of molar intrusion with temporary anchorage devices in patients with anterior open bite: A systematic review, Prog. Orthod. 17:9, 2016.
- 13. Proffit, W.R.; Phillips, C.; and Dann, C. IV: Who seeks surgical-orthodontic treatment? Int. J. Adult Orthod. Orthog. Surg. 5:153-160, 1990.
- 14. Janson, G.; Valarelli, F.P.; Henriques, J.F.; De Freitas, M.R.; and Cançado, R.H.: Stability of anterior open bite nonextraction treatment in the permanent dentition, Am. J. Orthod. 124:265-276, 2003.
- 15. Janson, G.; Valarelli, F.P.; Beltrão, R.T.; De Freitas, M.R.; and Henriques, J.F.: Stability of anterior open-bite extraction and nonextraction treatment in the permanent dentition, Am. J. Orthod. 129:768-774, 2006.
- 16. Janson, G.; Rizzo, M.; Laranjeira, V.; Garib, D.G.; and Valarelli, F.P.: Posterior teeth angulation in non-extraction and extraction treatment of anterior open-bite patients, Prog. Orthod. 18:13, 2017.
- 17. Antelo, O.M.; Meira, T.M.; Oliveira, D.D.; Pithon, M.M.; and Tanaka, O.M.: Long-term stability of a Class III malocclusion with severe anterior open bite and bilateral posterior crossbite in a hyperdivergent patient, Am. J. Orthod. 157:408-421, 2020.
- 18. Jefferson, Y.: Anterior open bite—simplified non surgical technique to correct in adults, Int. J. Orthod. Milwaukee 26:19-24, 2015.
- 19. Chang, Y.I. and Moon, S.C.: Cephalometric evaluation of the anterior open bite treatment, Am. J. Orthod. 115:29-38, 1999.
- 20. Küçükkeleş, N.; Acar, A.; Demirkaya, A.A.; Evrenol, B.; and Enacar, A.: Cephalometric evaluation of open bite treatment with NiTi arch wires and anterior elastics, Am. J. Orthod. 116:555-562, 1999.
- 21. Endo, T.; Kojima, K.; Kobayashi, Y.; and Shimooka, S.: Cephalometric evaluation of anterior open-bite nonextraction treatment, using multiloop edgewise archwire therapy, Odontol. 94:51-58, 2006.
- 22. Isaacson, R.J. and Lindauer, S.J.: Closing anterior open bites: The extrusion arch, Semin. Orthod. 7:34-41, 2001.
- 23. Hart, T.R.; Cousley, R.R.; Fishman, L.S.; and Tallents, R.H.: Dentoskeletal changes following mini-implant molar intrusion in anterior open bite patients, Angle Orthod. 85:941-948, 2015.
- 24. Xun, C.; Zeng, X.; and Wang, X.: Microscrew anchorage in skeletal anterior open-bite treatment, Angle Orthod. 77:47-56, 2007.
- 25. Park, H.S.; Kwon, O.W.; and Sung, J.H.: Nonextraction treatment of an open bite with microscrew implant anchorage, Am. J. Orthod. 130:391-402, 2006.
- 26. Umemori, M.; Sugawara, J.; Mitani, H.; Nagasaka, H.; and Kawamura, H.: Skeletal anchorage system for open-bite correction, Am. J. Orthod. 115:166-174, 1999.
- 27. Erverdi, N.; Keles, A.; and Nanda, R.: The use of skeletal anchorage in open bite treatment: A cephalometric evaluation, Angle Orthod. 74:381-390, 2004.
- 28. Park, Y.C.; Lee, H.A.; Choi, N.C.; and Kim, D.H.: Open bite correction by intrusion of posterior teeth with miniscrews, Angle Orthod. 78:699-710, 2008.
- 29. Foot, R.; Dalci, O.; Gonzales, C.; Tarraf, N.E.; and Darendeliler, M.A.: The short-term skeleto-dental effects of a new spring for the intrusion of maxillary posterior teeth in open bite patients, Prog. Orthod. 15:56, 2014.
- 30. Kaku, M.; Kawai, A.; Koseki, H.; Abedini, S.; Kawazoe, A.; Sasamoto, T.; Sunagawa, H.; Yamamoto, R.; Tsuka, N.; Motokawa, M.; Ohtani, J.; Fujita, T.; Kawata, T.; and Tanne, K.: Correction of severe open bite using miniscrew anchorage, Austral. Dent. J. 54:374-380, 2009.
- 31. Ribeiro, G.L.; Regis, S. Jr.; Da Cunha Tde, M.; Sabatoski, M.A.; Guariza-Filho, O.; and Tanaka, O.M.: Multiloop edgewise archwire in the treatment of a patient with an anterior open bite and a long face, Am. J. Orthod. 138:89-95, 2010.
- 32. Dellinger, E.L.: A clinical assessment of the Active Vertical Corrector—a nonsurgical alternative for skeletal open bite treatment, Am. J. Orthod. 89:428-436, 1986.
- 33. Braun, S. and Legan, H.L.: Changes in occlusion related to the cant of the occlusal plane, Am. J. Orthod. 111:184-188, 1997.
- 34. Roberts, W.E.; Viecilli, R.F.; Chang, C.; Katona, T.R.; and Paydar, N.H.: Biology of biomechanics: Finite element analysis of a statically determinate system to rotate the occlusal plane for correction of a skeletal Class III open-bite malocclusion, Am. J. Orthod. 148:943-955, 2015.
- 35. Cho, Y.M.; Cha, J.Y.; and Hwang, C.J.: The effect of rotation moment on the stability of immediately loaded orthodontic miniscrews: A pilot study, Eur. J. Orthod. 32:614-619, 2010.
- 36. Johnson, E.: Managing second molars, Am. J. Orthod. 140:269-273, 2011.
- 37. Sergl, H.G. and Zentner, A.: Predicting patient compliance in orthodontic treatment, Semin. Orthod. 6:231-236, 2000.
- 38. Salehi, P.; Pakshir, H.R.; and Hoseini, S.A.: Evaluating the stability of open bite treatments and its predictive factors in the retention phase during permanent dentition, J. Dent. (Shiraz) 16:22-29, 2015.
- 39. Deng, Y.; Sun, Y.; and Xu, T.: Evaluation of root resorption after comprehensive orthodontic treatment using cone beam computed tomography (CBCT): A meta-analysis, BMC Oral Health 18:116, 2018.
- 40. Tosun, H. and Kaya, B.: Effect of maxillary incisors, lower lip, and gingival display relationship on smile attractiveness, Am. J. Orthod. 157:340-347, 2020.
- 41. Peck, S.; Peck, L.; and Kataja, M.: The gingival smile line, Angle Orthod. 62:91-100, 1992.
- 42. Freitas, B.V.; Abas Frazão, M.C.; Dias, L.; Fernandes Dos Santos, P.C.; Freitas, H.V.; and Bosio, J.A.: Nonsurgical correction of a severe anterior open bite with mandibular molar intrusion using mini-implants and the multiloop edgewise archwire technique, Am. J. Orthod. 153:577-587, 2018.
- 43. Xu, Z.; Hu, Z.; Wang, X.; and Shen, G.: Severe anterior open bite with mandibular retrusion treated with multiloop edgewise archwires and microimplant anchorage complemented by genioplasty, Am. J. Orthod. 146:655-664, 2014.
- 44. Han, G.; Huang, S.; Von den Hoff, J.W.; Zeng, X.; and Kuijpers-Jagtman, A.M.: Root resorption after orthodontic intrusion and extrusion: An intraindividual study, Angle Orthod. 75:912-918, 2005.
- 45. Topkara, A.; Karaman, A.I.; and Kau, C.H.: Apical root resorption caused by orthodontic forces: A brief review and a long-term observation, Eur. J. Dent. 6:445-453, 2012.
- 46. Albogha, M.H.; Takahashi, I.; and Sawan, M.N.: Early treatment of anterior open bite: Comparison of the vertical and horizontal morphological changes induced by magnetic bite-blocks and adjusted rapid molar intruders, Kor. J. Orthod. 45:38-46, 2015.
- 47. Cinsar, A.; Alagha, A.R.; and Akyalçin, S.: Skeletal open bite correction with rapid molar intruder appliance in growing individuals, Angle Orthod. 77:632-639, 2007.
- 48. Menezes, L.M.; Ritter, D.E.; and Locks, A.: Combining traditional techniques to correct anterior open bite and posterior crossbite, Am. J. Orthod. 143:412-420, 2013.
- 49. Carrière, L.: Nonsurgical correction of severe skeletal Class III malocclusion, J. Clin. Orthod. 50:216-230, 2016.
- 50. Baek, S.H.; Shin, S.J.; Ahn, S.J.; and Chang, Y.I.: Initial effect of multiloop edgewise archwire on the mandibular dentition in Class III malocclusion subjects: A three-dimensional finite element study, Eur. J. Orthod. 30:10-15, 2008.
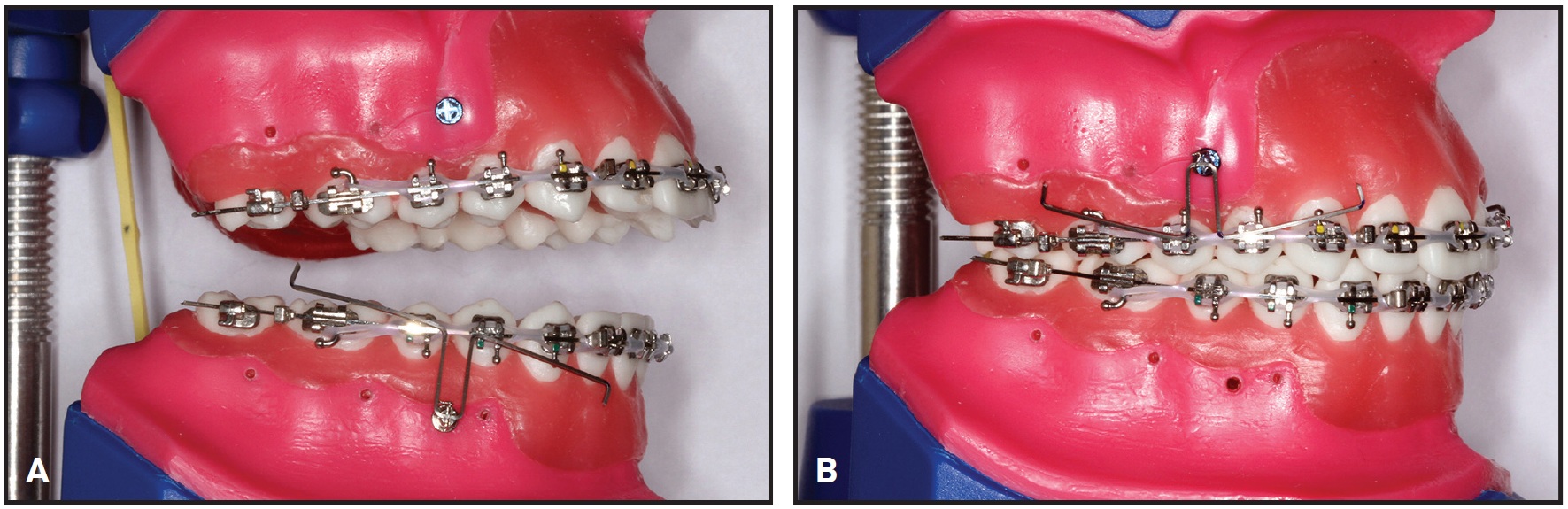
Fig. 12 A. Activation of DAVIT to correct deep bite with simultaneous anterior intrusion and posterior extrusion. B. Symmetrical activation of DAVIT arms to correct anterior and posterior vertical maxillary excess.
-
 DR. BARROS
DR. BARROS -
 DR. CHIQUETO
DR. CHIQUETO -
 DR. GUILHERME JANSON
DR. GUILHERME JANSON -
 DR. MARCOS JANSON
DR. MARCOS JANSON
Dr. Barros is an Associate Professor and Dr. Chiqueto is an Adjunct Professor, Department of Orthodontics, Faculty of Dentistry, Federal University of Rio Grande do Sul, Rua Ramiro Barcelos, 2492 Bairro Santana, Porto Alegre 90035-003, Brazil. Dr. G. Janson was a Professor and Department Head, Department of Orthodontics, Bauru Dental School, University of São Paulo, Bauru, Brazil. Dr. M. Janson is in the private practice of orthodontics in Bauru, Brazil. E-mail Dr. Barros at sergioestelita@yahoo.com.br.