Physiological Drifting of Ectopic Canines
The prevalence of ectopically erupted teeth is reportedly 1-2.2%.1-3 Ectopic eruption of the permanent maxillary canines has been attributed to a wide range of systemic factors such as endocrine deficiency and febrile diseases; environmental factors such as a long path of eruption and disturbances of the unerupted follicle; and local factors including lack of space, abnormal lateral-incisor root position, early loss of deciduous canines, and root dilaceration.4
Space can be gained for an ectopic canine by methods such as interproximal reduction, lateral expansion, and molar distalization.5 If first premolars are extracted, the canine can be moved distally and occlusally using loop or continuous-arch mechanics, but this approach creates a risk of dehiscence and gingival recession.6,7 As an alternative, the canine can be allowed to drift into the premolar extraction space. Physiological drift is defined as the natural migration of a tooth into a space created by extraction, congenital absence, decay, or interproximal reduction without the application of any orthodontic force.8 Spontaneous decrowding of teeth by physiological drift has been called “driftodontics”. Judiciously timed removal of teeth can thus enable desirable eruption and alignment of the permanent dentition, possibly avoiding or minimizing the need for future orthodontic treatment.9
This article describes two cases of buccally displaced canines that were resolved by physiological drift after premolar extractions.
Similar articles from the archive:
Case 1
A 15-year-old female presented with the chief complaint of irregular upper and lower front teeth. Clinical examination showed a convex profile, a high FMA, potentially competent lips, and a Class I molar relationship, with anterior crowding and ectopic canines in both arches (Fig. 1).
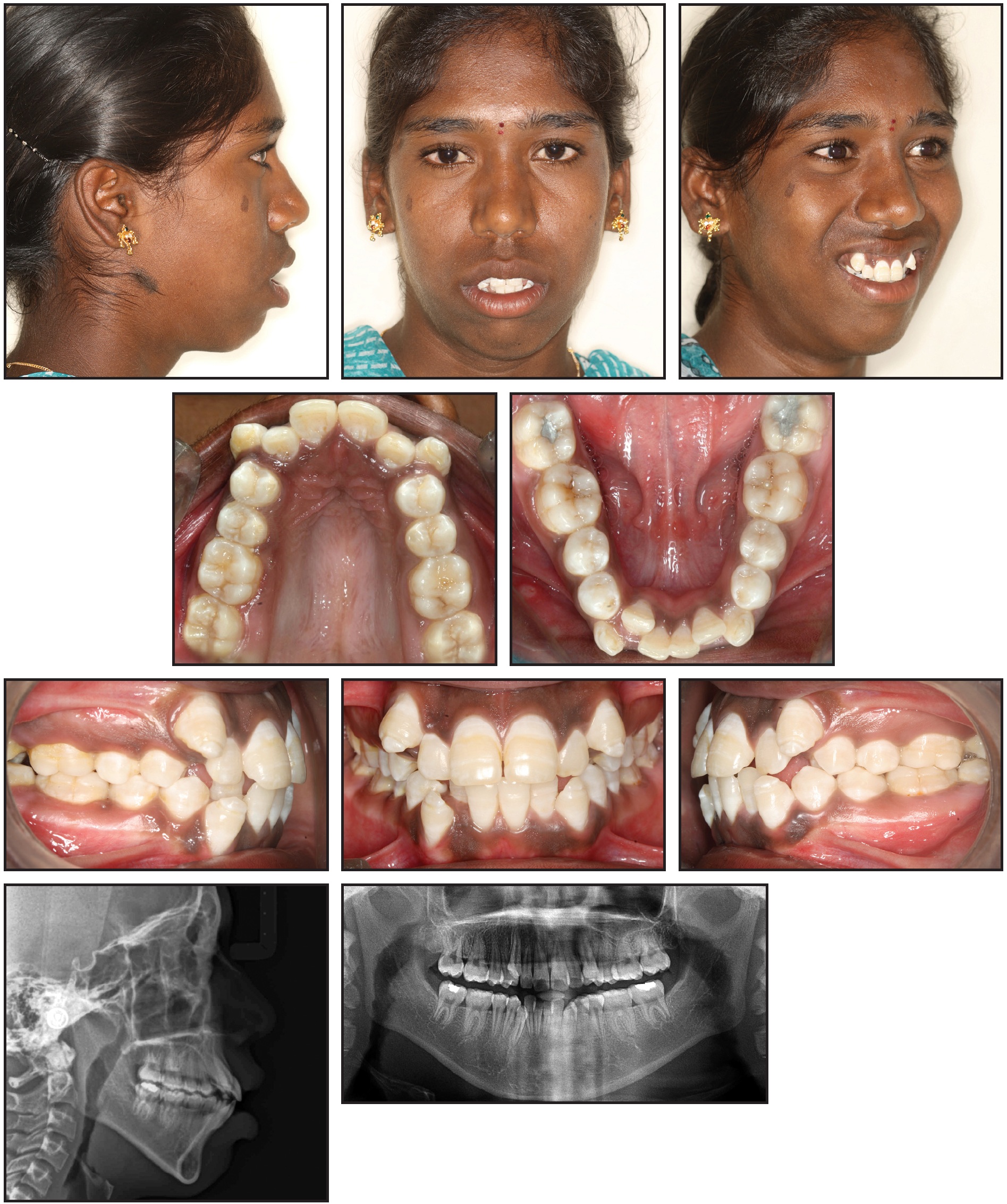
Fig. 1 Case 1. 15-year-old female patient with bilateral Class I molar relationship, anterior crowding, and ectopic canines in both arches before treatment.
Cephalometric analysis indicated skeletal Class II bases (ANB = 5°) and a hyperdivergent growth pattern (GoGn-Sn = 38°, FMA = 38°). The upper and lower anterior teeth were proclined (U1-SN = 111°, U1-NA = 28°/7mm, IMPA = 95°, L1-NB = 37°/13mm).
Considering the patient’s age, profile, and arch discrepancy, we decided to extract all four first premolars, followed by driftodontics with group A anchorage in both arches. Fixed mechanotherapy would involve .022" MBT* appliances and a transpalatal arch.
All teeth except the ectopic canines were bonded. The incisors were aligned with segmental mechanics on .014" and .016" nickel titanium archwires, and the canines were allowed to drift into the extraction spaces without any direct force application (Fig. 2).
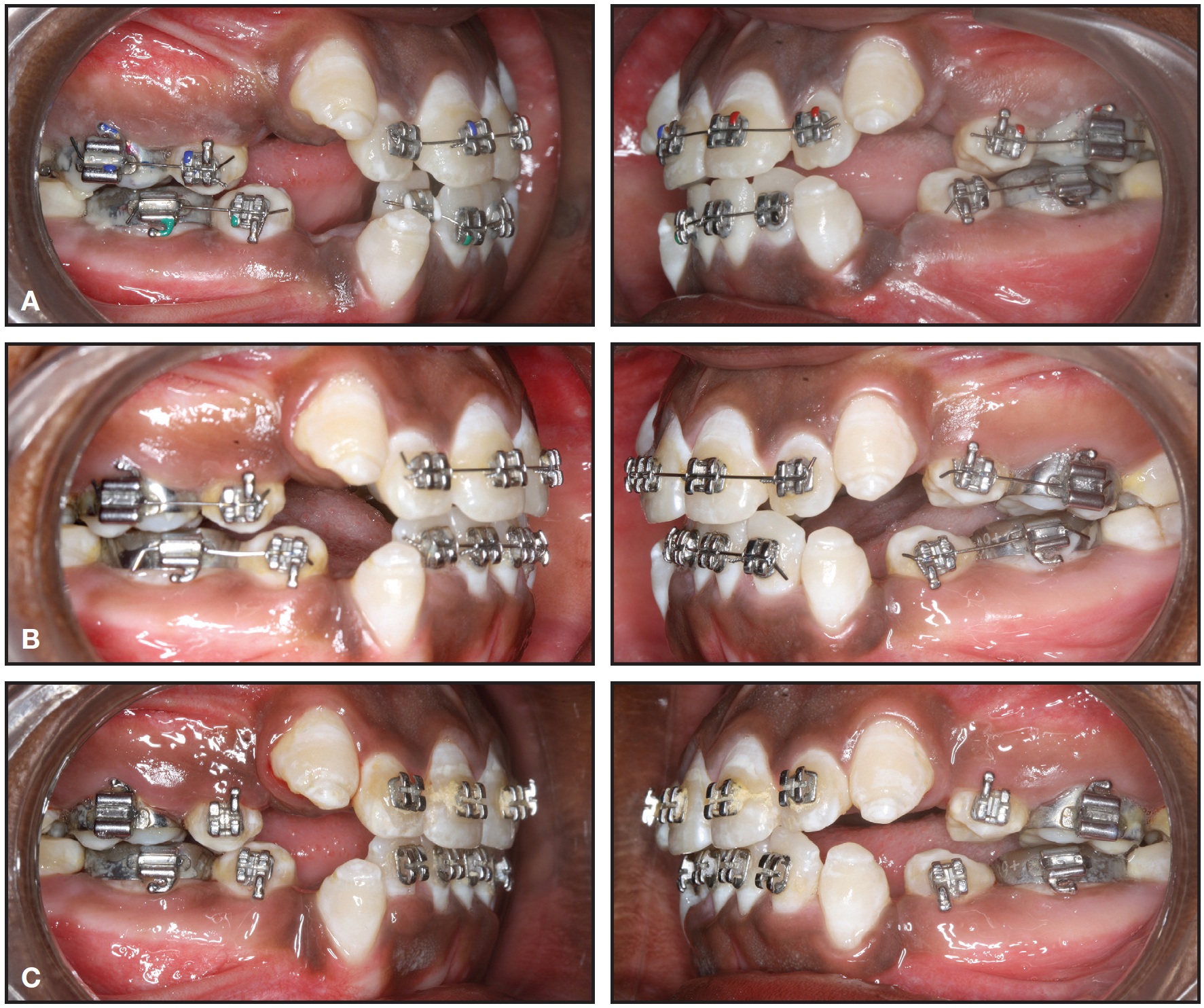
Fig. 2 Case 1. Sequential drifting of canines after one (A), three (B), and five (C) months of treatment with MBT* fixed appliances, transpalatal arch, and nickel titanium archwires.
After five months of treatment, the canines had erupted into position, and a continuous .016" nickel titanium archwire was placed. Leveling was completed using .016" × .022" nickel titanium and .016" × .022" and .017" × .025" stainless steel archwires. Space closure was accomplished with sliding mechanics on .019" × .025" stainless steel archwires. Finishing, detailing, and settling were carried out using .014" stainless steel archwires and red elastics (3⁄16", 3.5oz).**
Total treatment time was 18 months. The patient finished with ideal overjet and overbite and Class I molar and canine relationships (Fig. 3A). Superimposition of pre- and post-treatment cephalometric tracings showed a near-normal inclination of the upper and lower anterior teeth (ANB = 5°, GoGn-SN = 41°, FMA = 40°, U1-SN = 102°, U1-NA = 21°/4mm, IMPA = 87°, L1-NB = 28°/7mm), with a slight improvement in lip competency and a mild change in the vertical relationship (Fig. 3B). Fixed upper and lower 5-5 lingual retainers were bonded.
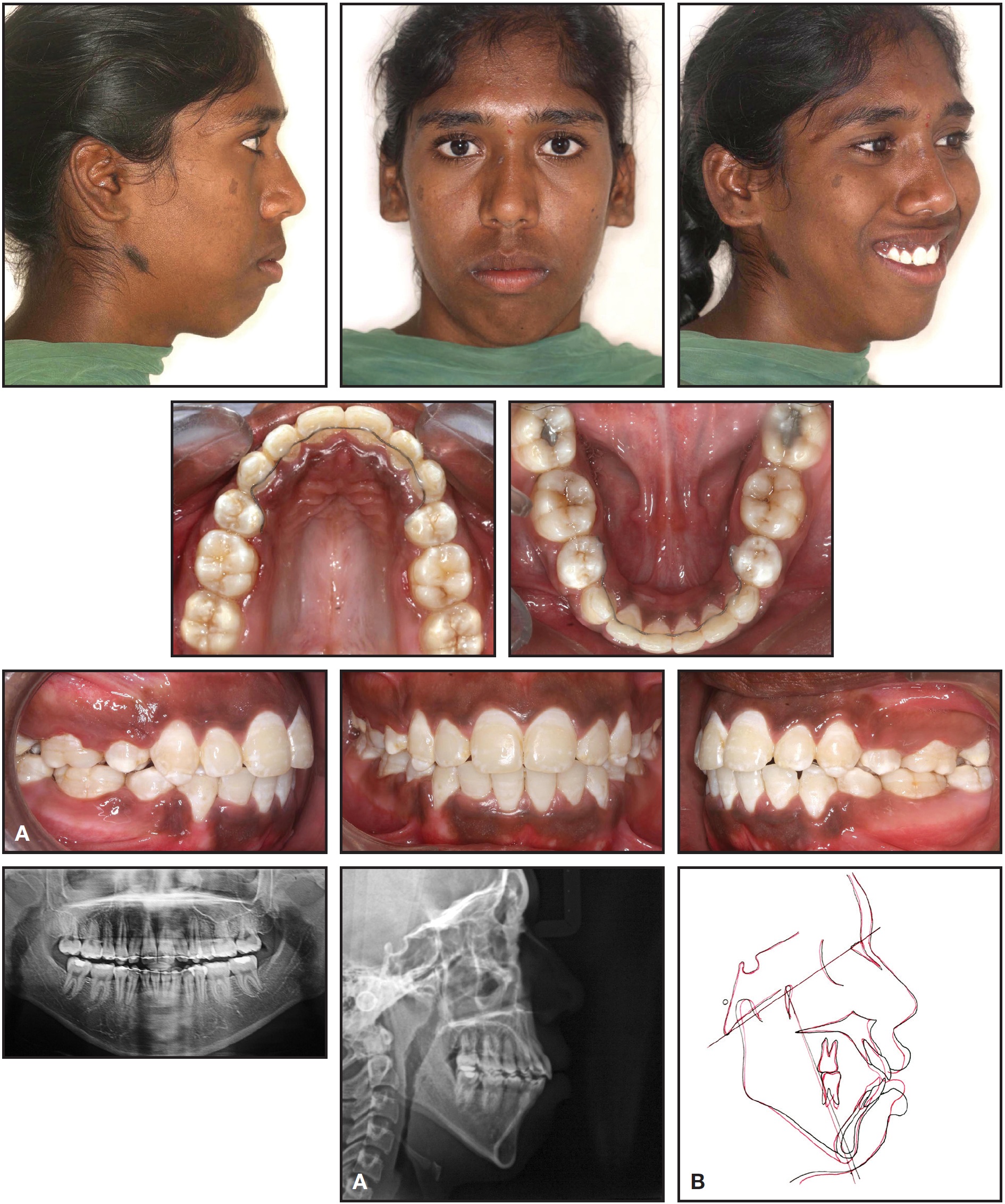
Fig. 3 Case 1. A. Patient after 18 months of treatment. B. Superimposition of pre- and post-treatment cephalometric tracings.
Case 2
A 16-year-old male presented with the chief complaint of irregular upper front teeth. He had a convex profile with a normal FMA and potentially competent lips (Fig. 4).
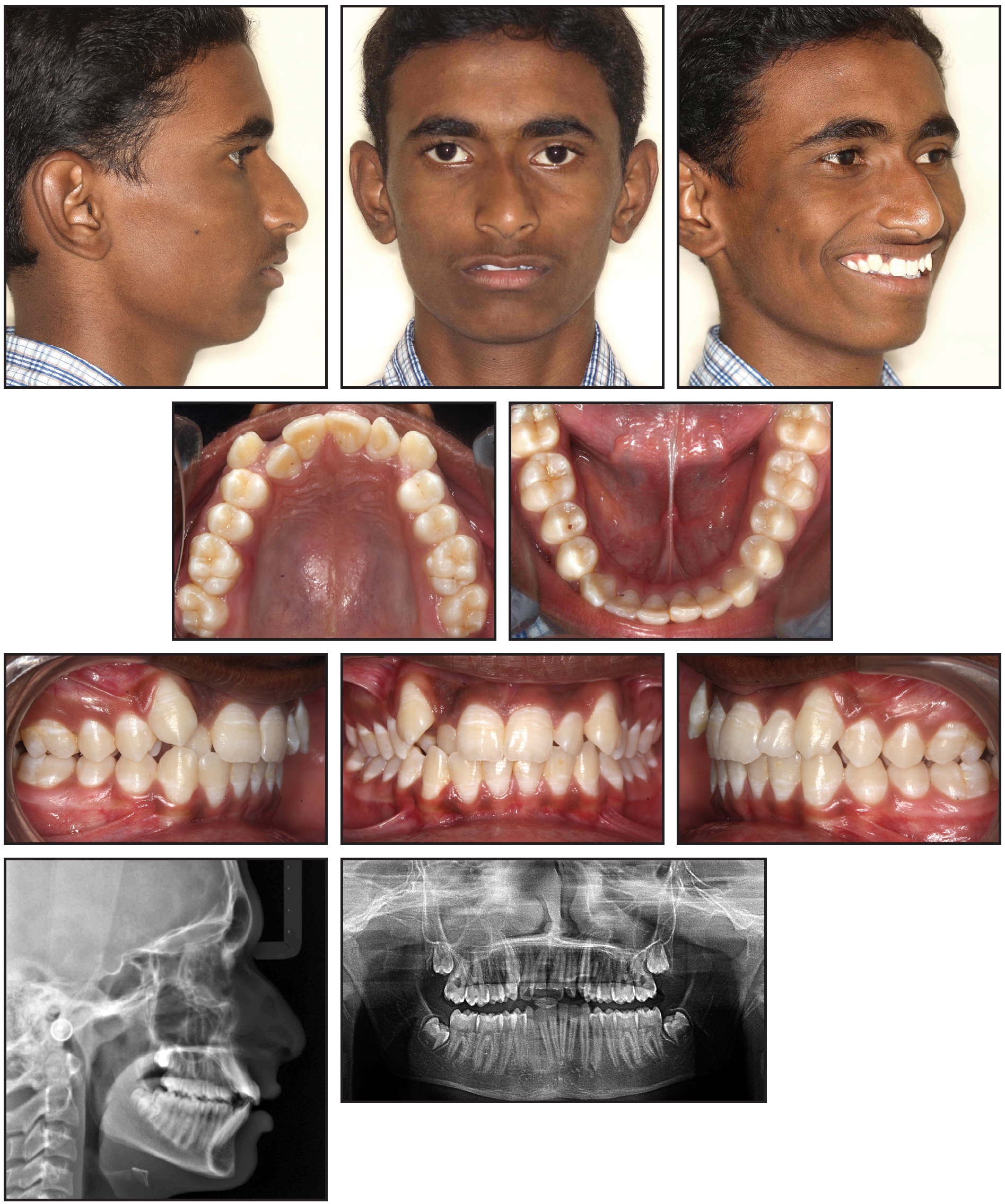
Fig. 4 Case 2. 16-year-old male patient with bilateral Class II molar relationship, severe upper crowding with ectopic canines, and mild lower crowding before treatment.
Intraoral examination revealed a Class II molar relationship with a Class II canine relationship on the left side and an end-on canine relationship on the right. The patient exhibited severe crowding in the upper arch and mild crowding in the lower, with ectopically erupted canines; the upper midline was shifted 2mm to the right, and the upper and lower right lateral incisors were in crossbite. Cephalometric analysis indicated skeletal Class I bases (ANB = 3°) and a normodivergent growth pattern (GoGn-Sn = 31°, FMA = 28°). The upper and lower anterior segments were proclined (U1-SN = 112°, U1-NA = 29°/5mm, IMPA = 101°, L1-NB = 33°/6mm).
The treatment plan was to extract the upper first premolars and use driftodontics with group B anchorage in the upper arch. All maxillary teeth except the canines were bonded with .022" MBT brackets, and the incisors were aligned with segmental mechanics on .014" and .016" nickel titanium archwires. The canines were allowed to drift into the extraction spaces without any direct force application (Fig. 5).
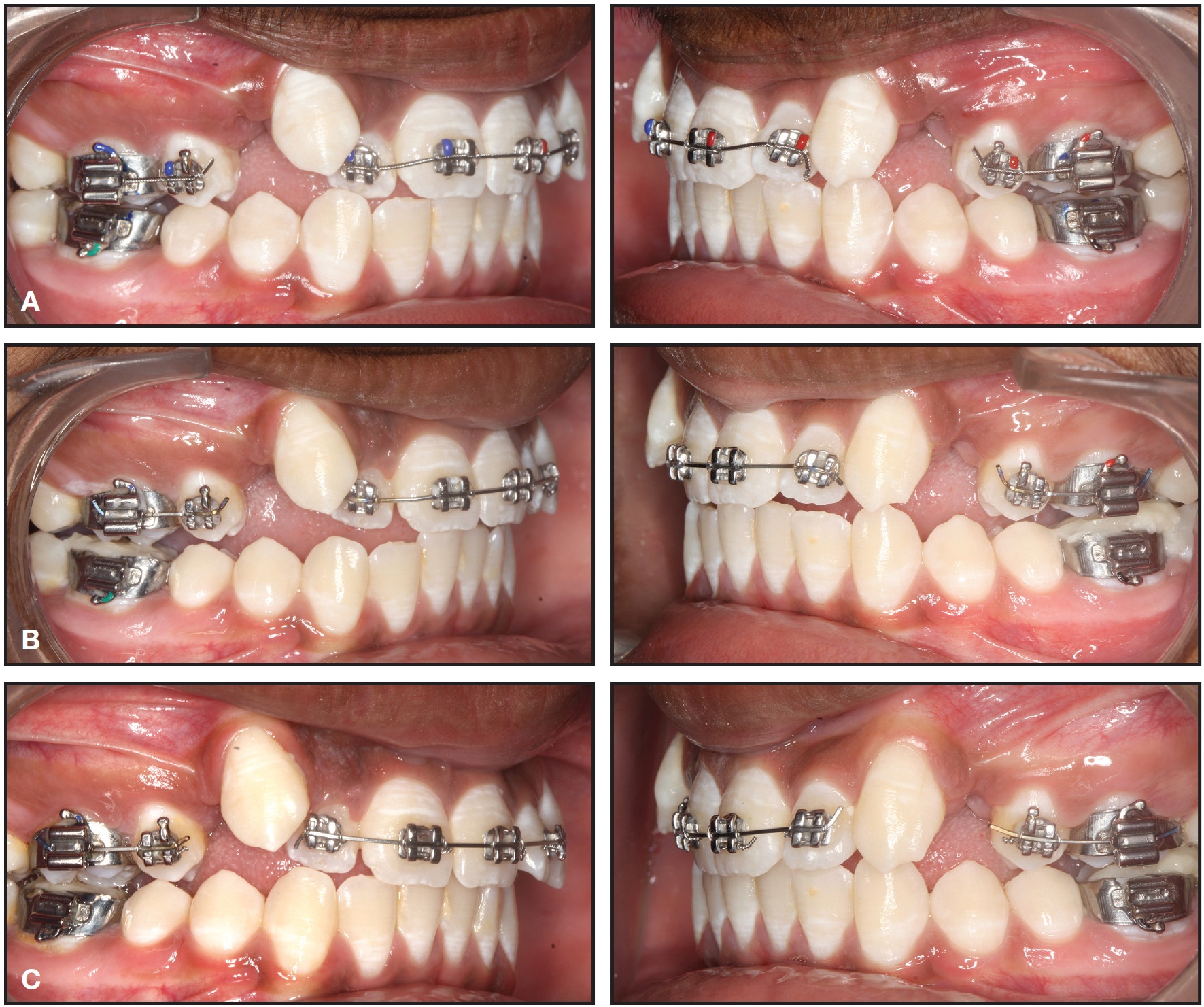
Fig. 5 Case 2. Sequential drifting of canines after one (A), two (B), three (C) months of treatment with MBT fixed appliances, transpalatal arch, and nickel titanium archwires.
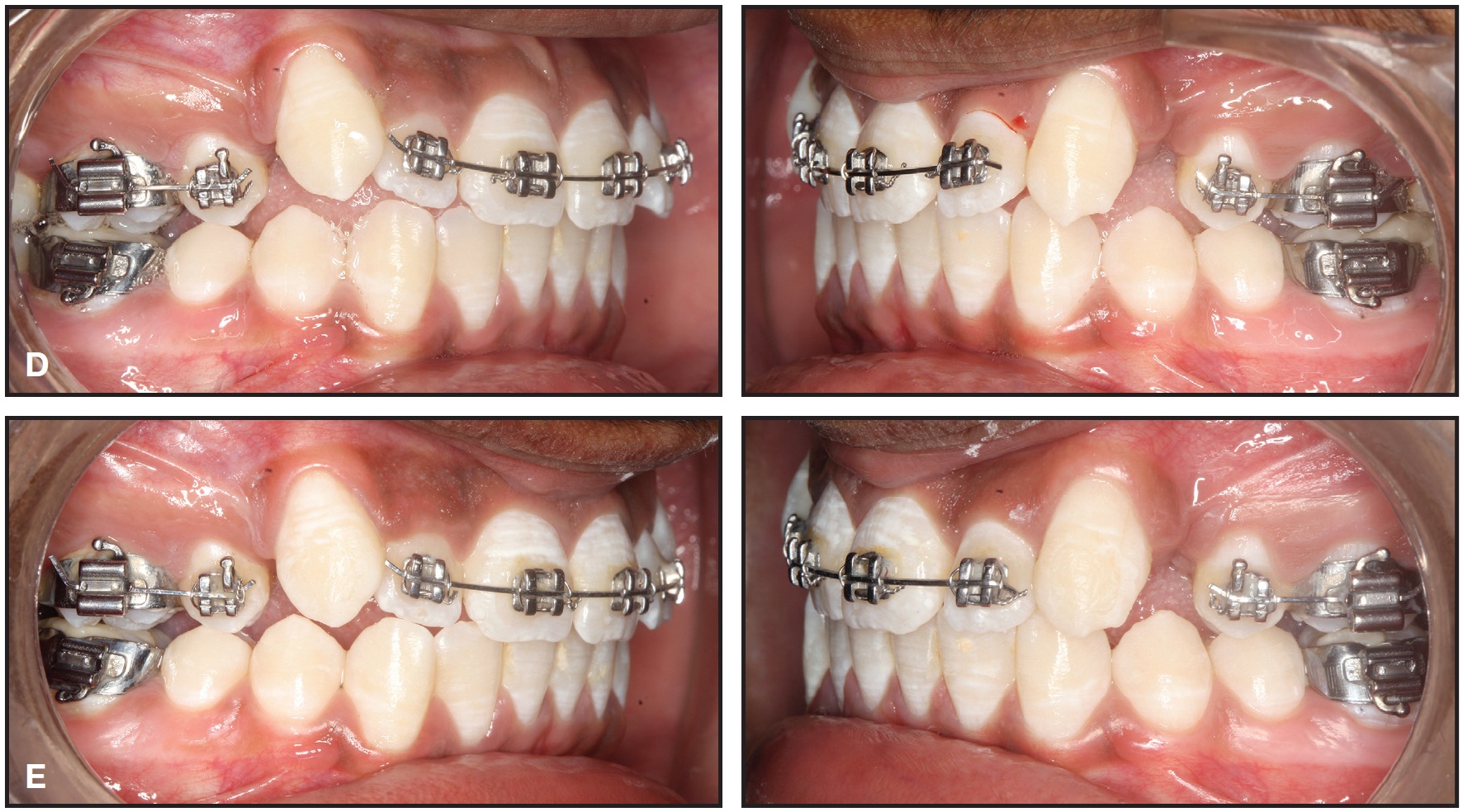
Fig. 5 (cont.) Case 2. Sequential drifting of canines after four (D) and five months (E) of treatment with MBT fixed appliances, transpalatal arch, and nickel titanium archwires.
After five months of driftodontics, the upper canines and lower arch were bonded. Leveling and alignment were carried out using .014", .018", and .016" × .022" nickel titanium and .016" × .022" and .017" × .025" stainless steel archwires. Space closure was completed using sliding mechanics on .019" × .025" stainless steel archwires with Class III elastics. Finishing, detailing, and settling were accomplished using .014" stainless steel archwires and red elastics (3⁄16", 3.5oz).
Total treatment time was 18 months. After treatment, the patient had ideal overjet and overbite, with Class II molar and Class I canine relationships (Fig. 6A). Superimposition of pre- and post-treatment cephalometric tracings confirmed a normal incisor inclination and mesialization of the upper molars (ANB = 3°, FMA = 28°, GoGn-SN = 29°, U1-SN = 104°, U1-NA = 24°/4mm, IMPA = 96°, L1-NB = 30°/6mm) and a Class II molar relationship, with no change in the vertical relationship (Fig. 6B). Fixed lingual retainers were bonded, 5-5 in the upper arch and 3-3 in the lower.
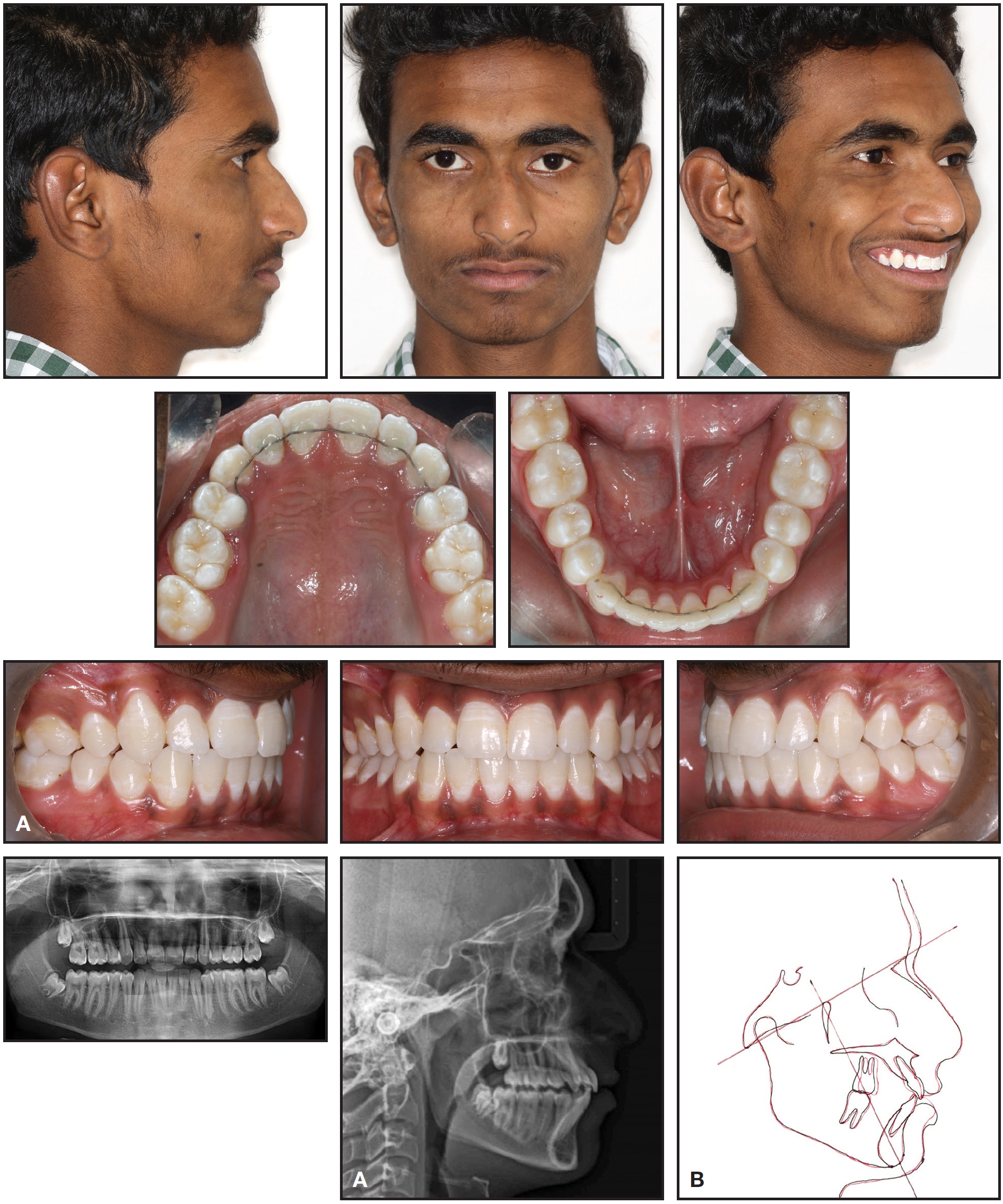
Fig. 6 Case 2. A. Patient after 18 months of treatment. B. Superimposition of pre- and post-treatment cephalometric tracings.
Discussion
Patients with severe anterior crowding and buccally erupting ectopic canines generally require first-premolar extractions. Anchorage control is critical in such cases. The 15-year-old adolescents with mild skeletal discrepancies and average overbites shown in this article are ideal candidates for driftodontics.10 Alexander recommended waiting to bond the lower arch until about six months after extractions to allow time for the lower incisors to unravel and upright.10 This phenomenon was also observed by Creekmore8 and by Papandreas and colleagues.11
The benefits of physiological drift include better occlusal relationships, increased dentoalveolar support, and a shorter period of full appliance therapy. After conventional orthodontic treatment, ectopically erupted canines tend to display increased plaque and gingival bleeding indices, greater pocket depths, reduced attached gingival width, higher gingival levels, increased crown lengths, higher electric pulp test scores, and reduced bone levels.6 The two cases presented here showed no gingival recession, no increase in pocket depth, and a normal thickness of attached gingivae after physiological drifting of the ectopic teeth. Well-aligned arches with proper overjet and overbite were achieved without any damage to the canines.
FOOTNOTES
- *Trademark of 3M Unitek, Monrovia, CA; www.3MUnitek.com.
- **Libral Traders, New Delhi, India; www.libraltraders.com.
REFERENCES
- 1. Bedoya, M.M. and Park, J.H.: A review of diagnosis and management of impacted maxillary canines, J. Am. Dent. Assoc. 140:1485-1493, 2009.
- 2. Fleming, P.S.; Scott, P.; Heidari, N.; and DiBiase, A.T.: Influence of radiographic position of ectopic canines on the duration of orthodontic treatment, Angle Orthod. 79:442-446, 2009.
- 3. Cooke, J. and Wang, H.L.: Canine impactions: Incidence and management, Int. J. Period. Restor. Dent. 26:483-491, 2006.
- 4. Fearne, J. and Lee, R.T.: Favorable spontaneous eruption of severely displaced maxillary canines with associated follicular disturbance, Br. J. Orthod. 115:93-98, 1988..
- 5. McNamara, J.A. and Brudon, W.L.: Treatment of tooth-size/arch-size discrepancy problems, in Orthodontic and Orthopedic Treatment in the Mixed Dentition, Needham Press, Ann Arbor, Ml, 1993, p. 67.
- 6. Evren, A.D.; Nevzatoğlu, S.; Arun, T.; and Acar, A.: Periodontal status of ectopic canines after orthodontic treatment, Angle Orthod. 84:18-23, 2013.
- 7. Chay, S.H. and Rabie, A.B.M.: Repositioning of gingival margin by extrusion, Am. J. Orthod. 122:95-102, 2002.
- 8. Creekmore, T.D.: Teeth want to be straight, J. Clin. Orthod. 16:745-764, 1982.
- 9. Tweed, C.: Clinical Orthodontics, St. Louis, C.V. Mosby Co., 1966.
- 10. Alexander, R.G.: The Alexander Discipline, Ormco Corporation, Glendora, CA, 1986.
- 11. Papandreas, S.G.; Buschang, P.H.; Alexander, R.G.; Kennedy, D.B.; and Koyama, I.: Physiologic drift of the mandibular dentition following first premolar extractions, Angle Orthod. 63:127-134, 1993.
-
 DR. DASARI
DR. DASARI -
DR. KISHORE
-
DR. AILENI
-
DR. BATTULA
-
DR. PRATHIMA
-
DR. RACHALA
Dr. Dasari is an Assistant Professor, Dr. Kishore is a Professor and Head, Dr. Aileni is a Professor, Dr. Battula is an Assistant Professor, Dr. Prathima is a postgraduate trainee, and Dr. Rachala is a Professor, Department of Orthodontics, SVS Institute of Dental Sciences, Mahabubnagar, 509002 Telangana, India. E-mail Dr. Dasari at dr.dasari.arun@gmail.com.