Digital Design and Manufacturing of the Lingualcare Bracket System
The first lingual orthodontic systems, introduced in the early 1970s, used conventional labial brackets that were modified by the clinician and bonded directly to the lingual surfaces. Brackets designed specifically for lingual usage1-4 were initially prone to technical problems that made them difficult to use in everyday practice.
The development of indirect bonding permitted more precise lingual bracket positioning and reduced the chairtime and labor required for bonding procedures.5-9 The next technological advance was the customization of lingual brackets with composite, which compensated for the gaps between standardized bracket bases and the variable morphology of the lingual tooth surfaces. This allowed the laboratory to incorporate much of the biomechanical plan into the brackets and their positioning, thus reducing the need for wire bending.
The Torque Angulation Reference Guide* (TARG) developed in 1984 by Ormco further improved the precision of bracket placement. Fillion added a thickness-measuring device to this system in 1987.6 Today, the most commonly used indirect laboratory procedures are:
Similar articles from the archive:
- The Lingual Plain-Wire System with Micro-Implant Anchorage July 2004
- Philippe Self-Ligating Lingual Brackets January 2002
- The Straight-Wire Concept in Lingual Orthodontics January 2001
- The Custom Lingual Appliance Setup Service** (CLASS).7 The lingual brackets are positioned on a target setup. To prevent having to use more than one transfer tray, the brackets are transferred to the working cast before the transfer tray is made.
- The Hiro System from Japan (named for its inventor).10 The brackets are positioned on a setup model, using an ideal archwire, and then transferred to the mouth using an individual mini-tray for each tooth.
- Fillion's Bonding with Equal Specific Thickness*** (BEST) system. The brackets are directly positioned on the working cast, using the modified TARG.6
- The German Transfer Optimized Positioning (TOP) System****.11-14 The setup is used for three-dimensional orientation of each tooth. Every bracket has at least a one-point contact with the teeth to minimize the volume of the appliance in the mouth. The brackets are positioned on the working cast, and a customized archwire is fabricated using computer technology.
Although the demand for lingual orthodontic treatment in Europe and Asia has boomed in recent years, there are still relatively few orthodontists in the United States providing lingual therapy. Clinicians seem to be discouraged by problems in three areas:
- Patient adaptation to the lingual appliances, especially in speech.
- Difficulty of precise finishing.
- Inaccuracy and complexity of rebonding in case of bond failures.
To address these deficiencies, Wiechmann developed a new lingual bracket system in 2001--the Lingualcare† concept.15-18 His goal was to improve the viability of lingual treatment by making the appliance more comfortable for the patient and easier to handle for the practitioner.
System Design
The unique aspect of the Lingualcare bracket is its computerized fabrication from a gold alloy. In this process, the clinician can choose how each bracket is designed and positioned on the base according to the specific treatment philosophy and type of malocclusion. Although the term "individualization" has been applied to a variety of different concepts in the past, it is taken to its full extent with this system by using state-of-the-art, computer-aided design/computer-aided manufacturing (CAD/CAM) software. The two processes of bracket production and bracket positioning are fused into one operation, and the archwires are also customized, as in the TOP system.11
Advantages of Lingualcare include:
- Improved patient comfort, thanks to a customized bracket that is smaller in profile and closer to the tooth.19,20
- Optimal finishing, due in part to extremely precise slot geometry.
- Ease of direct rebonding of the large, customized bracket base, which intimately conforms to the lingual tooth surface.
Bracket Manufacturing
A two-phase polyvinyl siloxane impression is taken to make two sets of casts, one of which is used to fabricate an individual target setup. Non-contact scanning of the therapeutic setup is performed with a high-resolution, optical three dimensional scanner‡. This device images the cast from various perspectives to create a compound surface consisting of many thousands of minute triangles (standard triangulation language), which can be viewed from any angle (Fig. 1).
The digital model is then oriented three-dimensionally along the plane of the slot positions (Fig. 2).
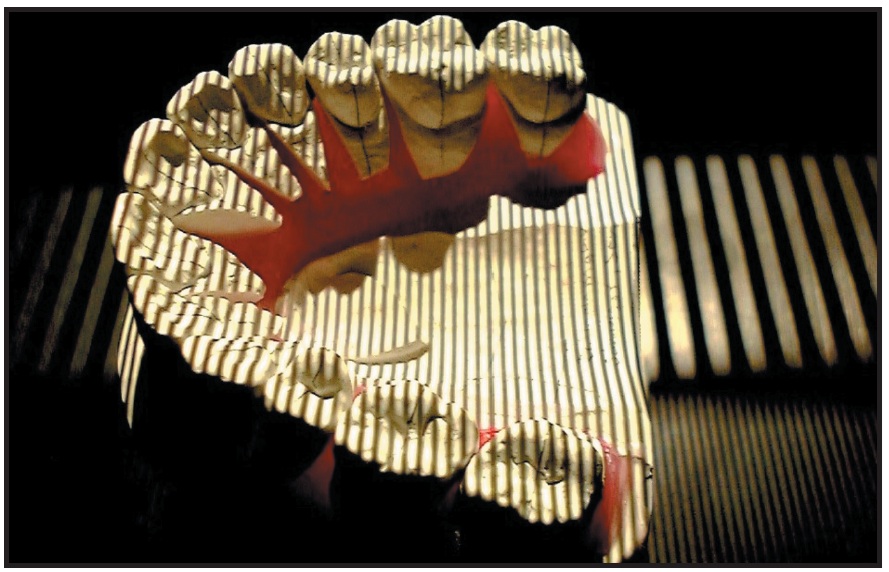
Fig. 1 Three-dimensional scanning of setup cast.
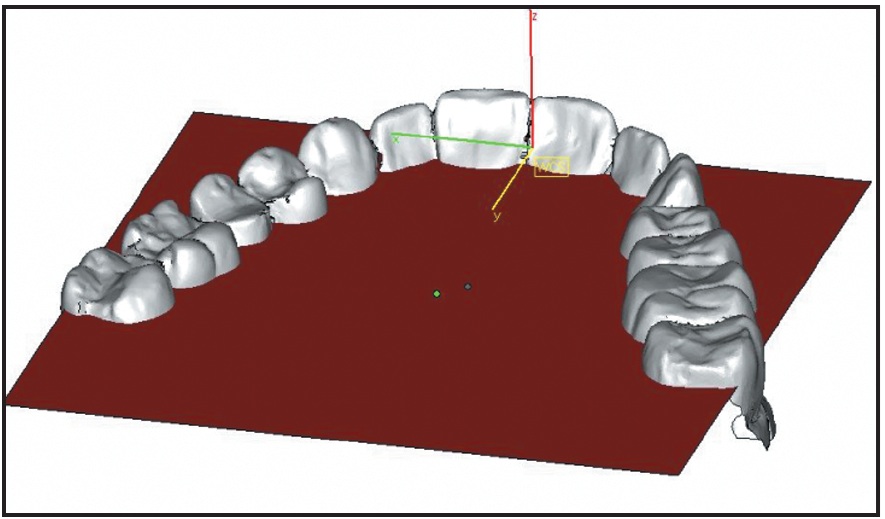
Fig. 2 Digital model oriented three-dimensionally along plane of slot positions.
The technician generates a digital bracket base for each tooth, taking into account the degree of crowding and the initial and target occlusions (Fig. 3). To avoid premature occlusal contacts on the bases, the initial and setup casts are used for reference. The pad surfaces are large enough to provide optimal bond strength and precise, form-fitting contours. The scanner is so accurate--with a resolution of at least 20 microns--that the bases will positively "lock" with the tooth surfaces, enabling unusually accurate bracket positioning.
The integrated bracket body, comprising the slot, wings, hooks, and wire-support structures, is designed with CAD/CAM software. Compared with conventional lingual brackets, the Lingualcare bracket has an extremely low profile, which allows a simplified ligation procedure without compromising control over tooth positions. The computerized bracket assembly is performed with custom software called Pro-lingual†, using standard triangulation language (Fig. 4).
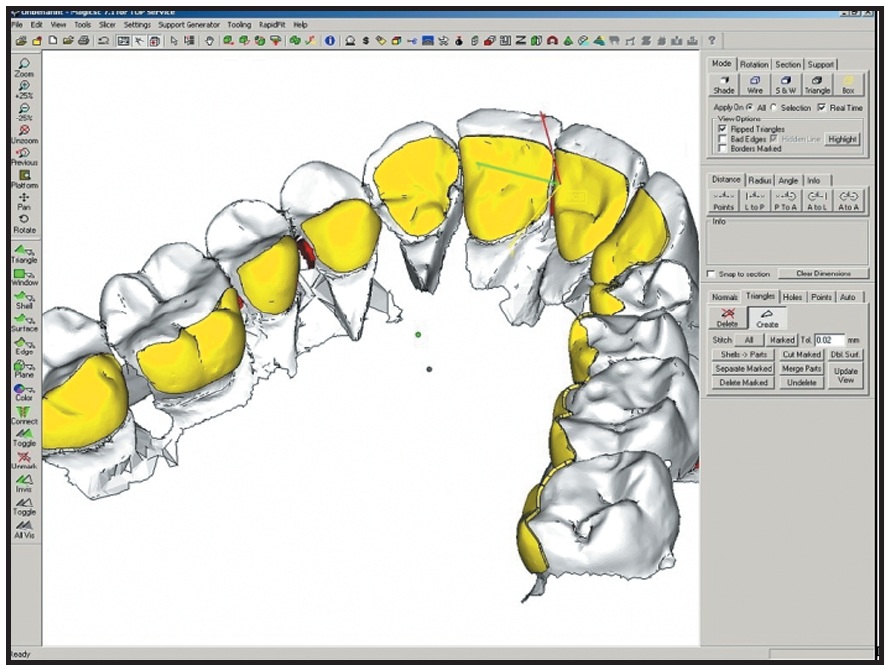
Fig. 3 Virtual bases created for all brackets.
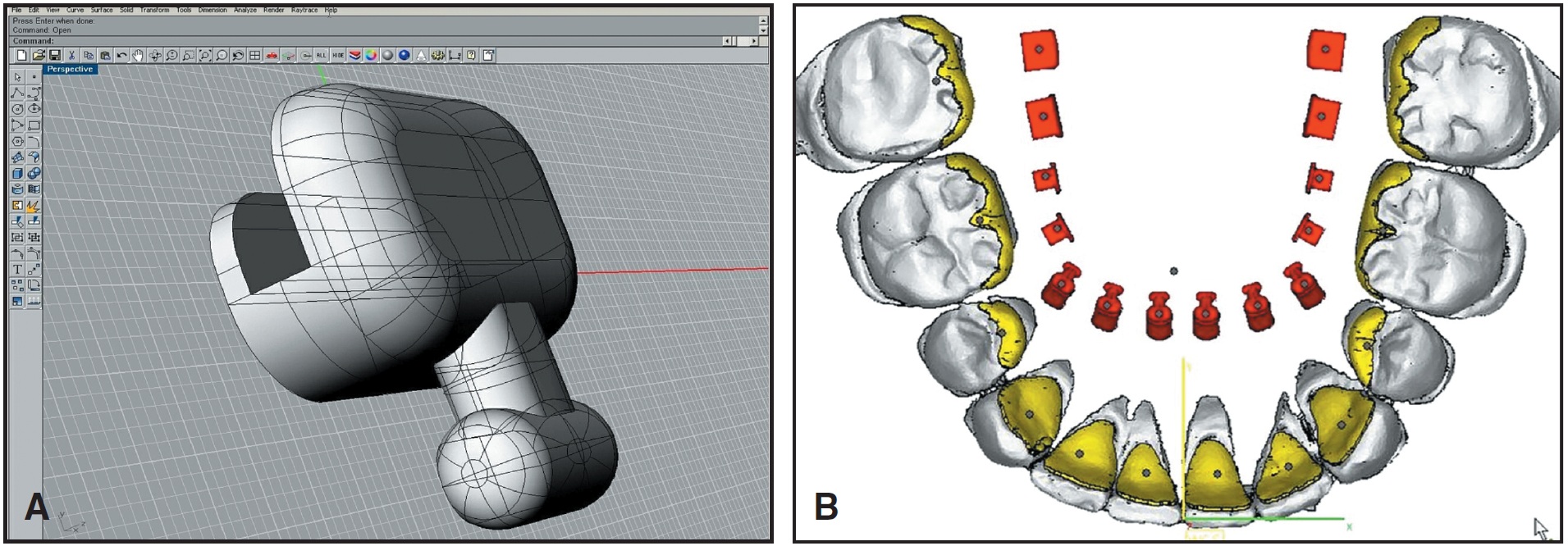
Fig. 4 A. Computerized assembly of Lingualcare bracket. B. Bracket library (red).
Digital libraries allow the clinician to select various features of the appliance, such as vertical or horizontal insertion of edgewise or ribbon archwires (Fig. 5).
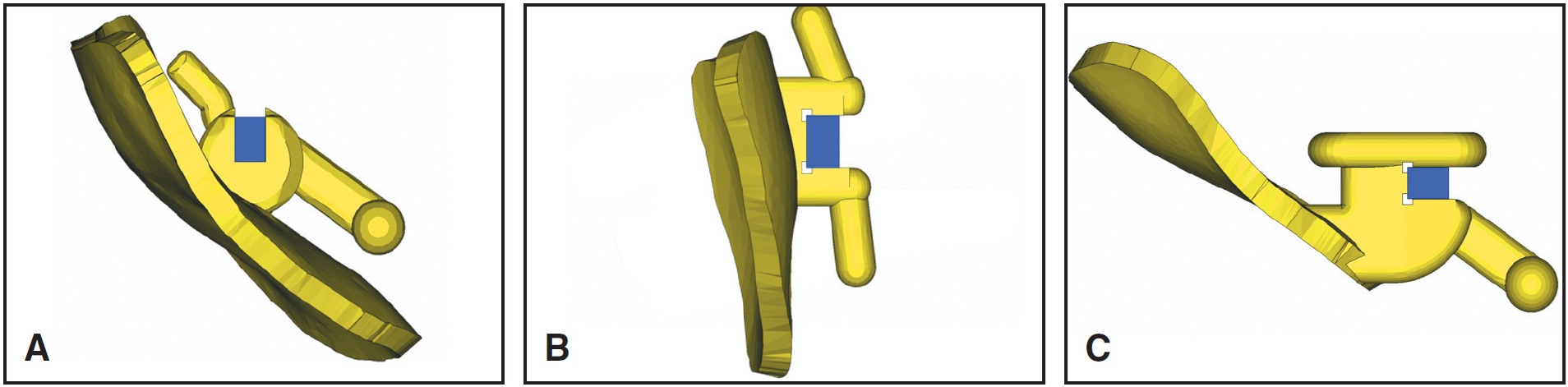
Fig. 5 A. Vertical slot with ribbon archwire. B. Horizontal slot with ribbon archwire. C. Horizontal slot with edgewise archwire.
The technician places each bracket on its base, and the program automatically aligns the slots in the virtual archwire plane (Fig. 6). The bracket height, angulation, and torque are thus preset; only the 1st-order shifting and turning is performed by the technician, who can also determine the orientation and height of the auxiliary hook (Fig. 7).
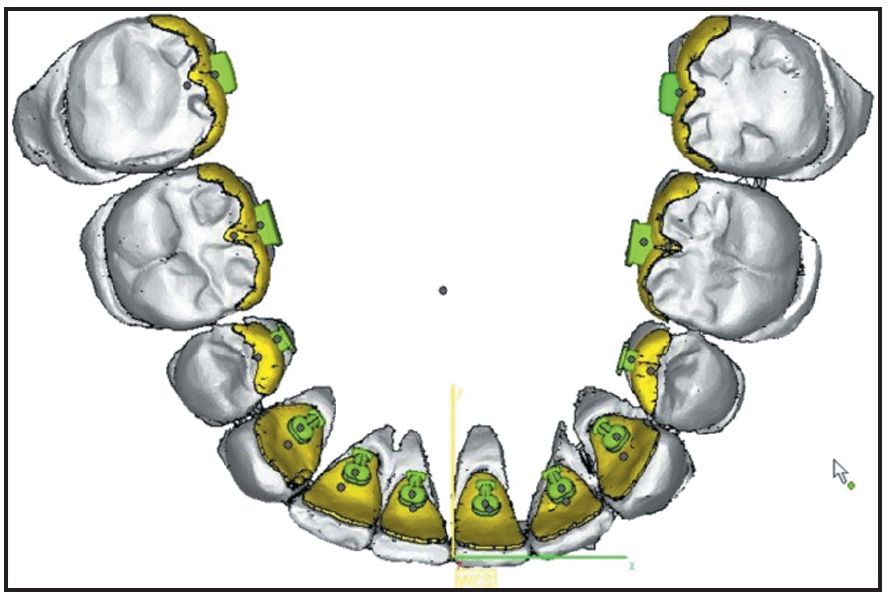
Fig. 6 Brackets virtually positioned on bases at level of slot plane.
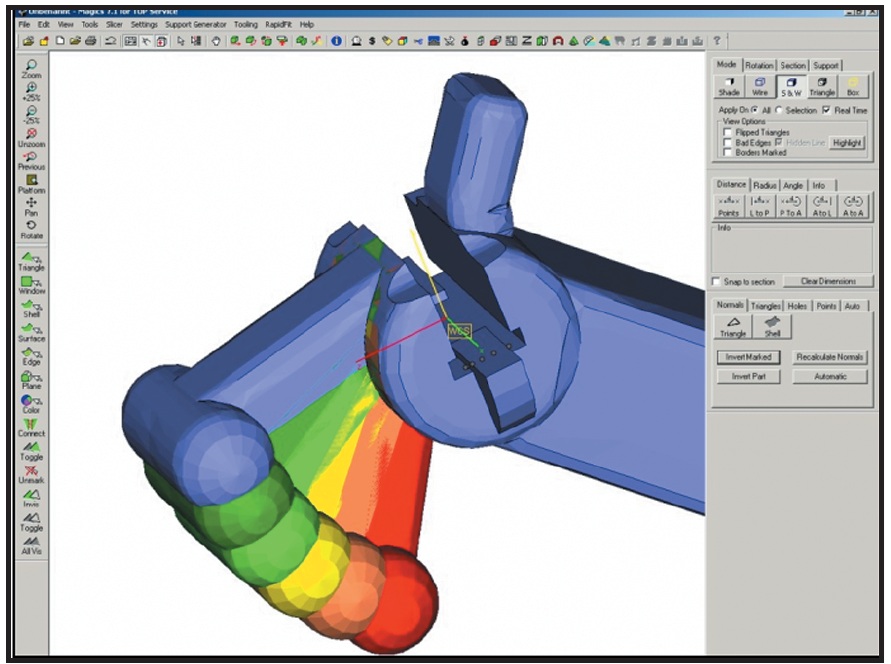
Fig. 7 Hook virtually adapted to bracket for optimum patient comfort.
A high-end rapid prototyping machine is used to convert the virtual bracket series into a wax analogue (Fig. 8). This machine uses two different colors of wax: red for the three-dimensional production and green, representing the brackets, for the casting. The wax is applied on a platform in layers thinner than 20 microns, similar to an ink-jet printer, with the green prototyping wax embedded in the red support wax. Because the melting points of the support and prototyping waxes are different, the red wax can be removed thermally. The brackets are isolated by bathing them in special solvents at a temperature of 60ºF. The technician attaches a casting spur to the "virtual" spur of each bracket, assembling the brackets like a bouquet in a tube to prepare them for investment (Fig. 9).
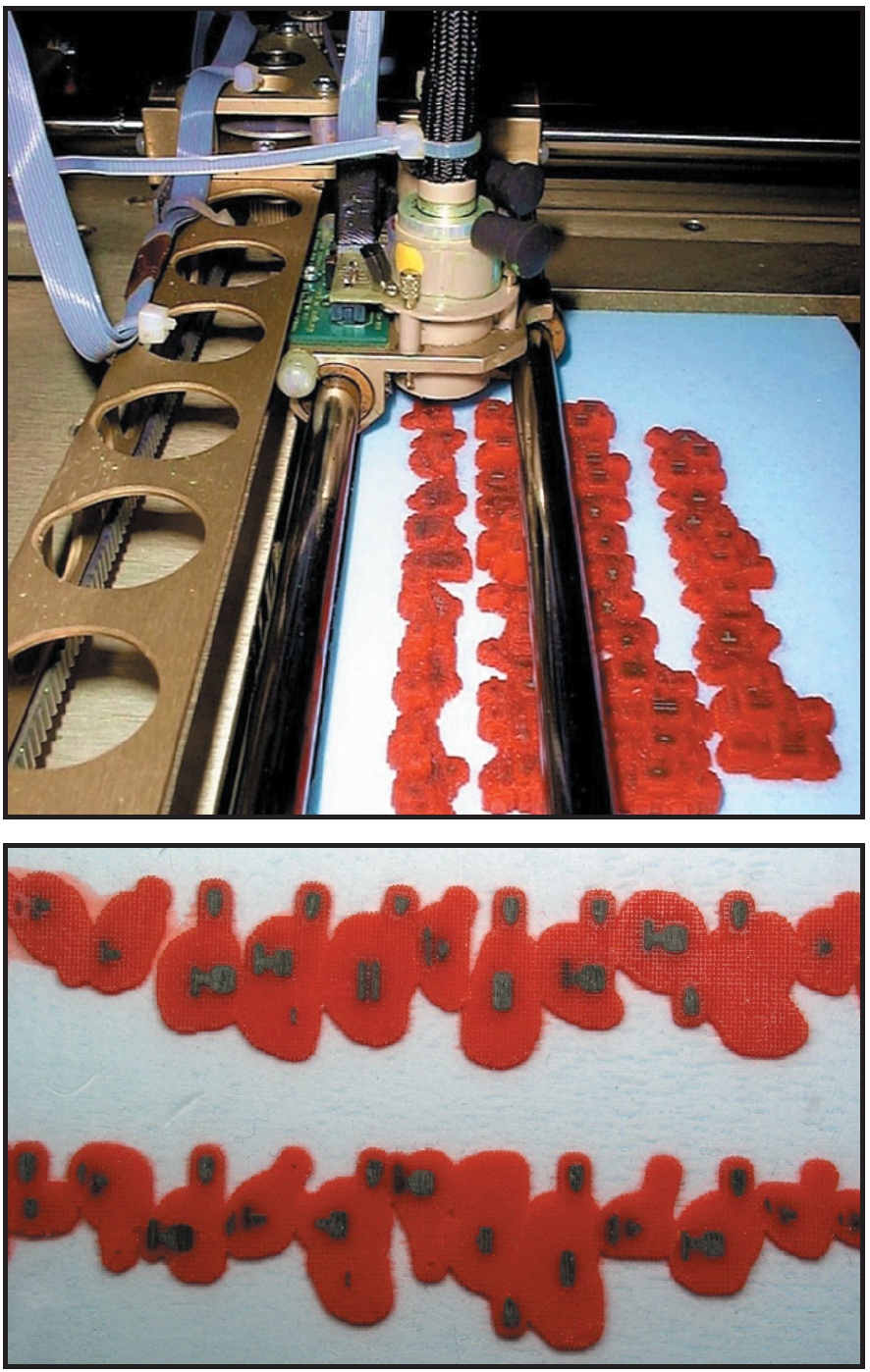
Fig. 8 Virtual bracket series converted to wax analogue.

Fig. 9 Brackets with casting spurs assembled in “bouquet” for investment.
The casting procedure, which is managed by a proprietary software program, is the same as in prosthetic dentistry. Trendgold is a Class A alloy with a hardness of 195 Vickers before casting and 305 Vickers after casting. After preheating at 690ºF, which evaporates the wax without leaving a residue, the final casting is performed by induction at 1,160ºF under an argon atmosphere (Fig. 10).

Fig. 10 Brackets cleaned and polished after casting.
The brackets are then cut away from their casting spurs, and each slot is measured with a high-precision gauge (Fig. 11). Any bracket whose slot does not measure within the allowed tolerance of .0180-.0183" is remade.
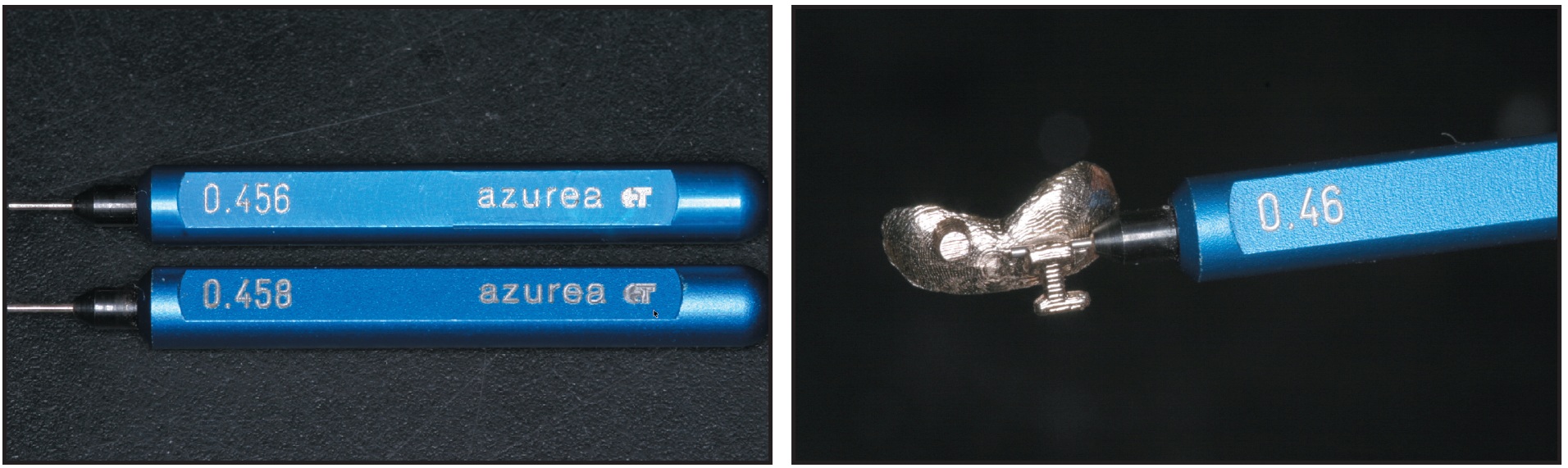
Fig. 11 Gauges used to measure slot tolerance.
Bracket Positioning
The bracket bases are sandblasted with 50-micron Rocatec-Pre†† aluminium oxide and coated with Rocatec-Plus†† to activate the surfaces, and a silane primer (ESPE Sil††) is applied. After the plaster is isolated, the brackets are directly positioned on the working cast. A filled, self-curing composite (Phase II A and B‡‡) is applied to the bracket bases in an ultra-thin layer, and excess composite is removed. The customized bases should "lock" readily to the lingual surfaces of the teeth.
A two-part indirect bonding tray is made with an inner, soft silicone (Exact N§) covering the brackets and an outer, hard silicone (Lutesil§) covering the soft silicone layer and the teeth (Fig. 12). The technician slightly uncovers the hooks for easier removal of the transfer tray after bonding. Finally, the bonding tray is trimmed and prepared for patient use.
Discussion
Custom fabrication of the Lingualcare brackets guarantees an exact fit with an extremely low profile, providing absolute control over bodily tooth movements. Modular construction allows the individual components of the system--base, bracket, and hook--to be positioned independently. Even in cases with severe crowding or short clinical roots, the enamel area will be sufficient to provide absolute control over bodily tooth movements (Fig. 13).
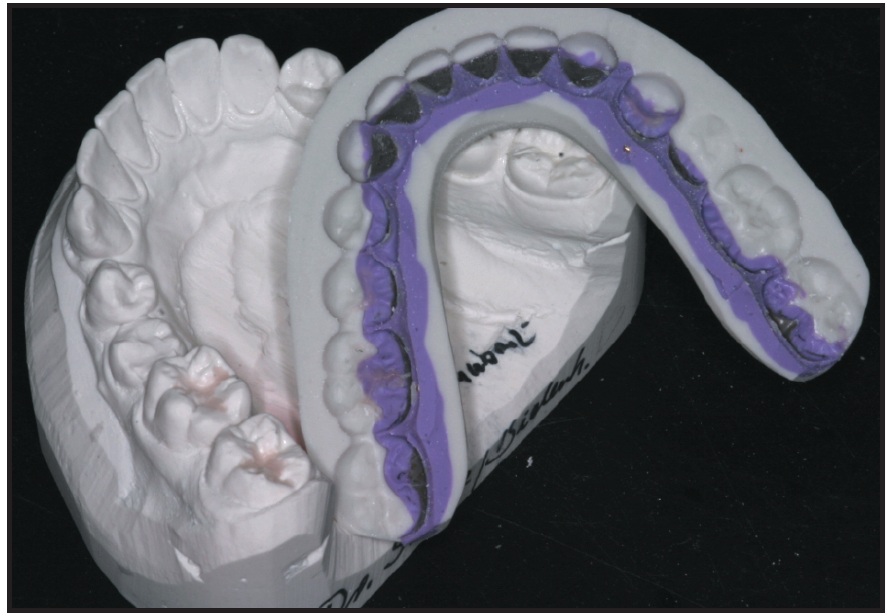
Fig. 12 Two-part silicone transfer tray
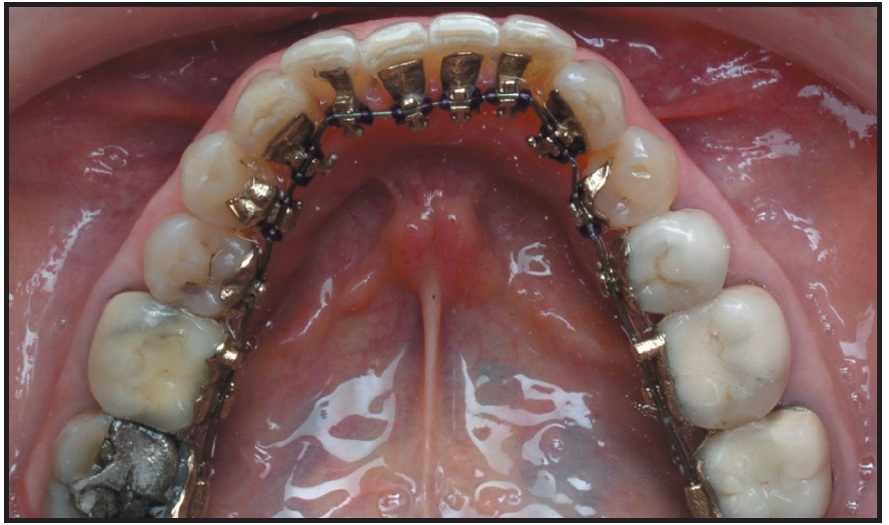
Fig. 13 Customized appliance design allows incisors to be bonded along with rest of arch, even in crowded cases.
The three-dimensional slot precision achieved during the manufacturing process results in minimal archwire play, allowing immediate insertion of a full-size, computer-designed archwire (Fig. 14).
The distance from the bracket to the tooth plays an important role in how torque is expressed. In general, the greater the distance from the bracket to the tooth, the greater the impact of errors in torque.21 Because the Lingualcare brackets are so close to the tooth surfaces (Fig. 15), the torque control provided by the system can greatly improve the accuracy of finishing procedures.

Fig. 14 Customized archwire-bending robot.
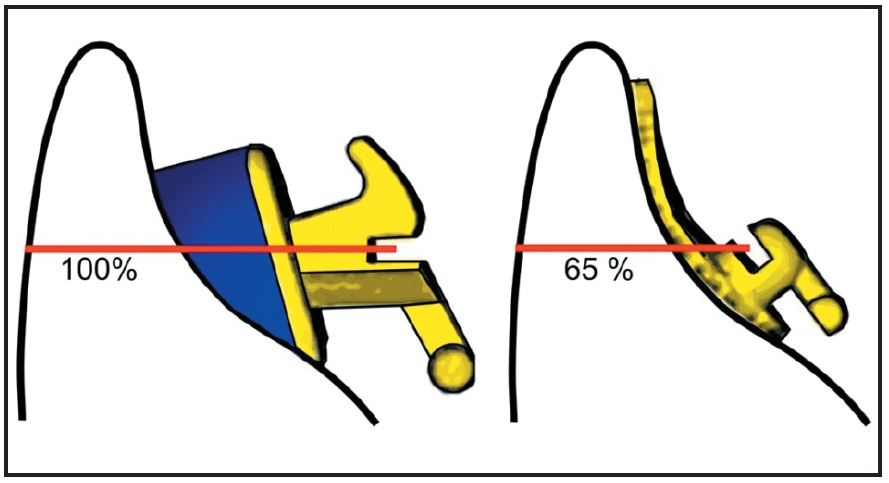
Fig. 15 Incorrect torque has less impact with Lingualcare bracket base, due to reduced distance between bracket slot and tooth surface.
The extended base of the Lingualcare bracket allows direct rebonding, as the bracket positively "locks" onto the lingual tooth surface without the need for a single-tooth transfer tray (Fig. 16). For teeth with fewer morphological features, such as the lower incisors, a printout of the three-dimensional bracket-positioning chart serves as an additional rebonding aid (Fig. 17)

Fig. 16 Form-fitting bracket base allows direct rebonding.
Conclusion
The Lingualcare system resolves many of the problems traditionally associated with lingual orthodontics, including the precision of finishing procedures and the efficiency of bonding and rebonding.22 Patient comfort is improved by a low-profile, form-fitting appliance; speech is less affected, and the tongue less irritated. The gold alloy also offers an alternative to patients with nickel allergies.
FOOTNOTES
- *Registered trademark of Ormco/“A” Company, 1717 W. Collins Ave., Orange, CO 92867.
- **AOA Orthodontic Appliances, P.O. Box 725, Sturtevant, WI 53177.
- ***ELOS, 145, rue Louis Rouquier, 92300 Le Vallois, France.
- ****T.O.P. Service, Lindenstrasse 42, 49152 Bad Essen, Germany.
- †Trademark of Lingualcare, Inc., 5304 Beltline Road, Dallas, TX 75254. Sold as Incognito outside North and South America by T.O.P. Service, Bad Essen, Germany.
- ‡GOM, Braunschweig, Germany.
- ††Trademark of 3M ESPE Dental Products, St. Paul, MN.
- ‡‡Registered trademark of Reliance Orthodontic Products, Inc., P.O. Box 678, Itasca, IL 60143.
- §Bisico, Johanneswerkstrasse 3, 33611 Bielefeld, Germany.
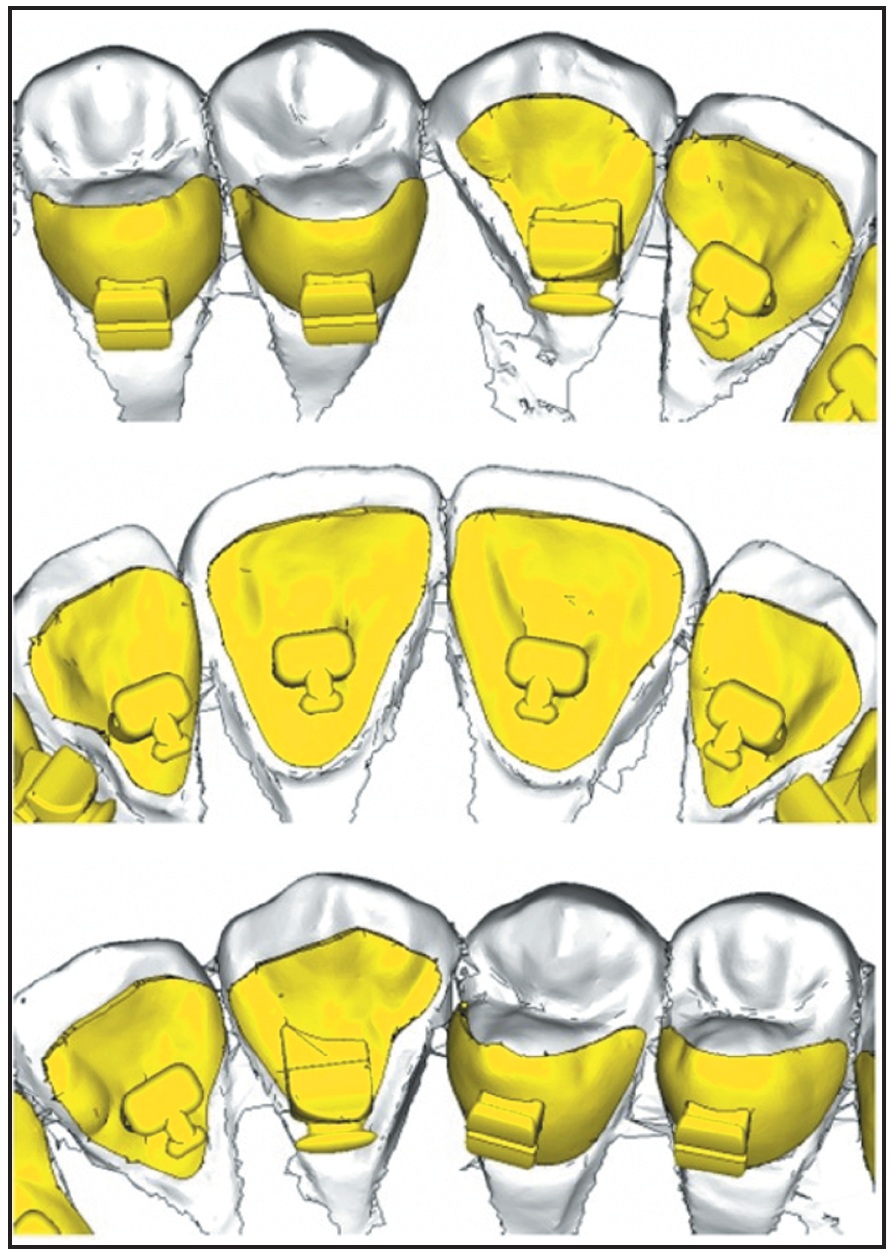
Fig. 17 Printout of three-dimensional bracket-positioning chart assists in rebonding.
REFERENCES
- 1. Kurz, C.R.; Swartz, M.L.; and Andreiko, C.: Lingual orthodontics: A status report, Part 2: Research and development, J. Clin. Orthod. 16:735-740, 1982.
- 2. Fujita, K.: Development of lingual-bracket technique, J. Jap. Orthod. Soc. 37:36-39, 1978.
- 3. Fujita, K.: Multilingual-bracket and mushroom arch wire technique: A clinical report, Am. J. Orthod. 82:120-140, 1982.
- 4. JCO Interviews Dr. Vincent M. Kelly on lingual orthodontics, J. Clin. Orthod. 16:461-476, 1982.
- 5. Creekmore, T.: Lingual orthodontics—its renaissance, Am. J. Orthod. 96:120-137, 1989.
- 6. Fillion, D. and Leclerc, J.F.: L’orthodontie linguale: Pourquoi est-elle en progrès? Orthod. Fr. 62:793-801, 1991.
- 7. Huge, S.A.: The customised lingual appliance set-up service (CLASS) system, in Lingual Orthodontics, ed. R. Romano, B.C. Decker, London, 1998, pp. 163-173.
- 8. Smith, J.R., Gorman, J.C.; Kurz, C.; and Dunn, R.M.: Keys to success in lingual therapy: Part 1, J. Clin. Orthod. 20:252-261, 1986.
- 9. Wiechmann, D.: Lingual orthodontics, Part 1: Laboratory procedure, J. Orofac. Orthop. 60:371-379, 1999.
- 10. Hiro, T. and Takemoto, K.: Resin core indirect bonding system—improvement of lingual orthodontic treatment, J. Jap. Orthod. Soc. 57:83-91, 1998.
- 11. Wiechmann, D.: Lingual orthodontics, Part 2: Archwire fabrication, J. Orofac. Orthop. 60:416-426, 1999.
- 12. Rummel, V.; Wiechmann, D.; and Sachdeva, R.: Precision finishing in lingual orthodontics, J. Clin. Orthod. 33:101-113, 1999.
- 13. Wiechmann, D.: Lingual orthodontics, Part 3: Intraoral sandblasting and indirect bonding, J. Orofac. Orthop. 61:280-291, 2000.
- 14. Wiechmann, D.: Lingual orthodontics, Part 4: Economic lingual treatment (ECO-lingual therapy), J. Orofac. Orthop. 61:359-370, 2000.
- 15. Wiechmann, D.: A new bracket system for lingual orthodontic treatment, Part 1: Theoretical background and development, J. Orofac. Orthop. 63:234-245, 2002.
- 16. Wiechmann, D.: La thérapeutique eco-linguale, Première partie: Une théorie pour un concept moderne de traitement lingual, J. Edge. 42:53-69, 2000
- 17. Wiechmann, D.: La thérapeutique eco-linguale, Deuxième partie: Aspects cliniques, J. Edge. 43:9-37, 2001.
- 18. Wiechmann, D.; Rummel, V.; Thalheim, A.; Simon, J.S.; and Wiechmann, L.: Customized brackets and archwires for lingual orthodontic treatment, Am. J. Orthod. 124:593-599, 2003.
- 19. Hohoff, A.; Stamm, T.; Goder, G.; Sauerland, C.; Ehmer, U.; and Seifert, E.: Comparison of three bonded lingual appliances by auditive analysis and subjective assessment, Am. J. Orthod. 124:737-745, 2003
- 20. Hohoff, A.; Stamm, T.; and Ehmer, U.: Comparison of the effect on oral discomfort of two positioning techniques with lingual brackets, Angle Orthod. 74:226-233, 2004.
- 21. Stamm, T.; Wiechmann, D.; Heinecken, A.; and Ehmer, U.: Relation between second and third order problems in lingual orthodontic treatment, J. Ling. Orthod. 3:5-11, 2000.
- 22. Galletti-Schweitz, C. and Garcia, R.: Orthodontie linguale—une technique d’avenir, Inf. Dent. 86:2043-2051, 2004.
-
 DR. MUJAGIC
DR. MUJAGIC -
 DR. FAUQUET
DR. FAUQUET -
DR. GALLETTI
-
DR. PALOT
-
DR. WIECHMANN
-
DR. MAH
Dr. Mujagic is a Clinical Assistant Professor, Department of Lingual Orthodontics; Dr. Fauquet is an Associate Professor and Dr. Galletti is a former Associate Professor, Department of Orthodontics, Paris VII University, France. Dr. Palot is Head, Orthodontic Department, Dental College, University of Reims-Champagne, Ardenne, France. Dr. Wiechmann is the owner of T.O.P. Service, Bad Essen, Germany. Dr. Mah is a Contributing Editor of the Journal of Clinical Orthodontics and an Assistant Professor, Division of Craniofacial Sciences and Therapeutics, University of Southern California School of Dentistry, Los Angeles ,CA. Contact Dr. Mujagic at R & S, 3, rue Saint Julien, 54000 Nancy, France; e-mail: magalimujagic@free.fr.