Prediction of Maxillary Lateral-Incisor Root Resorption Using Sector Analysis of Potentially Impacted Canines
Other than the third molars, the maxillary canine is the most frequently impacted tooth in the dental arch. Although the incidence of canine impaction is about 1 in 100 in the general population,1 the ratio tends to be much higher in an orthodontic practice--perhaps as high as 23.5%, according to one researcher.2 Palatal impactions are more prevalent (85%) than labial impactions (15%).3-5
Early detection of impactions is critical to the success of orthodontic treatment. Ericson and Kurol found that the more mesially located the crown of an impacted canine, the lower the likelihood of its eruption after deciduous extraction.6 Power and Short found that if a canine is angled more than 31º to the midline, its chance of eruption after deciduous extraction is reduced.7 Lindauer and colleagues, drawing on the work of Ericson and Kurol,6 developed a method for predicting eruption after deciduous extraction, based on the location of the impacted canine cusp tip and its relationship to the adjacent lateral incisor.8
Dividing impacted canines into four groups--sectors I through IV, with sector IV representing the most severe impaction-- they determined that as many as 78% of the canines with cusp tips in sectors II through IV were destined to become impacted (Fig. 1). Warford and colleagues reported that 82% of all impacted canines were classified in sectors II through IV, and that angulation was not as useful as sector analysis in predicting impaction.1
Similar articles from the archive:
Root resorption is not only the most common sequela of canine impaction but the most difficult to treat. Although the maxillary lateral-incisor root is the most commonly affected by ectopic eruption of the canine,9-11 there is also evidence that impacted canines can cause root resorption of the central incisors. In a study by Bjerklin and Ericson of cases with impacted canines, 38% of the lateral incisors showed root resorption, compared to 9% of the central incisors, but every case of central-incisor root resorption also showed root resorption of the adjacent lateral incisor.12 In a similar study, Walker and colleagues found that 66% of the lateral incisors and 11% of the central incisors showed root resorption, and that 50% of the cases with root resorption of a central incisor also demonstrated root resorption of the adjacent lateral incisor.13
In this retrospective study, we used cone- beam computed tomography (CBCT) to determine whether maxillary lateral-incisor root resorption can be predicted using a conventional panoramic radiograph and sector analysis.
Materials and Methods
Records were collected from 40 patients who were screened for unilaterally or bilaterally impacted maxillary canines--a total of 64 canines. CBCT scans from an i-CAT* dental imaging scanner were retrieved from the records of the School of Dental Medicine at the State University of New York at Stony Brook and from a private oral-surgery practice. All patients had fully erupted maxillary permanent lateral incisors adjacent to the impacted canines.
A traditional two-dimensional panoramic radiograph was created from each of the three-dimensional scans, using Invivo imaging software**, and standardized in natural head position (Fig. 2A). Each impacted canine was assigned to sector I-IV according to Lindauer and colleagues8 (Fig. 1):
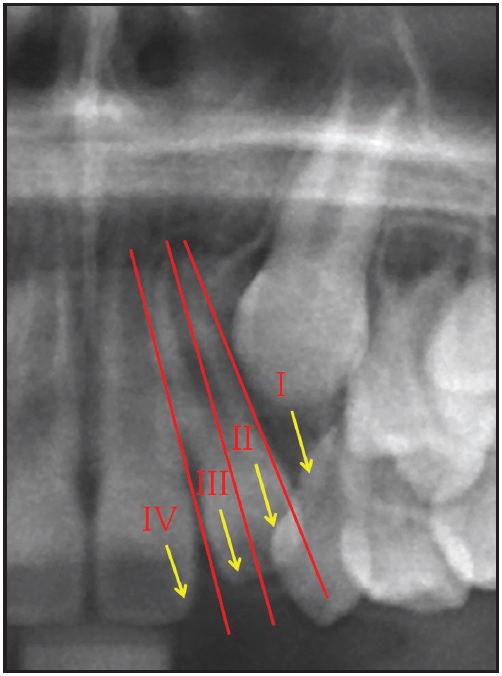
Fig. 1 Sector analysis of unerupted canines according to Lindauer and colleagues.8
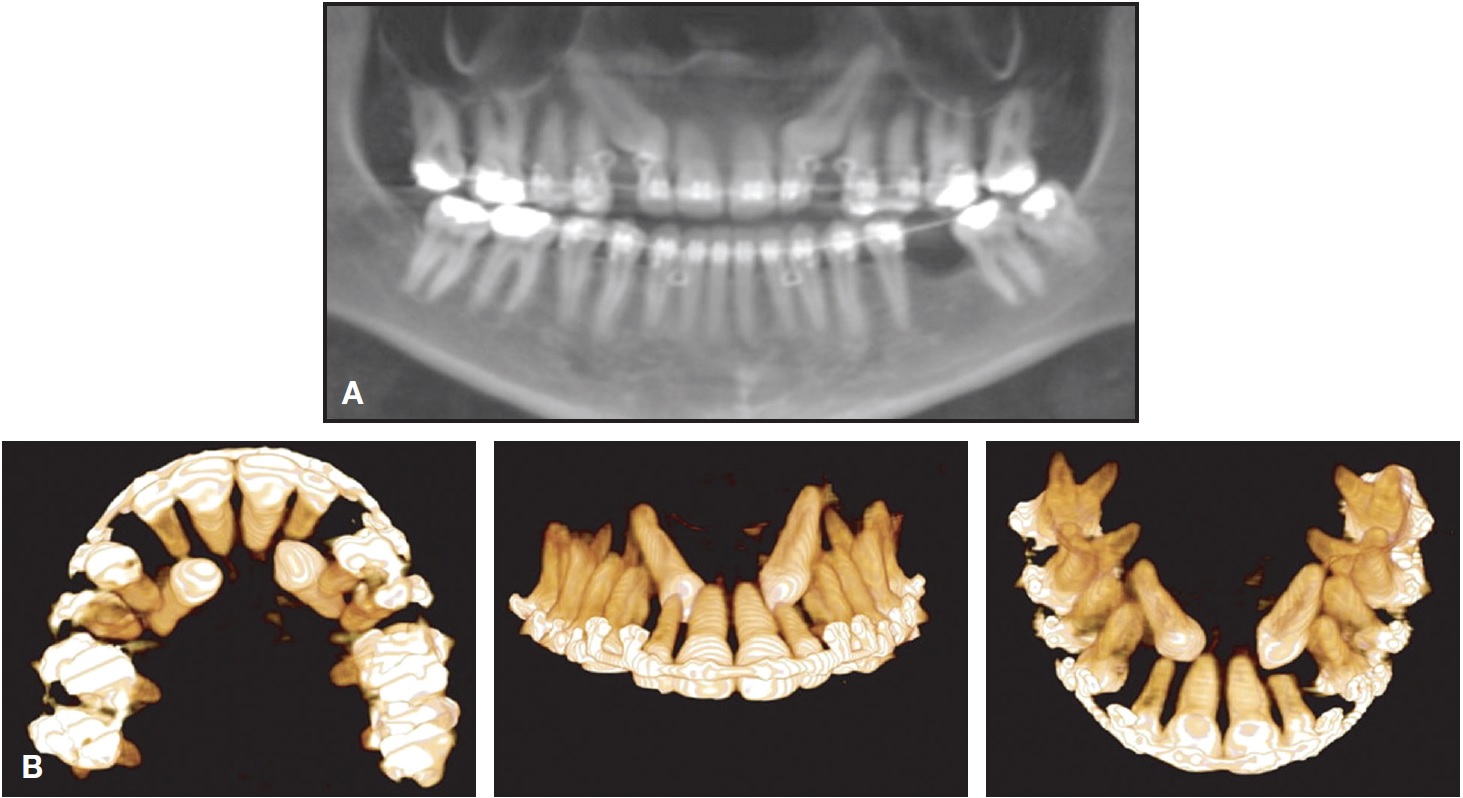
Fig. 2 A. Typical study patient’s panoramic radiograph created from cone-beam computed tomography (CBCT) for sector analysis. B. Patient’s volumetric CBCT images used to pinpoint root resorption.
• Sector I--cusp tip distal to a line tangent to the distal heights of contour of the lateral incisor crown and root.
• Sector II--mesial to sector I, with the cusp tip distal to a line bisecting the mesiodistal dimension of the lateral incisor along the long axis.
• Sector III--mesial to sector II, with the cusp tip distal to a line tangent to the mesial heights of contour of the lateral incisor crown and root.
• Sector IV--any position mesial to sector III.
The original CBCT scan was used to identify any root resorption of the adjacent lateral incisor (Fig. 2B).
Results
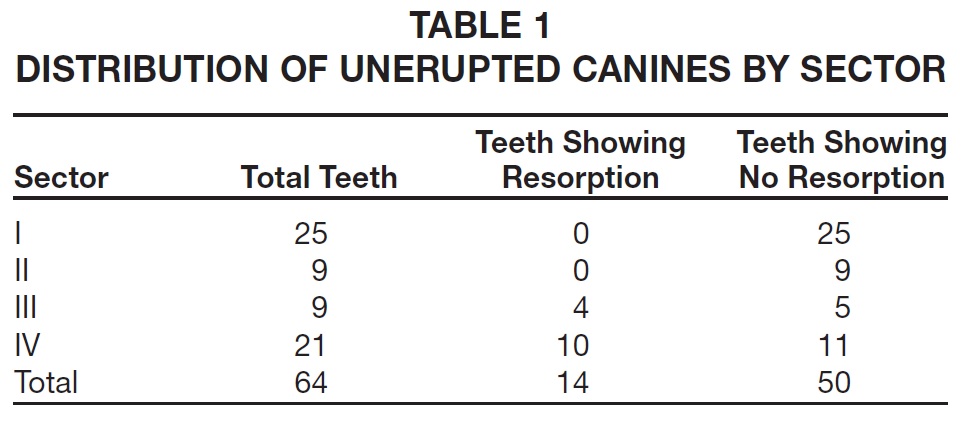
The basic results are presented in Table 1.
A logistic regression was performed using SAS 9.2 software***, with the sector (I-IV) as the common independent variable. We then chose the sector with the largest sample proportion (sector IV) as the baseline for an odds-ratio analysis (Table 2).
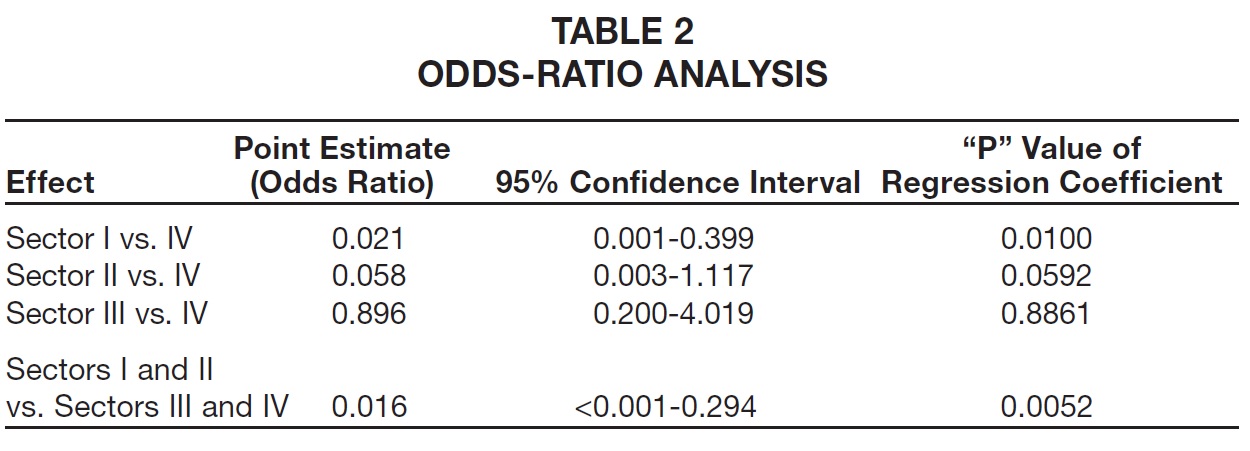
Compared to sector IV, the odds of sector I and II canines causing lateral root resorption were extremely small (.021 and .058, respectively). On the other hand, a canine in sector III had an odds ratio of .896, and the "p" value of regression coefficient for sector III was .8861, suggesting that it was no different statistically from a canine in sector IV. Furthermore, there was significantly more root resorption in sectors III and IV (p < .05) when they were combined and compared to sectors I and II.
Discussion
A pretreatment diagnosis of root resorption can drastically alter a treatment plan. In the study by Bjerklin and Ericson, diagnoses and treatment plans for 80 children with retained and ectopically positioned maxillary canines were originally based on extraoral and intraoral photos, study models, charts, conventional radiography, and, if available, lateral headfilms.12 About a year later, after supplemental medical CT scans were taken, the same examiner modified the treatment plans of 35 of the 80 children (44%). Among the patients with root resorption on the maxillary incisors adjacent to retained canines, more than half the treatment plans were altered. Without the information from the CT scans, 11 of the 80 children would not have been treated for pulp exposure due to the resorption of incisor roots, and 13 patients who showed no incisor root resorption would have had one or both lateral incisors extracted needlessly.
It can be concluded that the more severe the impaction of a canine, the more likely it is that the adjacent lateral incisor will show some level of root resorption. In our study, none of the 34 impacted canines in sectors I and II had adjacent lateral incisors with any root resorption. Of the nine canines in sector III, however, four had adjacent lateral incisors with root resorption; of the 21 canines in sector IV, 10 had adjacent lateral incisors evidencing root resorption. In other words, there was a nearly 50% chance that an impacted canine diagnosed in sector III or IV would have an associated lateral incisor with some root resorption--suggesting a "root resorption threshold" between sectors II and III.
A three-dimensional view can provide more accurate details for planning treatment of a case involving unerupted canines--including such factors as the amount of bone coverage, the volumetric size of the eruption follicle, and the stage of root development, as well as the presence of root resorption of either the lateral or central incisors. Even more important, the sector position of an unerupted canine can help determine its potential for impaction. Considering the possibility of higher levels of radiation exposure from the routine use of CBCT, however, it should not be recommended indiscriminately in all cases. Sector analysis of a panoramic radiograph can guide the practitioner in determining whether CBCT may be indicated when a potentially impacted canine is present.
FOOTNOTES
- *Registered trademark of Imaging Sciences International, LLC, Hatfield, PA; www.i-cat.com.
- **Trademark of Anatomage USA, San Jose, CA; www.anatomage.com.
- ***SAS Institute, Inc., Cary, NC; www.sas.com.
REFERENCES
- 1. Warford, J.H.; Grandhi, R.K.; and Tira, D.E.: Prediction of maxillary canine impaction using sectors and angular measurement, Am. J. Orthod. 124:651-655, 2003.
- 2. Ferguson, J.W.: Management of the unerupted maxillary canine, Br. Dent. J. 169:11-17, 1990.
- 3. Bishara, S.E.; Kommer, D.D.; McNeil, M.H.; Montagano, L.N.; Oesterle, L.J.; and Youngquist, H.W.: Management of impacted canines, Am. J. Orthod. 69:371-387, 1976.
- 4. Jacoby, H.: The etiology of maxillary canine impactions, Am. J. Orthod. 84:125-132, 1983.
- 5. Schindel, R.H. and Duffy, S.L.: Maxillary transverse discrepancies and potentially impacted maxillary canines in mixeddentition patients, Angle Orthod. 77:430-435, 2007.
- 6. Ericson, S. and Kurol, J.: Radiographic examination of ectopically erupting maxillary canines, Am. J. Orthod. 91:483-492, 1987.
- 7. Power, S.M. and Short, M.B.: An investigation into the response of palatally displaced canines to the removal of deciduous canines and an assessment of factors contributing to favorable eruption, Br. J. Orthod. 20:215-223, 1993.
- 8. Lindauer, S.J.; Rubenstein, L.K.; Hang, W.M.; Anderson, W.C.; and Isaacson, R.J.: Canine impaction identified early with panoramic radiographs, J. Am. Dent. Assoc. 123:91-92, 1992.
- 9. Arens, D.E.: An alternative treatment for severely resorbed maxillary lateral incisor: A sequela of ectopic eruption, J. Endod. 21:95-100, 1995.
- 10. Alqerban, A.; Jacobs, R.; Lambrechts, P.; Loozen, G.; and Willems, G.: Root resorption of the maxillary lateral incisor caused by impacted canine: A literature review, Clin. Oral Investig. 13:247-255, 2009.
- 11. Sameshima, G.T. and Sinclair, P.M.: Predicting and preventing root resorption: Parts I and II, Am. J. Orthod. 119:511-515, 2001.
- 12. Bjerklin, K. and Ericson, S.: How a computerized tomography examination changed the treatment plans of 80 children with retained and ectopically positioned maxillary canines, Angle Orthod. 76:43-51, 2006.
- 13. Walker, L.; Enciso, R.; and Mah, J.: Three-dimensional localization of maxillary canines with cone-beam computed tomography, Am. J. Orthod. 128:418-423, 2005.
-
 DR. SCHINDEL
DR. SCHINDEL -
 DR. SHEINIS
DR. SHEINIS
Dr. Schindel is an Associate Clinical Professor and Dr. Sheinis is a senior orthodontic resident, Department of Orthodontics and Pediatric Dentistry, School of Dental Medicine, Stony Brook University, Stony Brook, NY 11794. E-mail Dr. Schindel at schindelortho@optonline.net.