Physiologic Drift
Physiologic drift is defined as the natural migration of teeth, with no applied force, into space created by extraction, congenital absence, decay, proximal grinding, or orthodontic tooth movement.
Physiologic drift is akin to serial extraction in some respects because the advantage of both lies in the amount of self-correction that takes place after teeth are extracted. However, classical serial extraction is limited to Class I malocclusions with arch length discrepancies. Class II malocclusions with arch length discrepancies are usually made worse with serial extraction procedures because mandibular incisors upright lingually when deciduous cuspids are extracted, whereas maxillary incisors may align but seldom migrate lingually when the maxillary deciduous cuspids are removed This usually results in an increase in overbite and overjet. Also, maxillary molars tend to migrate mesially more readily than mandibular molars during serial extraction, thus creating more of a Class I posterior occlusal relationship.
The physiologic drift procedure, by delaying extractions until after the bicuspids erupt naturally, eliminates many of the disadvantages of classical serial extraction, while still gaining the benefits of self-correction.
If teeth are not crowded, there is no particular advantage in letting teeth drift. If they are not crowded in an extraction case, you just extract, band all the remaining teeth, and close the spaces en masse. The physiologic drift procedure applies to any type of arch length deficiency and it is not limited to Class I cases.
When permanent teeth are extracted, the entire case should have been diagnosed and treatment planned so that you know the arch length requirements and the extraoral anchorage requirements, if any. This will tell you how to manage the case while waiting for the teeth to erupt after the extractions. I try to time the extractions so that I have the least wait for teeth to erupt and yet time for optimum drift to take place. That time is when the teeth that you want to drift are just erupting into the mouth.
Physiologic drift is predictable and unfavorable drift is easily controlled. If you extract first bicuspids, the cuspids migrate distally into the extraction site. Or if you extract second bicuspids, the first bicuspids drift distally rapidly, the cuspids will follow, and the incisors-- especially the lower incisors-- will go lingually. There is not a great deal of migration in the lower molar, although it will vary from case to case. If the upper molar is in Class I, you don't have to worry about maintaining it. It will stay Class I. If it is end-on or Class II and the cuspids are end-on or Class II, then you'd better put in some form of space maintainer to keep the upper molar from drifting forward.
If the cuspids are not showing at all, it might take a year to a year and a half for them to erupt. I don't like to have bands on for that period of time, so I prefer a Nance palatal button on the upper
(Fig. 1), or a lingual arch on the lower to hold arch length. If you think anchorage is critical, maintain the space in some way. It is a lot easier to maintain space than to recover it later.
Case 1
A palatal button was used to maintain space in this case.
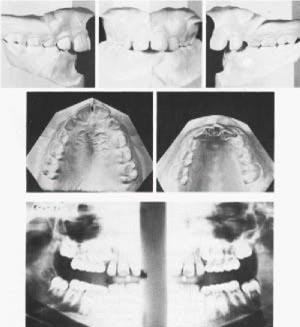
This boy was 10 years 5 months of age with a Class II malocclusion with all four cuspids blocked completely out of each arch (Fig. 2).
The panorex showed maxillary first bicuspids erupting toward the palate and limited root resorption of the maxillary deciduous first molars, while mandibular deciduous first molars were about to be shed. Mandibular cuspids were erupting slightly earlier than first bicuspids, which occurs about one-half of the time. Their cusp tips could be seen erupting beside the laterals.
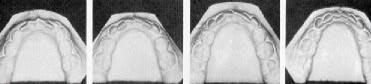
In August 1973, the maxillary deciduous first molars and mandibular first bicuspids were extracted and a palatal button holding arch was placed to maintain maxillary arch length. A progress model (Fig. 3) and a panorex taken in December 1973 demonstrate 3½ months drift of the mandibular cuspids. Even though the cuspids had begun eruption, they still drifted distally very rapidly. Often I have been asked why this drift occurs. Is it the occlusion? transeptal fibers? musculature? So far, my answer is still, "I don't know why--it just happens--and you can count on it!"
After 7 months of drift another progress model was taken (Fig. 3). In November 1974, four months later, after a total of 15 months of drift, the mandibular deciduous second molars had been shed and the second bicuspids and second molars had erupted (Fig. 3).
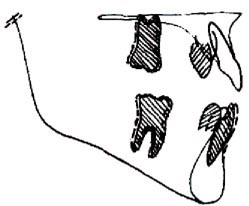
Superimposed cephalometric tracings of the mandible show the lower incisors have drifted lingually about 2mm, but have erupted very little (Fig. 4). Superimposing on the maxillary central incisors (Fig. 5) shows the overjet and overbite have increased due to the lingual movement of the lower incisors and continued eruption of the upper incisor. The contour of the lips has also gotten worse. However, completion of treatment for this patient now is immensely easier than it would have been had I waited until all the teeth erupted before extracting.
Case 2
Here is another case in which a palatal button was used.
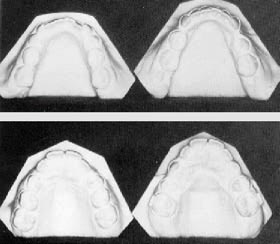
This was a girl 10 years and 8 months of age (Fig. 6).
On the upper right side there was about 2mm of space between the lateral and the deciduous first molar, with only a bit of extra space on the anteriors. Cuspids were pretty well blocked out. Lower cuspids were overlapping 2-2½mm. So, we took out all four first bicuspids, put in a palatal button and waited. In a year's time, look what drift has done (Fig. 7).
In this case I probably would have been better off without the palatal button and losing a little space. Look at the lower E space. The anteriors have aligned perfectly, yet there is still that much space. The difference between a deciduous second molar and a bicuspid is tremendous. Many men don't realize how much E space is. We were taught that there is 1.7mm of E space or leeway. But, the average deciduous second molar is 10mm and the average bicuspid is 7mm. That's a lot of difference Deciduous first molars are almost 8mm wide and first bicuspids average 7mm, so there is almost another millimeter there. If both first and second deciduous molars are in place, you can have almost 4mm of extra space on each side. The deciduous cuspid is about 5mm and the permanent cuspid 7, so you lose 2mm on that. Many times you will see a case in which the deciduous cuspid has been removed and you'll see 2-3mm space between the lateral and deciduous first molar. You'll think that this case is really going to be crowded. You extract bicuspids and you've got a 7mm space to close afterward and you wonder what happened.
There is a very strong distal component which you see here. The cephalometric superimposition (Fig. 8) showed that the cuspids and lower anteriors backed up. There was a millimeter of mesial movement of upper and lower molars, so posterior segments don't all just drop forward into the extraction space. This was like a classical serial extraction case, but it was picked up after the first bicuspids had erupted. It is not necessary to get in early and extract deciduous first molars to hasten eruption of the first bicuspids so that they can be extracted sooner. You get the same distal drift of the cuspids anyway.
Case 3
In this case, a lower lingual arch was used to maintain space.
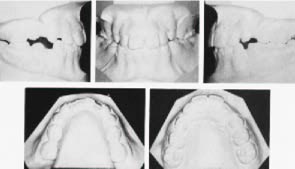
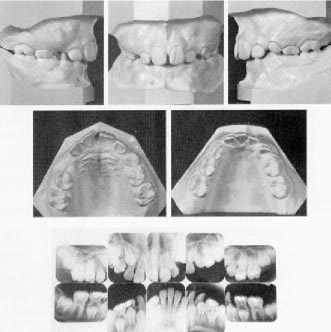
This boy was 10 years and nine months old with arch length discrepancy in both upper and lower arches (Fig. 9).
The upper cuspids were completely blocked out. The lower right lateral was almost touching the deciduous second molar. The bulge you see is the first bicuspid and the pencil mark next to it is the lower right cuspid which could be palpated labial to and between the central and lateral incisor roots. If the cuspid were to erupt in that position it would be a real problem to get it into position and might mean a cuspid extraction.
To avoid that, my plan was to move the lower incisors forward and to the left. This position would be retained with a fixed lingual arch and mandibular first bicuspids would be extracted when they erupted.
Maxillary first bicuspids would be extracted as soon as both have erupted and the maxillary teeth allowed to drift unrestrained. In the second phase of treatment, final space closure, tooth positioning and interarch relationships will be attained with the New Torqued Appliance.
First Phase
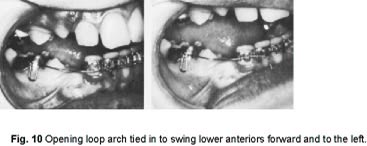
Mandibular incisors and first molars were banded (1/70) and an opening loop arch was inserted to open the space in the lower right quadrant by swinging the incisors around the midline (Fig. 10).
Maxillary first bicuspids were extracted (2/70).
After ten months, the mandibular bands were removed and a lingual arch was placed to retain the lower incisors. A hook was placed to the distal of the incisors to keep them from drifting distally while waiting for the eruption of the cuspids.
Mandibular first bicuspids were extracted (2/71).
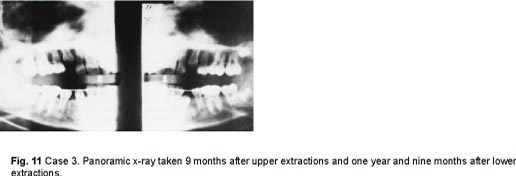
A panoramic x-ray was taken (11/71) nine months after the lower first bicuspids were extracted and a year and nine months after the uppers were extracted, to evaluate eruption of the cuspids (Fig. 11). See where the cuspids have gone.
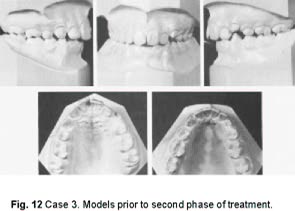
The mandibular lingual arch was removed and models were taken (1/ 72) in preparation for the second phase of treatment (Fig. 12).
Nothing has ever been on the upper. This is two years after extracting upper first bicuspids and one year after extracting lower first bicuspids. The molar relationship on the right side remained Class I; the molar relationship on the left side showed unfavorable mesial drift of the upper molar as a result of early loss of an abscessed deciduous second molar. It is interesting that the lower right cuspid, which we were most worried about, erupted in the best position Of course, the upper incisors were still irregular, bicuspids rotated and molars tipped. A second phase of orthodontic treatment was needed, but it is obvious to see the benefits of physiologic drift in this case. It would have been a most difficult case if extractions were delayed until all permanent teeth had erupted. Yet, I did not have to go in early. I did not have to extract first deciduous molars. I waited for the first bicuspids to erupt on their own before extracting them. And, the cuspids still drifted into the space.
Second Phase
The second phase of treatment was made quite easy by the first stage procedures. The maxillary teeth were banded with the New Torqued Appliance in July 1972; mandibular teeth were banded in October 1972. When both arches were in .018 X .025 finishing archwires, strong Class II elastics were worn for seven weeks, 24 hours a day and then another six weeks at night only, to correct the molar relationship. No headgear was used. All bands were removed at the same time in August, 1973. Hawley retainers were used for retention (Fig. 13).
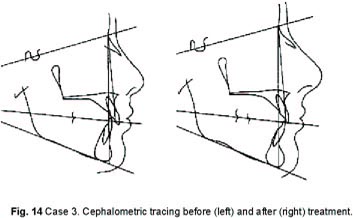
The tracings also show a satisfactory result (Fig. 14).
Bands were on the teeth in the second phase of treatment for 10 months on the lower and 13 months on the upper. This would have been a tough or maybe an impossible case if I had waited for complete eruption of the permanent teeth before extracting.
I don't call this serial extraction, because nothing was done serially. I waited for the deciduous teeth to fall out naturally and then extracted first bicuspids. There was still plenty of time for the cuspids to drift back into position. But I want you to see that you are not limited to this particular extraction timing for favorable drift. Many times we don't see the patient until the cuspids have erupted but they will still drift distally if given the opportunity, as will be seen in the next case.
Case 4
Here is a case where the cuspids were erupted (Fig. 15). The previous case would have been worse than this. But, you really don't want to wait until they get like this if you have a choice. If the patient comes in like this, you don't have that choice any more, but you can still treat them in the same way and still take advantage of drift. This boy was 11 years 6 months old, with a full Class II.
The upper cuspids were blocked out and high, and there was a mild arch length discrepancy on the lower arch. Maxillary first bicuspids and mandibular second bicuspids were extracted and treatment began with upper molar bands and a cervical facebow, and lower first molar and first bicuspid bands with closing loop sectional arches. The patient transferred and I asked the orthodontist for a set of models he made at that time (Fig. 16).
The maxillary cuspids drifted into these positions in just five months following the extractions, with no extrinsic force on these teeth whatsoever. The potential for rapid physiologic drift diminishes as the dentition matures and the physiologic drift principle is not as applicable to adult dentitions. If drift is not apparent with in two months, you probably won't get any.
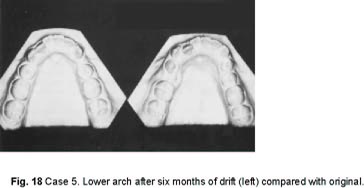
Case 5
If a case requires extraoral anchorage, you can put in a palatal button and start a facebow. In this way, you can be working on orthopedic movement of the upper denture, while waiting for the cuspids to drift into the extraction site. I happen to prefer a cervical or high pull facebow off of the first molars for this. If you like the kind of headgear that comes off the archwire, you can band the four incisors and two molars. The archwire will preserve arch length while you are waiting for teeth to erupt and provide the purchase point for that type of headgear.
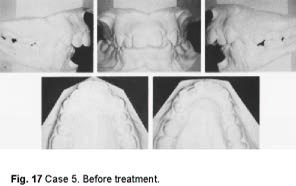
Here is a boy 12 years 4 months old with a full Class II and crowding in both arches (Fig. 17).
We extracted the four first bicuspids and started treatment on the upper arch with molar bands and a cervical facebow. I want to correct the Class II relationship by holding the maxillary denture back and without moving the lower incisors forward. That takes time for the patient to grow--about two years worth--much longer than it takes to treat the lower arch. So, while that is happening, I just let the lower go--let the cuspids move into the arch and let the incisors upright. Comparing the lower arch to the original, after just 6 months of drift (Fig. 18), I doubt if my best treatment procedures could have done as much in the same length of time. One advantage of this approach is that you are setting up the upper arch and if you should want to then set up the lowers with Class III mechanics, you have a firm upper platform to work from.
People ask me if I am not afraid to let things go. Won't the lower molars move forward and use up the extraction space? I think the mesial drift of molars, to the extent that most people envision it, is not a valid concept. We extract and we know the space will close, but do we know how it closes? The prevalent assumption is that the molar does all of the forward movement-- but that is not the case. I don't mean to imply that the molars don't move forward at all, but I can say from the things that I have seen the bicuspids, cuspids and incisors move distally more than the molars move mesially.
Second Bicuspid Extraction Cases
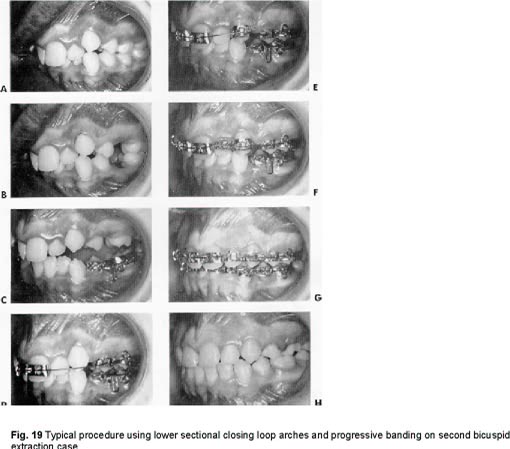
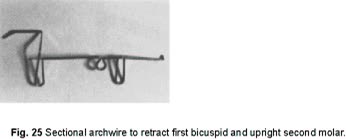
In crowded second bicuspid extraction cases, I band lower first molars and first bicuspids and use a sectional closing loop arch to retract the bicuspid into the extraction space (Fig. 19). The cuspid will follow the first bicuspid distally and the incisors will space and go lingually with no force on them. This is physiologic drift. The second molars will also follow the first molars as they move mesially and that is physiologic drift too. You can close an entire second bicuspid extraction space in this way and have virtually no space in the arch left to close.
The anterior teeth that were crowded and malaligned will correct themselves somewhat as space is provided. The remaining banding, rotations, leveling, and alignment requires no separation and less complicated archwires than are required if all the bands were placed at the beginning of treatment. This method of treatment also conserves anchorage more than the "band all the teeth before placing archwire" technique.
In this sequence of banding, you cannot use the unbanded teeth as markers to let you know what is happening, because they are all drifting and moving in what I term physiologic drift.
In the same situation in the maxillary arch, sectional closing loop archwires are not recommended because the maxillary first molar will tip and roll mesially, resulting in excessive anchorage loss and loss of control unless the molars are stabilized with some type lingual arch or facebow. However, the molars can be controlled without a lingual arch by banding in a different sequence.
Case 6
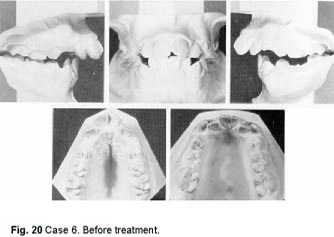
This boy was 9 years 4 months of age, with a full Class II, an open bite, protrusion of maxillary incisors and a moderate mandibular arch length discrepancy (Fig. 20).
The maxillary first bicuspids and deciduous second molars were extracted in December 1972 and a high pull facebow to the upper first molars was started. In June 1973, when the mandibular second bicuspids had erupted, they were extracted. A lower progress model was taken 2½ months later in August 1973 (Fig. 21).
Observe the distal drift of the first bicuspids and cuspids that took place in just 2½ months. No appliance of any kind had been used on the lower arch so far. Lower first molars and first bicuspids were banded at this time and .017 X .022 sectional closing loop arches were inserted to close the second bicuspid extraction sites. In December 1973, a progress model shows continued distal drift of the cuspids and incisor alignment as space was provided by the retraction of the first bicuspids. (Fig. 21).
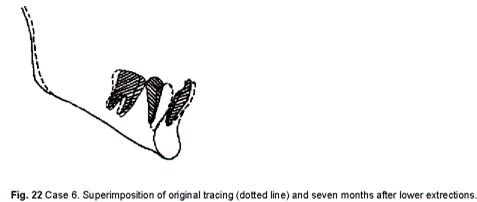
Progress headfilms and superimpositions show the lingual uprighting of the lower incisors (Fig. 22). Now, the rest of the teeth will be banded to finish the treatment.
This is typical and can be expected with this amount of discrepancy handled in this way. The spontaneous alignment of the mandibular anterior teeth may be a little better than usual. The tipping of first molars and first bicuspids apparent at this stage will be automatically corrected by the time the case is finished, by the uprighting and overtipping built into the angulation of the bicuspid and molar attachments in the New Torqued Appliance.
Case 7
The girl was 11 years 8 months old with a class I malocclusion with no arch length discrepancy in the maxillary arch, but with moderately protrusive incisors (Fig. 23).
There was a moderate arch length discrepancy in the mandibular arch complicated-by congenital absence of the mandibular right second bicuspid. Mandibular left second bicuspid was almost horizontal and very immature. Both mandibular second molars were mesially impacted.
In July 1973, the upper second bicuspids and the lower second deciduous molars and left second bicuspid were extracted. Lower first molars and first bicuspids were banded and .017 X .022 closing loop sectionals were used to close the lower extraction sites. After 5 months of drift and 4 months of sectional treatment in the lower arch, progress models were taken in December 1973 (Fig. 24).
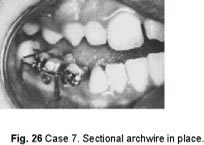
Observe the favorable distal drift of the maxillary first bicuspids and cuspids, and the unfavorable mesial tipping of first molars. Mandibular cuspids have followed the first bicuspids distally. The lower left second molar has erupted into a position that will permit banding later. The right second molar was still impacted and could not be banded so I had a hole drilled in the distal fossa about 1mm deep and large enough to receive an .017 X .022 sectional archwire (Fig. 25). This hole became the tube for insertion of the archwire. The first molar tube was changed to a bracket and a new .017 X .022 sectional opening-closing archwire was inserted to push the second molar distally as the first bicuspid retraction was continued (Fig. 26).
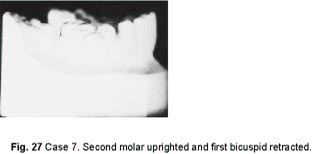
In February 1974, the maxillary first molars, first bicuspids and the incisors were banded and a round archwire was placed. Two months later, a lower progress model was taken (Fig. 24). At that time the rest of the lower teeth were banded including second molars and an .016 leveling arch was placed. Note that it was possible to retract the bicuspid and upright and move the second molar distally using the sectional loop arch with no extraoral anchorage (Fig. 27). Treatment was continued and completed, and bands were removed in January 1975 (Fig. 28).
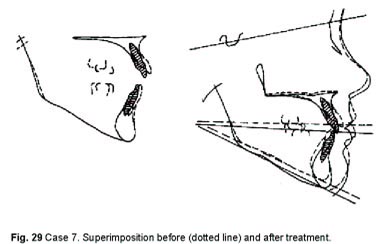
Treatment time had been 16 months on the lower and 11 months on the upper. The results and the treatment time should speak for themselves. Lower molar anchorage is also demonstrated and what to expect regarding anchorage in second bicuspid extraction cases. The crowding was resolved and the incisors were retracted about 2mm with no extraoral anchorage (Fig. 29).
Utilization of physiologic drift and a highly efficient appliance will enable the orthodontist to treat more patients faster, with fewer chairs and fewer auxiliary personnel.
Free Drift With No Space Maintenance
The kind of case in which you don't have to worry about holding space is a Class I case with a little extra space after extraction and a nice face. It is not a critical anchorage situation. You are not trying to retract anterior teeth much. Usually in this kind of a case, I extract when the bicuspids have just erupted and let the remaining teeth drift with no space maintenance at all. I then go in and progressively band all the teeth to finish it. This makes treatment easier, faster and more stable. Teeth that are not allowed to erupt into crowded positions do not have the same relapse tendency as those that fully erupt into malpositions and are then mechanically corrected.
Case 8
Here is a girl 8 years 11 months of age (Fig. 30). There is a Class II molar relationship on the right side; a Class I molar relationship on the left side; and both cuspids were in a Class II relationship. There is quite a difference in the available space on the two sides, because the lower posterior segment on the left side has drifted forward as well as the upper. The lower left deciduous second molar is retained and the first bicuspid is trapped by it.
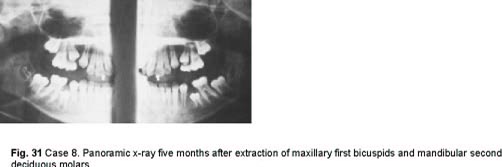
Maxillary first bicuspids and mandibular second deciduous molars were extracted Jan. 1972. No space maintenance was placed in either arch. A panoramic x-ray was taken five months later to evaluate eruption (Fig. 31).
Maxillary cuspids had already drifted distally into a very favorable position. Mandibular first bicuspids had also erupted distally trapping the second bicuspids under them. Ten millimeters of second deciduous molar space is down to about three millimeters, mostly from the first bicuspids coming up and back.
So, here is an important diagnostic criterion. In a situation such as this, if second bicuspids are the extractions of choice, they should be removed when the second deciduous molars are extracted. Otherwise, as we see here, it is impossible to extract second bicuspids without going in through the buccal or lingual in a difficult surgical procedure. So, in this case, although the extraction of lower second bicuspids was what I had in mind, the lower first bicuspids were extracted instead. So, what did I learn from this? In a crowded situation, if first bicuspids are erupting considerably ahead of second bicuspids and second deciduous molars are lost or removed, the first bicuspids will drift distally rapidly, trapping the second bicuspids beneath them. Still no space maintenance was used in either arch, a mistake that is obvious later. An upper progress model was taken 14 months after the upper bicuspids had been extracted (Fig. 32).
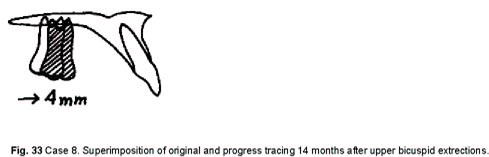
The cuspids have come into the space beautifully, but we have lost a lot of arch length. When you look at the headfilm, before and progress superimposition shows that the molar came forward about 4 mm in the 14 months (Fig. 33).
This demonstrates that the upper arch is different from the lower. Maxillary cuspids drift distally very favorably, however the incisors do not. They maintain their antero-posterior position and arch length is lost by the molars moving forward. In this case, the lost arch length was satisfactory leaving very little space to close, but the Class II condition was worse and still remained to be corrected.
In situations like this, with an end-on or Class II molar relationship where the end result of treatment will have a Class I molar relationship, the molar position should be maintained to prevent the undesirable mesial drift. A Nance palatal button is very satisfactory for this purpose.
Treatment
In November 1972, mandibular anteriors and first molars were banded.
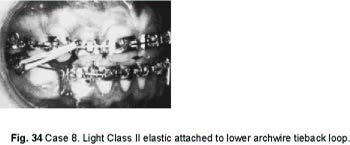
In March 1973, maxillary teeth were banded and a cervical facebow started. With no space to close in the upper arch, the archwire sequence was .016 round, .018 round, and than an .018 X .025 rectangular finishing arch. While waiting for the lower bicuspids to erupt, I went ahead with an .017 X .022 closing loop arcnwire in the lower. With this setup, I can close an entire lower extraction site by bringing the lower posterior segments forward. A light Class II elastic is not strong enough to move the upper teeth stabilized with the .018 X .025 arch, but it is the optimum force to move a lower molar forward.
The light elastic with a 4-ounce pull is attached to the lower archwire tieback loop (Fig. 34).
There is an important difference where the elastic is attached. When a closing loop archwire is activated, it produces a mesial force on the molar and a lingual force on the anterior teeth. If the elastic is attached to the molar, it will continue the mesial pull on the molar, but will never negate the lingual pull on the anteriors and they will continue to go lingually. With the elastic hooked to the archwire tieback, it will move the anteriors forward again after the loop has expended itself. With this approach, a lower molar can be moved forward 10mm if you wish, unilaterally or bilaterally, with practically no effect on the upper arch. You can burn lower anchorage in this way and then turn around and move the upper posterior segments forward with the same approach. First stabilize one and then the other. Spaces do not necessarily have to be closed on the arch that you want to stabilize. You just preserve arch length by setting the stops on a rectangular archwire and you can pull all day long with a 3-4 ounce elastic and the stabilized arch won't go anywhere.
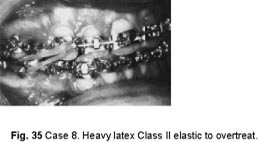
At the end of treatment, using a very heavy Class II elastic, I overdo the Class II correction (Fig. 35).
The elastic is a ¼-inch heavy latex elastic with 10-12 ounces of pull. It sets the teeth right on top of each other with the mandible as far retruded as it will go. That's the way I like to finish cases.
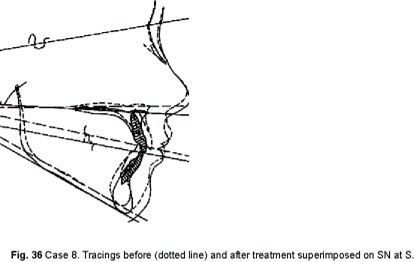
Here are the before and after tracings superimposed on SN at S (Fig. 36).
Treatment time in this case was 20 months on the lower and 16 months on the upper (Fig. 37).
Here's one where the occlusal plane tipped down in back. Mandibular plane held steady even with the use of cervical headgear and Class II elastics. When you superimpose maxilla on maxilla, it looks as if the upper incisors were depressed a couple of millimeters. She certainly didn't come out with a gummier smile (Fig. 38).
We had a nice favorable change between the upper and lower dentures and, if we look at the lower, we find that the lower incisor roots came lingually just a bit. See how ANS moved down. It would seem as if we tipped the palatal plane down a bit in front. But, the nose moved down the same amount as ANS, which carries the lip down the same amount. This shows that what some are saying about cervical headgear tipping the palatal plane and making a gummier smile is not true in this case. A gummier smile is produced by elongating the incisor relative to the maxilla, since anterior nasal spine moved vertically with the nose and upper lip. If you evaluate the incisor-lip line, the incisor is farther up under the lip than it was in the beginning.
Conclusion
The advantage of extracting and letting things drift is the self-correction and self-separation that can occur so rapidly. It becomes so much easier to band crowded teeth, rotate them, and incorporate them into the arch. You don't have to separate, and initial archwires are not nearly so complicated, since you don't need multilooped arches. Furthermore, with proper manipulation and timing, the combination of physiologic drift with progressive banding of teeth as they erupt achieves the very best in full-banded therapy while reducing treatment time and chair time. Waiting for physiologic drift after extractions can significantly simplify treatment mechanics and reduce treatment time. My young assistant, Margo Reneau, very aptly said, "Sometimes doing nothing is doing something."
Maybe we should reexamine the influence of muscle function of the oral and facial complex on malocclusion. Here we have seen gross, rapid, spontaneous changes in the dentition while completely ignoring muscle function, Only teeth were removed to make room for the remaining teeth. No myofunctional therapy or myofunctional training appliances were ever used.
Observations of physiologic drift, as seen in the cases presented, would indicate a need to also reexamine our thinking about: anchorage requirements and concepts, differential forces and their effects, the necessity to torque maxillary cuspids lingually so that they may be retracted with light forces, cuspid retraction procedures, and optimum forces.