JCO ROUNDTABLE
Clinical Practice in the Pandemic Era
DR. KEIM Thank you all for joining me in this discussion. In the current COVID-19 environment, will you be using different orthodontic treatment methods?
DR. BOWMAN Considering the significant number of unknowns regarding the transmission of the coronavirus, the lack of ideal treatments for COVID-19, no vaccine, and the risks of a pandemic recurrence, we will be more cognizant of the use of active and, especially, non-self-limiting orthodontic mechanisms (see our article on “Orthodontics in the COVID-19 Era: The Way Forward”). Examples requiring added caution may include reverse-curve archwires, Pendulum* distalizers, fixed functional appliances, and our own Quick Fix** and Kilroy*** springs. In addition, the application of premolar brackets may be delayed until full eruption of these teeth, as the risk for debonds is higher. Simple sliding space-closure mechanics may need to give way to conventional closed-loop mechanisms and greater use of crimpable stops, hooks, and “turning back distal ends”—all to reduce the incidence of emergency wire pokes.
DR. CARRIÈRE Orthodontics is going to change globally after COVID-19. Noncompliance appliances will probably be replaced by patient-driven appliances with goal-oriented design. We need to be able to telematically monitor our cases in between placement and completion of the action of every orthodontic appliance, and also, we need to be able to remotely stop activation when our objective is accomplished. We need our patients to be our partners in those tasks, converting them into our hands in the distance.
Similar articles from the archive:
- OVERVIEW Sterilization and Instrument Compatibility in a Digital World September 2012
- Optimizing Orthodontic Sterilization Techniques August 1997
- Efficient and Effective Infection Control January 1992
We have been working on simplifying the orthodontic procedure in recent years because of the increase in international patients in our practice and the impossibility of their visiting in person on a monthly basis. Complex mechanics and appliances with excessive moving parts or with continuous orthodontic activity will probably be replaced by minimalistic designs with few moving parts, ideally without continuous orthodontic activity. We need to decrease potential breakage emergencies and overcorrection. We need to have virtual orthodontic control of patient-activated appliances in order to maximize our efficiency and reduce the number of in-office appointments.
DR. KRAVITZ My first month back, I limited the number of debonding appointments until I got my systems in place. My biggest concern was managing my staff’s anxiety. For those patients who insisted on debonding or required the use of a handpiece because of multiple broken brackets, I saw them in a private room. The office has since been open for more than a month, and I no longer do this. I now operate a high-speed handpiece in all chairs that are open. There have been no changes in treatment methods, but rather a reduction in patient volume.
DR. SHOAF I do not anticipate using different treatment methods. We are cleaning more—six times throughout the day—and are finding ways to avoid touching doorknobs. We have two doors to our office; we designated one as “Entrance Only” and the other as “Exit Only.” For established patients, we allow only the patient to come into the office, and we direct them to seating to ensure social distancing. We also ask everyone a set of questions (we laughingly refer to them as the “Spanish Inquisition”): “Have you been/are you sick? Has anyone in your family or who resides with you been sick? Have you traveled out of the county? state? country? Been around anyone who has traveled?” If all answers are negative, then we will see the patient. If not, we reschedule them in three weeks. We have our reception area roped off to keep patients six feet away from the receptionists, and we have designated stations where people answer the screening questions and where they stand to check out and get their next appointments.
We have cleared all toys, magazines, and decorations out of our waiting room so there are fewer things for people to pick up and contaminate. All parents and siblings must wait in the car. With our new patients, we have a designated area in our waiting room (far from others!) where parents and children can sit together and fill out paperwork. When the assistants call the established patients back into the treatment area, we again go through the Spanish Inquisition just to see if they suddenly “remember” something.
All assistants know they are empowered to refuse to see a patient if any unsafe practices are revealed. We have two non-touch infrared temperature meters, and we have instituted a daily temperature check for every staff member upon arrival and checks for all patients and visitors upon arrival. Anyone with a fever will be rescheduled.
DR. COZZANI We will not change our treatment methods dramatically. Ours is a practice located in a small town, and our patients love to see us. During the lockdown, we didn’t have many emergencies, and the patients we saw on return were under control. We made the decision to reduce the number of patients per day and to work Monday through Friday and sometimes on Saturday mornings. Since we are two orthodontists working in the practice, we also decided to split up and work in two teams that have no contact with each other. One team works three days per week, and the other team the other three days. Patients are not shared, and if, unfortunately, we come in contact with a positive patient, one team will go into quarantine for 15 days, but the other will be able to work and the practice will not close.
We have developed a telephone triage process, which is repeated on arrival at the reception desk, when body temperature is also remotely measured. Patients must arrive wearing a mask and accompanied by one person at most, wash their hands, put on gloves that we supply, and go to an enclosed area to rinse with hydrogen peroxide. After this, they are accompanied to the chair, where they must not touch anything. The orthodontist removes the mask, works in the mouth, and when he is finished, puts the mask back on and dismisses the patient. At this point, the chair and the surfaces are cleaned and the room aired for five minutes. We do not see patients in open bays any more.
DR. KEIM How are you adjusting in terms of your equipment?
DR. SHOAF We have our usual personal protective equipment (PPE), eye wear, masks, and gloves. We were smart in that we started ordering extra PPE and other equipment early in the game, so we (knock on wood) have not run out at this point. All the staff knows they wash their hands (sing “Happy Birthday” twice to get the timing right!) upon arrival and after lunch, and then after patients. We keep hand sanitizer around, but know it is actually better to wash, so we keep sanitizer use to a minimum. We are having the patients wash their hands after they brush their teeth, before returning to our chairs. Chairs are wiped down with sanitizer wipes after every patient. We have the patients swish vigorously with Listerine**** prior to any handpiece use, and we use high-speed suction during any handpiece use. We do very little in the way of alginate impressions, so the scanners and three-dimensional printers are all cleaned normally. We are using the same bonding techniques with NOLA† suction devices.
DR. KRAVITZ Our staff are wearing high-level masks, gowns, and goggles or face shields. To date, I am not adding new office equipment, such as aerosol vacuums or ultraviolet (UV) lights. I am concerned that dental supply representatives are using this time as an opportunity to sell potentially unnecessary equipment.
DR. COZZANI We decided to divide the appointments into three types: with aerosol, without aerosol, and consultations. Those that produce aerosols are concentrated in one or two days, and consultations are at the beginning or end of the day. We then have different types of equipment and PPE for each of these types.
- With aerosol: disposable waterproof gown, hat, shield, N95 mask, and hypersuction.
- Without aerosol: disposable waterproof gown, hat, shield, and N95 mask.
- Consultations: disposable gown and surgical mask.
DR. CARRIÈRE In our case, the additions in our practice will be related to PPE for patient and staff protection. We understand that simplifying the orthodontic procedure is also a strong component of PPE.
DR. BOWMAN Certainly, maintaining a substantial amount of PPE (while continually revising the estimated burn rate of supplies) will be a constant challenge, especially considering the shortages in the supply chain that are likely to continue. We will have to be more cognizant of the use of PPE throughout the entire office, dependent upon the staff risk related to their job duties and their proper donning and doffing. The addition of thermometers; maintenance of our facility’s air filtration, including replacement filters, UV lights, and cleaning and monitoring equipment; greater awareness of more frequent disinfection in areas where we may not have been as detailed, such as bathrooms, common areas, staff lounge, and reception; and additional waste handling and disposal and laundering will all require added hours, training, and associated costs. At least for now, we have sadly stopped the office tour; reception amenities like video games, coffee bar, and magazines; and parents wandering throughout our office to enjoy our various displays. We have also temporarily closed our satellite offices to focus on changes in our primary location and to catch up on our backlog of government-mandated “abandoned” patients from the past few months. We have been diligently evaluating a variety of equipment for aerosol mitigation and will be adopting several options in the near future.
DR. KEIM How are you adapting your techniques to work with this new or modified equipment?
DR. COZZANI In our daily practice, we had always used indirect bonding systems. With the advent of 3D technologies, we used indirect bonding developed on virtual impressions of the dental arches. We have been using individualized rapid maxillary expansion for more than 10 years, and recently we have 3D-printed the appliance and laser-welded the screw. We also use these technologies to prepare individualized bands; all this enabled us to reduce the number of initial appointments. In case we have doubts about using aligners vs. other techniques, we tend to use aligners.
DR. CARRIÈRE Minimal-touch orthodontics will probably be the trend. Self-ligating brackets and indirect bonding may prevail over traditional brackets and direct bonding, as those will help diminish the number of in-office activations and appointments. As we do more steps in advance in our lab, less chairtime will be necessary, and this will consequently boost the office workflow while also allowing us to implement the new pandemic preventive steps, timings, and rules—all necessary to treat our current patients. The use of aligners will probably increase as well, although to me, treatment hybridization with other appliances to first correct the sagittal discrepancies will be an interesting alternative to allow short, predictable, and effective treatment with aligners.
DR. BOWMAN “Clearing the air” by reduction and mitigation of the aerosol plume during bonding and debonding will be a challenge. Paul Gange Jr. of Reliance Orthodontic Products‡ has provided some useful strategies to eliminate the requirements of using the air-water syringe.1 In terms of bracket removal, debonding pliers and/or electric high-speed handpieces (running at slow RPM while maintaining high torque with less vibration) or blocking “chip” air in handpieces are options for removing residual adhesive and polishing. During bonding, the acid etch and rinse may be done by employing small squirt bottles with needle tips to reduce splash, followed by dental “hair” dryers. During these procedures, we may have to increase the use of a variety of high-volume evacuation (HVE) attachments. These may include dual HVE tubes with different types of attachments, such as cheek retractors featuring an HVE device clipped just below the patient’s lip (Fig. 1). Other options include vacuum dental mirrors (Fig. 2) or perhaps a return to four-handed assisting using funnel and traditional suction-tip attachments.

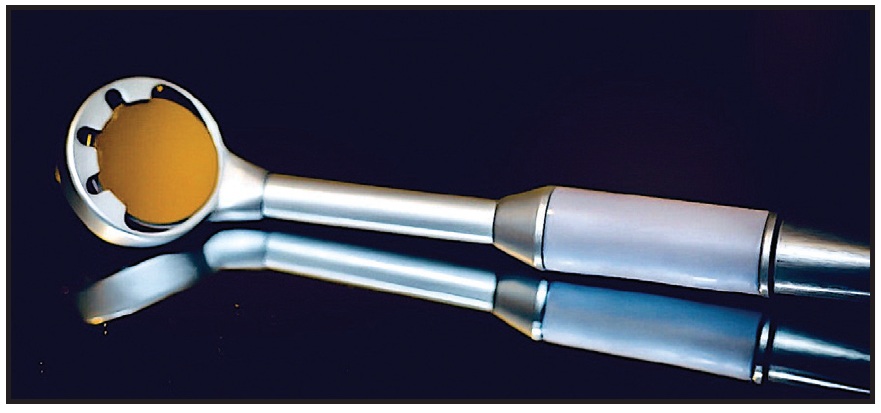
We may also employ a mobile “nail salon” vacuum-
filtration unit (Fig. 3) and even a clear plastic shield over the patient’s head, further cramping this crowded site. Necessity is certainly demonstrating its role as the mother of invention.
DR. KRAVITZ I do not plan on overhauling my bonding techniques, although my staff has favored the use of self-etching primer instead of the two-step etch and prime technique. I believe that the greatest change regarding high-aerosol procedures will be the need to separate patients, reduce the volume in the office, and simply slow down during the appointment to ensure that proper precautions are being taken. We have removed a column of patients from the schedule, and we work out of every other chair.
DR. BOWMAN We will also be required to reduce the capacity of our facility because of social distancing; the fact that there are no easy solutions for an open-bay clinic area; and the added time and detail involved in using PPE, between-patient preparations, and disinfection requirements. We will work in pairs of clinic chairs for non-aerosol-generating procedures such as simple wire changes and appliance and retainer checks. In this scenario, a patient will be treated in one chair while the other chair of the pair is being disinfected. One staff member will be working with the patient while a scribe (record-keeping assistant) is entering information into the computer, taking photographs, and sending orders, prescriptions, and progress notes to the reception area to be transmitted. Never the twain shall meet: the scribe does not have direct patient contact, and even though we have computer keyboards and mice that can be disinfected, the treating assistant does not touch the computer. Each pair of chairs will have a divider between them to demarcate distancing. At the conclusion of the appointment, the scribe then contacts the parent via video chat, phone, or text to discuss the appointment. It is important to note a demarcation between the front and back offices, as no clinical staff (in appropriate PPE garb, perhaps for an aerosol-generating procedure) will travel to the reception area and vice versa (Fig. 4). The patient entrance and egress are handled by our greeter (reception screener). A progress summary check sheet can be provided by e-mail or text to the parent as well. The next appointment will then be handled by phone by the appointment coordinator.

Fig. 3 HealthyAir§ oral aerosol vacuum and air-purification filter for close-to-mouth evacuation.
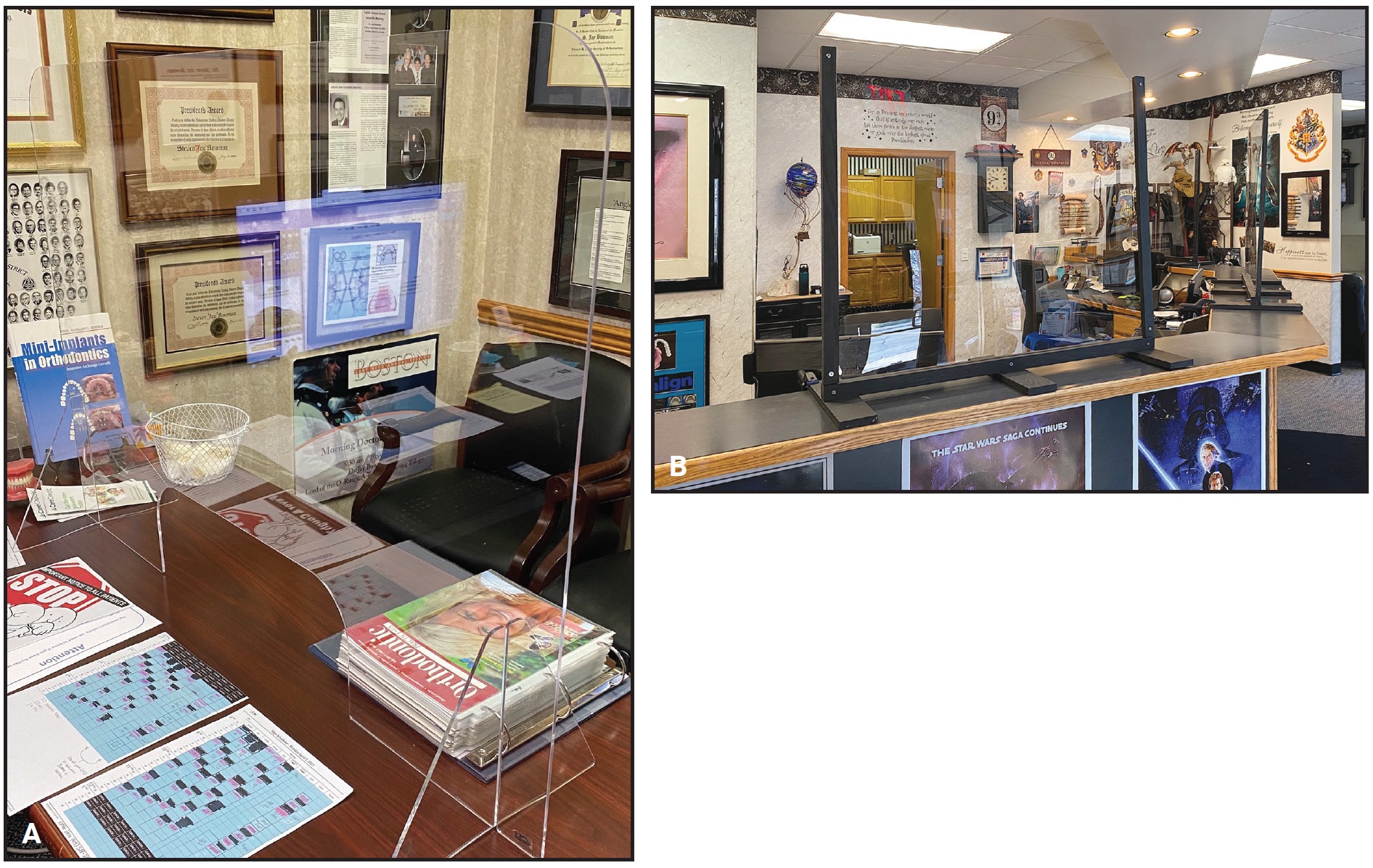
Fig. 4 A. “Sneeze guard” in front of treatment coordinator’s desk in office of Dr. Jay Bowman, Portage, MI. B. Clear plastic screens around reception desk in Dr. Bowman’s office.
DR. KEIM Are you going to try to treat with fewer office visits?
DR. CARRIÈRE Yes, we have designed protocols to be able to decrease the number of in-office appointments to four or five in total and have scheduled virtual checkups in between. The key point for this, in our point of view, is to convert all the cases into Class I at the beginning, using the Sagittal First§§ appliance, and then jump into passive and precise self-lighting brackets or aligners. It’s extremely important to place our brackets accurately, as this will diminish the need for wirebending at the end. Ideally, this is combined with a simple wire sequence; we use an efficient three-wire sequence today.
Goal-oriented appliance design, goal-oriented treatment strategies, simplicity, and clear protocols are going to be important for an economically healthy practice.
DR. KRAVITZ I need to see patients when I need to see them. I want to see VIP patients every three to four weeks. These patients include adults, patients with ectopic canines, challenging cases, and patients with questionable compliance. I simply plan on working longer days, through my lunch block, and on weekends to accommodate those patients who need appointments. I also worry that patients who haven’t been seen in three months will become infuriated that their next appointment is pushed out another three months.
DR. SHOAF Treating with fewer office visits is a real conundrum for me. As my office is almost 85% Medicaid, and we get paid only when patients come in for treatment, if we lengthen the time between appointments, we will get paid less over time. I have had a few patients come back in six weeks when the only thing we were waiting on was their more vigorous use of elastics for Class II and Class III correction, but that is not the vast majority of patients. We did give our Invisalign§§§ patients more aligners per visit (five to six instead of four) in March and April to allow appointments to be pushed farther out in the future, to where we hope protocols will be eased a little and we can provide services without all the additional inconvenience.
DR. COZZANI We are convinced that excellence needs continuous and accurate work. We believe it is correct to protect operators and patients from infection, but not to decrease our time dedicated to achieving the best result. For this reason, we are committed to reducing appointments at the beginning, as I mentioned earlier, and during treatment when some evaluations can be done remotely, but we are unable to reduce the finishing appointments. We believe that the patients deserve the highest level of finishing.
DR. KEIM Have you changed your retention protocol?
DR. KRAVITZ No change in my protocol. We still place an upper 2-1-1-2 Bond-a-Braid§§§§ and lower 3-2-1-1-2-3 Ortho-FlexTech§§§§ wire with an overlay Essix,††† and we scan for an upper circumferential and lower standard Hawley. We bring the patient back after three months, then another six months, and then another year.
DR. COZZANI I have always used removable retainers for both the upper and lower arches. My checks after the end of treatment are one month, six months, and, finally, once a year; I don’t see any reason to change this protocol.
DR. CARRIÈRE We will use vacuformed invisible retainers instead of bonded retainers. They are easy to replace remotely at any time using the original scan and 3D printing.
DR. BOWMAN At least for the near future, we will continue using primarily removable retainers—upper clear retainer and lower Apex Revolution Spring Retainer.‡‡‡ Since Dr. Kravitz reported that breakage of fixed retainers is about 50% upper and 20% lower,2,3 we had already moved toward a lower device that can be used not only as a retainer, but also as a bit of an insurance policy. Namely, if the patient notes any mild tooth movement, it can be easily corrected without a return visit by simply having the patient wear the same aligner full-time again, until the issue is resolved. This is in contrast to an aerosol-generating procedure to repair breakage. Plus, if tooth movement occurred in the interim since breakage, we would likely need to fabricate the Revolution Spring anyway to correct that. So we get prevention and treatment from the same device.
DR. SHOAF When the whole COVID-19 problem started, we stopped our retainer checks, new-patient consultations, and bonding appointments altogether. When we returned after being totally closed for three weeks, we saw only established patients for continued care. This cut our number of patients from about 125 per day to about 85 per day, which was fine with all the new infection-control protocols we instituted. Over several weeks, we gradually added bondings, observation recalls, and new patients. We are reinstigating retainer checks, but we will continue the prescreening questions as well as the temperature checks. Anyone who is found to be at risk will be rescheduled three weeks out, when the whole regimen will be repeated. We normally give patients their 3D-printed models at the time of initial retainer fitting and tell them to bring the models back for remakes if the retainers break or otherwise need replacement. Patients are now allowed to bring their models for remakes, but at delivery, they must undergo the usual questioning and thermometer checks to be able to receive their retainers.
DR. KEIM Have you introduced or expanded virtual visits?
DR. KRAVITZ Nope. I will continue to answer basic emergencies virtually on my cellphone or over social-media apps, like most orthodontists. But I assume this question pertains to virtual consults. I have zero intention of doing new-patient virtual consultations for now. I believe these appointments blur the lines between orthodontists and those at-home aligner companies that we are fighting so hard to differentiate from. As I have said before, the best way to improve office efficiency is to get the diagnosis correct!
DR. BOWMAN I believe that some definitions are necessary to avoid confusion. A so-called virtual consultation without such diagnostic records as quality photographs and radiographs would seem to be unethical, considering there is no actual dental intraoral examination. In other words, embarking on treatment without in-person evaluation would likely be insupportable, and it borders on objectionable, mirroring that direct-to-consumer, doctor-absent marketing. On the other hand, a virtual screening evaluation or exam seems reasonable for the patients and the practice to gather information (including a medical and dental history), assist patients in deciding whether an in-person exam and consultation is warranted, and perhaps answer basic financial questions.
A virtual visit would occur during treatment to assess and monitor treatment progress and determine when the patient should return for an in-person adjustment or evaluation. Visualizing treatment progress by attempting to evaluate intraoral fine details using a cellphone camera can be a challenge because of the issues of focus and lighting, poor retraction, and the patient’s inability to provide an accurate bite. I prefer to have patients attempt to provide still photos and submit them before any video meeting; they need to be guided in obtaining these photos with video, printed, or phone instructions. In this manner, we can triage emergencies or have a chance to formulate a strategy for answering questions or giving recommendations, rather than conducting an uninformed and off-the-cuff conversation by phone or video meeting.
DR. SHOAF Personally, I do not see how virtual office visits are of any help to the way I practice, except with clear aligner patients. We have such a small percentage of our patients in clear aligners that going through the expense and training to do virtual visits is just not practical. I use too many elastomerics and too few other appliances—Herbst,†††† Forsus,‡‡‡‡ bionators, headgear—to be able to use virtual office visits. I’m glad someone is able to do them, but they are not of any use for my practice.
DR. CARRIÈRE Our virtual visits will be scheduled between the in-office ones, and we will virtually sit in front of the patient, giving instructions according to what we need. Interactive monitoring tools will help very much for clinically accurate control and explanations.
DR. KEIM Are any of you introducing or expanding remote monitoring?
DR. CARRIÈRE Absolutely. Digital monitoring improves the accuracy of our virtual appointments and gives added value to our patients. Excellent platforms such as Grin,¶ Dental Monitoring,¶¶ and a few more are arising. It’s important to make it simple and economically affordable for patients and doctors. I am currently testing some of them, and I am personally very impressed. Today, we are working on a project to mathematically objectify the method using the new and precise 3D digital scanning technology.
DR. COZZANI Remote monitoring is very important to maintain contact and reassure patients, and we have done and continue to do many remote controls. Educated patients are able to make video clips or video calls useful for evaluating the progress of their treatment, but the evaluation may not be as accurate as it deserves to be because of differences in camera accuracy and because the video or photo is not taken by a professional. Moreover, orthodontics is a branch of dentistry, which is in turn a branch of medicine; therefore, we consider it indispensable to respect the cardinal principles of a medical evaluation: anamnesis and physical examination, including inspection, palpation, percussion, and auscultation. While anamnesis can be performed and reassessed remotely, the physical examination can be delayed, in emergency situations, but not eliminated. If necessary and possible, we can extend our normal schedule of appointments during treatment from the usual four weeks up to eight weeks with remote monitoring. We consider it necessary to evaluate our patients at least every eight weeks, not only from an orthodontic point of view, but also from the functional, dental, periodontal, occlusal, articular, and psychological points of view.
DR. SHOAF Remote monitoring is of little use in my practice. We have used intraoral photos from patients to determine if we needed to come into the office for emergency visits, but otherwise, remote monitoring does not work for me.
DR. KRAVITZ I don’t use it either, but I do believe teledentistry will become an increasing part of orthodontic practice. The smartphone has empowered the patient. We live in a world where “the patient will see you now!” I believe we are only years away from smartphones doing intraoral digital scans.
DR. BOWMAN The issue with remote monitoring devices and cellphone methods is long-term patient compliance: will they follow through for more than a few months once the novelty wears off? If they will, then we may have a useful tool to potentially reduce the number of visits. The high-tech nature will appeal to some patients, and considering the Hawthorne effect, the patient’s compliance may be enhanced simply by the fact that they know they are being monitored, but some others will fall by the wayside without benefit. It seems the response to so-called policing devices, like timing sensors or compliance dots, has been variable, so remote monitoring becomes a cost-benefit question—the time value of money (considering the associated costs and compliance) and the money value of time.
DR. KEIM What other ideas do you have for delivering quality treatment with fewer visits or less contact?
DR. KRAVITZ I don’t. There are no shortcuts in orthodontics. What gets inspected gets respected. Patients who are seen frequently, with professional records and thorough observation, will treat better than those seen infrequently with patient-taken photographs.
DR. SHOAF With the patient population I have at present, fewer visits can actually turn on me—if I do the treatment in less than a certain number of visits, I am penalized by Medicaid in my state, and we have to provide rigorous before-and-after records to prove the case was completed properly in so few visits. So it is not to my advantage to decrease the number of visits in my practice. As a physician assistant prior to becoming a dentist and orthodontist, I learned all about infection control, and I feel very comfortable and confident in my regimen.
DR. COZZANI We believe we can reduce the appointments at the beginning and during the treatment, as I described previously, but we must keep the utmost attention for the best possible result during the finishing phase. We are convinced that the name of the game is self-protection for patients and operators, maintaining the maximum quality of the result.
DR. BOWMAN Luckily, many of the superelastic materials that we use in orthodontics permit longer intervals between appointments. Since the introduction of these materials a few decades ago, we’ve had orthodontists recommend that we should just be patient and “let the wires and springs work themselves out.” Starting treatment at a bit later age will allow more complete eruption of the permanent teeth, with more crown length to improve bonding and thereby reduce broken-bracket emergencies. In addition, more observation, clear aligner, and retention checks may become specifically appointed as virtual visits.
DR. CARRIÈRE In our reopening stage, every patient has had three appointments on the same day. The first is a virtual appointment where we explain how they will find us unusually dressed with our PPE, as well as the technical steps and protocols of the in-office appointment. The second one is the clinical in-office appointment, which is devoted to purely orthodontic treatment. The third and final one is another virtual communication at the end of the day to summarize the evolution of their case, face to face without our PPE.
DR. KEIM How else do you communicate all these changes to your patients and the general public?
DR. BOWMAN We use a combination of office-generated (not “canned”) newsletters, blogs, our patient rewards hub, and daily social-media postings. Newsletters are printed as stuffers for statements, and they are sent to referrers as well as e-mailed to patients. The information is also reiterated by staff during phone calls, at reception, and in the clinic. It’s been said that it may take seven repeated exposures to information before the messages are absorbed (or even read).
DR. CARRIÈRE We have created a set of videos where I personally explain all the changes and protocols. We send this to the cellphone of every patient as a WhatsApp¶¶¶ message—a platform widely used in Europe.
DR. COZZANI We have also sent and keep sending videos through social-media apps to all patients explaining the procedures. Moreover, our website contains all the necessary information. Amazingly, after we restarted, all patients came in knowing how to behave during the appointments. We had an absolutely reduced number of no-shows compared to before the COVID-19 emergency.
DR. SHOAF We used our Facebook page to get the immediate word out and also had it recorded on the telephone message you got when you called the office. I had several receptionists come in for a few hours at a time by themselves with the rest of the office closed to call patients for rescheduling, especially when we figured out when we were going to open again. Everyone felt comfortable with the new procedures and understood them prior to our opening. As we rescheduled people, we told them on the telephone of the changes. More than a few parents and patients were unhappy with the changes in our schedule, but we told them we were going to do it this way for everyone’s safety, so it was hard to say a lot after that. My guess is that new patients will be down a lot over the summer (which is usually our busy season), until people can figure out what they want to do. Traveling and vacations will certainly put a crimp in our treatment schedules, more so than usual.
DR. KRAVITZ Most patients are understanding, but the few who are not can cause incredible stress for a practice. These patients refuse to accept multiple rescheduled appointments (owing to the ever-changing governor mandates), and they stress over their treatment being delayed a few months. I try to make myself personally available to answer any questions or concerns.
DR. KEIM Any comments on the financial impact of the pandemic?
DR. COZZANI We have not permanently changed our fees; from reading scientific articles on COVID-19, we are confident enough that this situation will be temporary, and we are skeptical about a “second wave.” Instead, we suspended payments during the lockdown, because we didn’t feel like asking money from patients and parents who were forced not to work. The economic, political, and social situation, at least in Italy, worries us more than the health situation.
DR. SHOAF I was lucky enough to get a loan through the Paycheck Protection Program to be able to pay our staff as usual during the time we were closed, so no one was fired, no one lost medical or dental benefits, and no one lost a lot of salary; they were able to handle their rent, food, and other expenses during the time we were closed. I was really glad I was able to provide this for my staff, as they work very hard, and I didn’t want any of them to have concerns about food, insurance, or rent or mortgage during this awful time.
DR. KEIM Thanks for your candid remarks.
FOOTNOTES
- *Ormco Corporation, Orange, CA; www.ormco.com.
- **Quick Fix Kit, trademark of American Orthodontics, Sheboygan, WI; www.americanortho.com.
- ***Trademark of American Orthodontics, Sheboygan, WI; www.americanortho.com.
- ****Registered trademark of Johnson & Johnson, New Brunswick, NJ; www.listerine.com.
- †NOLA Dry Field System, Great Lakes Dental Technologies, Tonawanda, NY; www.greatlakesdentaltech.com.
- ‡Reliance Orthodontic Products, Itasca, IL; www.relianceorthodontics.com.
- ††Xuction Dental, Midlothian, VA; www.xuctiondental.com.
- ‡‡Nu-Bird Inc., Maple Valley, WA; www.nu-bird.com.
- §HealthyAir System, registered trademark of Healthy Air Inc., Miami, FL; www.healthyair.com.
- §§Trademark of Henry Schein Orthodontics, Carlsbad, CA; www.henryscheinortho.com.
- §§§Registered trademark of Align Technology, Inc., San Jose, CA; www.aligntech.com.
- §§§§Trademark of Reliance Orthodontic Products, Itasca, IL; www.relianceorthodontics.com.
- †††Registered trademark of Denstply Sirona Orthodontics Inc., Sarasota, FL; www.essix.com.
- ‡‡‡QC Orthodontics Lab, Inc., Fuqua-Varina, NC; www.qcortho.com.
- ††††Registered trademark of Dentaurum, Inc., Newtown, PA; www.dentaurum.com.
- ‡‡‡‡Trademark of 3M, Monrovia, CA; www.3M.com.
- ¶Get-Grin Inc., Tel Aviv, Israel; www.get-grin.com.
- ¶¶Registered trademark of Dental Monitoring, Austin, TX; www.dental-monitoring.com.
REFERENCES
- 1. Gange, P. Jr.: Bonding in the COVID-19 Era, J. Clin. Orthod., www.jco-online.com/covid19-resources/bonding-in-the-covid-19-era, published online, April 2020, accessed May 23, 2020.
- 2. Kravitz, N.D.; Grauer, D.; Schumacher, P.; and Yo, Y.: Memotain: A CAD/CAM nickel-titanium lingual retainer, Am. J. Orthod. 151:812-815, 2017.
- 3. Kocher, K.E.; Gebistorf, M.C.; Pandis, N.; Fudalej, P.S.; and Katsaros, C.: Survival of maxillary and mandibular bonded retainers 10 to 15 years after orthodontic treatment: A retrospective observational study, Prog. Orthod. 20:28, 2019.
-
 DR. KEIM
DR. KEIM -
 DR. BOWMAN
DR. BOWMAN -
 DR. CARRIÈRE
DR. CARRIÈRE -
 DR. COZZANI
DR. COZZANI -
 DR. KRAVITZ
DR. KRAVITZ -
 DR. SHOAF
DR. SHOAF
Dr. Bowman is an Adjunct Associate Professor, St. Louis University, St. Louis; Assistant Clinical Professor, Case Western Reserve University, Cleveland; Instructor, University of Michigan, Ann Arbor, MI; and in the private practice of orthodontics in Portage, MI; e-mail: info@kalamazooorthodontics.com. Dr. Carrière is in the private practice of orthodontics at Clinica Carrière, Escoles Pies, 109, 08017 Barcelona, Spain; e-mail: luis@carriere.es. Dr. Cozzani is an instructor at the Istituto Giuseppe Cozzani, La Spezia, Italy, and in the private practice of orthodontics at Via Fontevivo 21N, 19125 La Spezia, Italy; e-mail: maurocozzani@gmail.com. Dr. Kravitz is in the private practice of orthodontics at 25055 Riding Plaza, Suite 110, South Riding, VA; e-mail: nealkravitz@gmail.com. Dr. Shoaf is in the private practice of orthodontics at Salem Smiles Orthodontics, 1063 W. Northwest Blvd., Winston-Salem, NC 27101; e-mail: sshoaf@salemsmilesortho.com. Dr. Keim is Editor-in-Chief, Dr. Kravitz is an Associate Editor, and Drs. Bowman, Carrière, Cozzani, and Shoaf are Contributing Editors of the Journal of Clinical Orthodontics.
