PRACTICE PROFILE
Sarah C. Shoaf, DDS, MEd, MS, Salem Smiles Orthodontics
In selecting orthodontists to highlight in our ongoing series of Practice Profiles, we look for those who contribute something unique, something that sets them apart from other private practitioners. With so many high-quality, highly ethical, and truly distinctive orthodontic offices in the country, that is not an easy task. We always welcome nominees for this feature, but occasionally we choose one of my own role models.
The first day of my graduate training at the Eastman Dental Center (now the Eastman Institute for Oral Health) in Rochester, New York, I was introduced to a delightful senior orthodontic resident, Dr. Sarah Shoaf, who eventually turned out to be one of the best orthodontists I have ever known. Her philosophy of life in general and orthodontics in particular impressed me right off the bat, and over the ensuing three decades she has never ceased to impress me. In addition to her considerable skills in orthodontics, I would be remiss if I did not mention her scuba-diving proficiency, her prowess on the golf course, and especially her award-winning, competition-level cooking.
Similar articles from the archive:
Many rural areas of North Carolina have no ready access to specialized orthodontic care. Dr. Shoaf has gone farther than anyone else I know to personally address this societal need and, in so doing, has built up an enjoyable, high-quality, and genuinely rewarding (on all levels) orthodontic practice that is truly unique. Once you read this profile, I think you will agree.
RGK
DR. KEIM What attracted you to orthodontics?
DR. SHOAF I was a physician assistant (PA) for six years before I went to dental school. I specifically went to dental school to become an orthodontist and work on a cleft palate-craniofacial team. Hard work in the classroom at the University of North Carolina got me a dentist-scientist scholarship to Eastman Dental Center under Dr. Daniel Subtelny, who emphasized clinical instruction on cleft palate-craniofacial anomaly patients because his own son had a cleft. My first position after graduation was actually my dream job—on the faculty of a medical school that had a dental department, and working closely with their cleft-craniofacial team. The medical-school environment also steered me into sleep appliances for the sleep-disorder group, as well as dental forensics.
I am especially proud that I completed my Diplomate status with the ABO in 2003 and have maintained that status. There are few orthodontists in our area with Diplomate status, and even fewer who are in private practice and not associated with a medical or dental school.
DR. KEIM What is unique about your practice?
DR. SHOAF I was in my mid-50s when I started this practice in 2012 (Fig. 1). After 17 years at a medical center teaching medical students, PA students, and medical and dental residents, I practiced for two years with a colleague in a nearby small town, Mount Airy. When he and I parted ways, I discovered a huge opportunity for an experienced orthodontist to treat Medicaid patients, and I became the only orthodontist in my county treating these patients. I miss the cleft team at the hospital, but I enjoy being my own boss, having the financial rewards of private practice, and helping a lot of patients who would otherwise not get the help they needed.
Our practice is unique in that it is 85% Medicaid insurance patients. We are the only office from the western tip of North Carolina coming east—about one-third of the state—that takes Medicaid. We feel we provide a huge service to those in need. To accommodate the differences in payments, we have a high-volume practice with six chairside assistants and one doctor seeing 115-125 patients per day. In the last three years, we have started more than 500 cases per year and seen more than 1,300 new consultations per year. Because we are one of the few offices that will treat Medicaid patients, we have a full roster of new patients.
One of the fun things about my office is that it is in a historical building on the edge of the historical district in Winston-Salem. We have beautiful hardwood floors, knotty pine paneling, and a generally warm atmosphere (Fig. 2). The office was featured in the West End Historical House Tour in December 2016.
Still, we emphasize high tech. We started the office using paperless charts with all of our clinic notes on computer, digital radiographs, and texting reminder systems. Oral scanning has been used rather than making alginate impressions since 2013. Our staff presently uses an iTero Element,* and we recently installed a new Element 2* scanner. A three-dimensional printer by EnvisionTEC** has been a staple of the office since 2013, and we just installed a new 3D printer from 365 Printing*** to keep up with our debonding demand. We give our completed patients vacuum-formed retainers made over 3D-printed models. We also give them the models and tell them if they break or lose a retainer, it is $200 per arch to replace, but if they bring their undamaged plastic models back, we will remake the retainers for $65 per arch. This makes it easier for us to remake retainers without new impressions and decreases the costs of “being stupid.” If a model is broken, we can reprint one from our iTero storage. As all of our models are stored in the cloud, we do not have the storage problem of keeping old before-and-after models. If we need a new set of models, we just reprint it on the EnvisionTec printer (Fig. 3).
DR. KEIM What are the main types of treatment in your practice?
DR. SHOAF Our advertising has a heavy bent toward Invisalign.* As I was in the original East Coast training session of Invisalign in 1999, I have been with them throughout their development and changes over time. I feel very comfortable doing complicated cases with extractions and elastics, and I am even working with mentally and physically challenged patients who would not be able to tolerate traditional fixed appliances (Fig. 4). With my PA background, I do not feel intimidated by long medicine lists or patients with type 1 diabetes, Down syndrome, cerebral palsy, craniofacial anomalies, or other disorders. I have done many cases with mentally and physically challenged patients using both fixed appliances and Invisalign. I do not use temporary anchorage devices, Herbst,† or other ancillary appliances, since they are more expensive than elastics. We also try to get our special-needs patients into Invisalign, as they tend to do better than with fixed appliances.
I do feel aligner therapy is the wave of the future for orthodontics, as it is truly the “kinder, gentler” way to move teeth. We do not charge a premium price for our Invisalign cases, and we often have Invisalign priced less than our fixed appliance cases to encourage patients to use Invisalign. My theory is that the teeth can’t tell if a wire or a piece of plastic is pushing them in a direction, so why should I charge additional money for the service? We actually feel it is more cost-effective to treat Invisalign cases because they do not have to come to the office as often, and they take up less chairtime, have fewer emergencies, and are generally happier about the progress of their treatment.
DR. KEIM What is involved in the treatment of sleep disorders?
DR. SHOAF While at the medical center, I helped a technician at AOA Lab‡ design a one-piece, nonadjustable mandibular-protrusion sleep appliance, and we have made them for several sleep-disorder physicians and centers in our area for the last 25 years (Fig. 5). In working with adjustable designs such as the Herbst-type in the past, I found most of them not to be durable and to be subject to frequent breakage at the point of adjustment. I’ve authored a number of articles in JCO, PA journals, and other publications about how to examine the patient, determine the new position for the appliance, and fit the appliance. One great new thing with sleep appliances is the use of oral scanners. We send our “models” electronically to the lab for printing on their 3D printer, and we send only a polyvinyl siloxane bite registration along with our prescription form in the mail. I’ve even worked with the good technicians at AOA Lab to make a sleep appliance that will fit over aligners, to accommodate patients who want to align their teeth while using oral sleep-positioning appliances.
This is an up-and-coming area of practice not only for orthodontists, but also for general practitioners, and I think all dentists should be taught something in school about sleep apnea. Most of my patients are referred from sleep-disorder physicians and teams in my area, and most are usually in their 40s or older, although I have had a couple of medical students who needed appliances.
DR. KEIM You mentioned dental forensics earlier.
Fig. 1 Dr. Shoaf in front of Salem Smiles Orthodontics in Winston-Salem, NC.

Fig. 2 Warm, light-filled treatment areas offer high-tech benefits in historical setting.

Fig. 3 In-office three-dimensional printers from EnvisionTEC** and 365 Printing*** create models from digital scans stored in cloud.

Fig. 4 Practice emphasizes lower-cost approaches for Medicaid recipients and Invisalign* treatment, especially for special-needs patients.
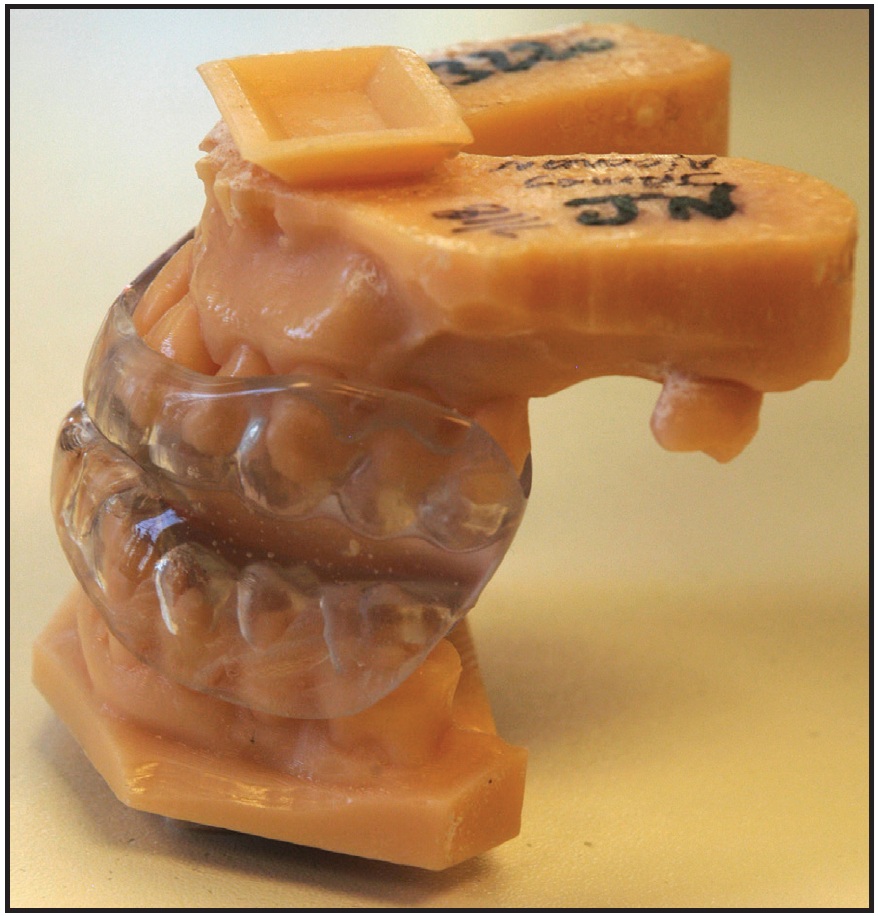
Fig. 5 Sleep-disorder appliance.
DR. SHOAF One of the fun things I do in my practice is to work with local medical examiners and law-enforcement agencies on forensic cases. John/Jane Does, skulls found by hikers, bones dug up in backyards, plane crashes, automobile crashes, decomposed bodies in rivers, burned buildings, and bitemarks all create opportunities to identify victims or perpetrators. Most of my cases have been simple identifications, but some have not been very simple because of poor antemortem records or a lack of possibilities to compare. Let me be the first to put in a plug for good record keeping, good-quality radiographs, and an excellent system for indexing all of these to enable a forensic specialist to bring someone to justice.
DR. KEIM Are there any forensic cases that stand out in your memory?
DR. SHOAF My first case was a John Doe found in the median of I-40. We did a dental charting because the medical examiner thought it was a vagrant. But the boy had perfect teeth, which could have come only from an environment of care. We had a makeup artist get the deceased looking presentable enough to post pictures on the news and in newspapers, and someone recognized this late teen. He was from Charlotte and had gone to visit friends of his at the North Carolina School of the Arts in Winston-Salem. His parents thought he was still with his friends, and his friends thought he had gone home, so no one had filed a missing-person report. Turned out he was just despondent and had thrown himself in front of a truck in the middle of the night to end it all.
Another case was actually famous in our area: a satanic cult that was found to have buried two murdered cult members in their backyard. The house was eventually condemned, the bodies were found, and we were able to identify them from lists of associates and people who had gone missing in the area.
DR. KEIM Do you have any advice for an orthodontist starting out today?
DR. SHOAF If someone asked me the secret of starting a practice and being successful with it, I would have to reply “having good people around me.” My Wake Forest connections got me set up with an accountant who made the initial bank-loan predictions for presentation, and another Wake Forest connection got me the bank loan at a fabulous rate. I worked hard when hiring people—made a few mistakes, but also rectified them—and have had the same staff for almost three of the six years I’ve been in business (Fig. 6). A private practice is hard work, but it can also be very rewarding if you have the right people around you.

Fig. 6 Dr. Shoaf’s secret to successful, rewarding practice? Good people.
DR. KEIM What would you say specifically to a woman who wanted to start a practice?
DR. SHOAF As the comics say, a woman has to do twice as much to be considered half as good, but fortunately, in comparison with our male brethren, that is not too difficult to accomplish. Again, you just need to surround yourself with good people who will work with you and for you in your endeavors.
DR. KEIM What do you see as the primary differences between male and female orthodontists?
DR. SHOAF I think women are more altruistic. Many of my female colleagues are on cleft teams, do a lot of Medicaid work, work in hospital settings, or are educators. Women tend to want to have an interesting job, rather than focus solely on the financial remuneration. Women are also more likely to take jobs with groups or large companies, because it allows them more freedom to take time off for children, and someone will be available to treat their patients when they are not in the office. I think men like to be more in control and work very hard to measure their success by finances rather than “how many people did I help today?”
DR. KEIM What do you enjoy doing when you’re not practicing orthodontics?
DR. SHOAF Aside from scuba diving around the world with my husband, Alan Miller, who is an underwater photographer (Fig. 7), I also make jewelry. I am a professional baker for a local restaurant, creating desserts, sourdough bread, and other baked goods. I usually enter jams, jellies, and breads each year in regional fairs and the North Carolina State Fair, and I have won many prizes.
DR. KEIM What do you see in the future for you and your practice?
DR. SHOAF Our summer project was to enlarge our waiting room, gain more storage space, and add additional offices for financial assistants. This will make the environment even more comfortable for the waiting parents and siblings. Every new case start receives our signature tie-dyed shirt, which we feel encourages “local” trade (Fig. 8). We will continue to make mouthguards for local soccer, roller derby, and ice hockey teams. We want to continue our commitment to the community by sponsoring activities in food, sports, and the arts. And we mostly want to continue to serve a population that is often overlooked.
FOOTNOTES
- *Registered trademark of Align Technology, Inc., San Jose, CA; www.aligntech.com.
- **Micro Plus XL, EnvisionTEC, Inc., Dearborn, MI; www.envisiontec.com.
- ***365 Printing, Norcross, GA; 365printing.com.
- †Registered trademark of Dentaurum, Inc., Newtown, PA; www.dentaurum.com.
- ‡AOA Orthodontic Appliances, Sturtevant, WI; www.aoalab.com.

Fig. 7 Dr. Shoaf scuba diving in the Coral Sea, off the northwest Australian coast, in a photo taken by her husband, Alan Miller.

Fig. 8 Tie-dyed shirts for new patients.
-
 DR. KEIM
DR. KEIM -
 DR. SHOAF
DR. SHOAF
Dr. Shoaf is a Contributing Editor of the Journal of Clinical Orthodontics and in the private practice of orthodontics at Salem Smiles Orthodontics, 1063 W. Northwest Blvd., Winston-Salem, NC 27101; salemsmilesortho.com. Dr. Robert G. Keim is Editor of the Journal of Clinical Orthodontics.
