Effectiveness of Composite Attachments in Controlling Upper-Molar Movement with Aligners
In nonextraction treatment, upper-molar distalization is often the method of choice to gain 2-3mm of arch space and obtain a Class I relationship.1 To achieve bodily movement, either the applied force must pass through the tooth's center of resistance or a sophisticated equivalent system of forces and moments must be applied to the molar crown.2,3
Although a systematic study has found aligners to be more effective than fixed appliances in treating mild-to-moderate crowding,4 Brezniak has suggested that bodily movement is not possible with aligners, even when composite attachments are used.5 Recent studies indicate, however, that the forces and moments generated by Invisalign* trays are within the range of orthodontic forces.6,7 Simon and colleagues also reported a high degree of accuracy of upper-molar bodily movement with aligners when a distalization movement of at least 1.5mm was prescribed, attributing any significant difference to the use of attachments.6 These observations were made in the horizontal plane; tipping effects were not analyzed.
Tipping movements are difficult to control during molar distalization with aligners because of the trays' limited contact with the tooth surfaces in the direction of force application.8 Gomez and colleagues showed that when an aligner segment was displaced distally without attachments, a clockwise moment and distal inclination were produced on the upper canine.9 Vertical rectangular attachments on the buccal aspects of the molars helped counteract this inclination tendency by producing a countermoment that promoted bodily movement.9
Similar articles from the archive:
The present case-control study was designed to test the hypothesis that the number of long vertical attachments on the distalizing teeth has no effect on the amount of bodily upper-molar movement achieved with aligner therapy.
Materials and Methods
Subject Selection
Thirty consecutive non-growing Invisalign patients (12 males, 18 females; mean age 30.50) were randomly assigned to two experimental groups based on the number of attachments used to control their distalized molars (Fig. 1). The randomization sequence** involved patients in two orthodontic clinics: one in Turin, Italy, and one in Vancouver, British Columbia. In the Case 1 (C1) group (seven males, nine females; mean age 29.24), rectangular composite attachments were placed on all distalized teeth from canine to second molar (five attachments per quadrant). In the Case 2 (C2) group (five males, nine females; mean age 31.75), attachments were used only on the first and second premolars and the first molar (three attachments per quadrant), based on a previously described protocol.10
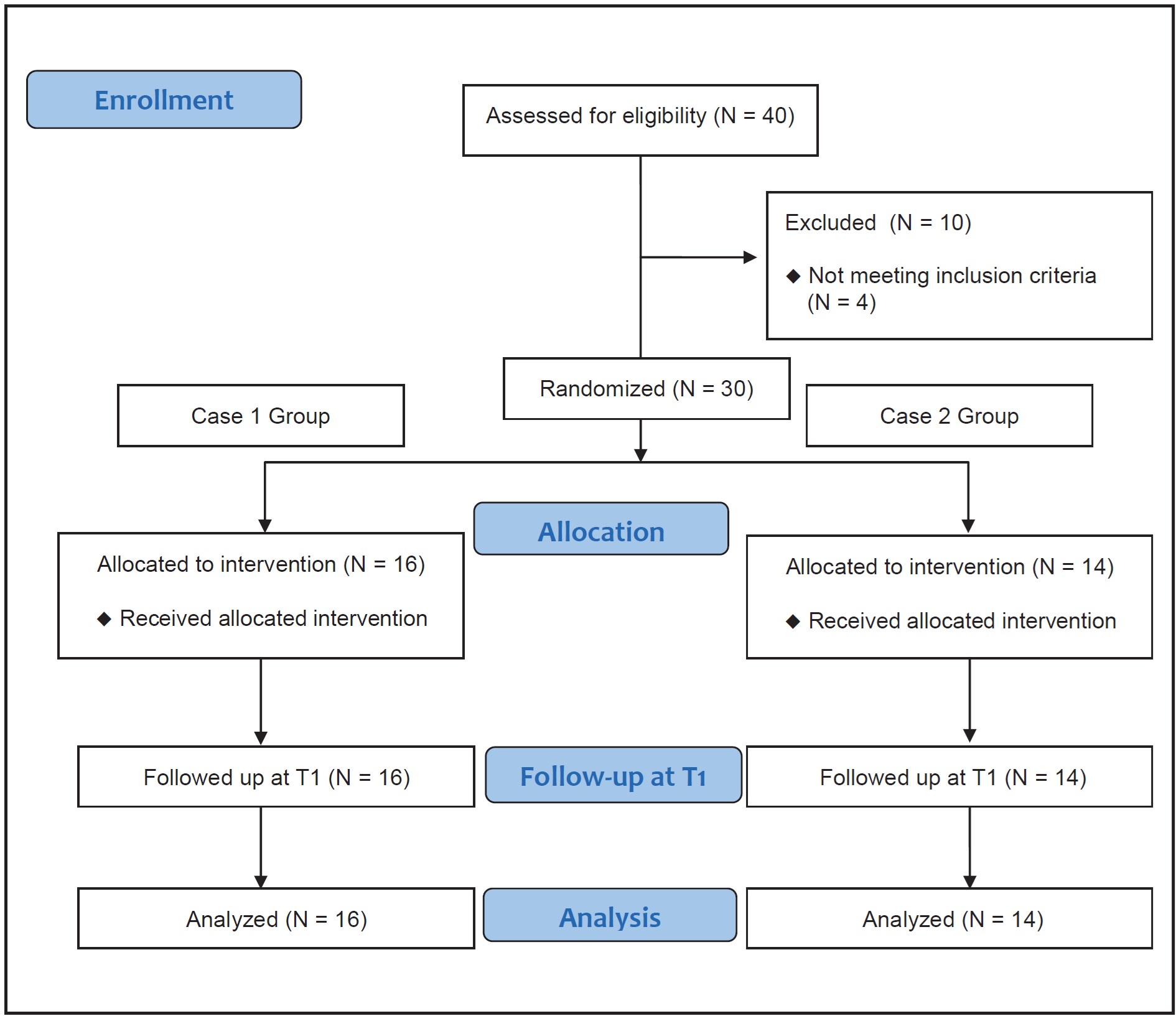
Fig. 1 CONSORT diagram showing flow of subjects in study (T1 = end of Invisalign* treatment).
As a control (C) group, 20 subjects matched by age and sex to the study group were selected from the following collections of the AAO Foundation Craniofacial Growth Legacy: Case Western Reserve University Bolton-Brush Growth Study, Oregon Growth Study, and University of Oklahoma Denver Growth Study. The diagnostic criteria for both study and control groups were the same: a half-cusp Class II molar relationship, a need for molar distalization, maxillary dentoalveolar protrusion, and normodivergence of the vertical plane (palatal plane to mandibular plane angle of 20º ± 5º). Exclusion criteria were transverse dental or skeletal discrepancies, vertical dental or skeletal discrepancies, extraction treatment (except for third molars), unilateral distalization, signs or symptoms of TMD according to standard diagnostic criteria,11 periodontal disease, and endodontic treatment or prosthodontic rehabilitation of the upper molars.
Each patient provided informed consent, and the study was conducted in accordance with the Declaration of Helsinki and approved by the Lingotto Dental School Ethical Committee at the University of Turin. All patients were treated by Dr. Garino, Dr. Castroflorio, or Dr. Daher.
Prior to the start of treatment, the patients' upper third molars (if present) were extracted to make room for molar distalization.10 Initial (T0) and post-treatment (T1) lateral radiographs were taken using three x-ray machines; for standardization purposes, the magnification was corrected to 8%.
Initial cephalograms (T0) were obtained for the 20 subjects of the control group. A second set of images (T1) was obtained for the same subjects at least two years later, or at the age corresponding to the mean age of the experimental groups at the end of treatment.
All digital x-rays were stored on a computer and imported into OrisCeph Rx3*** software for landmark identification and cephalometric tracing. Operations were performed in random order by a single investigator (Dr. Ravera), who was blinded to the study, using a customized digitization set including 47 landmarks and 54 variables.
The reference axes were the palatal plane (x-axis) and a line perpendicular to the palatal plane passing through the Ricketts PT point (yaxis).12 The occlusal plane was also traced, passing through the upper central incisor edge and the mesial cusp of the first molar (Fig. 2).13 The palatal plane/mandibular plane (PP/MP) and sella-nasion/mandibular plane (SN/MP) angles were used as indicators of skeletal posterior vertical changes. Overall craniofacial treatment changes were evaluated by superimposing on SN at sella.
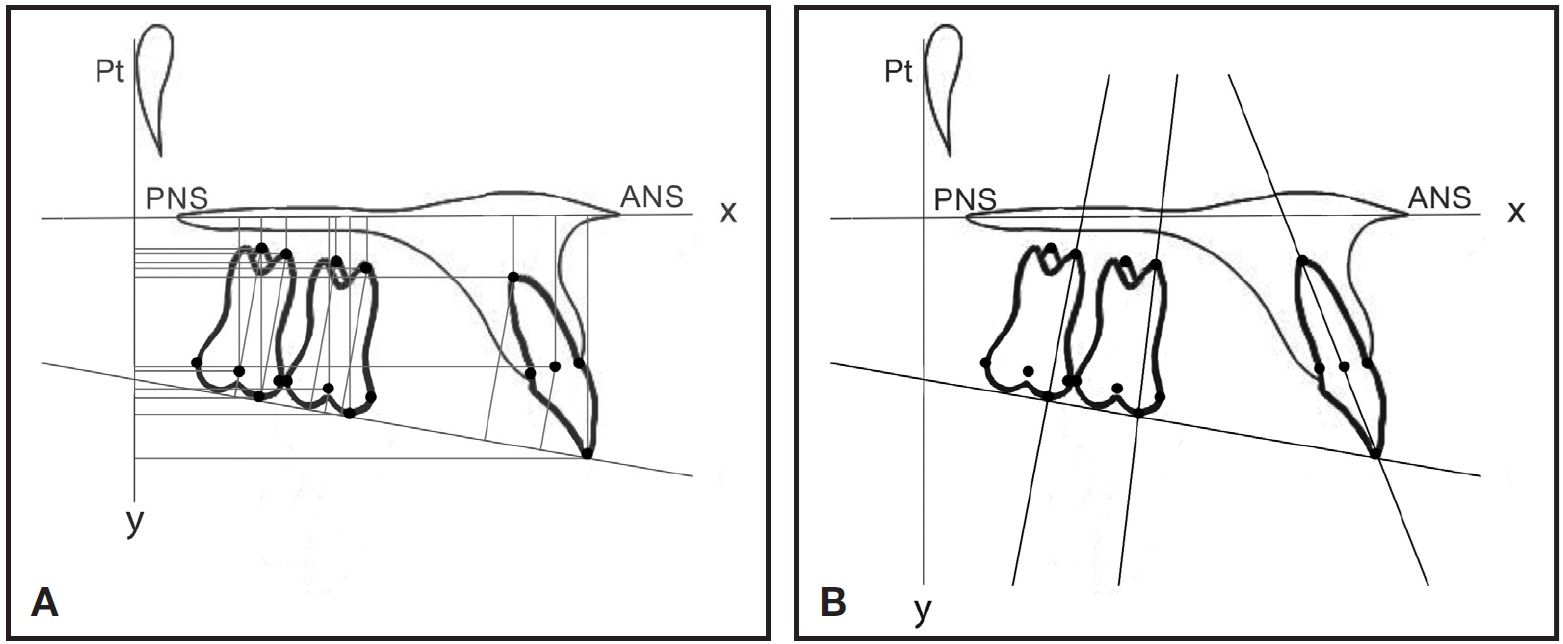
Fig. 2 A. Horizontal measurements (mm) expressed by distances from y-axis of following points: second molar center of crown, mesiobuccal cusp, mesiobuccal root apex, and palatal root apex; first molar center of crown, mesiobuccal cusp, mesiobuccal root apex, and palatal root apex; and central incisor center of crown, incisal edge, and radicular apex. Vertical measurements (mm) expressed by distances of same points from x-axis and occlusal plane (except for incisal edge point and mesiobuccal cusp points, both tangential to occlusal plane). B. Angular measurements of upper second molar, upper first molar, and central incisor, with inclination expressed as angle between tooth’s long axis (passing through mesiobuccal cusp and mesiobuccal root apex for first or second molar, and through incisal edge and root apex for central incisor) and x-axis (palatal plane).
Maxillary regional superimpositions were made along the palatal plane (internal structures of the maxilla) and the constructed y-axis to assess only the amount of molar distalization,14 since adults exhibit no substantial changes in the palatal plane. In case of a difference between the left and right sides of the superimposition, the more distally positioned landmark was chosen.
Treatment Sequence
ClinCheck* software was used to plan a maximum movement of .25mm per aligner. When the upper second molars had been distalized two-thirds of the way, the first-molar retraction was scheduled to begin, similarly followed by the premolars.10 The canines and incisors were sequentially retracted after the first premolars were in their final positions. To maintain proper buccolingual inclination during distalization of the upper incisors, Power Ridge* features were prescribed for placement after intrusion had been completed.15 No interproximal reduction was performed in the upper arch. All prescriptions were reviewed and submitted by Dr. Castroflorio.
The average number of required aligners was 42.6 in the upper arch and 21.4 in the lower. Patients were instructed to wear their aligners and 3/16", 4.5oz Class II elastics† at least 22 hours per day, starting at first-molar distalization and continuing until a full Class I canine relationship was achieved.16 The interval between appointments was six to eight weeks, with each set of aligners worn for two weeks. A refinement phase with a mean 9.1 upper aligners and 6.7 lower aligners was ordered for each case; aligners were worn for 10 days each during refinement. Mean total treatment time was 24.3 months.
Statistical Analysis
The statistician (Mr. Cugliari) was blinded to the orthodontic characteristics of the two study groups. Since no previous data were available regarding the effect of the number of attachments on the amount of upper-molar distal movement, we considered a 20% increase in movement of the first molar to be clinically relevant, with 80% power at the 5% significance level. The required sample size was 14 subjects, as calculated by Survey System‡ software.
Statistical analysis was performed using the R version 3.0.1†† statistical package. Differences between the two experimental groups before treatment (C1T0 - C2T0) were evaluated by means of Fisher's exact test for qualitative variables and the unpaired t-test for quantitative variables. The normality assumption of the data was measured using the Kolmogorov-Smirnov and Shapiro-Wilk tests, and homogeneity of the variables with the Levene and Brown-Forsythe tests.
Differences between pre- and post-treatment results for the Case 1 (C1T1 - C1T0) and Case 2 (C2T1 - C2T0) groups and between the two groups (C1[T1-T0] - C2[T1-T0]) were assessed by a mixed two-way analysis of variance with repeated measurements. The level of significance for all tests was set at p < .05.
To estimate the error of the method, 30 randomly chosen cephalometric radiographs were traced, digitized, and analyzed by the same examiner three weeks and six months after the first assessment. Dahlberg's error was less than .5, indicating good intra-observer accuracy and reliability.17
Results
Case 1 Group
Case 1 results can be found here.
The statistical analysis indicated bodily movement of the second molar, with significant values (p < .0001) found for distal movement of the mesial cusp (2.30mm), center of the crown (1.71mm), palatal root apex (1.47mm), and buccomesial root apex (1.68mm). A significant amount of intrusion was measured at the crown center (1.25mm, p < .001), but no significant tipping movement was found.
The first molar also moved bodily, with significant values for the center of the crown (2.13mm, p < .0001) and for the apices of the palatal and buccomesial roots (1.71mm and 1.75mm, respectively, p < .001). Again, there was significant intrusion at the crown center (1.11mm, p < .05), but no significant tipping.
Distal movement of the central incisor was significant (p < .05) at the incisal edge (2.48mm) and center of the crown (1.58mm), but not at the root apex. The incisor retraction was associated with significant intrusion (.91mm, p < .05), but no significant inclination.
Case 2 Group
Case 2 results can be found here.
In this group, there was significant distal movement only of the mesial cusps of the second and first molars (1.54mm, p < .01, and 1.52mm, p < .05, respectively). Analysis also indicated significant tipping (p < .05) of the first molar (2.49º) and central incisor (4.12º).
Comparison of Case 1 and 2 Groups
Comparison of Case 1 and 2 group results can be found here.
Although there were no significant differences with regard to distal movement of the second molar, the Case 1 group demonstrated significantly greater (p < .05) distal movement of the first molar at the center of the crown and the buccomesial root apex (mean differences of 1.57mm and 1.95mm, respectively). This distal movement was associated with significantly more intrusion (p < .05) with respect to the palatal plane, measured at the center of the crown for both first and second molars (mean differences of 1.64mm and 1.41mm, respectively).
Central-incisor retraction was significantly more efficient in the Case 1 group (p < .05), as demonstrated by bodily movement at the root apex (mean difference of 3.17mm), center of the crown (mean difference of 2.41mm), and incisal edge (mean difference of 2.61mm).
Comparison with Control Group
The only significant differences were for the sagittal positions of the upper molars and central incisors at T1.
Discussion
Several articles have demonstrated the possibility of achieving Class II correction using clear aligners without attachments.18-23 It should be noted, however, that these were mainly case reports. To our knowledge, the present study represents the first attempt to establish a reliable clinical approach for correcting Class II malocclusions with aligners.
Our two experimental groups showed no significant differences in the amount of second-molar movement with or without vertical rectangular attachments (Fig. 3).
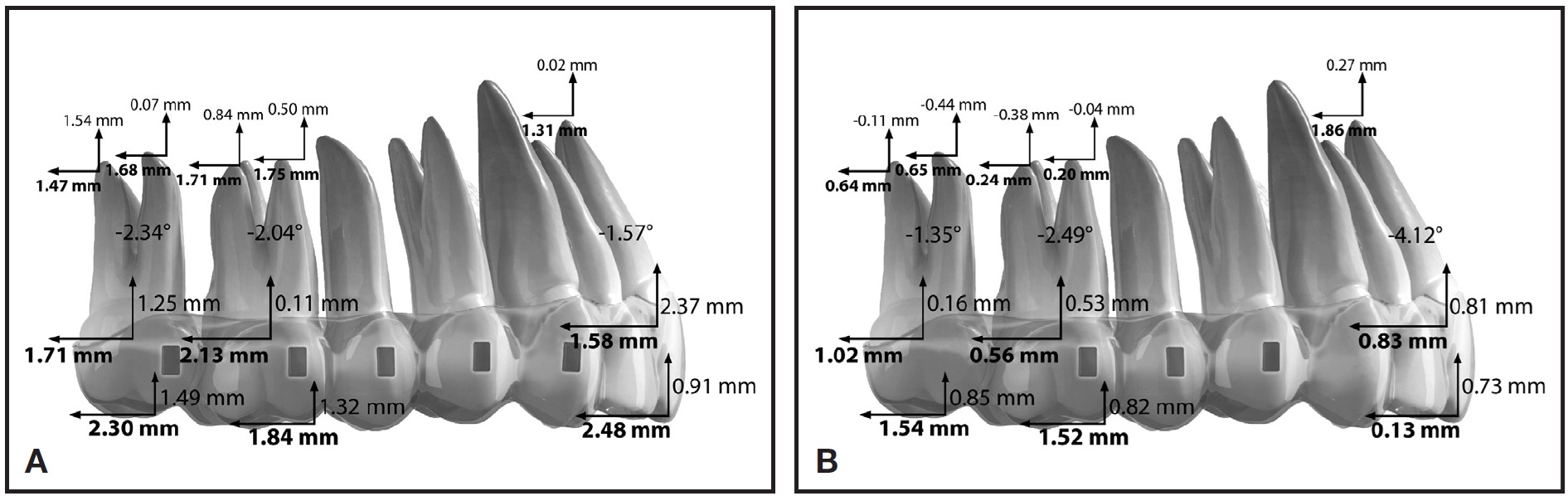
Fig. 3 Clinically relevant results for Case 1 (A) and Case 2 (B) groups.
There was significantly more distal movement of the first molar and central incisor, however, in the Case 1 group, where attachments were placed on five teeth. In particular, bodily movement of the incisor was more accurately controlled in this group. This demonstrates that vertical attachments not only control tipping during molar distalization, but also enhance posterior anchorage during anterior retraction. In the Case 2 group, without attachments on the second molars, a loss of anchorage during first-molar distalization appeared to result in less distal movement of the second molar and significant tipping of the first molar. The lack of anchorage preparation in the posterior segment also inhibited control of the anterior teeth during retraction, leading to uncontrolled tipping of the central incisors (Fig. 4).
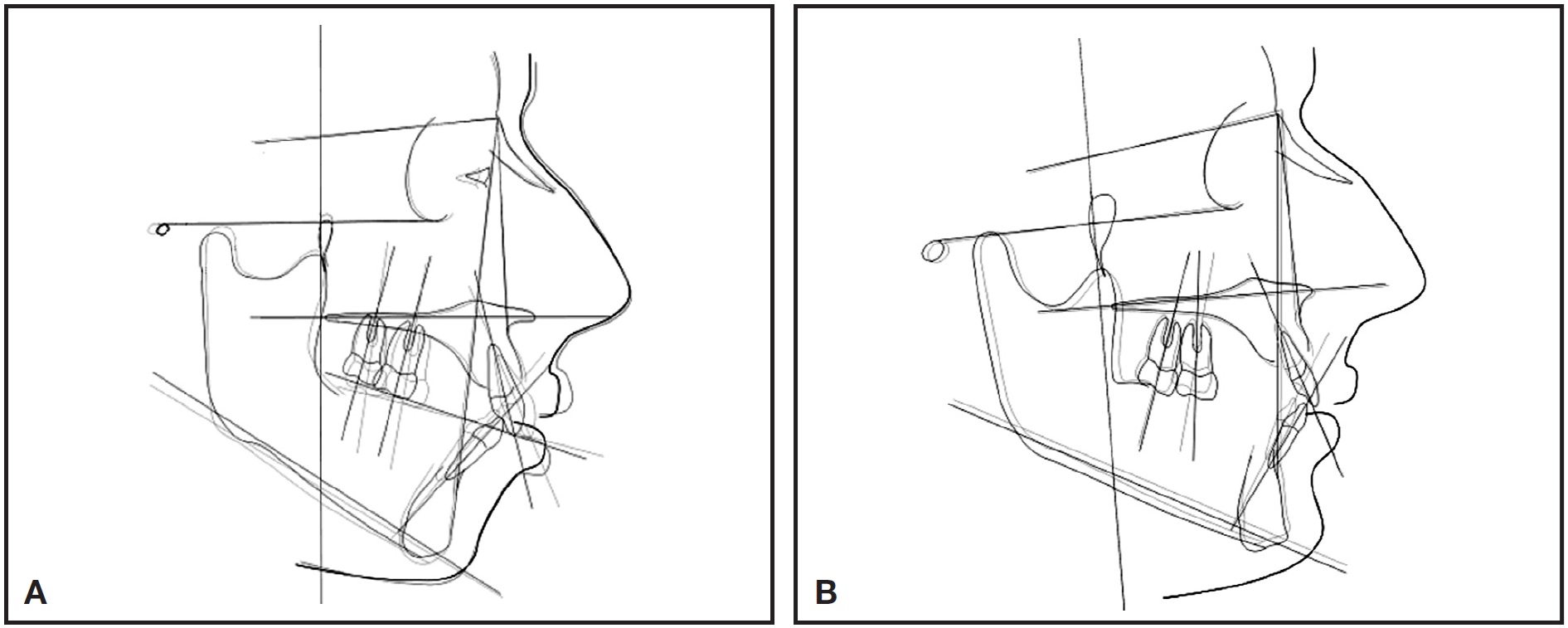
Fig. 4 Representative superimpositions of pre- and post-treatment cephalometric tracings in Case 1 (A) and Case 2 (B) groups.
The vertical pattern is an important consideration in planning molar distalization. In our Case 1 group, distal movement was associated with significant molar intrusion. The thickness of the aligners and the occlusal force exerted on them tend to promote intrusion and thus avoid any change in the anterior vertical dimension during distalization. Gomez and colleagues reported a marked flaring tendency of the buccal and palatal aligner segments during distal displacement,9 which would also suggest an intrusive effect.
The main limitation of our study was the absence of a group treated with a different technique. Of course, any investigation has the potential for selection or participation bias.
Conclusion
In a case-control study of adult Class II Invisalign patients, the upper first and second molars were each distalized about 2mm, accompanied by intrusion of about 1mm, when vertical rectangular attachments were placed on all five distalized teeth. This approach appears to be effective in minimizing distal crown tipping and preventing molar extrusion, anterior anchorage loss, and undesirable changes in lower facial height. Therefore, clinicians should consider the use of such attachments in non-growing patients requiring 2-3mm of bodily upper-molar distalization.
FOOTNOTES
- *Registered trademark of Align Technology, Inc., Santa Clara, CA; www.aligntech.com.
- **www.random.org.
- ***Registered trademark of Elite Computer Italia, Vimodrone, Italy; www.orisline.com.
- †Ormco Corporation, Orange, CA; www.ormco.com.
- ‡Creative Research Systems, Petaluma, CA; www.surveysystem.com.
- ††R Core Team, Foundation for Statistical Computing, Vienna, Austria; www.r-project.org.
REFERENCES
- 1. Nanda, R. and Tosun, Y.S.: Correction of anteroposterior discrepancies, in Biomechanics in Orthodontics: Principle and Practice, Quintessence Publishing Co., Inc., Hanover Park, IL, 2010, pp. 133-144.
- 2. Kusy, R.P.: Influence of force systems on archwire-bracket combinations, Am. J. Orthod. 127:333-342, 2005.
- 3. Smith, R.J. and Burstone, C.J.: Mechanics of tooth movement, Am. J. Orthod. 85:294-307, 1984.
- 4. Rossini, G.; Parrini, S.; Castroflorio, T.; Deregibus, A.; and Debernardi, C.L.: Efficacy of clear aligners in controlling orthodontic tooth movement: A systematic review, Angle Orthod. 85:881-889, 2014.
- 5. Brezniak, N.: The clear plastic appliance: A biomechanical point of view, Angle Orthod. 78:381-382, 2008.
- 6. Simon, M.; Keilig, L.; Schwarze, J.; Jung, B.A.; and Bourauel, C.: Treatment outcome and efficacy of an aligner technique—Regarding incisor torque, premolar derotation and molar distalization, BMC Oral Health 14:68, 2014.
- 7. Simon, M.; Keilig, L.; Schwarze, J.; Jung, B.A.; and Bourauel, C.: Forces and moments generated by removable thermoplastic aligners: Incisor torque, premolar derotation, and molar distalization, Am. J. Orthod. 145:728-736, 2014.
- 8. Paquette, D.E.: Extraction treatment with Invisalign, in The Invisalign System, Tuncay, O.C., Quintessence Publishing Co., Inc., Hanover Park, IL, 2006, pp.195-205.
- 9. Gomez, J.P.; Peña, F.M.; Martínez, V.; Giraldo, D.C.; and Cardona, C.I.: Initial force systems during bodily tooth movement with plastic aligners and composite attachments: A three-dimensional finite element analysis, Angle Orthod. 85:454-460, 2015.
- 10. Align Technology, Inc.: Dr. Sam Daher’s techniques for Class II correction with Invisalign and elastics, April 2011, https://s3.amazonaws.com/learn-invisalign/docs/06840000000Fp2xAAC.pdf, accessed Feb. 1, 2016.
- 11. Schiffman, E. et al.; International RDC/TMD Consortium Network; International association for Dental Research; and Orofacial Pain Special Interest Group, International Association for the Study of Pain: Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: Recommendations of the International RDC/TMD Consortium Network and Orofacial Pain Special Interest Group, J. Oral Facial Pain Headache 28:6-27, 2014.
- 12. Ghosh, J. and Nanda, R.S.: Evaluation of an intraoral maxillary molar distalization technique, Am. J. Orthod. 110:639-646, 1996.
- 13. Byloff, F.K. and Darendeliler, M.A.: Distal molar movement using the Pendulum appliance, Part 1: Clinical and radiological evaluation, Angle Orthod. 67:249-260, 1997.
- 14. McNamara, J.A. Jr.: A method of cephalometric evaluation, Am. J. Orthod. 86:449-469, 1984.
- 15. Castroflorio, T.; Garino, F.; Lazzaro, A.; and Debernardi, C.: Upper-incisor root control with Invisalign appliances, J. Clin. Orthod. 47:346-351, 2013.
- 16. Schupp, W.; Haubrich, J.; and Neumann, I.: Class II correction with the Invisalign system, J. Clin. Orthod. 44:28-35, 2010.
- 17. Dahlberg, G.: Statistical Methods for Medical and Biological Students, George Allen and Unwin, London, 1940, pp. 122-132.
- 18. Boyd, R. and Vlaskalic, V.: Three-dimensional diagnosis and orthodontic treatment of complex malocclusions with the Invisalign appliance, Semin. Orthod. 7:274-293, 2001.
- 19. Vlaskalic, V. and Boyd, R.L.: Clinical evolution of the Invisalign appliance, J. Calif. Dent. Assoc. 30:769-776, 2002.
- 20. Boyd, R.L.; Oh, H.; Fallah, M.; and Vlaskalic, V.: An update on present and future considerations of aligners, J. Calif. Dent. Assoc. 34:793-805, 2006.
- 21. Boyd, R.L.: Complex orthodontic treatment using a new protocol for the Invisalign appliance, J. Clin. Orthod. 41:525-547, 2007.
- 22. Boyd, R.L.: Esthetic orthodontic treatment using the Invisalign appliance for moderate to complex malocclusions, J. Dent. Ed. 72:948-967, 2008.
- 23. Vlaskalic, V. and Boyd, R.: Orthodontic treatment of a mildly crowded malocclusion using the Invisalign system, Aust. Orthod. J. 17:41-46, 2001.
-
 DR. GARINO
DR. GARINO -
DR. CASTROFLORIO
-
DR. DAHER
-
DR. RAVERA
-
DR. ROSSINI
-
MR. CUGLIARI
-
DR. DEREGIBUS
Dr. Garino is in the private practice of orthodontics in Turin, Italy. Dr. Castroflorio is an Adjunct Professor, Dr. Deregibus is Director, Dr. Ravera is an Adjunct Professor, and Dr. Rossini is a Resident, Postgraduate School of Orthodontics, Department of Surgical Sciences, Lingotto Dental School, University of Turin, Via Nizza 230, 10100 Turin, Italy. Dr. Daher is a Visiting Professor, Department of Orthodontics, University of the Pacific, Arthur A. Dugoni School of Dentistry, San Francisco. Mr. Cugliari is a Fellow, Department of Statistics and Quantitative Methods, University of Milano-Bicocca, Milan, Italy. E-mail Dr. Ravera at serenaravera@gmail.com.