CASE REPORT
Resolution of a Complex Malocclusion Using a Hybrid Aligner Approach
Clear aligner therapy is often the treatment of choice in today’s orthodontic practice, especially for nonextraction cases of mild to moderate difficulty.1 Aligners offer optimal esthetic properties and patient comfort, making them particularly suitable for adults.2 In addition, because they are removable, they are less likely to impact periodontal health.3
Although diagnostic indications for clear aligner therapy have broadened, some orthodontic movements remain unpredictable, even with good treatment planning.4 Extrusion, intrusion, bodily movements, torque, and substantial rotations of rounded teeth are difficult to manage using clear aligners alone,5 making them less efficient than conventional biomechanics in complex treatment.6 Extrusion or rotation auxiliaries or interarch elastics are therefore often needed.7,8 Another approach is to use partial or full fixed appliances to correct the most critical problems before or during clear aligner therapy.9
One such problem, scissor bite, is an alteration in the normal relationship between the cusps and fossae of antagonistic teeth. Although the incidence of scissor bite is rare—1.1% of the children investigated in one study10—it can create issues with masticatory function and growth patterns in prepubertal patients due to functional displacement of the lower jaw.11 Since there are discrepancies in both the vertical and buccopalatal dimensions, a scissor bite is difficult to correct using only clear aligners.11
Orthodontic miniscrews have made it possible to resolve complex anomalies such as scissor bite without loss of anchorage.12,13 Miniscrews are safe, inexpensive, and minimally invasive and have a wide range of clinical applications, owing to their small size and ease of placement and removal.
This report shows a patient with a unilateral scissor bite of the upper and lower right second molars who was treated using a hybrid approach—involving clear aligners and fixed buccal sectional appliances with miniscrew anchorage—after aligners alone failed to achieve the planned outcome.
Similar articles from the archive:
- A Miniscrew-Supported Intrusion Auxiliary for Open-Bite Treatment with Invisalign June 2014
- Treatment of Challenging Malocclusions with Invisalign and Miniscrew Anchorage January 2014
- Maxillary Space Closure Using Aligners and Palatal Mini-Implants in Patients with Congenitally Missing Lateral Incisors January 2021
Diagnosis and Treatment Plan
A 27-year-old female presented with the chief complaint of unsightly front teeth and traumatic biting in the right posterior cheek region (Fig. 1A).

Fig. 1 27-year-old female patient with borderline Class I molar and canine relationships, moderate crowding in both arches, and scissor bite involving upper and lower right second molars before treatment (continued in next image).
Extraoral analysis found a convex profile, a long lower third of the face, and lip strain from the attempt to achieve lip competence. The patient had a gummy smile with complete incisor exposure, bilateral buccal black corridors, and a slight occlusal cant. She had borderline Class I molar and canine relationships with excessive overbite and overjet. The lower midline was deviated 1mm to the left of the upper midline, and the curve of Spee was accentuated on both sides. Moderate crowding and malalignment were present in both arches. A scissor bite of the upper and lower second molars was observed on the right side (Fig 1B).
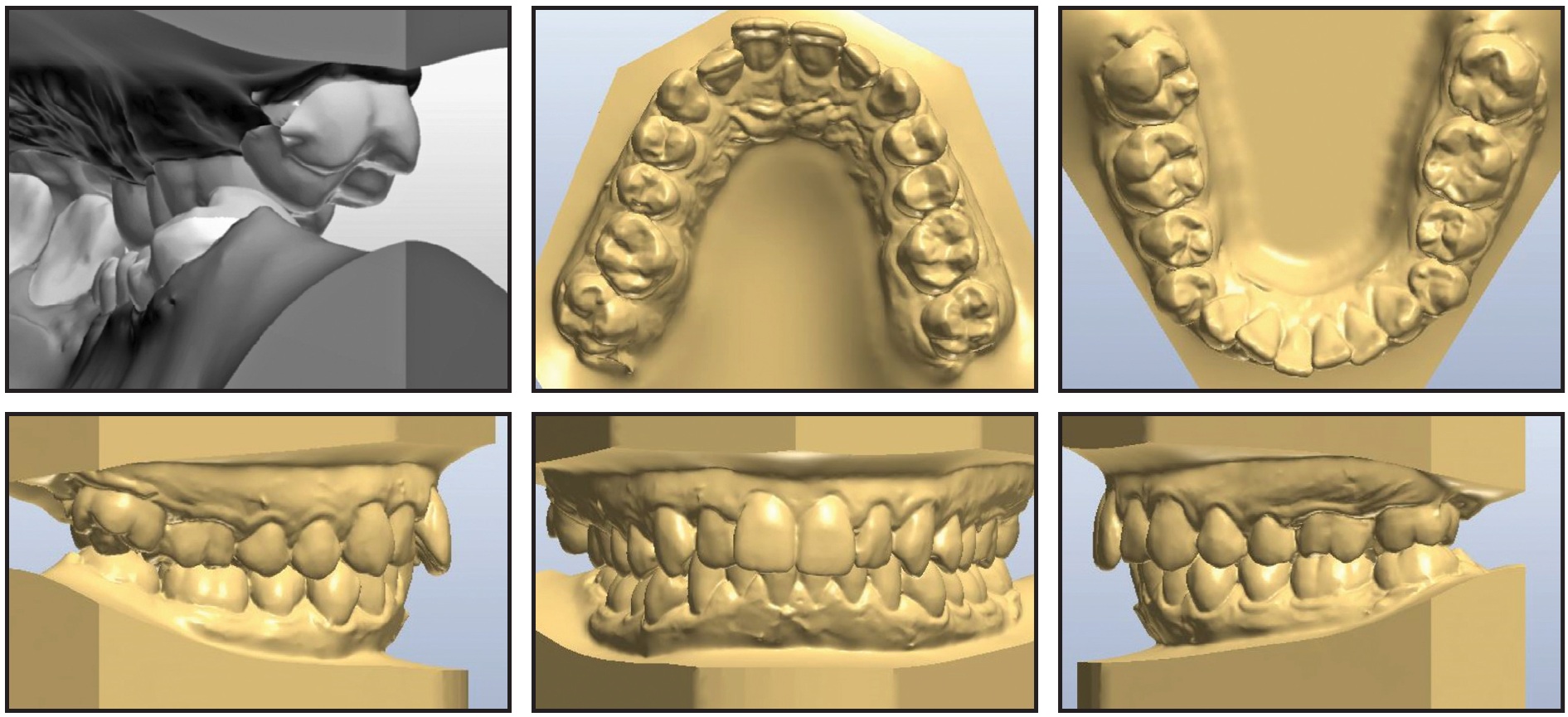
Fig. 1 (cont.) 27-year-old female patient with borderline Class I molar and canine relationships, moderate crowding in both arches, and scissor bite involving upper and lower right second molars before treatment.
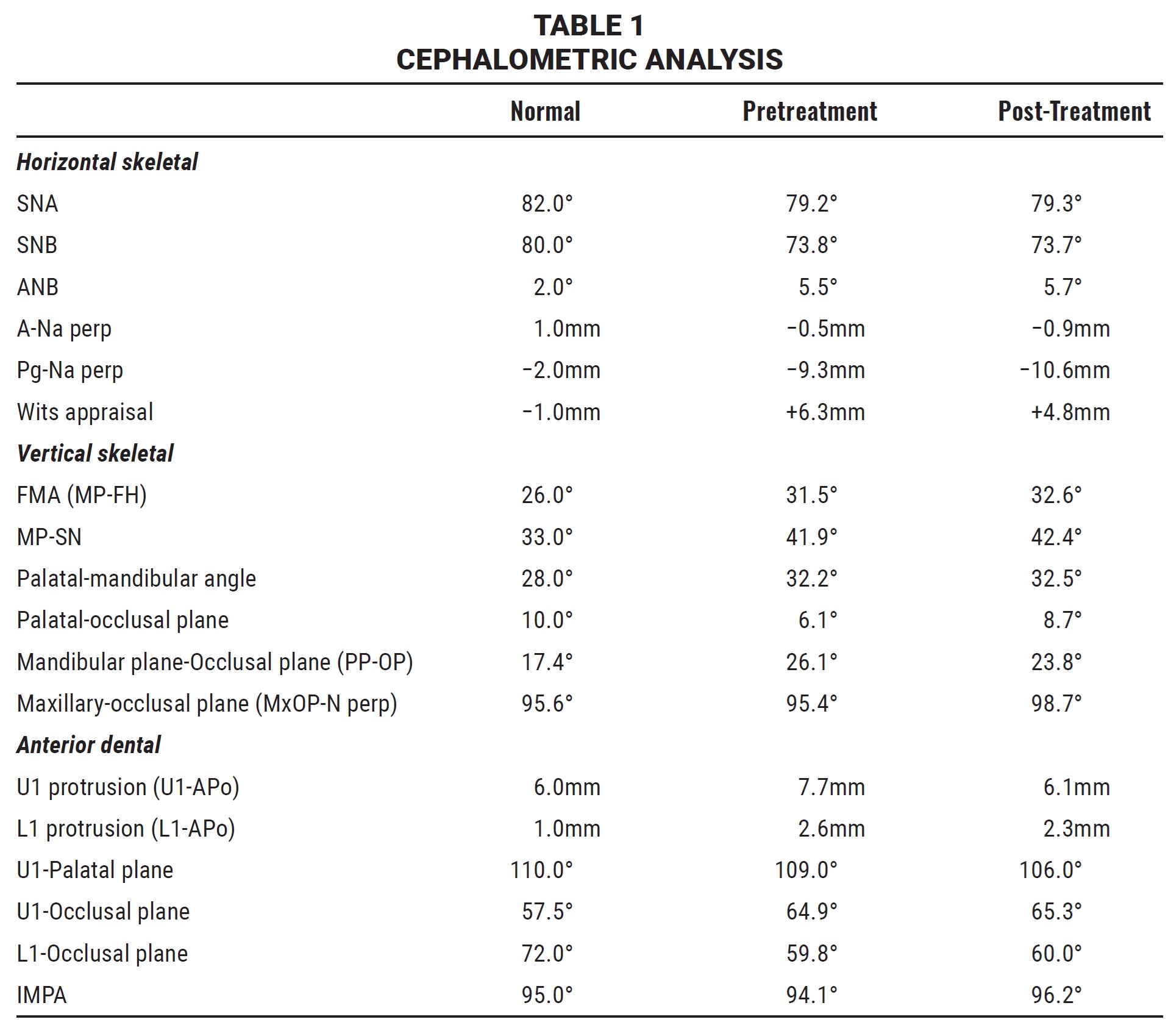
The patient did not report any TMJ symptomatology, as confirmed by the clinical and functional exam. All teeth were present on the panoramic radiograph. Cephalometric analysis (Table 1) indicated a moderate biretrusive skeletal Class II (ANB = 5.5°) with a primarily mandibular component (SNB = 73.8°) and a hyperdivergent pattern (FMA = 31.5°). Upper and lower incisor inclinations seemed to be normal.
The main treatment objectives were to maintain the bilateral Class I molar and canine relationships, resolve the malalignment and crowding in both arches, reduce gingival exposure in smiling, center the midlines, and improve lip competence. An additional objective was to correct the scissor bite and resolve the traumatic biting issue in the right cheek region.
Because the patient requested esthetic treatment, conventional fixed labial appliances were not considered. We evaluated the possibility of using lingual appliances, but the marked lingual inclination of the lower right second molar and the close contact between the buccal surface of the lower right second molar and the lingual surface of the upper right second molar would have hindered lingual bracket placement on these teeth. A lingual bracket on the upper right second molar would likely have been sheared off due to premature contact with the opposing arch. An alternative was to bond lingual brackets to all teeth except the upper and lower right second molars, where buccal tubes could be placed using the so-called “crossover technique.”14 Despite this viable option, the patient preferred an appliance that would be less invasive and more comfortable than a full lingual setup.
We therefore proposed an esthetic approach using clear aligner therapy. We recognized that the unilateral scissor bite would be more difficult to resolve because the posterior section of the aligner is more elastic, and it is therefore less suitable for delivering the orthodontic forces and moments necessary to resolve such a complex problem.
Treatment Progress
The patient was advised to have all four third molars extracted before orthodontic treatment. Digital models were then obtained from a CS 2600* intraoral scanner, and a digital setup was performed. The first phase of treatment involved a series of 12 individualized F22** clear aligners per arch (Fig. 2).
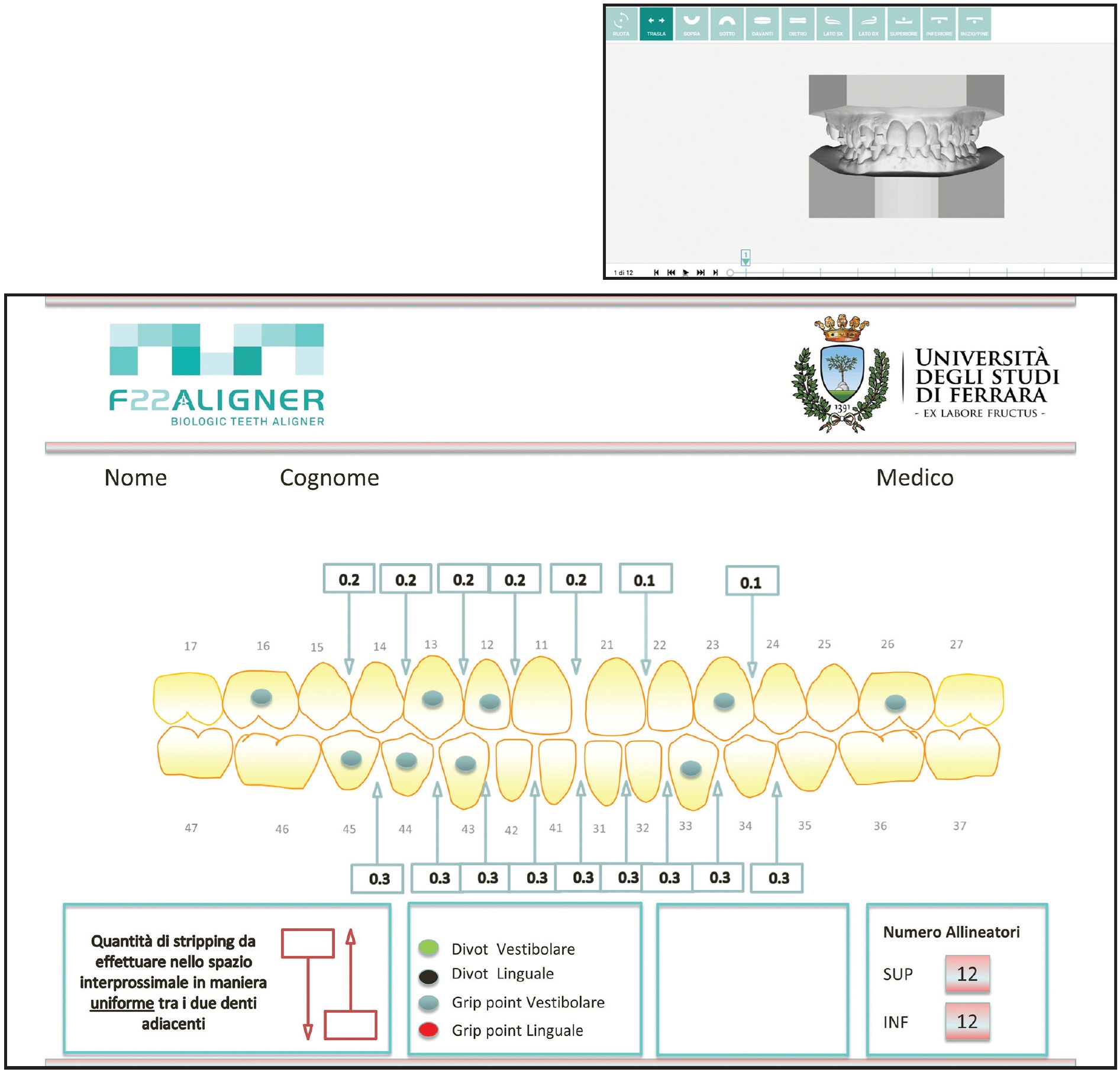
Fig. 2 Virtual setup for F22** aligners.
In the upper arch, grip points were positioned on the right first molar (8.8° distal rotation), left first molar (11.7° distal rotation), right canine (8.1° mesial rotation), left canine (15.9° mesial rotation), and right lateral incisor (.6mm extrusion). In the lower arch, grip points were placed at the left canine (10.6° mesial rotation), right canine (7.5° distal rotation), right first premolar (16.1° mesial rotation), and right second premolar (18.1° mesial rotation). The patient was instructed to wear each pair of aligners 22 hours per day for 15 days, removing them only for meals and brushing.
The patient was seen monthly to check progress and to perform the interproximal reduction (IPR) needed to facilitate the rotation and extrusion movements and resolve the crowding. The amount of IPR prescribed in the upper arch was .2mm from the mesial contact of the right second premolar to the mesial contact of the right central incisor, and .1mm at the contact points between the left central and lateral incisors and the left canine and first premolar. In the lower arch, .3mm of IPR was prescribed from the mesial contact of the left second premolar to the mesial contact of the right second premolar.
After two months of treatment, the scissor bite had not improved, and the patient complained of difficulty in fitting the aligners over the posterior regions of both arches (Fig. 3).

Fig. 3 Scissor bite unimproved after two months of treatment.
With the patient’s consent, we decided to cut off the remaining aligner trays on the right side in both arches and to end the first phase of therapy, postponing the correction of the scissor bite to the refinement stage. The patient was instructed to wear each pair of modified aligners for 10 days. This first treatment phase lasted four months and 20 days (Fig. 4). The crowding and malalignment were resolved, gingival exposure in smiling was reduced, and the midlines were partially centered.

Fig. 4 After four months and 20 days of treatment (end of first phase).
The aims of the second phase were to refine the occlusion and the alignment, fully center the midlines, and resolve the right posterior scissor bite. To improve the predictability and efficiency of the scissor-bite correction, a hybrid approach was planned using aligners with fixed buccal sectional appliances, orthodontic miniscrews, and criss-cross elastics. Brackets*** were bonded to the upper right first and second molars and the lower right first and second molars, and .016" × .022" nickel titanium wires† were placed (Fig. 5).
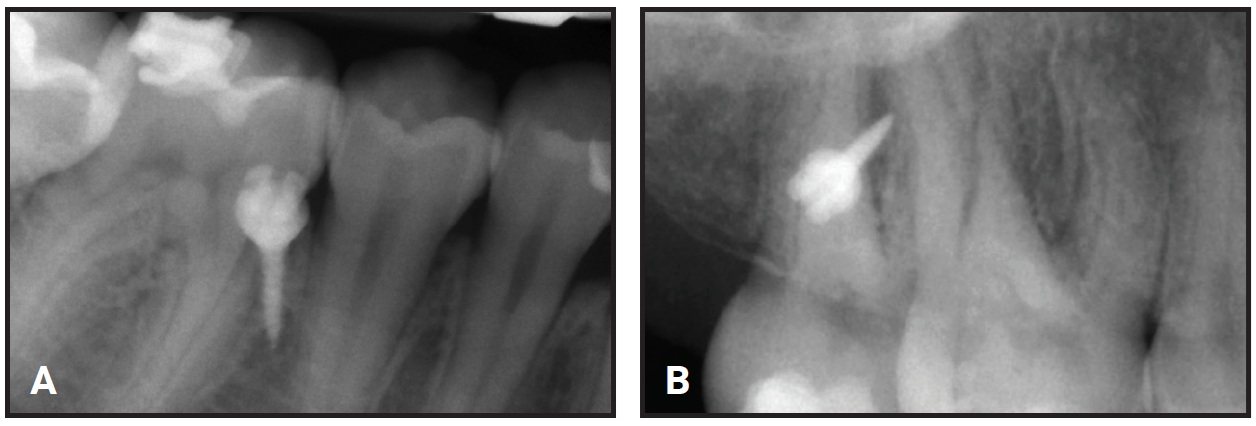
Fig. 5 A. Miniscrew‡ inserted in interradicular space between right second premolar and first molar. B. Miniscrew inserted in interradicular space between upper right first and second molars.
A 1.5mm × 8mm orthodontic miniscrew‡ was manually inserted into the buccal interradicular space between the lower right second premolar and first molar. An .017" × .025" stainless steel sectional wire† was attached from the screw head to the buccal surface of the lower right first molar to obtain indirect anchorage for buccal uprighting of the lower right second molar. Temporary bite turbos were built with light-cured flowable resin on the occlusal surfaces of the mandibular first molars to facilitate scissor-bite correction.
After the sectional appliances were placed, new intraoral scans were taken and a refinement setup was performed, involving eight trays in each arch. Before the refinement aligners were delivered, a 1.5mm × 8mm palatal miniscrew was inserted in the interradicular space between the upper right first and second molars, and metal buttons were bonded to the palatal surfaces of the upper right second molar and the lower right second molar. An elastic chain was connected directly between the miniscrew and the palatal button on the upper right second molar to exert an intrusive force for the scissor-bite correction (Fig. 6).

Fig. 6 A. Intrusion of upper right second molar with elastic chain between lingual button and miniscrew. B. Criss-cross elastic placed between buccal tube hook on upper right second molar and lingual button on lower right second molar.
A criss-cross elastic was applied between the hook on the buccal tube of the upper right second molar and the lingual button on the lower right second molar.
The refinement aligners were delivered to the patient, who was instructed to wear each pair for 20 days to allow scissor-bite resolution without unwanted extrusion of the other teeth due to temporary bite-raising, which might have worsened the patient’s facial divergence. The combination of buccal sectional appliances, miniscrews, and criss-cross elastics generated sufficient intrusion forces and moments to enable correction of the scissor bite within about five months (Fig. 7).
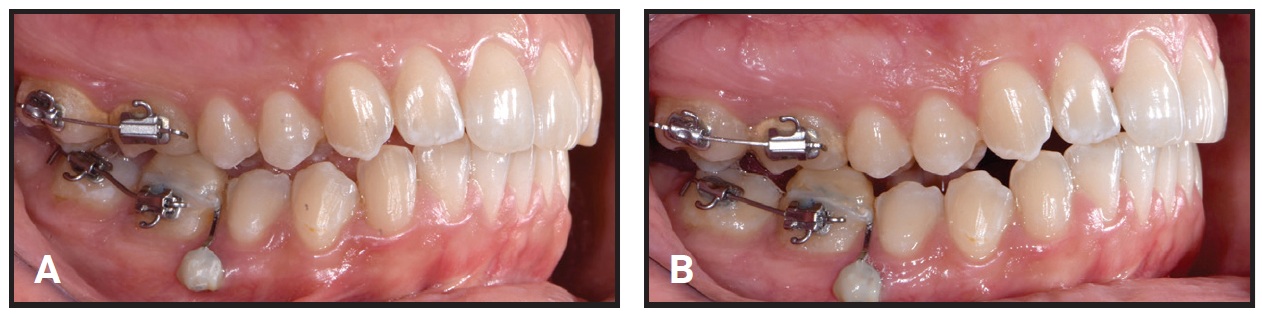
Fig. 7 A. Beginning of refinement stage, five months after start of treatment. B. One month later, with .019" × .025" nickel titanium sectional archwires placed in both arches and criss-cross elastics continued.
A month later, .019" × .025" nickel titanium orthodontic archwires were placed in the upper and lower arches, while the criss-cross elastics continued to be worn. The refinement stage lasted five months and 10 days. The miniscrews were then removed, and removable retainers were delivered.
Treatment Results
After a total 10 months of treatment, the objectives had been achieved (Fig. 8A).

Fig. 8 A. Patient after 10 months of treatment (continued in next image).
Both the lip competence and the anterior dental display in smiling were improved. The Class I molar and canine relationships were preserved, the anterior crowding and malalignment were corrected, the midlines were fully centered, and satisfactory overjet and overbite were attained. The scissor bite on the right side was resolved (Fig. 8B.
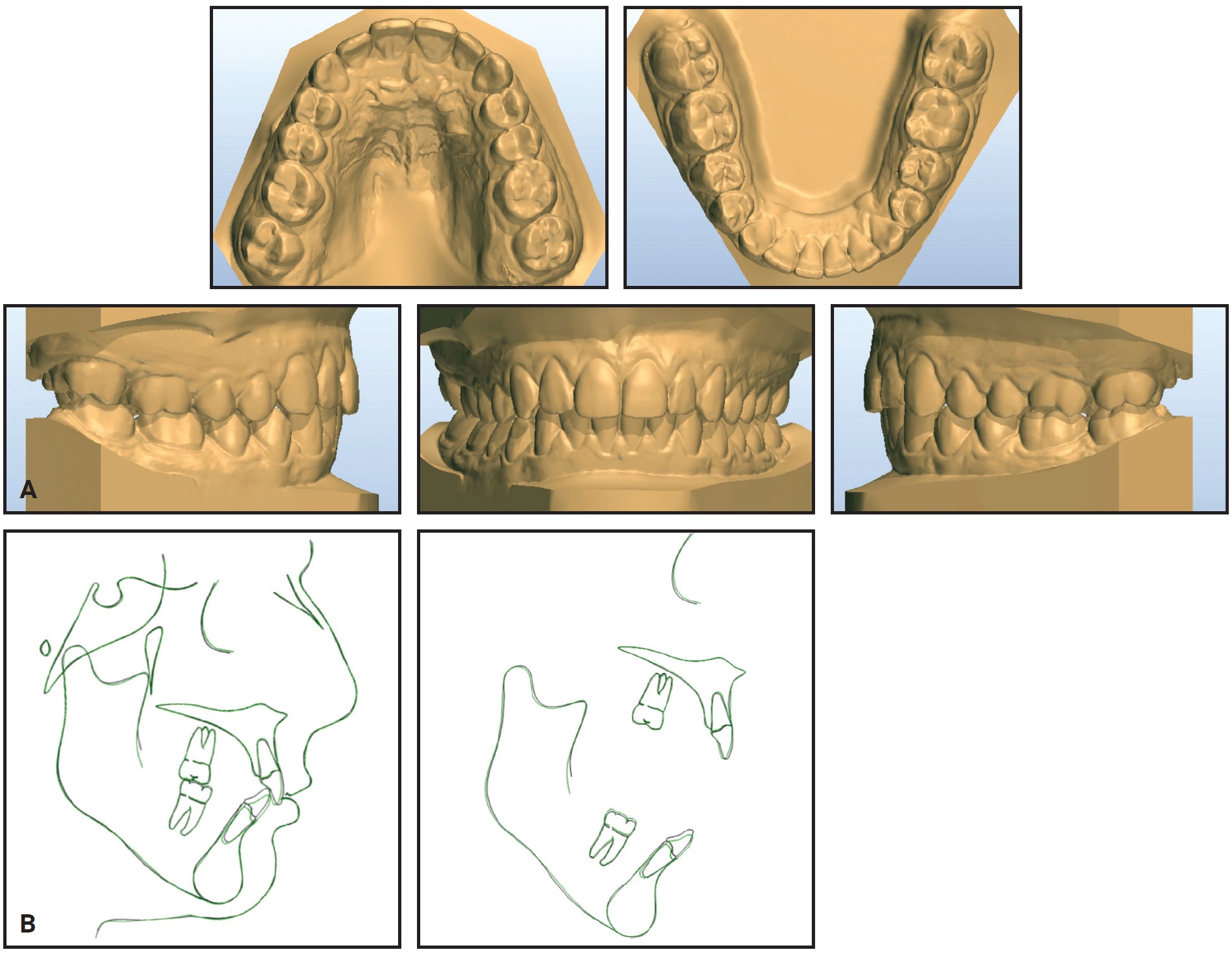
Fig. 8 (cont.) A. Patient after 10 months of treatment. B. Superimposition of pre- and post-treatment cephalometric tracings.
The post-treatment panoramic radiograph showed good root parallelism with no signs of root resorption or bone defects. Cephalometric analysis confirmed retroclination of the upper anterior teeth and slight intrusion and proclination of the lower teeth (Table 1). The skeletal divergence did not worsen, and a proper vertical facial relationship was maintained.
Discussion
This report shows how a complex case with a posterior scissor bite can be treated by means of a hybrid aligner approach involving aligners and other auxiliaries. Correction of the scissor bite was imperative not only because of its potential to compromise periodontal health, but also because the patient complained of traumatic biting of the inner right cheek. It was impossible to use full lingual appliances, and the patient declined a combination of lingual brackets with buccal tubes on the upper and lower right second molars.14 We therefore attempted to correct the malocclusion using clear aligner therapy, even though there was little chance of completely resolving the scissor bite. In fact, after two months, we decided to cut off the remaining aligners distal to the first molars to complete the alignment of both arches.
Before digital impressions were taken for the refinement stage, we planned to correct the scissor bite using sectional appliances with miniscrew anchorage. Combined with criss-cross elastics and the favorable mechanical and esthetic properties of the F22 aligners,4 this created the system of forces and moments required to resolve the scissor bite without compromising the patient’s periodontal health.15
This case report is similar to that presented by Tamamura and colleagues, in which a scissor bite at the second molars was corrected using an upper lingual appliance and a lower labial appliance, with skeletal anchorage in the upper arch.16 Unlike those authors, however, we used skeletal anchorage in both arches, along with criss-cross elastics.
In the second phase of our treatment, the occlusion and the anterior alignment were improved by clear aligner therapy while the scissor bite was corrected by the fixed component. Comparison of pre- and post-treatment cephalometric tracings showed that only dentoalveolar effects were obtained, including retroclination of the upper anterior segment and intrusion and proclination of the lower anterior teeth (Fig. 8B). The superimpositions demonstrated proper control of the patient’s skeletal divergence.
FOOTNOTES
- *Carestream Dental LLC, Atlanta, GA; www.carestreamdental.com.
- **Sweden & Martina, Due Carrare, Italy; www.f22aligner.com.
- ***Legend LP tubes, GC America, Inc., Alsip, IL; www.gcamerica.com.
- †GC Orthodontics Europe GmbH, Breckerfeld, Germany; www.gcorthodontics.eu.
- ‡Spider Screw K1 short neck, registered trademark of HDC SRL, Thiene, Italy. Distributed by Ortho Technology, Inc., Lutz, FL; www.orthotechnology.com.
REFERENCES
- 1. Zheng, M.; Liu, R.; Ni, Z.; and Yu, Z.: Efficiency, effectiveness and treatment stability of clear aligners: A systematic review and meta-analysis, Orthod. Craniofac. Res. 20:127-133, 2017.
- 2. Miller, K.B.; McGorray, S.P.; Womack, R.; Quintero, J.C.; Perelmuter, M.; Gibson, J.; Dolan, T.A.; and Wheeler, T.T.: A comparison of treatment impacts between Invisalign aligner and fixed appliance therapy during the first week of treatment, Am. J. Orthod. 131:302, 2007.
- 3. Rossini, G.; Parrini, S.; Castroflorio, T.; Deregibus, A.; and Debernardi, C.L.: Periodontal health during clear aligners treatment: A systematic review, Eur. J. Orthod. 37:539-543, 2015.
- 4. Lombardo, L.; Arreghini, A.; Ramina, F.; Huanca Ghislanzoni, L.T.; and Siciliani, G.: Predictability of orthodontic movement with orthodontic aligners: A retrospective study, Prog. Orthod. 18:35, 2017.
- 5. Kravitz, N.D.; Kusnoto, B.; Agran, B.; and Viana, G.: Influence of attachments and interproximal reduction on the accuracy of canine rotation with Invisalign: A prospective clinical study, Angle Orthod. 78:682-687, 2008.
- 6. Papadimitriou, A.; Mousoulea, S.; Gkantidis, N.; and Kloukos, D.: Clinical effectiveness of Invisalign orthodontic treatment: A systematic review, Prog. Orthod. 19:37, 2018.
- 7. Lombardo, L.; Carlucci, A.; Maino, B.G.; Colonna, A.; Paoletto, E.; and Siciliani, G.: Class III malocclusion and bilateral cross-bite in an adult patient treated with miniscrew-assisted rapid palatal expander and aligners, Angle Orthod. 88:649-664, 2018.
- 8. Rossini, G.; Parrini, S.; Castroflorio, T.; Deregibus, A.; and Debernardi, C.L.: Efficacy of clear aligners in controlling orthodontic tooth movement: A systematic review, Angle Orthod. 85:881-889, 2015.
- 9. Lombardo, L.; Colonna, A.; Carlucci, A.; Oliverio, T.; and Siciliani, G.: Class II subdivision correction with clear aligners using intermaxilary elastics, Prog. Orthod. 19:32, 2018.
- 10. Keski-Nisula, K.; Lehto, R.; Lusa, V.; Keski-Nisula, L.; and Varrela, J.: Occurrence of malocclusion and need of orthodontic treatment in early mixed dentition, Am. J. Orthod. 124:631-638, 2003.
- 11. Favero, V.; Sbricoli, L.; and Favero, L.: Scissor bite in a young patient treated with an orthodontic-orthopedic device: A case report, Eur. J. Paediat. Dent. 14:153-155, 2013.
- 12. Lee, S.A.; Chang, C.C.H.; and Roberts, W.E.: Severe unilateral scissors-bite with a constricted mandibular arch: Bite turbos and extra-alveolar bone screws in the infrazygomatic crests and mandibular buccal shelf, Am. J. Orthod. 154:554-569, 2018.
- 13. Shimazaki, K.; Otsubo, K.; Yonemitsu, I.; Kimizuka, S.; Omura, S.; and Ono, T.: Severe unilateral scissor bite and bimaxillary protrusion treated by horseshoe Le Fort I osteotomy combined with mid-alveolar osteotomy, Angle Orthod. 84:374-379, 2014.
- 14. Ludwig, B.; Alexander, J.C.; Cacciafesta, V.; Fillion, D.; Gilbert, A.; Moles, R.C.; Paz, M.E.; Silli, S.M.; and Takemoto, K.: JCO Roundtable: Lingual orthodontics, Part 2, J. Clin. Orthod. 46:275-292, 2012.
- 15. Abbate, G.M.; Caria, M.P.; Montanari, P.; Mannu, C.; Orrù, G.; Capodoglio, A.; and Levrini, L.: Periodontal health in teenagers treated with removable aligners and fixed orthodontic appliances, J. Orofac. Orthop. 76:240-250, 2015.
- 16. Tamamura, N.; Kuroda, S.; Sugawara, Y.; Takano-Yamashiro, T.; and Yamashiro, T.: Use of palatal miniscrew anchorage and lingual multi-bracket appliances to enhance efficiency of molar scissors-bite correction, Angle Orthod. 79:577-584, 2009.
-
 DR. PALONE
DR. PALONE -
 DR. CERVINARA
DR. CERVINARA -
 DR. CASELLA
DR. CASELLA -
 DR. SICILIANI
DR. SICILIANI -
 DR. LOMBARDO
DR. LOMBARDO
Dr. Palone is a researcher and Dr. Casella is a resident, Department of Orthodontics, University of Ferrara, Via Luigi Borsari 46, Ferrara 44121, Italy. Dr. Cervinara is in the private practice of orthodontics in Bari, Italy. Dr. Siciliani is Chairman, School of Dentistry, and Dr. Lombardo is Associate Professor and Chairman, Postgraduate School of Orthodontics, University of Ferrara, Italy. E-mail Dr. Palone at mario.palone88@gmail.com.