COMMENTARY Complex Orthodontic Treatment Using a New Protocol for the Invisalign Appliance
ROBERT L. BOYD Sep. 2007
In 1997, as part of the requirement for their degree completion, two MBA students at the Stanford University School of Business devised and submitted a business plan for a new company. Their concept was a revolutionary approach to orthodontics involving the use of sets of clear, vacuum-formed retainer-like aligners to move teeth in stages, based on a computer-generated sequence of movements. In their small apartment, the two students and one PhD computer-graphics engineering student gave birth to Align Technology and the product we know as Invisalign.*
Attempting to move teeth with removable appliances was not a new concept. Most orthodontists, myself included, had tried removable appliances for simple tooth movements with marginal results. In 1998, Align was eager to find clinicians to be “alpha” testers for their new product. When I was approached, I listened politely and declined. But they were so desperate for testers that they agreed to buy me a personal computer and show me how to use it (which was the real challenge).
I was still unconvinced about participating, though, so they played their trump card. I was assured that the lead investigator for Invisalign treatment was Dr. Bob Boyd, Chairman of Orthodontics at the University of the Pacific Arthur A. Dugoni School of Dentistry. While I did not know Dr. Boyd personally at that time, I had admired his research and writings, as well as his commitment to orthodontics. He is now widely recognized as a pioneer in the specialty.2 I later learned that he turned down a lucrative offer to become a full-time researcher for Align, preferring to stay true to his values and love of teaching. Dr. Boyd’s integrity and commitment to the profession swayed me, and I agreed to help as a tester. I was certain it would not work well, however, and would not enter the mainstream of orthodontics. As my wife and staff like to remind me, “You are seldom in doubt, but often wrong!”
Since that time, I have had the joy of working with Dr. Boyd on numerous projects, including many years of service on Align’s North American Clinical Advisory Board. He is very persuasive. He convinced me to join the faculty at the University of the Pacific. He taught me how to use and value clear aligners. He constantly challenged me and the entire profession to do more difficult cases with Invisalign. He also taught us how to treat those difficult cases. He paved the way by doing it first. As one example, I noted with considerable interest that Dr. Boyd was experimenting with one-week aligner changes as early as 2003. Even the clinical advisory board of which he is a member has only recently reached a consensus and recommended one-week aligner changes as the standard protocol.
Dr. Boyd’s seminal JCO article on treating complex cases with Invisalign gave an honest assessment of the early challenges we encountered with this new approach. He freely discussed what he believed were contraindications for Invisalign treatment. (In a recent discussion, he shared with me that he believes several of these problems, such as crossbites and arch development, can now be resolved with Invisalign.) He also pointed out situations where Invisalign may be superior to fixed appliances. For instance, he was the first to demonstrate to the profession the benefits of aligners in treating anterior open bites.
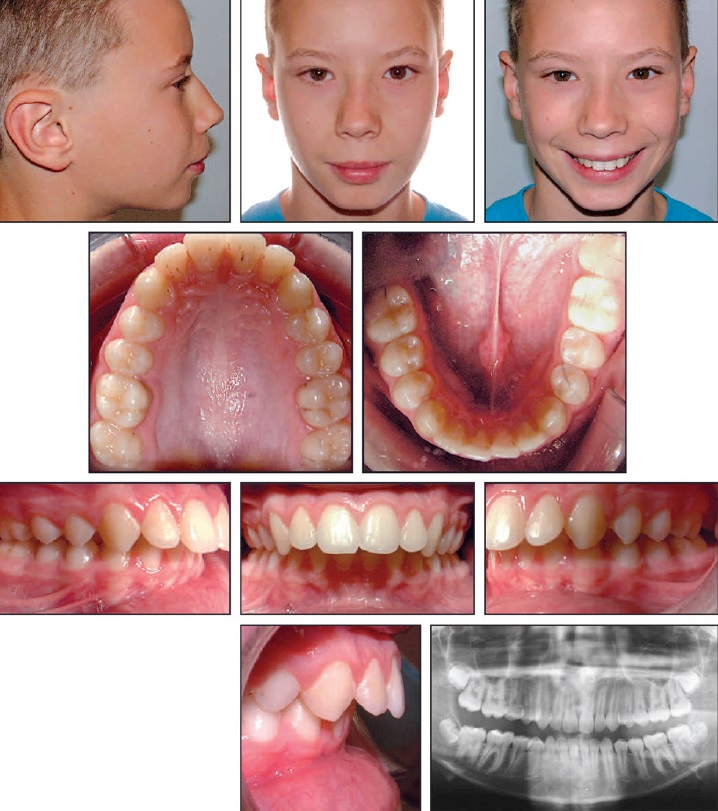
13-year-old male patient with Class II, division 1 malocclusion before treatment.1
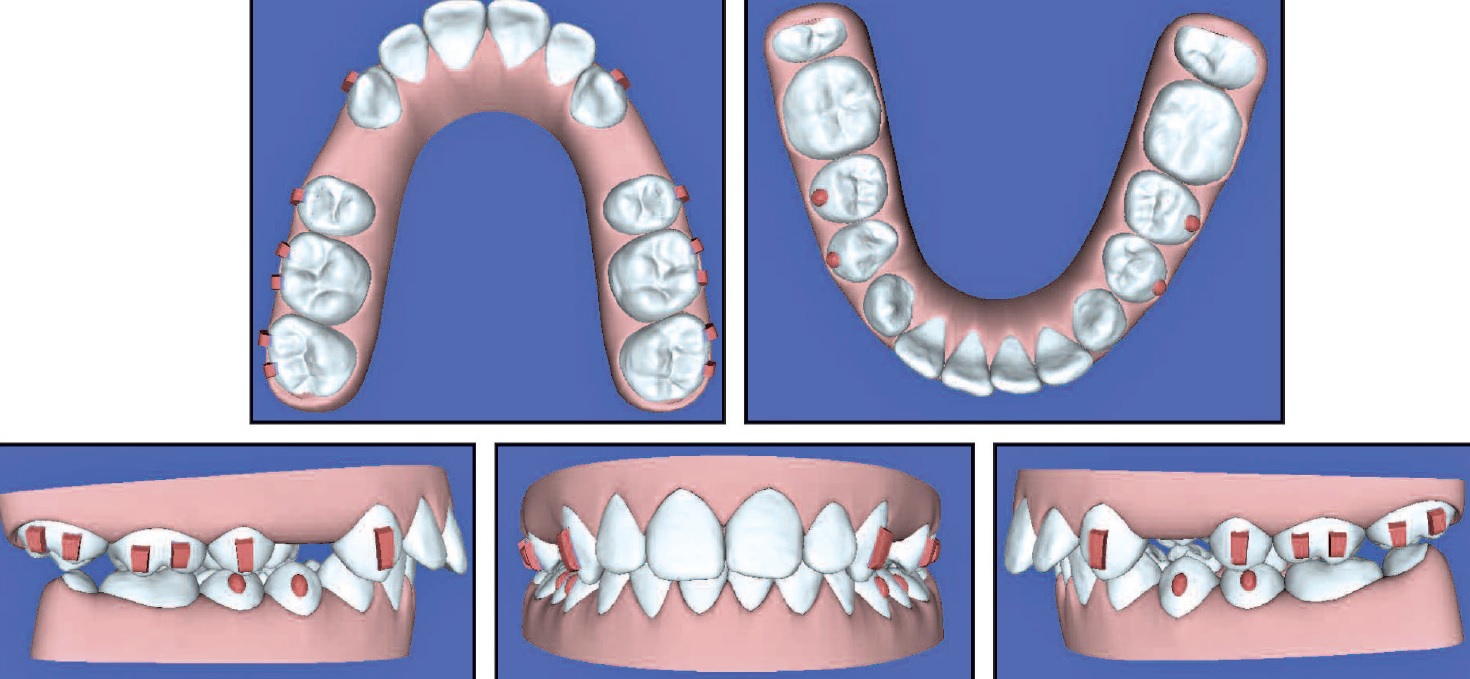
The four cases shown in Dr. Boyd’s article would have been considered difficult and outside the realm of possibility for most Invisalign practitioners. All four were treated to excellent results without the benefits of several subsequent, wonderful innovations from Align: SmartTrack** proprietary aligner material, SmartForce* attachments and features, power ridges for torquing, cutouts for elastics, digital scanning with iTero* vs. physical polyvinyl siloxane impressions, and more. Dr. Boyd believes all of these early patients could be treated more efficiently today, perhaps with different treatment plans. The case reproduced here, he says, could have been treated without extractions in two-thirds of the time.
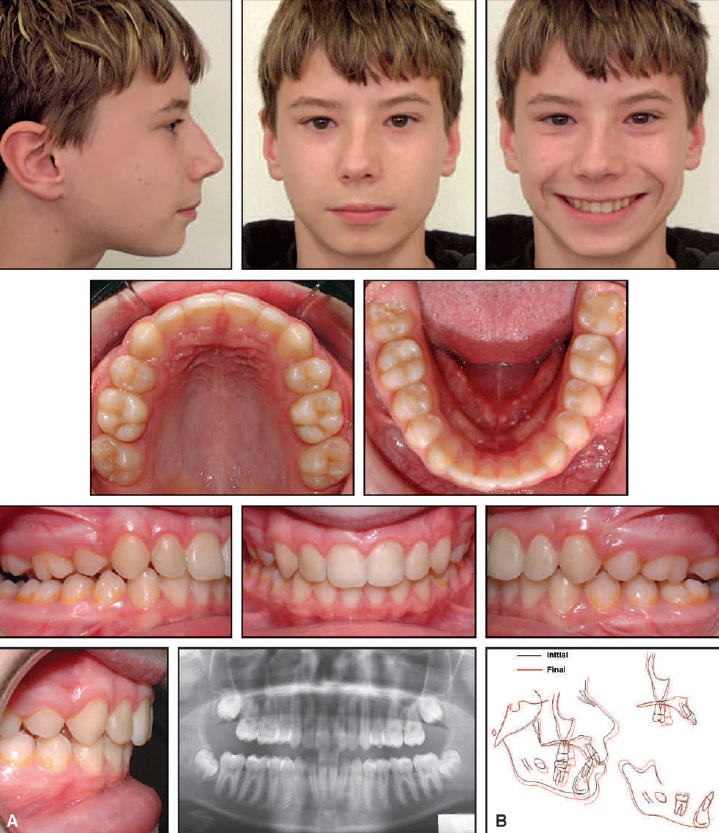
A. Patient after 14½ months of treatment. B. Superimposition of pre- and post-treatment cephalometric tracings.1
This article—which appeared in JCO’s 40th Anniversary Issue—had its share of skeptics and detractors in 2007, but it helped the orthodontic profession see what was possible. It was a challenge to many of us, serving as a reminder that we should not let our biases limit our vision. In terms of historical significance, it may have done for Invisalign therapy what Andrews’s “six keys” did for fixed appliance treatment.
REFERENCES
- 1. Boyd, R.L.: Complex orthodontic treatment using a new protocol for the Invisalign appliance, J. Clin. Orthod. 41:525-541, 2007.
- 2. Keim, R.G.: Game changers in orthodontics, J. Clin. Orthod. 46:257-258, 2012.
-
 DR. FRY
DR. FRY
Dr. Fry is an Adjunct Clinical Professor of Orthodontics at the University of Southern California, Los Angeles; University of the Pacific, San Francisco; and New York University, New York City, and in the private practice of orthodontics at Fry Orthodontic Specialists (www.fryorthodontics.com), 11940 Quivira Road, Overland Park, KS 66213; e-mail: bobfryortho@gmail.com.