CASE REPORT
Treatment of an Impacted and Inverted Upper Premolar
The upper and lower third molars and upper canines are the most commonly impacted teeth in the permanent dentition. Impaction can be horizontal, vertical, mesioangular, distoangular, or inverted.1-3 Inverted impaction has been reported in a variety of teeth, including incisors, canines, molars, and supernumerary teeth (most commonly a mesiodens).4-6
Although inverted premolar impactions are extremely rare, one author reported surgical removal of an inverted upper premolar followed by reimplantation in an upright position.7 In another case of an impacted and inverted lower second premolar tooth germ, surgical uprighting was performed and the deciduous lower second molar was preserved.8 Our case report demonstrates successful orthodontic treatment of an impacted and inverted upper premolar without extraction or reimplantation.
Diagnosis and Treatment Plan
A 14-year-old female presented with the chief complaint of prolonged retention of a second deciduous molar (Fig. 1). She had bilateral Class I canine and molar relationships and a balanced facial pattern. A retained upper left second deciduous molar was found in the position of the missing second premolar. Radiography revealed an impacted and inverted upper left second premolar, with the crown facing toward the maxillary sinus floor.
Similar articles from the archive:
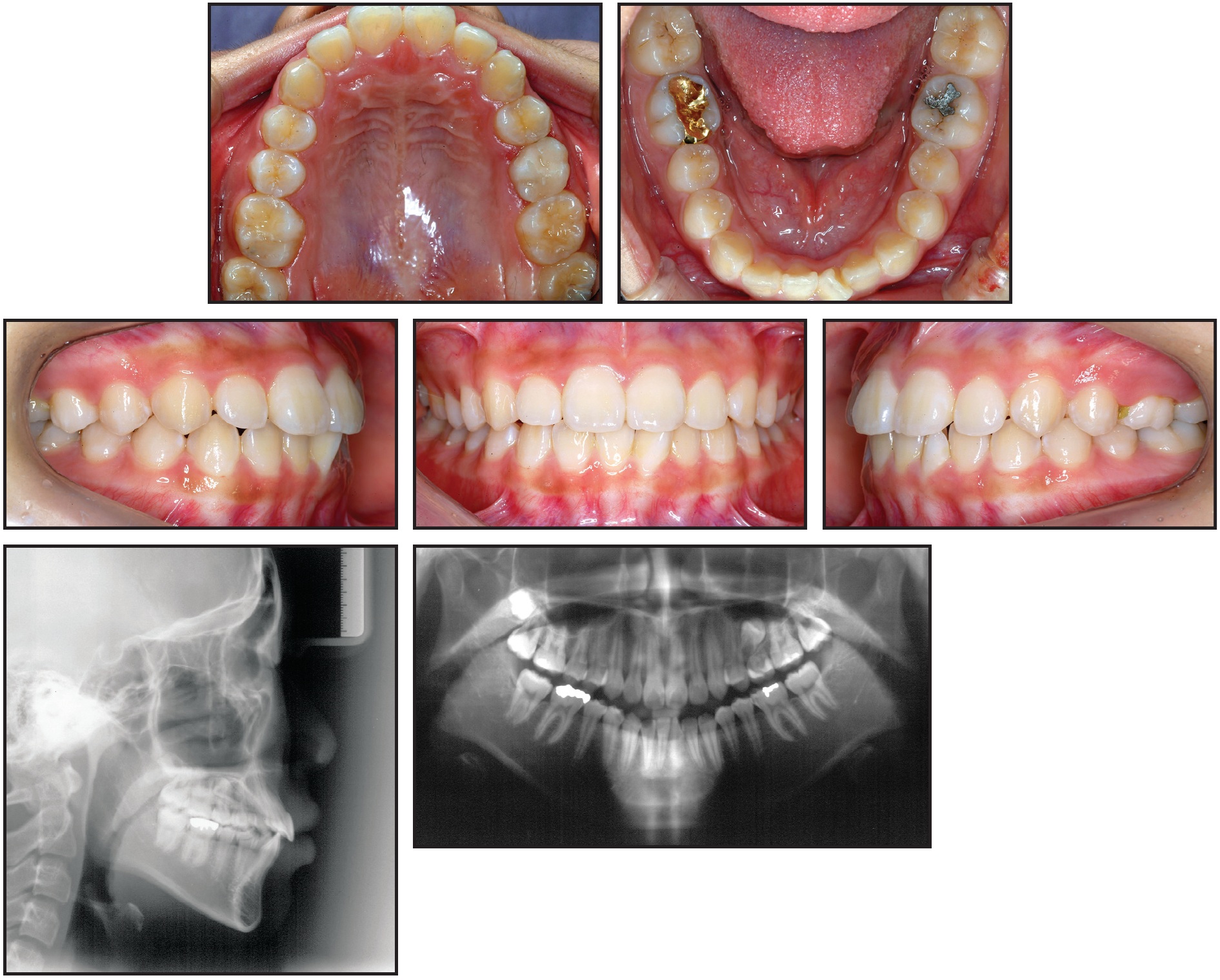
Fig. 1 14-year-old female patient with prolonged retention of second deciduous molar and bilateral Class I canine and molar relationships before treatment.
The treatment plan called for extraction of the retained deciduous teeth, space maintenance by fixed orthodontic treatment, and surgical exposure and traction of the impacted tooth into its proper position. Treatment was planned only for the upper dentition because of the patient’s concerns about cost.
Treatment Progress
An .018" × .022" MBT-prescription Inspire ICE* clear fixed appliance was bonded in the upper arch. After three months of initial leveling on .014", .016", and .016" × .022" G4** nickel titanium archwires, an .016" × .022" stainless steel archwire was inserted. The patient was then referred for extraction of the retained tooth and exposure of the impacted premolar by an oral surgeon. A metal lingual button was bonded to the impacted tooth, and a twisted stainless steel ligature wire was tied to the attachment (Fig. 2). The ligature wire was drawn inferiorly through the sutured edges of the flap, so that the surgical site could be completely closed.
After seven days of healing, orthodontic treatment was resumed. Traction was applied to the twisted stainless steel ligature to bring about full eruption of the tooth. Since the distance between the ligature wire and the main archwire was too short to apply force, a stepdown bend was made in the archwire, and an open-coil spring was inserted between the first molar and first premolar to open and maintain adequate space for the second premolar (Fig. 3). The progress of impacted tooth movement was evaluated monthly (Fig. 4). After three months, to produce more clockwise rotation of the impacted tooth, the metal button was replaced by a minitube and an .016" × .022" TMA*** auxiliary wire was bent and attached (Fig. 5). Three months later, the wire was activated to create an additional rotational moment (Fig. 6).
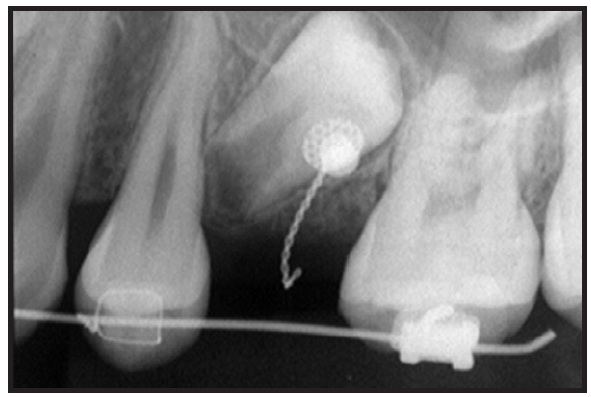
Fig. 2 After three months of upper leveling and alignment, metal lingual button bonded to impacted upper left second premolar, and twisted stainless steel ligature wire tied to attachment.
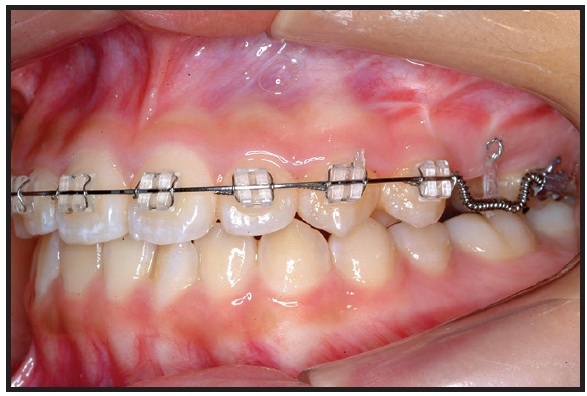
Fig. 3 After one week of healing, stepdown bend made in main .016" × .022" stainless steel archwire to increase distance for eruption force application; open coil spring inserted between first molar and first premolar to open space for second premolar.
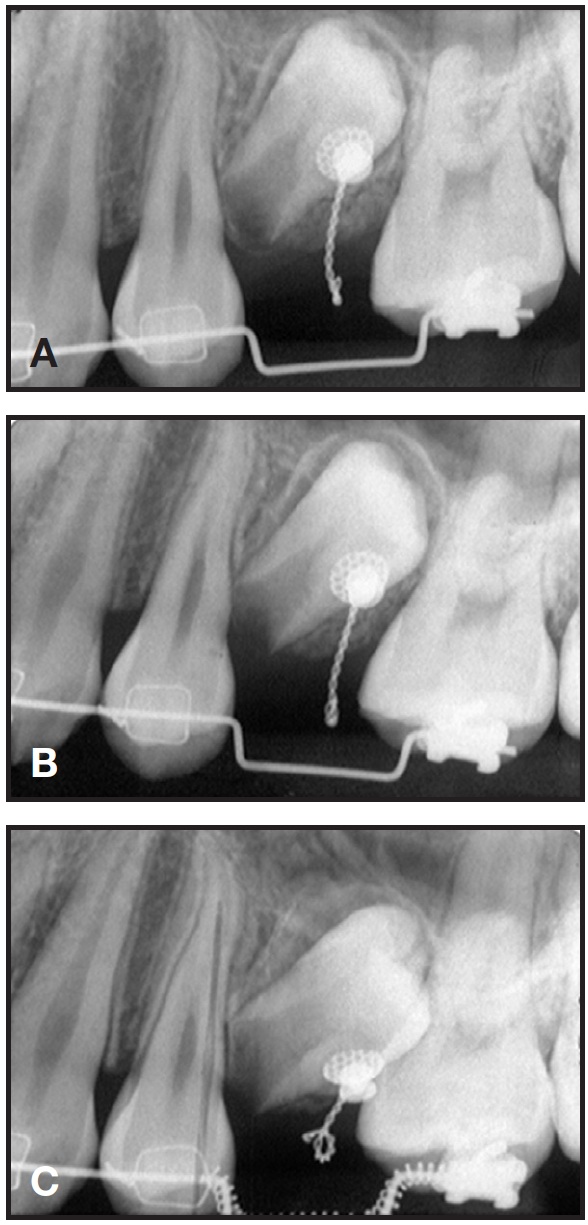
Fig. 4 Impacted premolar after one (A), two (B), and three (C) months of eruption.
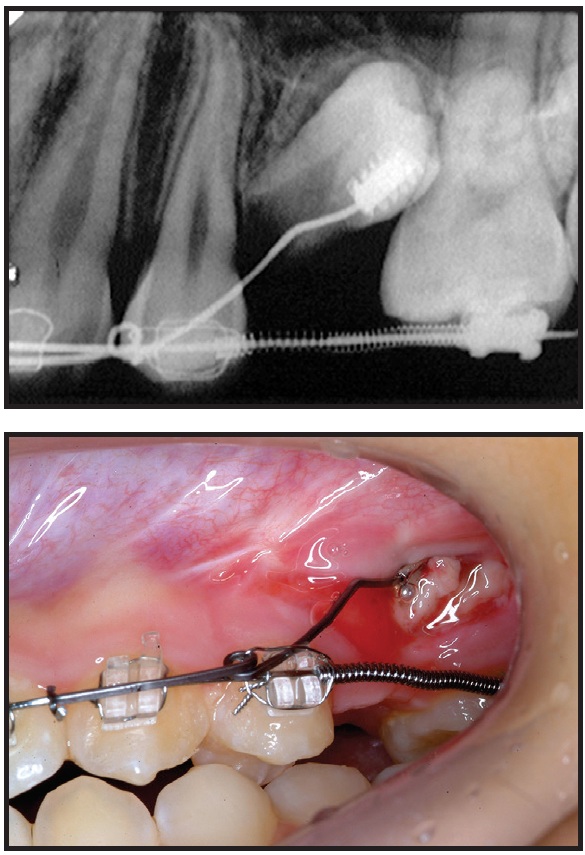
Fig. 5 Minitube bonded to impacted premolar, and .016" × .022" TMA*** auxiliary wire bent and attached.
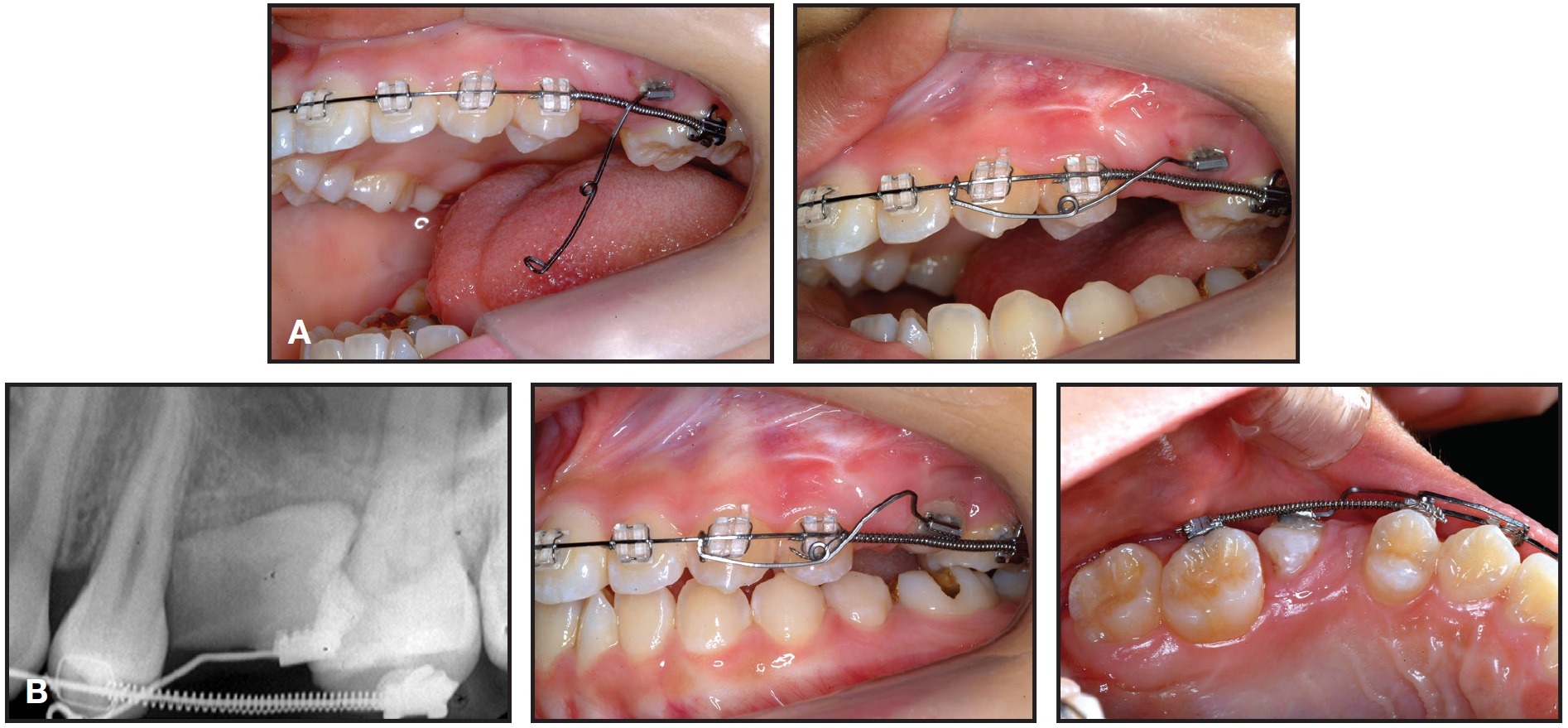
Fig. 6 A. Three months later, auxiliary wire activated to create additional rotational moment. B. After 11 months of treatment.
In another four months, the crown had been sufficiently rotated to replace the minitube with a bracket, and a segmental .014" nickel titanium wire was inserted for alignment (Fig. 7). The inverted upper left second premolar was successfully positioned in proper alignment within another 10 months (Fig. 8). After a total 23 months of treatment, the fixed appliances were removed and an upper 2-2 lingual retainer wire was bonded. Follow-up records taken three years after treatment confirmed the stability of results (Fig. 9).

Fig. 7 After 13 months of treatment, minitube replaced by bracket and segmental .014" nickel titanium wire inserted for alignment.

Fig. 8 Patient after 23 months of treatment.
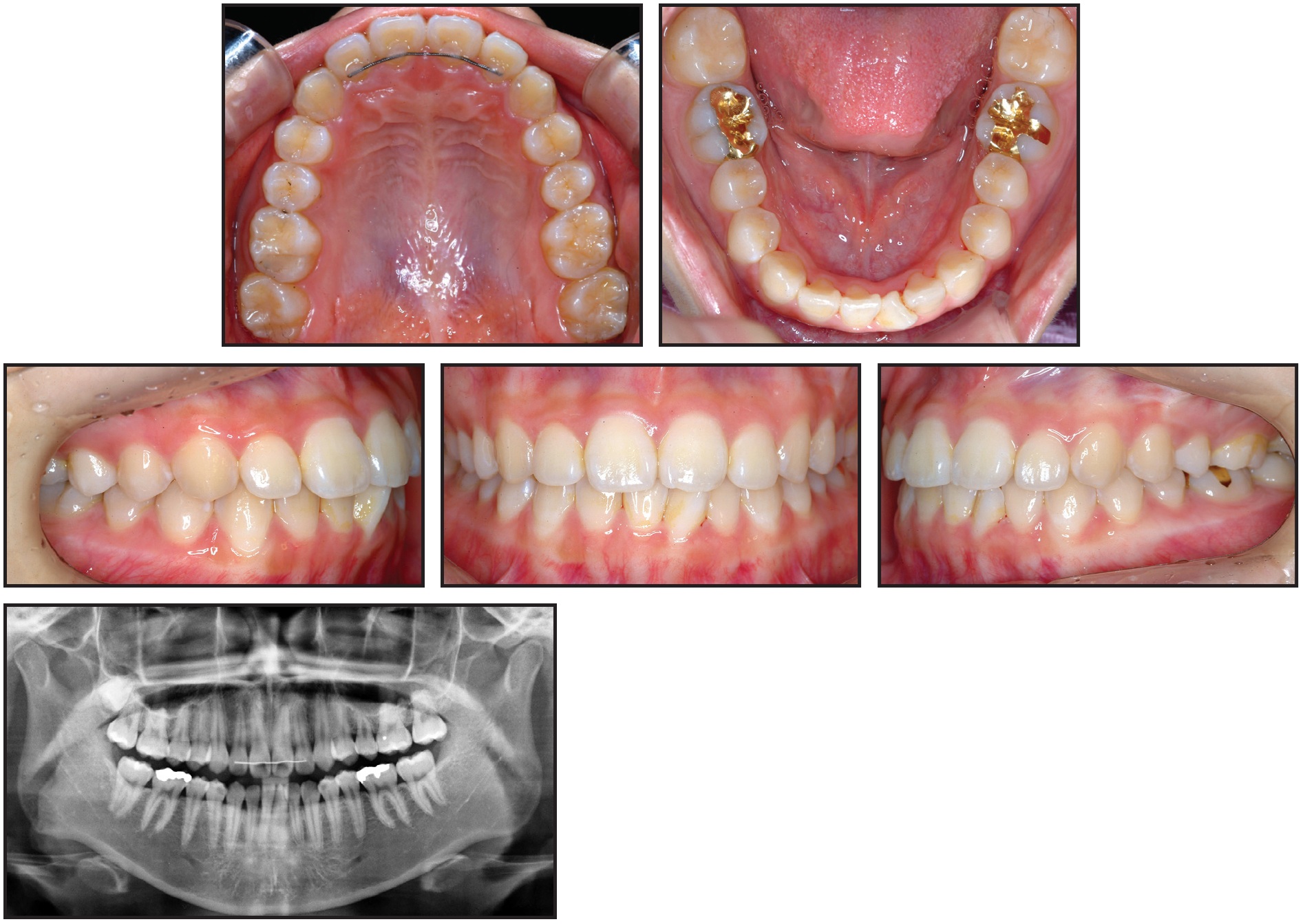
Fig. 9 Patient three years after treatment.
Discussion
Reimplantation is generally considered the best treatment approach for an inverted premolar.9 Surgical intervention is more problematic with an inverted tooth than with other types of impactions, however, because the inaccessibility of the crown necessitates extensive bone removal. Potential complications of surgical extraction, such as perforation of the maxillary sinus, should also be taken into consideration.4
Traumatic injuries and obstructions to eruption are believed to be the most common causes of impacted anterior teeth; improper oral habits, such as nail biting or fingersucking, may also contribute.10 There was no history of facial or jaw trauma or TMD in our patient. We chose to use a closed-eruption technique because it usually provides the most esthetically pleasing result.11,12 Our patient’s premolar had a short root due to extensive tooth movement during root development. Therefore, the greatest challenge was to produce enough clockwise force to rotate the inverted tooth nearly 180° within the alveolar bone.
Some studies have reported a relatively high prevalence of gingival defects in the area of impacted anterior teeth, which may require adjunctive postorthodontic periodontal surgery to achieve an esthetic gingival contour.13 In our patient, the gingival contour of the exposed premolar was acceptable after orthodontic treatment, and no further mucogingival surgery was recommended.
Conclusion
As this case illustrates, conservative surgical exposure and orthodontic treatment can be an appropriate solution for an impacted and inverted tooth if the principles of biomechanics are properly applied.
FOOTNOTES
- *Trademark of Ormco Corporation, Orange, CA; www.ormco.com.
- **Trademark of G&H Wire Company, Franklin, IN; www.ghwire.com.
- ***Registered trademark of Ormco Corporation, Orange, CA; < a href="http://www.ormco.com" target="_blank">www.ormco.com.
REFERENCES
- 1. El-Khateeb, S.M.; Arnout, E.A.; and Hifnawy, T.: Radiographic assessment of impacted teeth and associated pathosis prevalence: Pattern of occurrence at different ages in Saudi male in Western Saudi Arabia, Saudi Med. J. 36:973- 979, 2015.
- 2. Pedro, F.L.; Bandéca, M.C.; Volpato L.E.; Marques, A.T.; Borba, A.M.; Musis, C.R.; and Borges, A.H.: Prevalence of impacted teeth in a Brazilian subpopulation, J. Contemp. Dent. Pract. 15:209-213, 2014.
- 3. Msagati, F.; Simon, E.N.; and Owibingire, S.: Pattern of occurrence and treatment of impacted teeth at the Muhimbili National Hospital, Dar es Salaam, Tanzania, BMC Oral Health 13:37, 2013.
- 4. Chen, C.Y.; Wang, W.C.; Lin, L.M.; and Chen, Y.K.: Incidental detection of a rare inverted and impacted maxillary third molar in a patient of mandibular unicystic ameloblastoma, Dentistry 4:213, 2014.
- 5. . Lakshman, A.R.; Kanneppady, S.K.; and Balan, P.: A rare case report of inverted eruption of supernumerary tooth in the anterior maxilla, J. Marmara Univ. Inst. Health Sci. 3:164, 2013.
- 6. Abu-Mostafa N.; Barakat, A.; AlTurkmani, T.; and Al-Yousef, A.: Bilateral inverted and impacted maxillary third molars: A case report, J. Clin. Exp. Dent. 7:e441-e443, 2015.
- 7. Ulusoy, A.T.; Akkocaoglu, M.; Akan, S.; Kocadereli, I.; and Cehreli, Z.C.: Reimplantation of an inverted maxillary premolar: Case report of a multidisciplinary treatment approach, J. Clin. Pediat. Dent. 33:279-282, 2009.
- 8. . Engel, M. and Katsaros, C.: Replantation of an inverted lower second premolar germ, J. Orofac. Orthop. 58:282-285, 1997.
- 9. Mohan, S.; Kankariya, H.; and Fauzdar, S.: Impacted inverted teeth with their possible treatment protocols, J. Maxillofac. Oral Surg. 11:455-457, 2012
- 10. Chaushu, S.; Becker, T.; and Becker, A.: Impacted central incisors: Factors affecting prognosis and treatment duration, Am. J. Orthod. 147:355-362, 2015.
- 11. Becker, A.; Brin, I.; Ben-Bassat, Y.; Zilberman, Y.; and Chaushu, S.: Closed-eruption surgical technique for impacted maxillary incisors: A postorthodontic periodontal evaluation, Am. J. Orthod. 122:9-14, 2002.
- 12. Pinho, T.; Neves, M.; and Alves, C.: Impacted maxillary central incisor: Surgical exposure and orthodontic treatment, Am. J. Orthod. 140:256-265, 2011.
- 13. Chaushu, S.; Brin, I.; Ben-Bassat, Y.; Zilberman, Y.; and Becker, A.: Periodontal status following surgicalorthodontic alignment of impacted central incisors with an open-eruption technique, Eur. J. Orthod. 25:579-584, 2003.
-
 DR. BAE
DR. BAE -
 DR. HUNG
DR. HUNG -
 DR. LEE
DR. LEE -
 DR. KYUNG
DR. KYUNG
Dr. Bae is a Clinical Faculty Member, Dr. Hung is a PhD student, and Dr. Kyung is a Professor, Department of Orthodontics, School of Dentistry, Kyungpook National University, 2177 Dalgubeol aero, Jung-gu, Daegu 41940, Korea. Dr. Lee is in the private practice of orthodontics in Daegu. E-mail Dr. Kyung at hmkyung@knu.ac.kr.
