PRACTICE PROFILE
Jeremy Fry, DDS, MS Fry Orthodontic Specialists
In this issue of JCO, we are reintroducing a feature that dates back to the 1970s, when it was called “JCO Visits”. Now under the heading of “Practice Profiles”, these articles are intended to give our readers an inside view of outstanding orthodontic practice models. Some may be familiar, but others may represent a change in current paradigms. Our initial offering is an example of the latter.
Fry Orthodontic Specialists is an expanding, multi-office practice in the Kansas City metropolitan area. Founded by Dr. Bob Fry in 1977 as part of a larger group, it split off as a thriving single-doctor practice in 1987. I am honored to have known Bob since he began guest lecturing in the graduate orthodontic program at the University of Southern California (USC) in the early 2000s. I am also proud to note that his son, Jeremy, was one of my graduate orthodontic students at USC. Bob has since retired from the practice and I have since retired from USC, but Jeremy has continued as chief executive officer of Fry Orthodontic Specialists. Under his leadership, the practice has grown to a remarkable new level. Because of the Frys’ unique approach to management and treatment, their practice was selected as our first profile in this new series of articles. I trust that you will enjoy learning about it as much as I have.
RGK
Similar articles from the archive:
- JCO Visits a Four-by-Four Practice July 1977
DR. KEIM Can you tell us a little bit about your orthodontic practice?
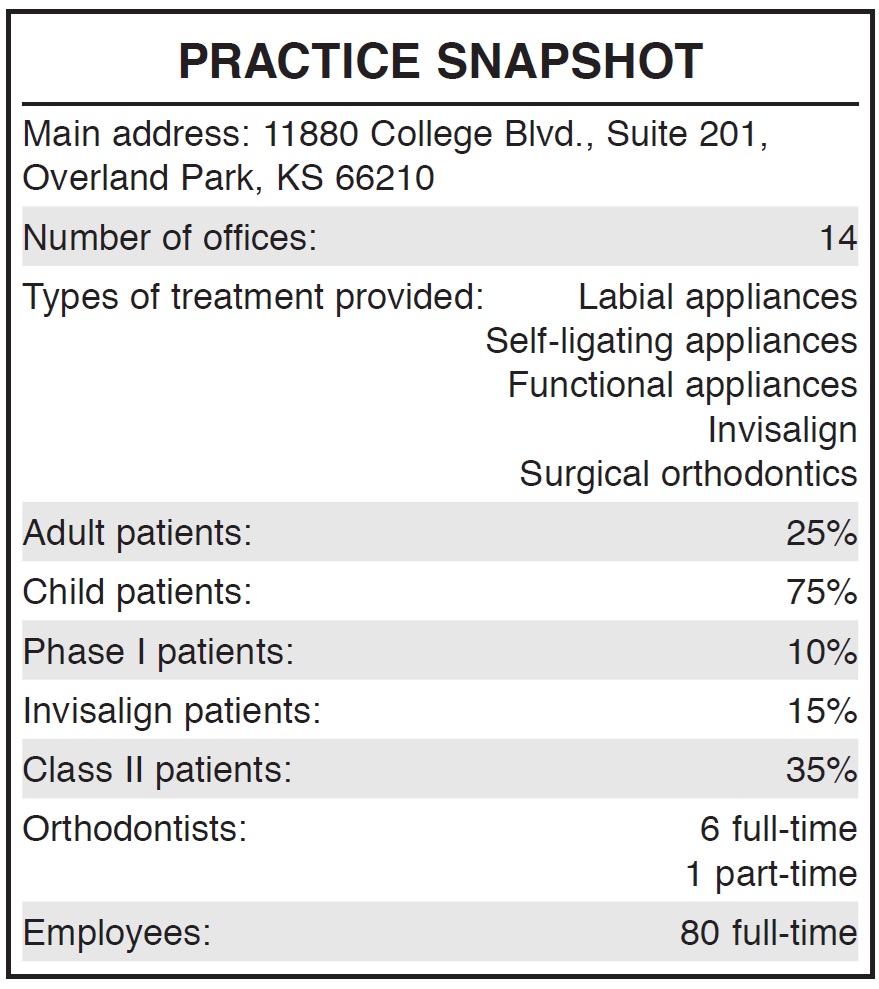
DR. FRY Fry Orthodontic Specialists is a solely orthodontic group practice consisting of 14 offices in the Kansas City area, owned and managed by orthodontists. With the changing environment and consolidation of dental businesses, we want to create options for orthodontists to help alleviate the burden of student debt, offer an exit strategy for retiring orthodontists, and provide affiliation opportunities for those in the middle of their careers who want to treat patients without all of the burdens that come with being a solo practitioner.
We believe in high-quality, patient-centered treatment that allows growth for doctors and their teams. We provide the opportunity to construct the future on their terms. While currently in Kansas City, we are growing into other metro areas over the next several years.
DR. KEIM How did your practice come to be what it is today?
DR. FRY When we were a stable three-office orthodontic practice, our doctors and team members were limited in their potential for professional and financial growth. A senior clinical assistant, for example, didn’t have a role to grow into for those skills that could add earnings potential and personal growth. When we began to affiliate with other offices, we had needs for leadership roles that we didn’t have before. There were then tracks for team members for growth in areas where there used to be none. They began to grow professionally, personally, and financially. This growth for our team is the reason we are continuing to add offices and affiliate with other offices that share our values.
DR. KEIM You mention values. What does that mean to an orthodontist in practical terms?
DR. FRY We have three simple and concise values (Fig. 1): 1. Do what’s right. 2. Treat others the way they want to be treated. 3. Tell the truth. We carry our values a bit further to include some key outcomes of these values that specifically relate to our orthodontic practice. One of those outcomes is to have the feel of a small office with the sophistication of a large one. We believe this philosophy is a differentiating factor that makes our office appealing to patients and their families, while promoting a great work environment for orthodontists and team members (Fig. 2).
DR. KEIM What makes your model different from the large multi-specialty dental offices that seem to be doing an increasing amount of orthodontics?
Fig. 1 Values of Fry Orthodontic Specialists.

Fig. 2 Philosophy of having feel of small office with sophistication of large one makes office appealing to patients and families and enhances work environment.
DR. FRY Since we are owned only by orthodontists, there is less pressure to treat patients based solely on the cheapest method or to maximize profits at the expense of orthodontic care. The “small office feel” for patients and the team is not the most productive model. There are other successful orthodontic offices that see more than 100 patients per day with one orthodontist and lots of team members. I’m sure their systems allow them to treat patients well, but we have found those types of busy days are really not conducive to building great relationships. Team members and doctors often feel beat down at the end of those days, which bleeds into the care or the perception of care that they provide. When people discuss something being “corporate”, there is a stereotypical belief that you lose that patient interaction that caused many of us to become orthodontists in the first place. We believe in a model that can facilitate the best of both worlds.
DR. KEIM With your growing number of offices, how do you maintain the quality of care?
DR. FRY I was taught by my dad only to expect what you inspect. We believe that having multiple doctors inspecting treatment plans, mid-treatment care, and finished results is actually a better quality control than most traditional orthodontic offices have in place. We have a clinical director who evaluates every treatment plan and every finished patient. We have weekly doctor meetings to discuss individual patients, difficulties with mechanics, and treatment systems. I don’t think this robust system of quality checks can be implemented without multiple doctors and offices. We discuss difficult situations, as this evaluation is the only way we can improve clinical outcomes and efficiency. Essentially, we have established an internal peer review system for all cases treated.
DR. KEIM Since you have grown primarily through acquisition, I have to assume that there are differences between the 14 offices. Have specific characteristics of one or more practices contributed so much to your efficiency that you incorporated those characteristics into the others?
DR. FRY We have an ideal model that works well within our system: a 2,500-square-foot space, six treatment chairs, and two treatment-coordinator chairs (Fig. 3). We have a centralized patient care (call) center, which allows us to staff only one receptionist (Fig. 4A). In our typical space, we usually have four patient managers (assistants), one sterilization technician, and one treatment coordinator (Fig. 4B). Although this seems a bit smaller than some models out there, we find this size allows a comfortable environment for our team and patients.
When we affiliate with another office, it is a challenge to keep the workflow efficiencies that were successful for the other orthodontist while allowing our systems to thrive. The team seems to make all situations work, but we gravitate toward ultimately implementing structural changes or moving locations so we can best care for our team and patients. We believe that all of our efficiencies stem from our treatment systems. For this reason, we usually begin all new patients in affiliated practices with GAC In-Ovation* and our general mechanics.
DR. KEIM What types of patients do you typically see, and what types of mechanics are used within your treatment systems?
DR. FRY Our practice is 75% children and 25% adults. Phase I patients represent 10% of all starts. Our Phase I patients consist mostly of crossbite correction and patients’ psychosocial desires. Most of our patients are treated with either full braces or full Invisalign.** Very few patients receive partial or sectional braces. Invisalign represents 15% of our patients.
Class II patients represent 35% of all patients treated. Our Class II protocol begins with Class II elastics and moves toward the Forsus*** appliance if cooperation is not adequately achieved. We have used all functional appliances; most recently, we have primarily used the Herbst† appliance and the Mandibular Anterior Repositioning Appliance (MARA).‡ We have found, however, that the treatment times for these functional patients were unacceptable, and similar results were experienced with Class II elastics alone. We do not use headgear for any treatments in our offices.
We have extensive surgical training among our orthodontists, but we find that surgical orthodontics is becoming a lost art. With insurance reimbursement for surgeons so low, many surgeons in our area cannot afford even to offer orthognathic surgical options to patients. Those who still offer these options have to charge so much that most patients cannot afford it. Two of our doctors, as well as my wife, did have orthognathic surgery, but we cannot seem to get those patient percentages very high. Most of the surgical patients we see are the 20-something Class III males who have known surgery was the only option for years. They show up to a new exam and tell us they are now ready. Without a large surgical percentage, we have to be very creative at expanding the envelope of discrepancy. We have patients who choose to have compromised results, and we continually monitor their stability and overall periodontal health.
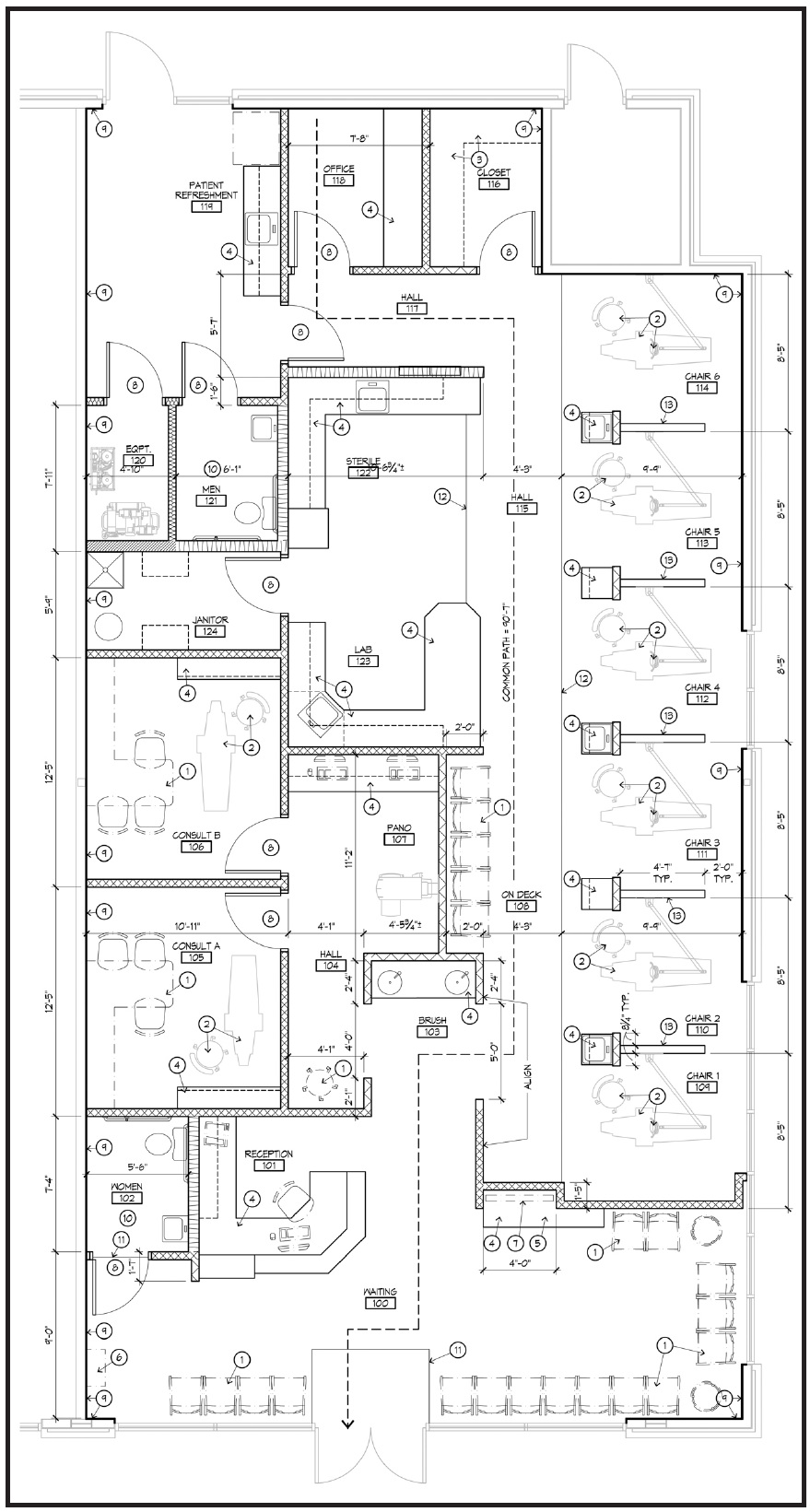
Fig. 3 Typical office floor plan.
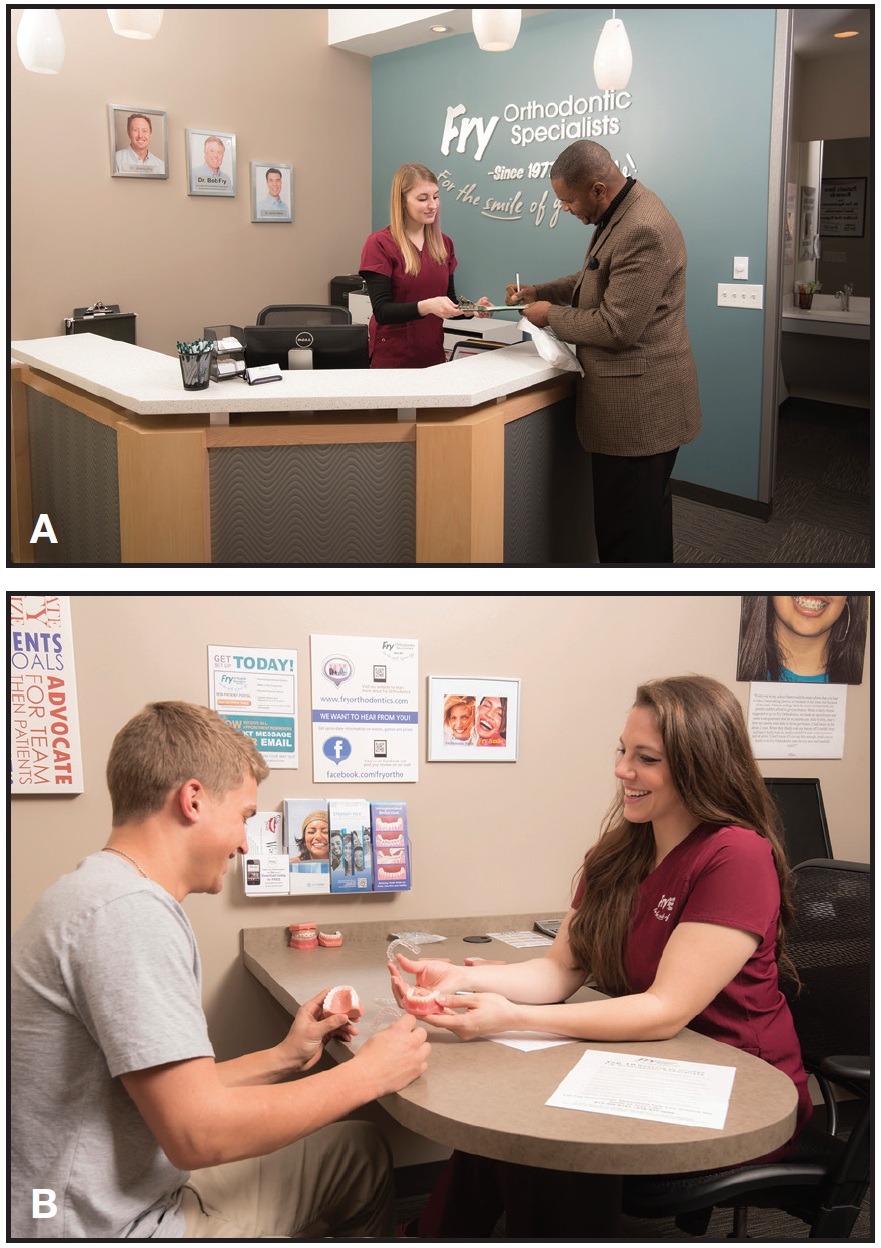
Fig. 4 A. Centralized patient care (call) center allows staffing by only one receptionist. B. Typical office space has one treatment coordinator.
DR. KEIM How do you treat patients so efficiently with different doctors from different educational backgrounds and philosophies?
DR. FRY We are proud of our treatment times. Historical statistics show that we treat average Class I crowded patients in 15 months and Class II patients in 16 months. Many clinicians want to discuss certain brackets and wires and such. I think brackets and wires are important, but those tools alone are not the key to clinical efficiency. We believe in self-ligation, and my dad has lectured on the benefits of light-force mechanics ever since I can remember. We also have a strong partnership with Invisalign, which offers a great alternative for many patients. However, I think that the key to clinical efficiency is a simple, consistent, systematic approach to patient care. There are many recipes with different brackets and wires, but minimizing the variables allows us to treat patients more efficiently. We create the riverbanks of treatment, and we allow the doctors to dictate treatment within those riverbanks. We limit Phase I orthodontics as much as possible, as we believe that it lessens our ability to get patients excited about comprehensive care when you really need their help to correct their malocclusions.
DR. KEIM Why not treat more Phase I cases?
DR. FRY There is little doubt that Phase I orthodontics is beneficial in certain limited situations. Being a father of three young kids, I really think about it in practical terms of trying to get kids to do what you want them to do, when you want them to do it. Very rarely does Phase I lead to an elimination of Phase II. I believe the comprehensive phase is where most of the work is going to get done, and patients will have to wear elastics, have more braces to brush around, and so on. I really want them motivated to help us achieve the longterm goal of getting braces off as quickly as possible with exceptional results. If they have gone through a year of Phase I, they really don’t want braces again. As orthodontists, we start Phase II with apathetic patients, and sometimes we can never get them motivated to do what we need them to do.
DR. KEIM What was it like coming into your father’s practice with a growth vision that seems different?
DR. FRY With any conversation about the history of our office, I always start by saying how profoundly lucky and grateful I am for having a father who established our foundation for excellence and for ultimate growth. This growth and vision did not just happen—it took years and years of difficult work by him and his team to fine-tune systems and allow our current team to grow. The successes and struggles of a parent-child orthodontic office transition is probably a topic for an entire magazine. It is most appropriate for me to say that my dad stepped away from the daily workings of the practice with supreme grace, and I hope that I have worked hard enough to justify his faith in transitioning control. I do not believe it could have happened any better for both of us.
DR. KEIM Can you offer any advice for other parent-child practices on what the pitfalls might be and how best to avoid them?
DR. FRY Just as in any relationship, communication of expectations is the most important part of a successful family business transition. There are many examples of these transitions in orthodontics working well and also failing. Most of the failures have been due to either the younger doctor feeling entitled and wanting to change everything about the practice, or the senior doctor being unwilling to let the younger doctor have any say. We talked openly about these potential pitfalls. We are similar people with similar egos and drive, and there was always a real risk of failure. My dad wisely decided early in the discussions never to be partners. I worked for my dad as an associate, earning the trust of him, the team, and the patients. After several years, we transitioned ownership, and then he worked for me. This structure left no doubt that the final say for any issue was with the owner. There are other ways that have been successful for some, but this model worked well for us.
DR. KEIM To what factors do you attribute your recent growth?
DR. FRY As most of us have seen, the rise of orthodontics as a rite of passage for teenagers has opened the door for practice growth. Specifically in our case, we believe our values and practice environment facilitate a culture that patients and parents desire. I think the specialty has seen a rise in entrepreneurial-minded orthodontists. There are more and more orthodontists putting the patient’s experience over some of the more traditional orthodontic metrics used to judge success. We strive to be a patient-centered experience, and I believe that has contributed to our growth (Fig. 5). Fortunately for me, my dad’s philosophy was exactly that way before it was common to be patient-service-centered. Our most recent growth has come simply by expanding our footprint with more offices while maintaining the exceptional service component.
DR. KEIM What’s next for your practice?
DR. FRY We are excited to grow to other metro areas over the next several years. We want to provide that opportunity to grow with others who have matching goals of efficient, high-quality, patient-driven orthodontics.
DR. KEIM Thank you for sharing your practice philosophy with our readers.
FOOTNOTES
- *Registered trademark of Dentsply GAC, Islandia, NY; www.dentsply.com.
- ***Registered trademark of Align Technology, Inc., Santa Clara, CA; www.aligntech.com.
- ***Trademark of 3M Unitek, Monrovia, CA; www.3MUnitek.com.
- †Registered trademark of Dentaurum, Inc., Newtown, PA; www.dentaurum.com.
- ‡AOA Orthodontic Appliances, Sturtevant, WI; www.aoalab.com.

Fig. 5 In Dr. Fry’s view, striving for patient centered experience has contributed to practice growth.
