Hybrid Aligner Therapy for Growing Patients with Anterior Open Bites
Anterior open bite is one of the most challenging malocclusions to treat.1 The etiology is generally multifactorial, involving a combination of skeletal, dental, and soft-tissue problems. The prevalence is reportedly 17-18% among all children in the mixed dentition,2-4 but increases to 36.3% in patients with prolonged sucking habits and hyperdivergent vertical relationships.5
Oral habits and mouthbreathing represent risk factors for the development of anterior open bite because they affect the physiological balance of growth. Early interception is crucial to prevent a worsening of the malocclusion and to promote optimal development of the masticatory system. Some self-correction of the overbite can be expected from the deciduous to the late mixed dentition, but no significant changes will occur in the pubertal and post-pubertal stages.6 Although early treatment of anterior open bite seems to be supported by the literature, more studies with longer follow-up periods are needed to evaluate the effectiveness of various treatment strategies and the long-term stability of results.7,8
This article demonstrates a two-phase approach to the treatment of anterior open bite. The interceptive phase corrects the orthopedic problems, thus promoting favorable growth and simplifying the second phase, which is carried out with clear aligners.
Case 1
An 8-year-old male presented for treatment with a well-proportioned face, a slight deviation of the mandibular symphysis toward the left, a receding chin, a retrusive mandible, and a normal nasolabial angle (Fig. 1). The upper midline seemed to be coincident with the facial midline, although there was a diastema between the central incisors, and the lateral incisors had not yet erupted. The patient was in the first phase of the transitional dentition, with a Class I molar relationship, transverse maxillary constriction, excessive anterior overjet, and negative overbite. A long-term tongue-thrust habit had contributed to the development of a severe anterior open bite.
Similar articles from the archive:
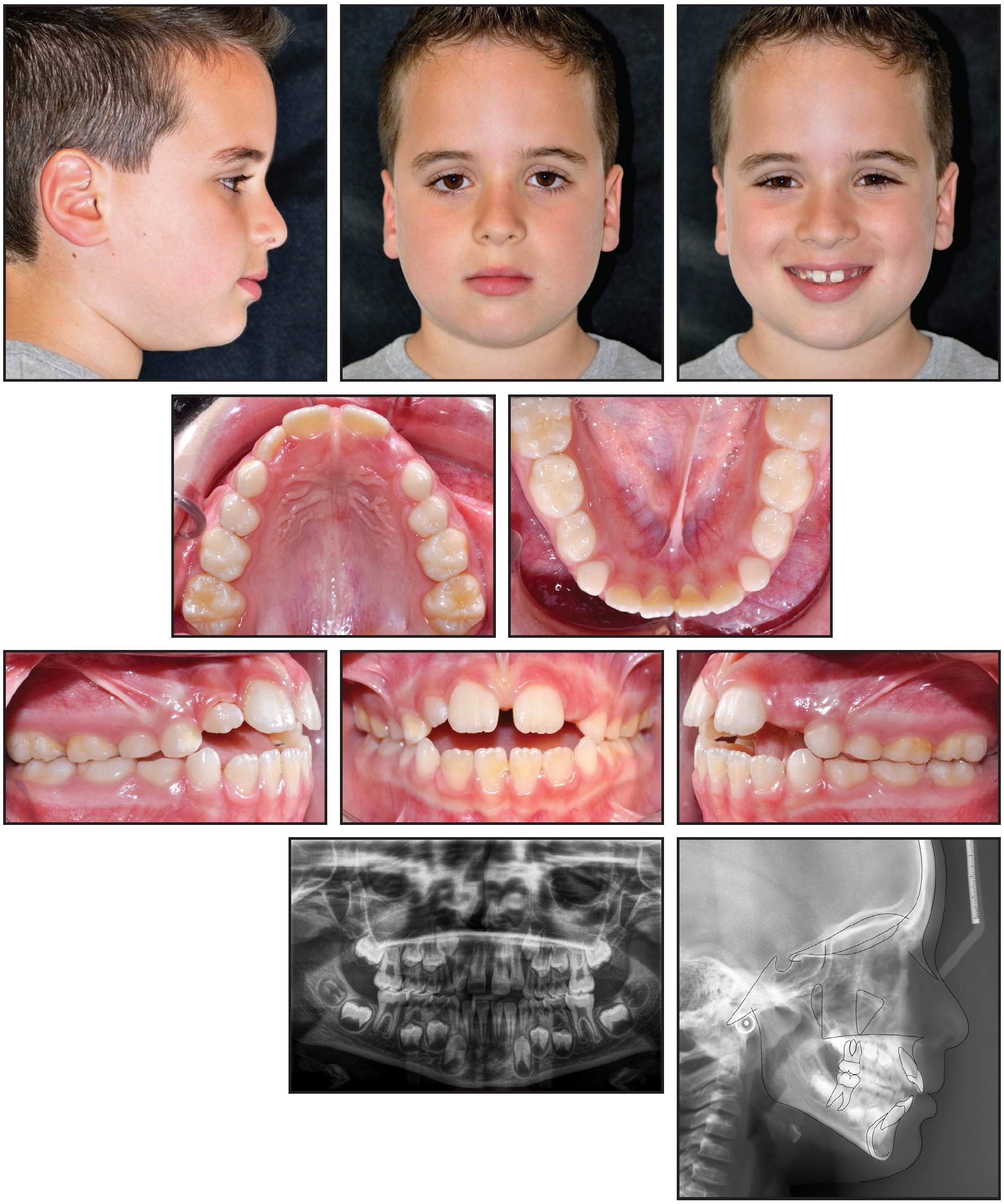
Fig. 1 Case 1. 8-year-old male patient with Class I molar relationship, Class II sagittal skeletal relationship, severe anterior open bite, and hyperdivergent growth pattern before treatment.
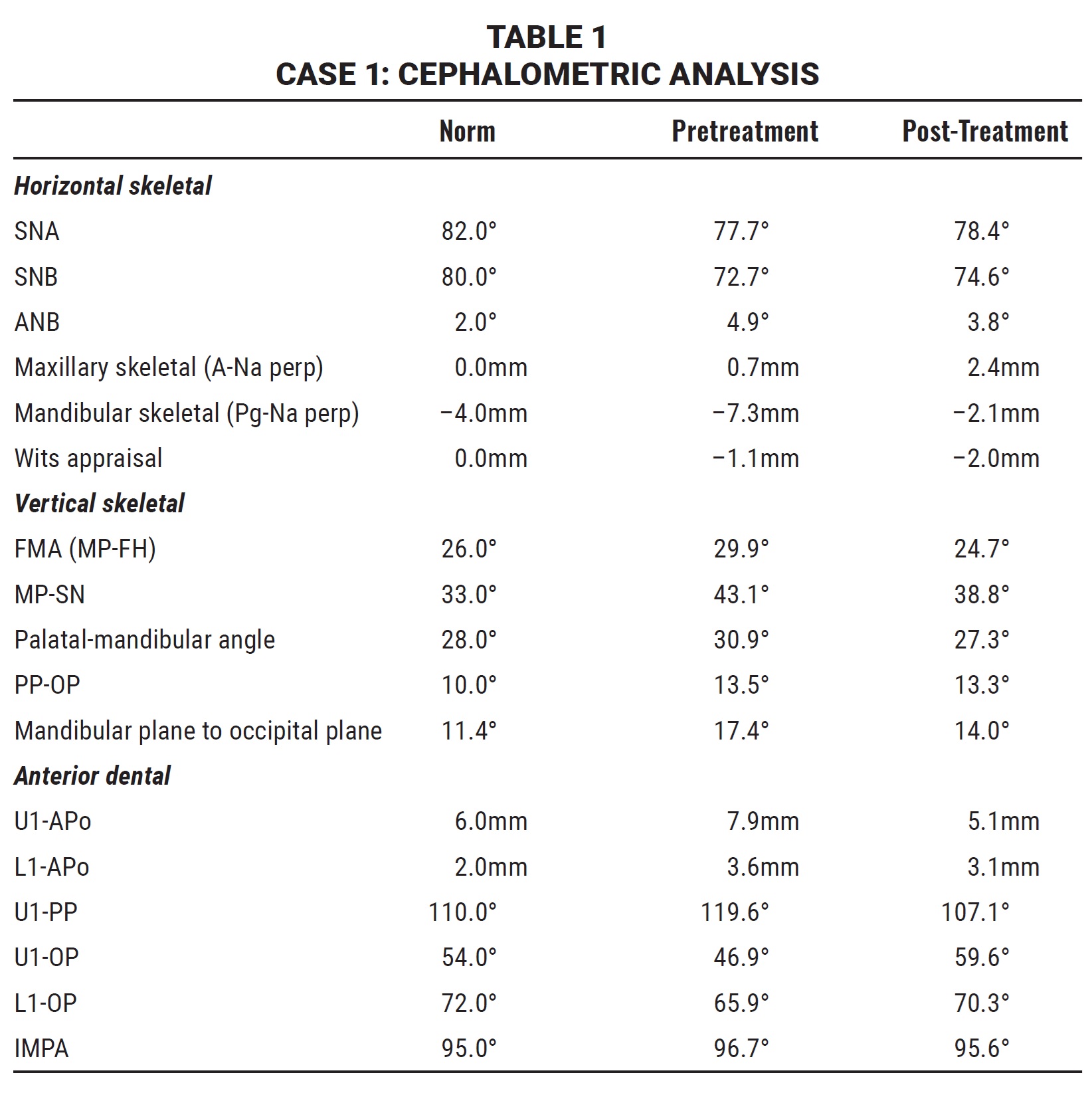
The panoramic radiograph revealed the presence of all permanent teeth in the proper stages of eruption. Cephalometric analysis (Table 1) found a hyperdivergent growth pattern (FMA = 29.9°), caused by a retrusive mandible, and a skeletal Class II relationship (ANB = 4.9°). As would be expected, the maxillary incisors were excessively tipped forward (U1-PP = 119.6°), while the mandibular incisors were normally inclined (IMPA = 96.7°). The patient was in Cervical Stage 2 (CS2) of skeletal development, indicating that the pubertal growth spurt would occur at least a year later.8 The periodontal biotype was thick, with no gingival recession.
Interceptive treatment was planned to interrupt the tongue-thrust habit, allowing the teeth to reestablish normal eruption. Treatment objectives were to correct the anterior open bite, achieve ideal overbite and overjet, resolve the transverse arch discrepancy, and achieve a skeletal Class I relationship.
An RPE with posterior bite blocks was bonded to correct the transverse maxillary deficiency and control the vertical dimension (Fig. 2). After discussing with the parents the importance of correcting the patient’s oral habits at an early age, we decided to add a fixed tongue crib to the RPE. The expansion protocol involved one activation of .2mm per day for 20 days, which would provide an overcorrection to counteract any minor skeletal relapse.9 The wire of the tongue crib was flexible enough to expand with the palate.
After six months of passive stabilization, the RPE and tongue crib were removed. Reevaluation of the case was postponed for 18 months, until all permanent teeth were present in both arches, except for the second and third molars. Intraoral examination at this time showed a normal transverse maxillary dimension, ideal overjet and overbite, and a Class I molar relationship (Fig. 3).
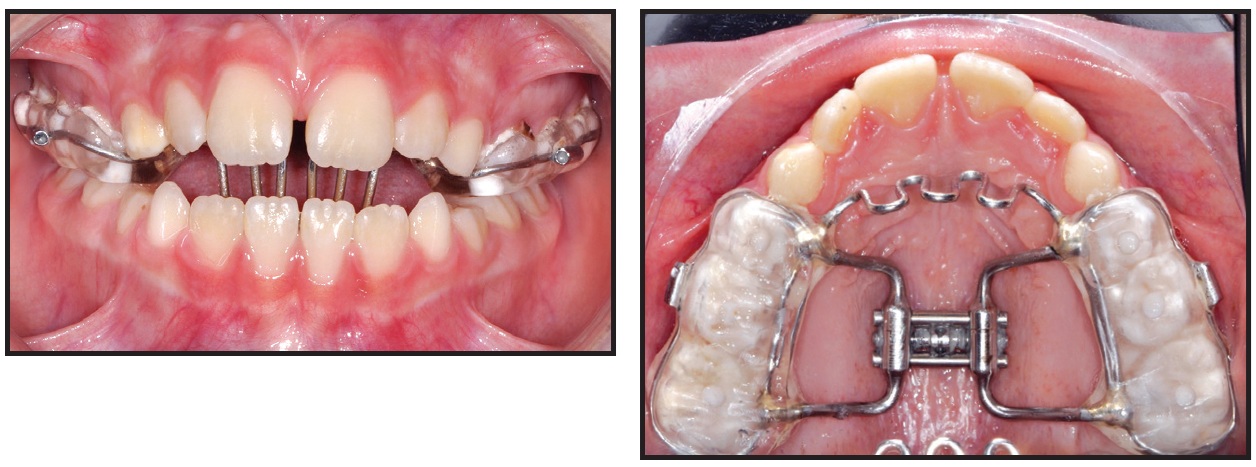
Fig. 2 Case 1. Rapid palatal expander (RPE) with posterior bite blocks and fixed tongue crib.

Fig. 3 Case 1. Case reevaluation after 20 days of active expansion, six months of passive stabilization, and 18 months of observation.
After the successful first phase of treatment, we decided to use F22* aligners to refine the alignment and coordinate the arches. Ten sets of aligners were planned, to be changed every two weeks (Fig. 4). Composite grip points were bonded to the buccal surfaces of the upper canines, first premolars, and second premolars, and to the lingual surfaces of the upper right lateral and lower right central incisor, as prescribed by the virtual setup. Interproximal reduction (IPR) was also performed. The aligner phase lasted five months (Fig. 5).
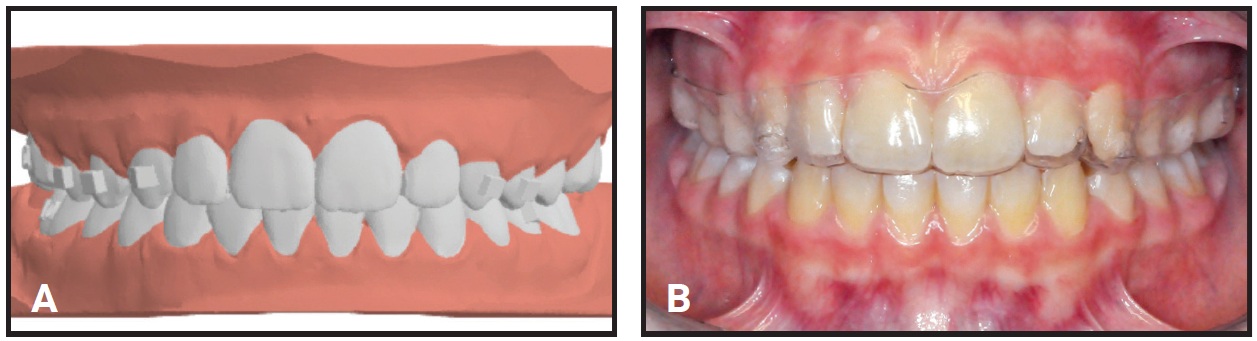
Fig. 4 Case 1. A. Virtual setup for treatment with F22* aligners. B. Phase II treatment using 10 sets of aligners, changed every two weeks.
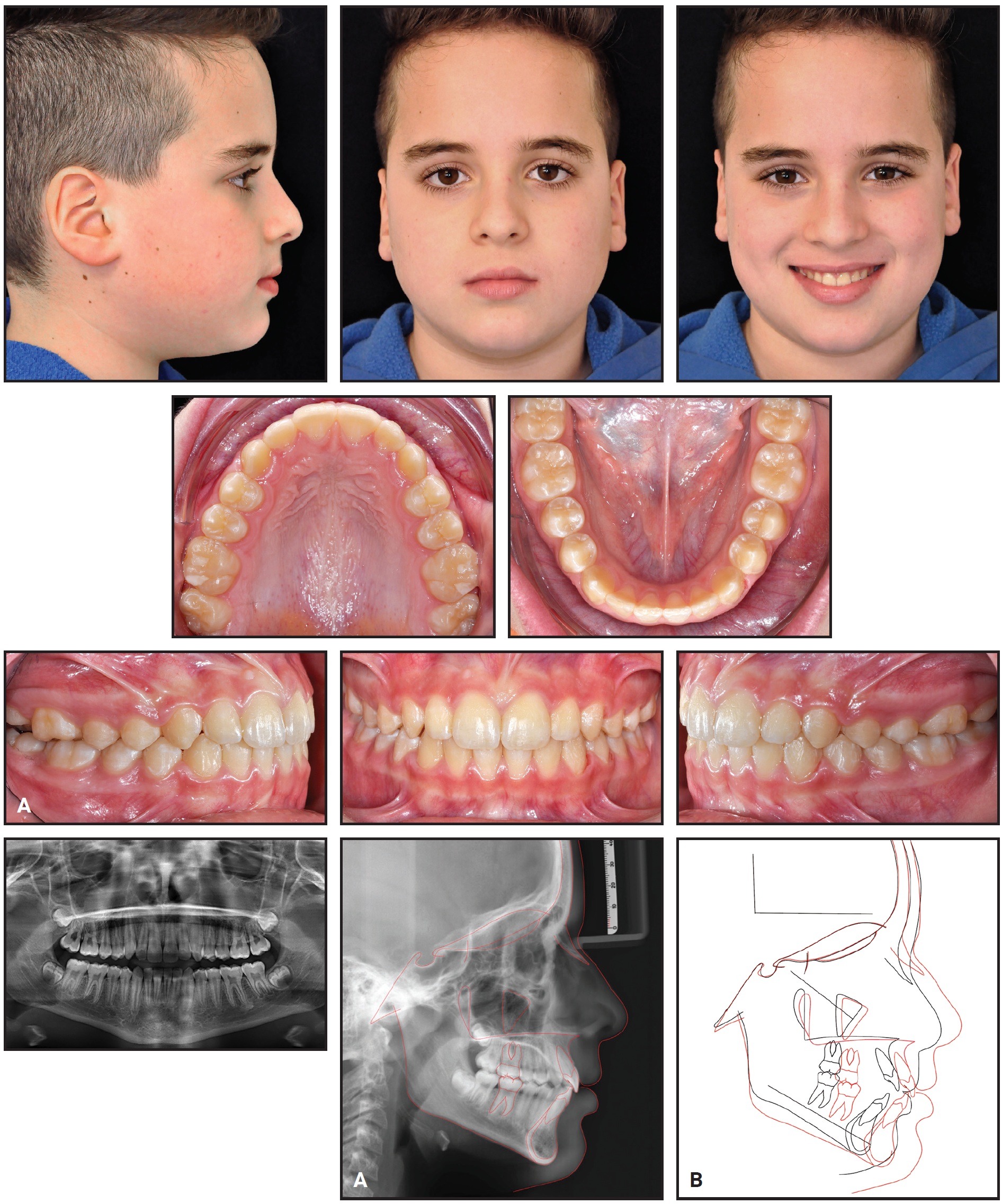
Fig. 5 Case 1. A. Patient after five months of aligner treatment. B. Superimposition of pre- and post-treatment cephalometric tracings.
Post-treatment records demonstrated an esthetic profile, proper incisor display in smiling, bilateral Class I molar and canine relationships, well-aligned dental arches, and normal overjet and overbite. Panoramic radiography showed good root parallelism, no sign of crestal bone-height reduction, and no evidence of apical root resorption. All four third-molar buds were present. Cephalometric analysis confirmed a Class I skeletal relationship (ANB = 3.8°) with a slight improvement in the mandibular position, probably due to residual growth (Table 1). The inclination of the upper incisors was greatly improved (107.1°). Superimposition of cephalometric tracings10,11 highlighted a normal mandibular growth pattern with a predominantly forward direction. There was no worsening of the vertical dimension, indicating effective vertical control during the aligner phase.
Case 2
A 7-year-old female presented for treatment with a well-proportioned face, a minor deviation of the mandibular symphysis toward the right, a mildly protrusive mandible, and a normal nasolabial angle (Fig. 6). The upper midline seemed to be coincident with the facial midline, but the lower midline deviated slightly to the right. Intraoral examination showed that the patient was in the first phase of the transitional dentition, with a Class I molar relationship, transverse maxillary constriction, negative overbite, and accentuated curves of Wilson. A prolonged tongue-thrust habit had contributed to the development of a severe anterior open bite.
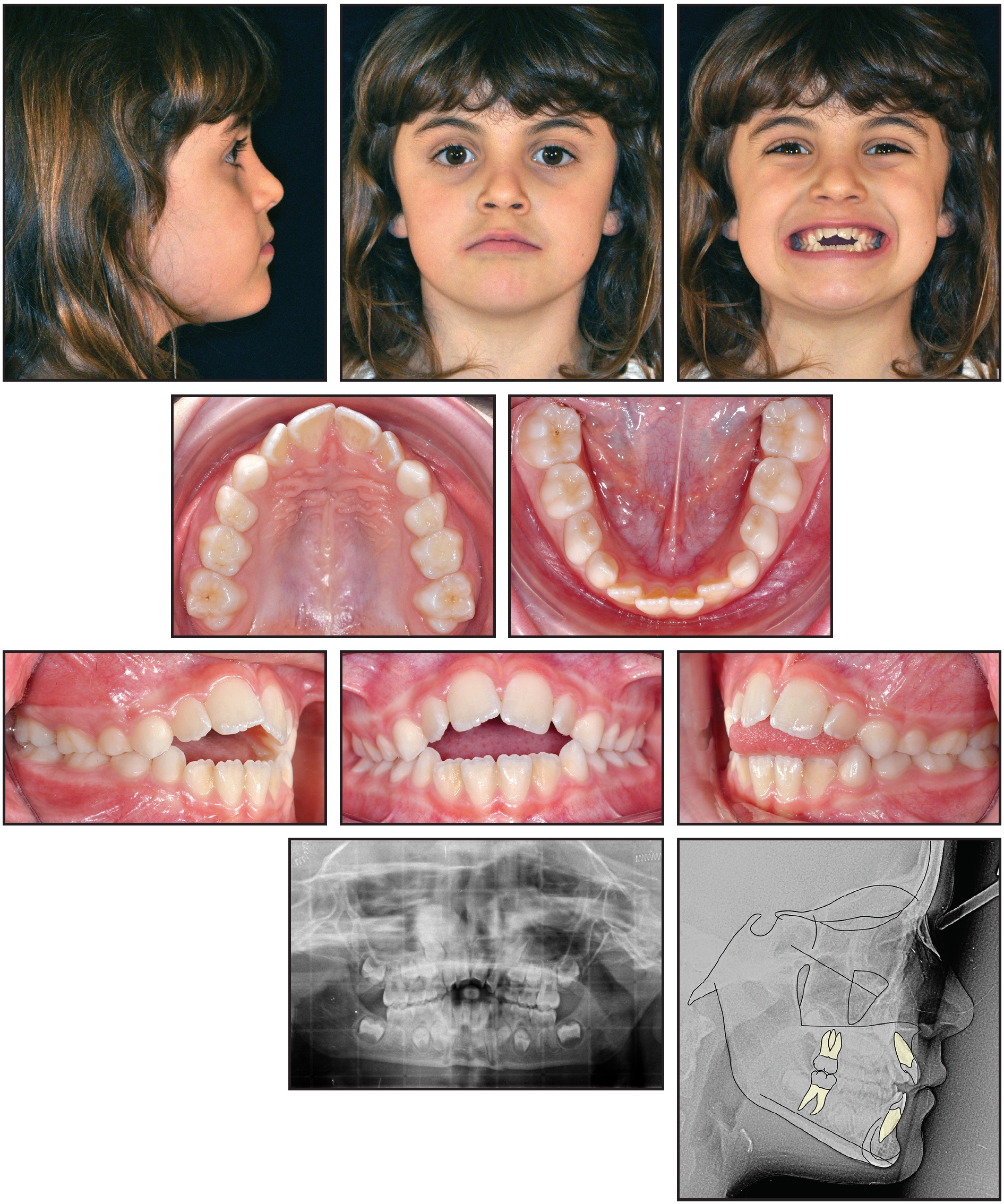
Fig. 6 Case 2. 7-year-old female patient with Class I molar relationship, Class I sagittal skeletal relationship, severe anterior open bite, and hypodivergent growth pattern before treatment.
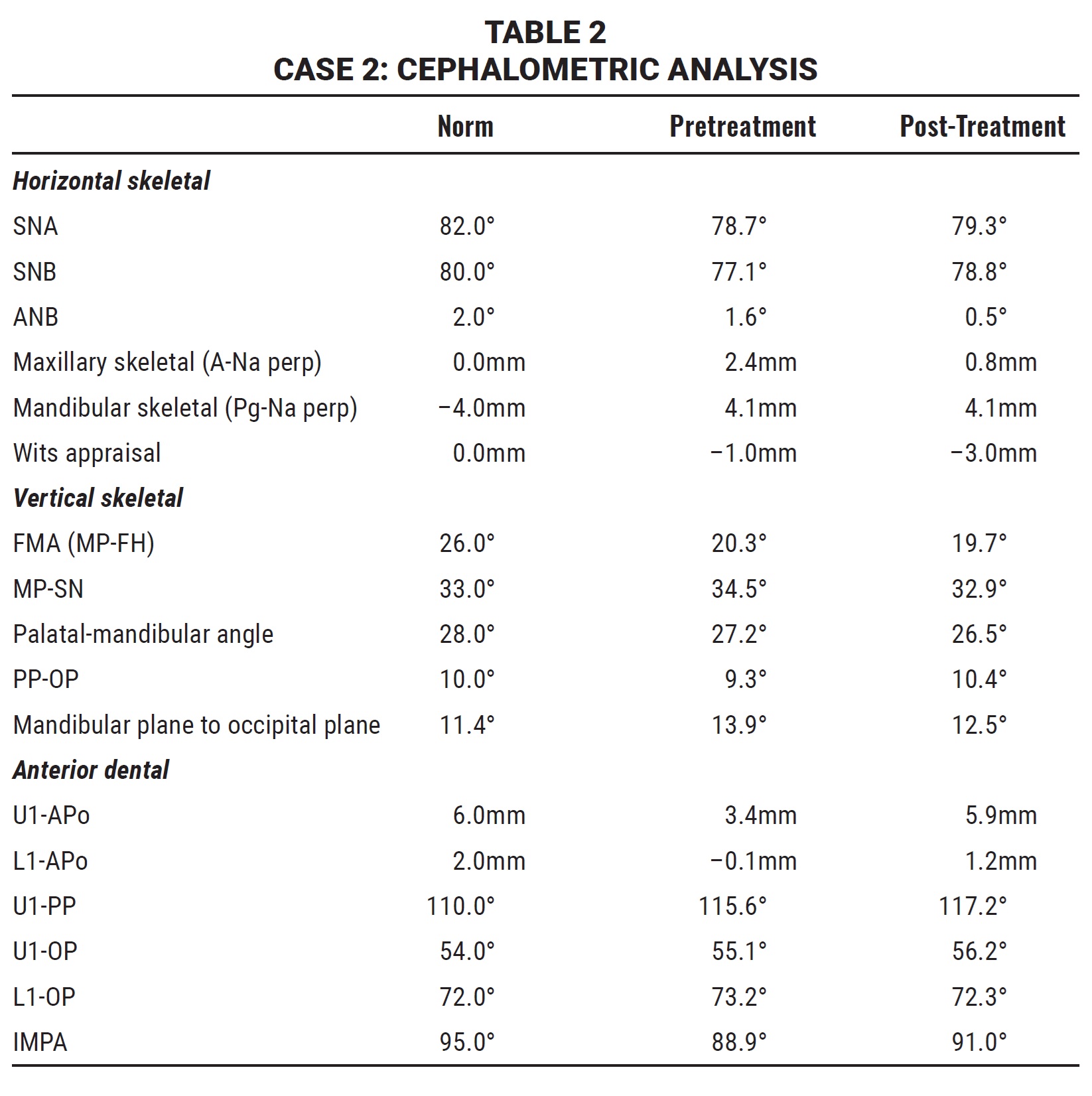
The panoramic radiograph indicated the presence of all permanent teeth in the proper stages of eruption. According to the cephalometric analysis (Table 2), the patient had a hypodivergent growth pattern (FMA = 20.3°) and a Class I sagittal skeletal relationship (ANB = 1.6°). The maxillary incisors were slightly tipped forward (U1-PP = 115.6°), while the mandibular incisors were normally inclined (IMPA = 88.9°). The patient was in stage CS2 of skeletal development, so that the pubertal growth spurt would be expected to occur in no less than one year.8 The periodontal biotype was thick, with no gingival recession.
Interceptive treatment was planned to interrupt the tongue-thrusting habit, allowing the teeth to resume normal eruption. Objectives were to achieve ideal overbite and overjet, correct the transverse arch discrepancy, and obtain a skeletal Class I relationship.
An RPE with a fixed tongue crib was bonded and a lower removable plate was delivered to correct the transverse maxillary deficiency, normalize the curves of Wilson, and control the vertical dimension (Fig. 7). The expansion protocol included one activation of .2mm per day for 34 days, thus providing an overcorrection to counteract minor skeletal relapse.9
The appliance was removed after six months of passive stabilization. A reevaluation was postponed for 20 months, until all permanent teeth were present in both arches, except for the second and third molars. Intraoral examination then showed a normal transverse maxillary dimension, ideal overjet and overbite, and Class I molar relationships (Fig. 8).
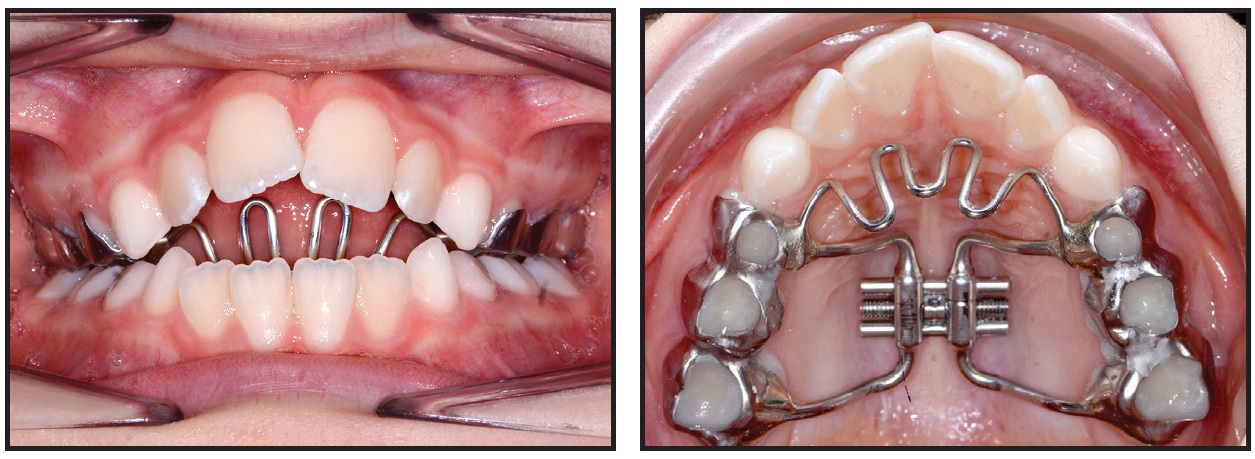
Fig. 7 Case 2. RPE with fixed tongue crib.
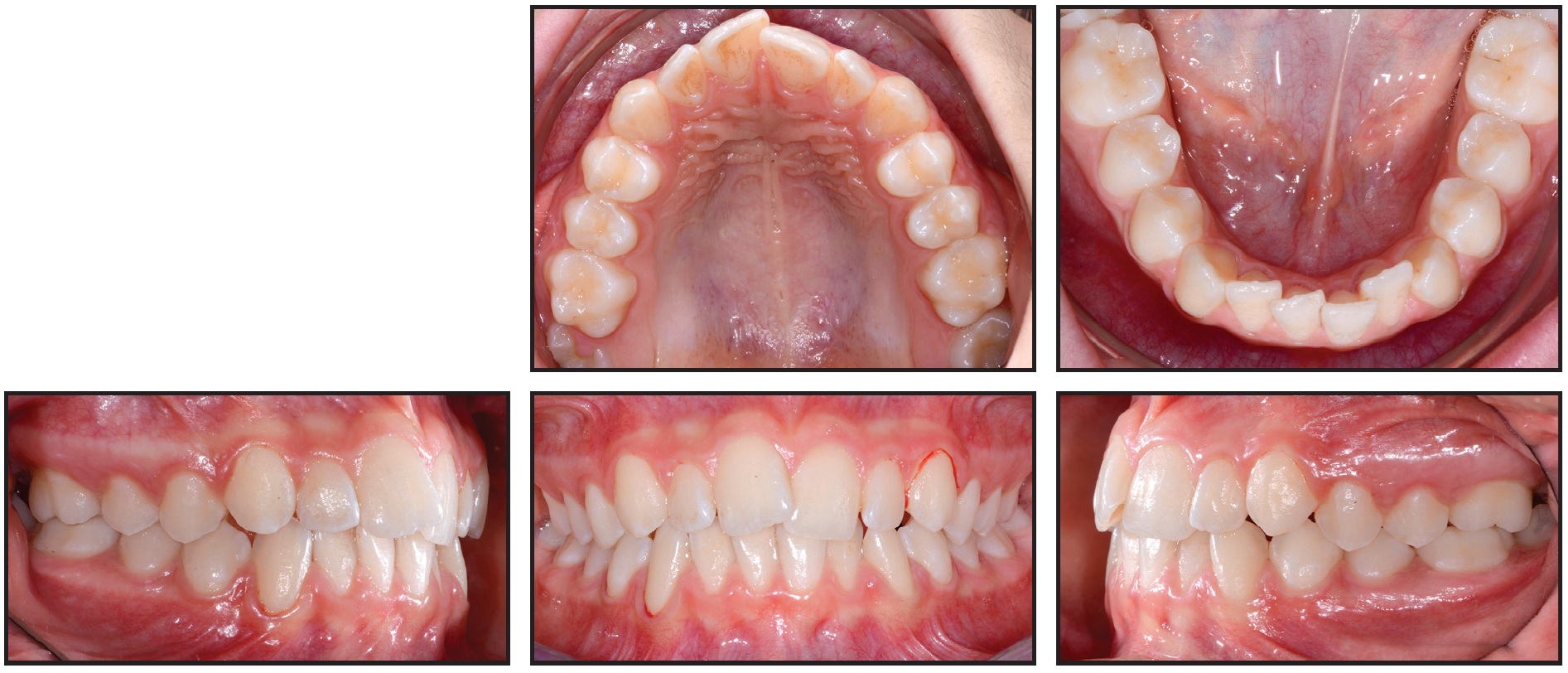
Fig. 8 Case 2. Case reevaluation after 34 days of active expansion, six months of passive stabilization, and 20 months of observation.
After the successful first phase, a second phase of orthodontic treatment was planned using F22 aligners to refine the alignment and coordinate the arches. Twelve sets of aligners were delivered, to be changed every two weeks (Fig. 9). Composite grip points were bonded to the buccal surfaces of the upper right first molar and lower right first premolar, as prescribed by the virtual setup, and IPR was also performed. The aligner phase lasted six months (Fig. 10).
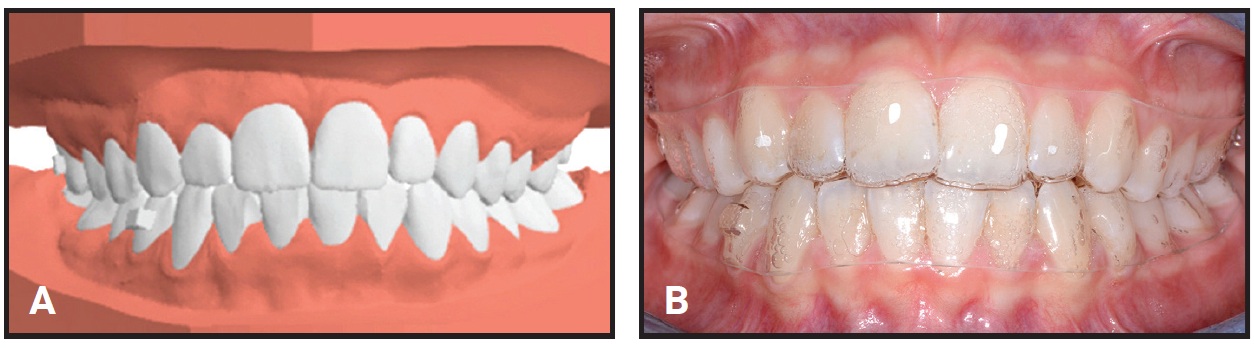
Fig. 9 Case 2. A. Virtual setup for treatment with F22 aligners. B. Phase II treatment using 12 sets of aligners, changed every two weeks.
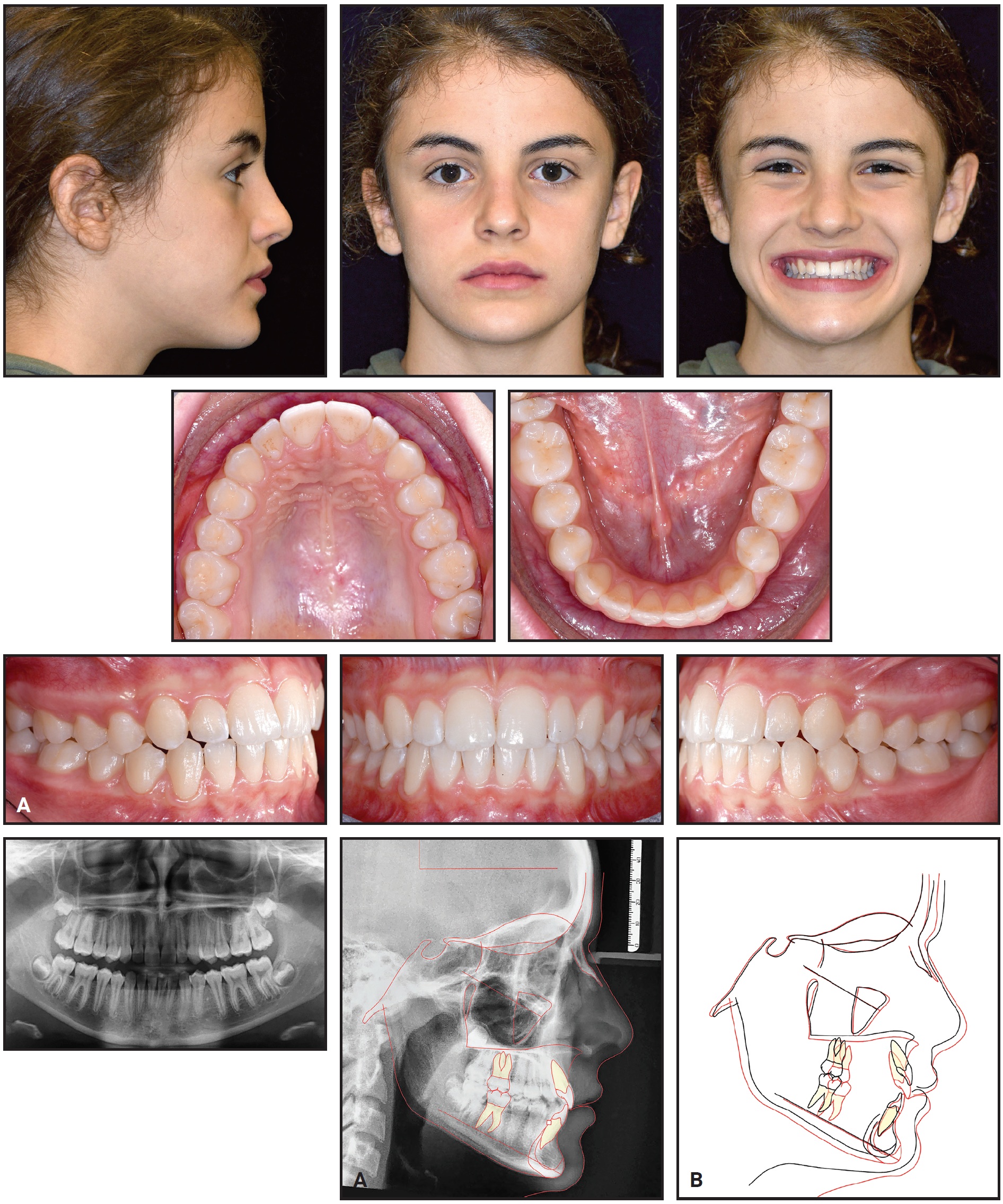
Fig. 10 Case 2. A. Patient after six months of aligner treatment. B. Superimposition of pre- and post-treatment cephalometric tracings.
Final records confirmed the achievement of a pleasant profile, proper incisor display in smiling, bilateral Class I molar and canine relationships, well-aligned dental arches, and ideal overjet and overbite. The post-treatment panoramic radiograph showed good root parallelism, no sign of crestal bone-height reduction, and no evidence of apical root resorption. Cephalometric analysis indicated a skeletal Class I relationship (ANB = .5°) with a slight Class III tendency (Table 2). The inclinations of the upper and lower incisors were normalized (U1-PP = 117.2°, IMPA = 91°).
Discussion
Proposed options for early treatment of anterior open bite all have the goal of eliminating mechanical factors that can perpetuate the open bite, such as thumbsucking or tongue thrusting, and that can promote excessive vertical growth of the mandible.7,12 Indeed, cephalometric investigations have found that anterior open bite is often associated with increased dentoalveolar and skeletal vertical dimensions.13 If the situation is not addressed early, orthognathic surgery may be the only alternative.
The treatment approaches shown here differed slightly because of the two patients’ opposite skeletal patterns. Maxillary expansion must be performed carefully in the presence of an anterior open bite, since the RPE tends to promote posterior mandibular rotation. In the first case, because of the patient’s hyperdivergent growth pattern, a posterior bite block was added. Superimposition of pre- and post-treatment cephalometric tracings showed good vertical control and a predominantly forward mandibular growth pattern, confirming that any side effects of the RPE are reversible and should not prevent its use in open-bite patients.14 The combination of RPE and posterior bite blocks has proven effective in correcting negative overbite in growing patients, producing a significant improvement in the vertical skeletal pattern thanks to the control of molar extrusion, along with lingual tipping of the incisors.15,16 Vertical control is one of the most important aspects of open-bite treatment, but pure molar intrusion is difficult to achieve with fixed orthodontic appliances.17
Because the tongue’s anterior resting position plays a causative role in the relapse of anterior open bite, the fixed tongue crib was maintained in each of these cases until the end of the first treatment phase. As expected, the tongue crib altered the anterior resting position and thus permitted normal eruption of the incisors.18 Although the addition of a tongue crib creates some initial discomfort, this approach is more effective than removable devices in correcting anterior open bite, since it does not require patient compliance.19
In each case, the second phase of treatment was carried out using clear aligners, which satisfied the esthetic demands of the young patient. Given appropriate diagnosis, clear aligners can be effective in mild to moderate cases, allowing shorter treatment with less chairtime compared to conventional fixed appliances.20,21 After our interceptive phase resolved the orthopedic problems and permitted normal eruption of the permanent dentition,22,23 the aligner phase then had only to level and coordinate the dental arches and correct any tooth rotations. The digital setup produced highly predictable tooth movements, including crown tipping for optimal light anterior contact and solid posterior occlusion.24
A limitation of this case series is the absence of long-term follow-up, considering that some relapse has been associated with nonsurgical treatment of anterior open bites.25
FOOTNOTES
- *Registered trademark of Sweden & Martina Inc., Du Carrare, Padua, Italy; www.sweden-martinainc.com.
REFERENCES
- 1. Subtelny, J.D. and Sakuda, M.: Open-bite: Diagnosis and treatment, Am. J. Orthod. 50:337-358, 1964.
- 2. Kasparaviciene, K.; Sidlauskas, A.; Zasciurinskiene, E.; Vasiliauskas, A.; Juodzbalys, G.; Sidlauskas, M.; and Marmaite, U.: The prevalence of malocclusion and oral habits among 5-7-year-old children, Med. Sci. Monit. 20:2036-2042, 2014.
- 3. Tausche, E.; Luck, O.; and Harzer, W.: Prevalence of malocclusions in the early mixed dentition and orthodontic treatment need, Eur. J. Orthod. 26:237-244, 2004.
- 4. Silvestrini-Biavati, A.; Salamone, S.; Silvestrini-Biavati, F.; Agostino, P.; and Ugolini, A.: Anterior open-bite and sucking habits in Italian preschool children, Eur. J. Paediat. Dent. 17:43-46, 2016.
- 5. Cozza, P.; Baccetti, T.; Franchi, L.; Mucedero, M.; and Polimeni, A.: Sucking habits and facial hyperdivergency as risk factors for anterior open bite in the mixed dentition, Am. J. Orthod. 128:517-519, 2005.
- 6. Phelan, A.; Franchi, L.; Baccetti, T.; Darendeliler, M.A.; and McNamara, J.A. Jr.: Longitudinal growth changes in subjects with open-bite tendency: A retrospective study, Am. J. Orthod. 145:28-35, 2014.
- 7. Pisani, L.; Bonaccorso, L.; Fastuca, R.; Spena, R.; Lombardo, L.; and Caprioglio, A.: Systematic review for orthodontic and orthopedic treatments for anterior open bite in the mixed dentition, Prog. Orthod. 17:28, 2016.
- 8. Baccetti, T.; Franchi, L.; and McNamara, J.A. Jr.: The cervical vertebral maturation (CVM) method for the assessment of optimal treatment timing in dentofacial orthopedics, Semin. Orthod. 11:119-129, 2005.
- 9. Cannavale, R.; Chiodini, P.; Perillo, L.; and Piancino, M.G.: Rapid palatal expansion (RPE): Meta-analysis of long-term effects, Orthod. Craniofac. Res. 21:225-235, 2018.
- 10. Björk, A. and Skieller, V.: Growth of the maxilla in three dimensions as revealed radiographically by the implant method, Br. J. Orthod. 4:53-64, 1977.
- 11. Björk, A.: Prediction of mandibular growth rotation, Am. J. Orthod. 55:585-599, 1969.
- 12. Cangialosi, T.J.: Skeletal morphologic features of anterior open bite, Am. J. Orthod. 85:28-36, 1984.
- 13. Zecca, P.A.; Fastuca, R.; Beretta, M.; Caprioglio, A.; and Macchi, A.: Correlation assessment between three-dimensional facial soft tissue scan and lateral cephalometric radiography in orthodontic diagnosis, Int. J. Dent. 2016:1473918, 2016.
- 14. Bishara, S.E. and Staley, R.N.: Maxillary expansion: Clinical implications, Am. J. Orthod. 91:3-14, 1987.
- 15. Mucedero, M.; Fusaroli, D.; Franchi, L.; Pavoni, C.; Cozza, P.; and Lione, R.: Long-term evaluation of rapid maxillary expansion and bite-block therapy in open bite growing subjects: A controlled clinical study, Angle. Orthod. 88:523-529, 2018.
- 16. Turkkahraman, H. and Cetin, E.: Comparison of two treatment strategies for the early treatment of an anterior skeletal open bite: Posterior bite block-vertical pull chin cup (PBB-VPC) vs. posterior bite block-high pull headgear (PBB-HPH), J. Orofac. Orthop. 78:338-347, 2017.
- 17. Guarneri, M.P.; Oliverio, T.; Silvestre, I.; Lombardo, L.; and Siciliani, G.: Open bite treatment using clear aligners, Angle. Orthod. 83:913-919, 2013.
- 18. Smithpeter, J. and Covell, D. Jr.: Relapse of anterior open bites treated with orthodontic appliances with and without orofacial myofunctional therapy, Am. J. Orthod. 137:605-614, 2010.
- 19. Giuntini, V.; Franchi, L.; Baccetti, T.; Mucedero, M.; and Cozza, P.: Dentoskeletal changes associated with fixed and removable appliances with a crib in open-bite patients in the mixed dentition, Am. J. Orthod. 133:77-80, 2008.
- 20. Zheng, M.; Liu, R.; Ni, Z.; and Yu, Z.: Efficiency, effectiveness and treatment stability of clear aligners: A systematic review and meta-analysis, Orthod. Craniofac. Res. 20:127-133, 2017.
- 21. Robertson, L.; Kaur, H.; Fagundes, N.C.F.; Romanyk, D.; Major, P.; and Flores Mir, C.: Effectiveness of clear aligner therapy for orthodontic treatment: A systematic review, Orthod. Craniofac. Res. 23:133-142, 2020.
- 22. Lombardo, L.; Palone, M.; Carlucci, A.; and Siciliani, G.: Clear aligner hybrid approach: A case report, J. World Fed. Orthod. 9:32-43, 2020.
- 23. Lombardo, L.; Albertini, P.; Cervinara, F.; Brucculeri, L.; and Siciliani, G.: Early Class III treatment with hybrid rapid palatal expander combined with facemask, Int. Orthod. 18:624-635, 2020.
- 24. Lombardo, L.; Arreghini, A.; Ramina, F.; Huanca Ghislanzoni, L.T.; and Siciliani, G.: Predictability of orthodontic movement with orthodontic aligners: A retrospective study, Prog. Orthod. 18:35, 2017.
- 25. Greenlee, G.M.; Huang, G.J.; Chen, S.S.; Chen, J.; Koepsell, T.; and Hujoel, P.: Stability of treatment for anterior open-bite malocclusion: A meta-analysis, Am. J. Orthod. 139:154-169, 2011.
-
 DR. LOMBARDO
DR. LOMBARDO -
 DR. CARLUCCI
DR. CARLUCCI -
 DR. ALBERTINI
DR. ALBERTINI -
 DR. CREMONINI
DR. CREMONINI -
 DR. SICILIANI
DR. SICILIANI
Dr. Lombardo is a Professor and Chairman, Drs. Carlucci and Cremonini are Research Assistants, and Dr. Albertini is a Research Fellow, Postgraduate School of Orthodontics; and Dr. Siciliani is Chairman, School of Dentistry, University of Ferrara, Via Luigi Borsari 46, 44121 Ferrara, Italy. E-mail Dr. Cremonini at dr.ssafrancescacremonini@gmail.com.
