Editor's note: Dr. Robert L. Boyd, a Contributing Editor of JCO, was honored by the AAO Foundation in May with the establishment of a Biomedical Research Award in his name. To fund the award, his friends and colleagues committed more than $250,000 to the foundation. Dr. Boyd is currently the Frederick T. West Endowed Chair of the Department of Orthodontics at the University of the Pacific's Arthur A. Dugoni School of Dentistry in San Francisco. He has been a pioneer in research related to cone-beam computed tomography (CBCT) and the Invisalign system, among many other topics. In recognition of his named award and other achievements, we asked him to write this month's Editor's Corner about exciting new developments in digital diagnostics.
As most JCO readers know, CBCT images represent the contents of the volume of the skull, including the bone and many of the soft tissues. Soft tissues can be visualized with especially good resolution where there is a low-density interface of only air or space to demarcate the boundaries, as with the skin or airways. An intraoral scan (IS) is a surface map of the teeth and surrounding soft tissue of the periodontium. As orthodontists, our focus is mainly on the tooth surfaces and interocclusal relationships to for planning treatment or fabricating fixed or removable appliances.
Similar articles from the archive:
- OVERVIEW Intraoral Digital Scanners June 2014
- OVERVIEW Cone-Beam Volumetric Imaging: A Two-Minute Drill April 2010
- Improving the Efficiency of Intraoral Scanning September 2014
As most JCO readers know, CBCT images represent the contents of the volume of the skull, including the bone and many of the soft tissues. Soft tissues can be visualized with especially good resolution where there is a low-density interface of only air or space to demarcate the boundaries, as with the skin or airways. An intraoral scan (IS) is a surface map of the teeth and surrounding soft tissue of the periodontium. As orthodontists, our focus is mainly on the tooth surfaces and interocclusal relationships to for planning treatment or fabricating fixed or removable appliances.
An IS can be taken in a few minutes, and the latest models are compact enough to fit on a countertop in the operatory. An assistant holds a lightweight wand as it records the various angles of filtered, non-invasive light reflected back from the teeth and gingiva. These signals are merged by the software to form a surface map consisting of millions of pixels. The software lets the doctor know when the image has met the criteria for accuracy and completeness, avoiding the retakes that we often need with impressions that do not capture some anatomical features. Recent studies have shown that IS is more accurate than even our most accurate polyvinyl siloxane (PVS) impressions. Patients report that the procedure is much more comfortable than impression taking, with no gag reflex, and it can be done even in a patient with limited opening. Moreover, IS is less expensive than PVS impressions. As a result of these advantages, it is one of the most rapidly emerging technologies in both restorative dentistry and orthodontics.
While it is also possible to generate a surface map of the teeth from a CBCT data set, we cannot yet achieve the level of accuracy provided by IS. Computer smoothing operations have thus far been unable to solve the problem of radiation scatter from metallic restorations (Fig. 1). In addition, CBCT images are limited in resolution because manufacturers and dentists have kept radiation doses as low as possible to make them comparable to or even lower than those of conventional cephalograms or pantomograms. In 2005 and 2006, an Align Technology project that I assisted in concluded that with the present signal strength of CBCT (which has actually decreased since then), there were too many inaccuracies in the model surfaces to make stereolithographic models for properly fitting aligners. Another disadvantage is that the gingiva is not dense enough to show accurately on a CBCT, but is required to determine changes in clinical crown length or to make appliances such as clear aligners that require the gingival margin to be delineated.
Given these limitations, how might we combine the internal structures provided by the CBCT with the tooth surfaces of an IS to achieve the accuracy we need? Some software programs allow the operator to manually "best fit" the IS over the crowns of the CBCT teeth. Unfortunately, this could lead to significant measurement errors because the IS is a rigid body--meaning that an error of only 1º of second-molar tip at one end of the arch could accumulate into a much more significant error at the opposite second molar. Engineers at both Align Technology and Anatomage (maker of Invivo5 software) have developed elaborate algorithms to simultaneously shape-match thousands of measurements of the closest distances from the pixels of the IS to the crown surfaces of the CBCT (Figs. 2,3; Figure 3 video sequence). Our lab is presently testing the accuracy of these algorithms by making repeated physical measurements from standardized locations on dried skulls to standardized locations on the teeth, then comparing these direct caliper measurements to those of the same points from the merged IS-CBCT model.

Fig. 1 Anatomage cone-beam computed tomography (CBCT) dental model, called Anatomodel, produced after segmentation of crowns and roots. Note obvious distortion of posterior teeth in patient with several large metallic restorations.
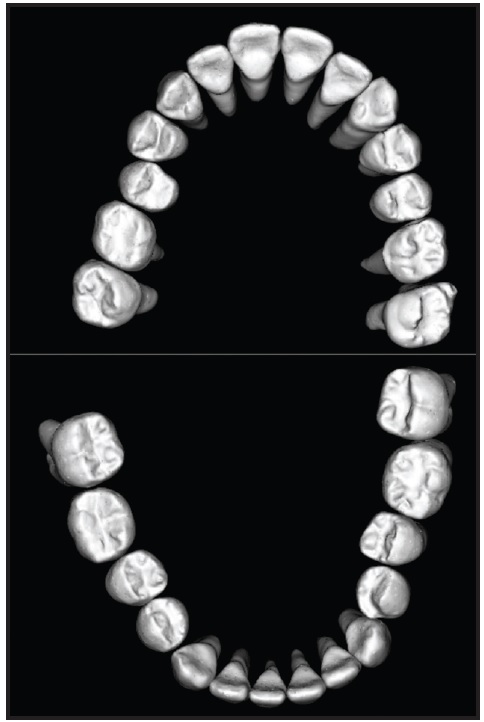
Fig. 2 Anatomage shape-matching of teeth from CBCT with teeth from intraoral scan (IS), used in surgical-orthodontic treatment planning for 26-year-old male with Class III malocclusion. Note excellent detail of crowns; slight interproximal spaces appear because teeth have been sectioned apart so they can be moved with tools to desired positions.
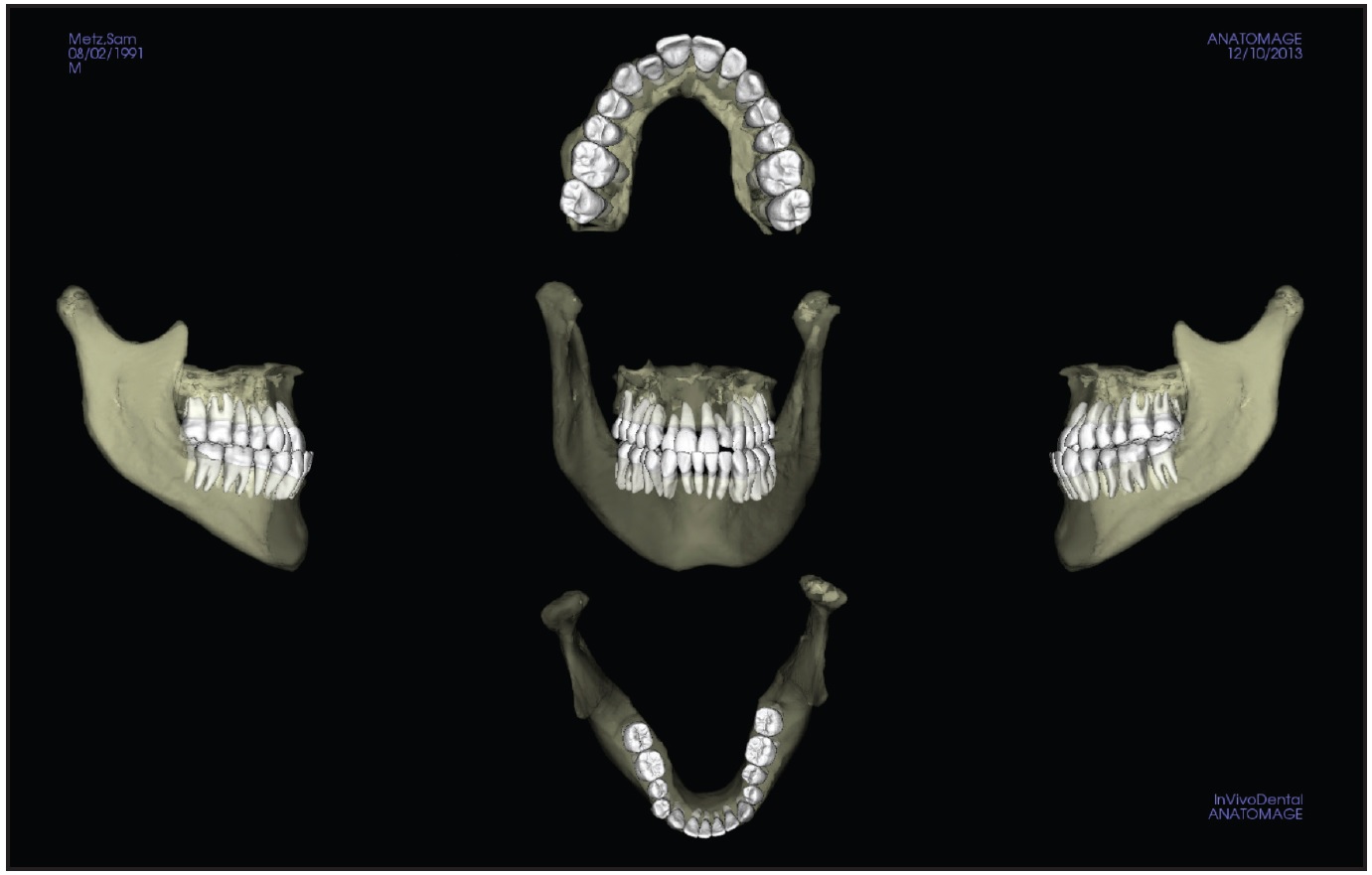
Fig. 3 In merged IS-CBCT, maxillary and mandibular arches are placed within jaw structure to form bony models that can be moved into correct locations with operator tools from Anatomodel.
In the near future, we will also be able to relate two different time points in treatment with these combined IS-CBCT images, allowing us to determine three-dimensional differences in tooth movement with 6º of freedom. This will require accurate superimposition on a reference such as the cranial base, which changes very little as growth completes in adolescents and even less in adults. We are already using Anatomage software to measure 3D tooth displacements against a volume reference in the cranium. Align Technology is finalizing its own software, called Quantify, which will be made available to all qualified investigators for a better understanding how teeth really move in space (Fig. 4; Figure 4 video sequence is available on the JCO Facebook page).
ROBERT L. BOYD, DDS, MEd
ACKNOWLEDGMENTS: I want to thank my fellow faculty member, Dr. Joorok Park, and resident, Dr. Armin Vahidnia, for their assistance in the preparation of these figures.
Fig. 4 Experimental software integrating CBCT and IS, supplied by Srini Kaza of Align Technology. Teeth can be moved as in standard Invisalign treatment plan, using Treat software, and shown to doctor as lower-resolution ClinCheck models for approval.