In orthodontic treatment, esthetics has traditionally been associated with profile enhancement. Both the Angle classification of malocclusion and the cephalometric analysis have focused attention on the profile, without considering the frontal view. Even though patients come to us mainly to improve their smiles, the orthodontic literature contains more studies on skeletal structure than on soft-tissue structure, and the smile still receives relatively little attention.
The purpose of this article is to review the eight major components of the smile (Fig. 1) and discuss their impact on orthodontic diagnosis and treatment planning.
1. Lip Line
The lip line is the amount of vertical tooth exposure in smiling--in other words, the height of the upper lip relative to the maxillary central incisors. As a general guideline, the lip line is optimal when the upper lip reaches the gingival margin, displaying the total cervicoincisal length of the maxillary central incisors, along with the interproximal gingivae.1,2 A high lip line exposes all of the clinical crowns plus a contiguous band of gingival tissue, whereas a low lip line displays less than 75% of the maxillary anterior teeth.3,4 Because female lip lines are an average 1.5mm higher than male lip lines, 1-2mm of gingival display at maximum smile could be considered normal for females.3,5,6 Dental professionals have been conditioned to see a "gummy smile" as undesirable, but some gingival display is certainly acceptable, and is even considered a sign of youthful appearance.7,8
Similar articles from the archive:
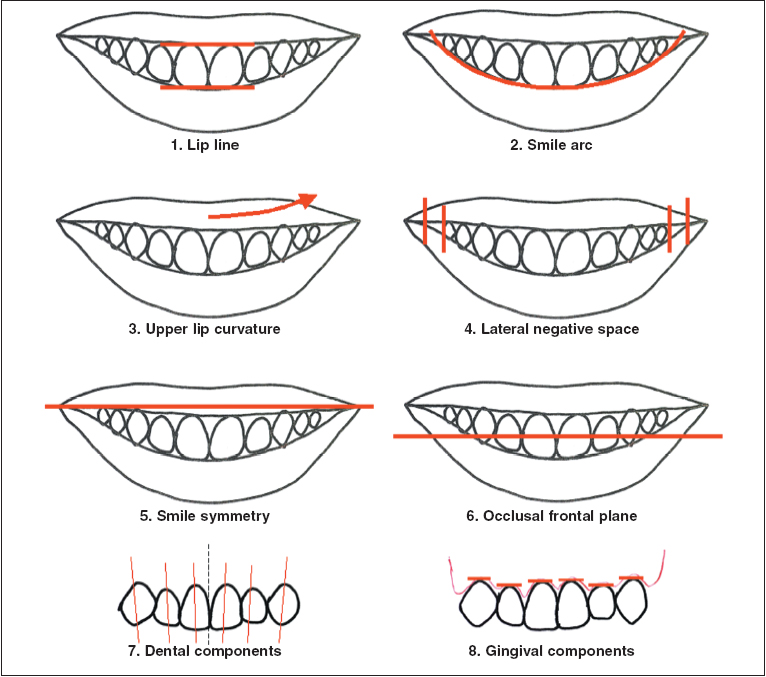
Fig. 1 Eight components of balanced smile.
The starting point of a smile is the lip line at rest, with an average maxillary incisor display of 1.91mm in men and nearly twice that amount, 3.40mm, in women.9 With aging, there is a gradual decrease in exposure of the maxillary incisors at rest and, to a much lesser degree, in smiling.4,9,10 This steady decline in maxillary tooth exposure at rest is accompanied by an increase in mandibular incisor display.9,11
It is important to differentiate between the posed smile and the spontaneous smile. A posed smile is the voluntary expression made when introduced to someone, or when taking a passport photograph or orthodontic records. A posed smile is repeatable; studies have found little difference among numerous consecutive photographs of posed smiles by the same individuals.1,6,12-15 A spontaneous smile, by contrast, is involuntary, natural, and driven by emotions. With all the muscles of facial expression involved, a spontaneous smile always has more lip elevation than a posed smile.16 Most studies refer to the posed smile because it is reproducible and can therefore be used as a reference position.13,15,17
The amount of vertical exposure in smiling depends on the following six factors.
Upper Lip Length
The average lip length at rest, as measured from subnasale to the most inferior portion of the upper lip at the midline, is about 23mm in males and 20mm in females (Table 1). What is significant, however, is the relationship of the upper lip to the maxillary incisors and to the commissures of the mouth.12 Lip length should be roughly equal to the commissure height, which is the vertical distance between the commissure and a horizontal line from subnasale (Fig. 2A).
A short lip length relative to commissure height results in an unesthetic, reverse-resting upper lip line23 (Fig. 2B). It is not easy to alter commissure height, but lip lengthening is possible with lip surgery, either as a single procedure or in combination with a Le Fort I osteotomy.24-26 In adolescents, a short upper lip relative to commissure height could be considered normal because of the lip lengthening that continues even after vertical skeletal growth is complete.27,28 It is interesting to note that a short upper lip is not always associated with a high lip line; on the contrary, the upper lip was found to be longer in a gingival-display group than in a non-displaying sample.7
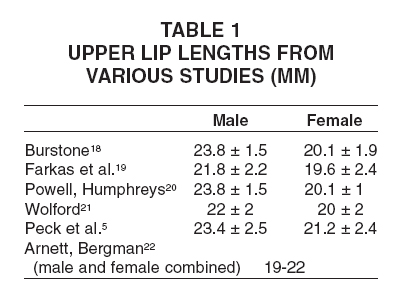
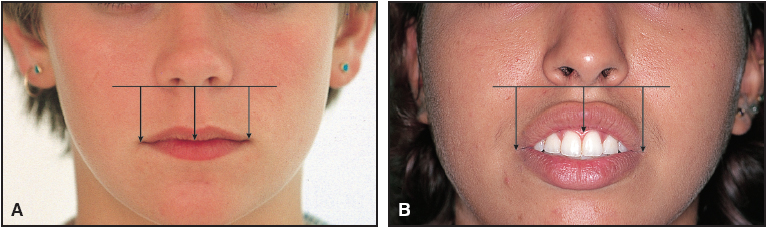
Fig. 2 Lip length compared to commissure height. A. Normal lip length at rest. B. Reverse-resting lip line.
Lip Elevation
In smiling, the upper lip is elevated by about 80% of its original length, displaying 10mm of the maxillary incisors.6 Women have 3.5% more lip elevation than men.6 Actually, there is considerable individual variability in upper lip elevation from rest position to the full smile,29 ranging from 2-12mm, with an average of 7-8mm.30 If a gingival smile is caused by a hypermobile lip, it would be a mistake to correct it with aggressive incisor intrusion or maxillary impaction surgery, because that would result in little or no incisor display at rest and thus make the patient look older. Excessive lip elevation should therefore be recognized as a limiting factor (Fig. 3).
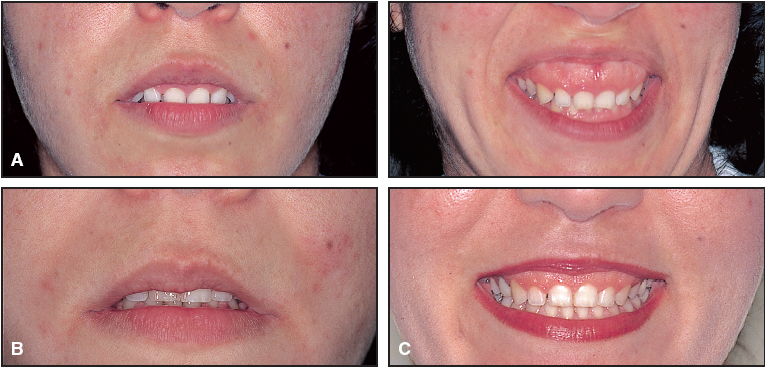
Fig. 3 A. Patient with excessive lip elevation from rest position to full smile. B,C. After orthodontics and maxillary impaction surgery. Persistence of some gingival display after treatment (C) is due to hypermobile lip and short clinical crowns. More surgical impaction would have resulted in no incisor display at rest (B).
Likewise, if a low lip line is due to a hypomobile lip (Fig. 4), extensive incisor extrusion would result in an overbite with excessive incisor display at rest.
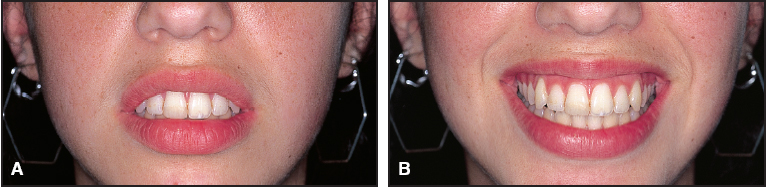
Fig. 4 Patient with limited lip elevation from rest position to full smile. Absence of gingival display (B) despite high lip line at rest (A) is due to hypomobile lip.
Vertical Maxillary Height
The importance of the vertical position of the maxilla in tooth display has been demonstrated in both prosthetic dentistry and orthognathic surgery. When upper lip length and mobility are normal, a gingival smile with excessive incisor display at rest can be attributed to vertical maxillary excess. This kind of "skeletal" gingival smile is generally associated with excessive lower facial height. Conversely, a low lip line with no incisor display at rest is "skeletal" when associated with inadequate lower facial height due to a vertically deficient maxilla (Fig. 5).
The best reference for impacting or lengthening the maxilla is the incisor display at rest, taking upper lip length and any incisor attrition into account. The full smile does not make a good reference, partly because of the individual variation in lip mobility.30 A short upper lip should not be treated by shortening the maxilla unless the facial outline can accommodate such a change.22 It should also be noted that in maxillary impaction, the upper lip shortens by as much as 50% of the surgical skeletal intrusion.31
Crown Height
The average vertical height of the maxillary central incisor is 10.6mm in males and 9.8mm in females.5,32 A short crown can be due to attrition or excessive gingival encroachment. If there is little or no incisor display at rest, but the lip line is normal in smiling, the crown height can be increased incisally with cosmetic dentistry. A gingivectomy or a crown-lengthening procedure with crestal bone removal is recommended when short clinical crowns are associated with a gingival smile and a normal incisor display at rest33,34 (Fig. 6).
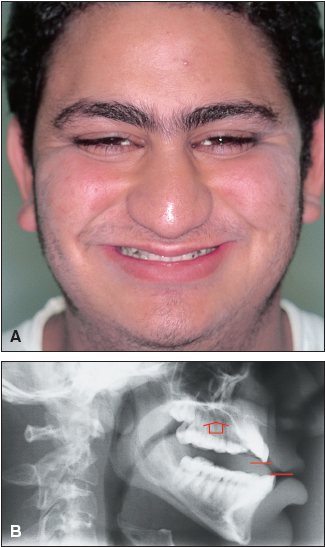
Fig. 5 A. Patient with low lip line due to vertical maxillary deficiency. B. Lateral cephalogram taken in rest position is used to measure “negative” lip line at rest.

Fig. 6 A. Patient with gingival smile, overbite, and short clinical crowns. B. After orthodontic maxillary incisor intrusion and crown-lengthening surgery.
Vertical Dental Height
As mentioned earlier, the incisor exposure at rest, rather than the overbite, determines the vertical position of the incisal edge, all other factors being equal. Therefore, a deep bite should be corrected by maxillary incisor intrusion in a patient with excessive incisor display at rest, but with posterior extrusion and/or lower incisor intrusion in a patient with a normal lip line at rest. The opposite applies to an open bite, which should be corrected by maxillary incisor extrusion if there is inadequate incisor display at rest, but with posterior intrusion and/or lower incisor extrusion if the lip line is normal at rest.
Incisor Inclination
Proclined maxillary incisors, whether in a Class II, division 1 malocclusion or in a Class III compensation, tend to reduce the incisor display at rest and in smiling (Fig. 7). On the other hand, uprighted or retroclined maxillary incisors, as seen in Class II, division 2 malocclusion or after orthodontic retraction without torque control, tend to increase the incisor display.12 Maxillary incisor inclination can best be assessed on profile and oblique smiling photographs, which should become standard orthodontic records.35
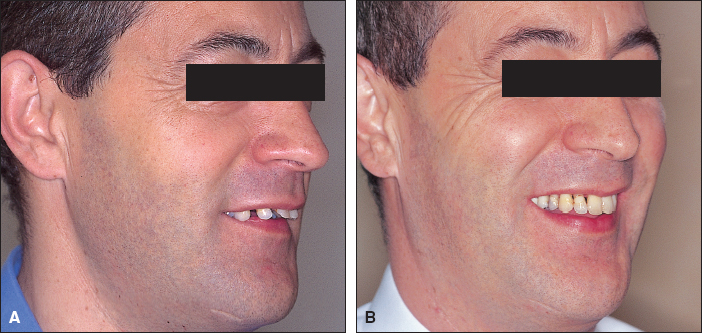
Fig. 7 A. Lip line with reduced incisor display due to proclined maxillary incisors. B. Normal incisor display after orthodontic uprighting of maxillary incisors.
2. Smile Arc
The smile arc is the relationship between a hypothetical curve drawn along the edges of the maxillary anterior teeth and the inner contour of the lower lip in the posed smile.3,4,16,36-39 The curvature of the incisal edges appears to be more pronounced for women than for men, and tends to flatten with age. The curvature of the lower lip is usually more pronounced in younger smiles.38 In an optimal smile arc--described as "consonant"--the curvature of the maxillary incisal edges coincides with or parallels the border of the lower lip in smiling.35 The lower lip can either touch, not touch, or slightly cover the upper incisal edges; in one study of untreated subjects, the patients whose lower lips touched or did not touch the incisal edges had a higher esthetic score than those whose incisal edges were slightly covered (15.76% of the sample).3,4 In a "nonconsonant" smile arc, the maxillary incisal edges are either flat or reversed relative to the curvature of the lower lip16,36 (Fig. 8).
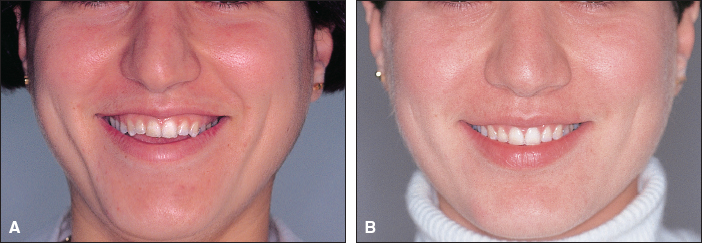
Fig. 8 A. Patient with reverse smile arc. B. Consonant smile arc after clockwise rotation of occlusal plane with orthodontics and posterior maxillary impaction surgery.
Smile arcs were found to be flatter in orthodontically treated patients than in an untreated group with normal occlusions, resulting in a "denture mouth" appearance1,40 (Fig. 9). In another study, flattening of the smile arc was found in one-third of the 30 treated patients, but in only two of the 30 untreated subjects.15 The smile arc can be unintentionally flattened during orthodontic treatment by any or all of the following three techniques.
Overintrusion of Maxillary Incisors
If the maxillary incisors are overintruded to correct an overbite or a gingival smile without considering or monitoring the incisor-lip position at rest, the smile arc may be flattened.30 Indiscriminate use of utility arches or archwires with accentuated curves can not only flatten the smile arc, but can also result in a low lip line at rest and in smiling, which ages the patient as described above.

Fig. 9 Patient with flat smile arc after orthodontic treatment.
Bracket Positioning
The same bracket heights should not be used for parallel, flat, and reverse smile arcs. If optimal smile arc esthetics are to be achieved, the bracket positions must take into account the relationship of the incisal edges to the lower lip curvature for each individual patient.16 In a reverse smile arc, for example, the brackets should be positioned higher than usual on the maxillary central incisors and progressively lower on the lateral incisors and canines.
Cant of the Occlusal Plane
Extraoral forces, intermaxillary elastics, and orthognathic surgery can affect the cant of the occlusal plane. If the maxillary occlusal plane is canted upward anteriorly, for instance, the incisal edges will move away from the lower lip, resulting in a nonconsonant smile arc (Fig. 8). Conversely, if the occlusal plane has an excessive clockwise tilt, the upper incisal edges will be covered by the lower lip, making the smile arc less attractive.
Other factors that can affect the smile arc are attrition due to shortening of the central incisors, habits such as thumbsucking, excessive posterior vertical growth (mostly seen in brachyfacial patterns), and the lower lip musculature.16 Maxillary incisor inclination affects not only the lip line, but the smile arc as well, when the curvature of the incisal edges does not coincide with the border of the lower lip in smiling (Fig. 7). Excessively proclined incisors will be associated with an everted lower lip, whereas uprighted or retroclined incisors will be partially covered by the lower lip.
3. Upper Lip Curvature
The upper lip curvature is assessed from the central position to the corner of the mouth in smiling. It is upward when the corner of the mouth is higher than the central position, straight when the corner of the mouth and the central position are at the same level, and downward when the corner of the mouth is lower than the central position1,4,41,42 (Fig. 10). Upward and straight lip curvatures are considered more esthetic than downward lip curvatures.4 In a non-orthodontic population with normal occlusions, upward lip curvatures were rare (12%), but straight (45%) and downward (43%) lip curvatures were almost equally prevalent.4 Because it is a muscle-driven position, upper lip curvature is not subject to alteration by orthodontic therapy. A downward lip curvature could therefore be considered a limiting factor in achieving an optimal smile (Fig. 10C).

Fig. 10 Upper lip curvature. A. Upward. B. Straight. C. Downward.
4. Lateral Negative Space
The transverse dimension of the smile is also referred to as "transverse dental projection". Lateral negative space is the buccal corridor between the posterior teeth and the corner of the mouth in smiling16,36 (Fig. 11A). Although the prosthodontic literature describes a smile lacking buccal corridors as unrealistic-looking and denture-like, orthodontists refer to buccal corridors as "negative" spaces to be eliminated by transverse maxillary expansion (Fig. 11B). A first-molar-to-first-molar smile is often advocated in orthodontics, but is considered evidence of a poorly constructed denture in prosthodontics.36 In studies measuring the number of teeth displayed in the smiles of young subjects with normal occlusions, those displaying the first molars were ranked the highest esthetically.4,43 A first molar display was found in only 3.7% of one sample, however, with most of the subjects (57%) displaying only the second premolars.3,4 In fact, nonextraction treatment with maxillary expansion does not necessarily improve the attractiveness of the smile.1 Research has shown that premolar extraction does not lead to arch constriction or a widening of buccal corridors.44 Furthermore, repeated surveys of lay persons have failed to establish any adverse esthetic perception of negative spaces.6,36,44
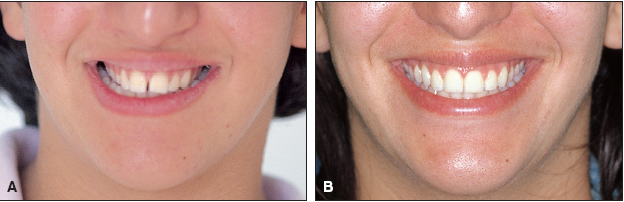
Fig. 11 A. Patient with lateral negative space. B. After rapid palatal expansion.
Archform also affects the transverse dimension of the smile: A broad arch is more likely to fill the buccal corridors than a narrow and constricted arch. In addition, buccal corridors are heavily influenced by the anteroposterior position of the maxilla relative to the lip drape. Moving the maxilla forward will reduce the negative space because a wider portion of the arch will come forward to fill the intercommissure space.12,16 In smiling, the width of the mouth increases by as much as 30%6; therefore, an excessive transverse lip extension in smiling would theoretically produce a wider buccal corridor. Further research is needed to confirm this hypothesis.
5. Smile Symmetry
Smile symmetry, the relative positioning of the corners of the mouth in the vertical plane,1,45 can be assessed by the parallelism of the commissural and pupillary lines. Although the commissures move up and laterally in smiling, studies have shown a difference in the amount and direction of movement between the right and left sides.29,46,47 A large differential elevation of the upper lip in an asymmetrical smile may be due to a deficiency of muscular tonus on one side of the face1 (Fig. 12). Myofunctional exercises have been recommended to help overcome this deficiency and restore smile symmetry.1,48 An oblique commissural line in an asymmetrical smile can give the illusion of a transverse cant of the maxilla or a skeletal asymmetry.12
6. Frontal Occlusal Plane
The frontal occlusal plane is represented by a line running from the tip of the right canine to the tip of the left canine. A transverse cant can be caused by differential eruption of the maxillary anterior teeth or a skeletal asymmetry of the mandible12 (Fig. 13). This relationship of the maxilla to the smile cannot be seen on intraoral images or study casts, and smile photographs can also be misleading. Therefore, clinical examination and digital video documentation are essential in making a differential diagnosis between smile asymmetry, a canted occlusal plane, and facial asymmetry.23,49-52 Having the patient bite on a tongue blade or a mouth mirror in the premolar area during the clinical examination is a good way to recognize an asymmetrical cant of the maxillary frontal occlusal plane.
7. Dental Components
The first six components of the smile considered the relationship between the teeth and lips and the way the lips and soft tissue frame the smile. A pleasant smile also depends on the quality and beauty of the dental elements it contains and their harmonious integration. Dental components of the smile include the size, shape, color, alignment, and crown angulation (tip) of the teeth; the midline; and arch symmetry.53
The dental midline is an important focal point in an esthetic smile.40 A practical and reliable method of locating the facial midline, which normally coincides with the dental midline, is to use two anatomical landmarks: nasion and the base of the philtrum, known as the "cupid's bow", in the center of the upper lip. A line drawn between these two landmarks not only locates the facial midline, but also determines its direction.54 The parallelism between the maxillary central incisor midline and the facial midline is more important than the coincidence between the dental and facial midlines. In fact, in one study, a 4mm maxillary midline deviation was not detected by dentists or lay persons, whereas a 2mm deviation in incisor angulation was rated as noticeably unattractive8 (Fig. 14). A mild midline discrepancy is acceptable as long as the interproximal contact area (connector space) between the maxillary central incisors is vertical.
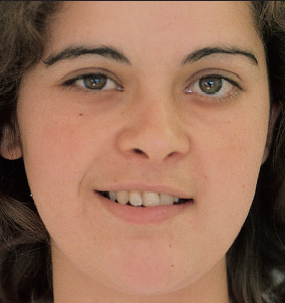
Fig. 12 Patient with asymmetrical smile due to deficiency of muscle tonus on one side of face.

Fig. 13 Patient with canted occlusal frontal plane and unilateral posterior gingival smile.

Fig. 14 Patient with unattractive maxillary central incisor midline angulation, referred to as canted midline.
Arch symmetry is also important in achieving a balanced smile, which is why cases with peg-shaped or missing lateral incisors are particularly challenging (Fig. 15). Other factors that can disturb the continuity of the dental composition include midline diastemas and a lack of interproximal contacts.3

Fig. 15 A. Patient with arch asymmetry due to peg-shaped lateral incisor and missing lateral incisor. B. Symmetrical arch after extraction of peg lateral and orthodontic space closure.
8. Gingival Components
The gingival components of the smile are the color, contour, texture, and height of the gingivae. Inflammation, blunted papillae, open gingival embrasures, and uneven gingival margins detract from the esthetic quality of the smile54 (Fig. 16). The space created by a missing papilla above the central incisor contact point, referred to as a "black triangle", may be caused by root divergence, triangular teeth, or advanced periodontal disease. Orthodontic root paralleling and flattening of the mesial surfaces of the central incisors, followed by space closure, will lengthen this contact area and move it apically toward the papilla.34
The gingival margins of the central incisors are normally at the same level or slightly lower than those of the canines, while the gingival margins of the lateral incisors are lower than those of the central incisors. Gingival margin discrepancies may be caused by attrition of the incisal edges, ankylosis due to trauma in a growing patient, severe crowding, or delayed migration of the gingival tissue55 (Fig. 17). The gingival margins can be leveled by orthodontic intrusion or extrusion or by periodontal surgery, depending on the lip line, the crown heights, and the gingival levels of the adjacent teeth.34

Fig. 16 Patient with full smile displaying uneven gingival heights.

Fig. 17 A. Patient with uneven gingival heights due to crowding and ankylosis. B. After orthodontic space closure, replacing ankylosed maxillary right central incisor with lateral incisor. C. Lateral incisor after composite build-up.
Conclusion
In summary, an optimal smile is characterized by an upper lip that reaches the gingival margins, with an upward or straight curvature between the philtrum and commissures; an upper incisal line coincident with the border of the lower lip; minimal or no lateral negative space; a commissural line and occlusal frontal plane parallel to the pupillary line; and harmoniously integrated dental and gingival components.
These concepts of smile esthetics are not new, but are too often overlooked in orthodontic treatment planning. The eight components of the smile should be considered not as rigid boundaries, but as artistic guidelines to help orthodontists treat individual patients who are today, more than ever, highly aware of smile esthetics.
REFERENCES
- 1. Hulsey, C.M.: An esthetic evaluation of lip-teeth relationships present in the smile, Am. J. Orthod. 57:132-144, 1970.
- 2. Mackley, R.J.: An evaluation of smiles before and after orthodontic treatment, Angle Orthod. 63:183-190, 1993.
- 3. Tjan, A.H.L.; Miller, G.D; and The, J.G.: Some esthetic factors in a smile, J. Prosth. Dent. 51:24-28, 1984.
- 4. Dong, J.K.; Jin, T.H.; Cho, H.W.; and Oh, S.C.: The esthetics of the smile: A review of some recent studies, Int. J. Prosthod. 12:9-19, 1999.
- 5. Peck, S.; Peck, L.; and Kataja, M.: Some vertical lineaments of lip position, Am. J. Orthod. 101:519-524, 1992.
- 6. Rigsbee, O.H. 3rd; Sperry, T.P.; and BeGole, E.A.: The influence of facial animation on smile characteristics, Int. J. Adult Orthod. Orthog. Surg. 3:233-239, 1988.
- 7. Peck, S.; Peck, L.; and Kataja, M.: The gingival smile line, Angle Orthod. 62:91-100, 1992.
- 8. Kokich, V.O.; Kiyak, H.A.; and Shapiro, P.A.: Comparing the perception of dentists and lay people to altered dental esthetics, J. Esth. Dent. 11:311-324, 1999.
- 9. Vig, R.G. and Brundo, G.C.: The kinetics of anterior tooth display, J. Prosth. Dent. 39:502-504, 1978.
- 10. Kim, H.S.; Jin, T.H.; and Dong, J.K.: A study on the relation between lip and teeth at smile in old aged Korean, J. Kor. Dent. Assoc. 31:533-541, 1993.
- 11. Choi, T.R.; Jin, T.H.; and Dong, J.K.: A study on the exposure of maxillary and mandibular central incisor in smiling and physiologic rest position, J. Wonkwang Dent. Res. Inst. 5:371-379, 1995.
- 12. Sarver, D.M. and Ackerman, M.B.: Dynamic smile visualization and quantification: Part 2. Smile analysis and treatment strategies, Am. J. Orthod. 124:116-127, 2003.
- 13. Peck, S. and Peck, L.: Selected aspects of the art and science of facial esthetics, Semin. Orthod. 1:105-126, 1995.
- 14. Ekman, P.: Darwin and Facial Expression: A Century of Research in Review, Academic Press, New York, 1973.
- 15. Ackerman, J.L.; Ackerman, M.B.; Brensinger, C.M.; and Landis, J.R.: A morphometric analysis of the posed smile, Clin. Orthod. Res. 1:2-11, 1998.
- 16. Sarver, D.M.: The importance of incisor positioning in the esthetic smile: The smile arc, Am. J. Orthod. 120:98-111, 2001.
- 17. Kim, H.S.; Kim, I.P.; Oh, S.C.; and Dong, J.K.: The effect of personality on the smile, J. Wonkwang Dent. Res. Inst. 5:299-314, 1995.
- 18. Burstone, C.J.: Lip posture and its significance in treatment planning, Am. J. Orthod. 53:262-284, 1967.
- 19. Farkas, L.G.; Katic, M.J.; Hreczko, T.A.; Deutsch, C.; and Munro, I.R.: Anthropometric proportions in the upper lip-lower lip-chin area of the lower face in young white adults, Am. J. Orthod. 86:52-60, 1984.
- 20. Powell, N. and Humphreys, B.: Proportions of the Esthetic Face, Thieme, New York, 1984.
- 21. Wolford, L.M.: Discussion: Lip-nasal aesthetics following LeFort osteotomy, Plast. Reconstr. Surg. 81:180-182, 1988.
- 22. Arnett, G.W. and Bergman, R.T.: Facial keys to orthodontic diagnosis and treatment planning, Part II, Am. J. Orthod. 103:395-411, 1993.
- 23. Ackerman, M.B. and Ackerman, J.L.: Smile analysis and design in the digital era, J. Clin. Orthod. 36:221-236, 2002.
- 24. Kamer, F.M.: Smile surgery, Laryngoscope 89:1528-1532, 1979.
- 25. Litton, C. and Fournier, P.: Simple surgical correction of the gummy smile, Plast. Reconstr. Surg. 63:372-373, 1979.
- 26. Kostianovsky, A.: The unpleasant smile, Aesth. Plast. Surg. 1:161, 1977.
- 27. Vig, P.S. and Cohen, A.M.: Vertical growth of the lips: A serial cephalometric study, Am. J. Orthod. 75:405-415, 1979.
- 28. Dickens, S.; Sarver, D.M.; and Proffit,W.R.: Changes in frontal soft tissue dimensions of the lower face by age and gender, World J. Orthod. 3:313-320, 2002.
- 29. Rubin, L.R.: The anatomy of a smile: Its importance in the treatment of facial paralysis, Plast. Reconstr. Surg. 53:384-387, 1974.
- 30. Zachrisson, B.U.: Esthetic factors involved in anterior tooth display and the smile: Vertical dimension, J. Clin. Orthod. 32:432-445, 1998.
- 31. Sarver, D.M. and Weissman, S.M.: Long-term soft tissue response to LeFort I maxillary superior repositioning, Angle Orthod. 61:267-276, 1991.
- 32. Gillen, R.J.; Schwartz, R.S.; Hilton, T.J.; and Evans, D.B.: An analysis of selected normative tooth proportions, Int. J. Prosthod. 7:410-417, 1994.
- 33. Garber, D.A. and Salama, M.A.: The aesthetic smile: Diagnosis and treatment, Periodontol. 2000 11:18-28, 1996.
- 34. Kokich, V.G.: Esthetics: The orthodontic-periodontic restorative connection, Semin. Orthod. 2:21-30, 1996.
- 35. Sarver, D.M. and Ackerman, M.B.: Dynamic smile visualization and quantification: Part 1. Evolution of the concept and dynamic records for smile capture, Am. J. Orthod. 124:4-12, 2003.
- 36. Frush, J.P. and Fisher, R.D.: The dynesthetic interpretation of the dentogenic concept, J. Prosth. Dent. 8:558-581, 1958.
- 37. Matthews, T.G.: The anatomy of a smile, J. Prosth. Dent. 39:128-134, 1978.
- 38. Miller, C.J.: The smile line as a guide to anterior esthetics, Dent. Clin. N. Am. 33:157-164, 1989.
- 39. Mabrito, C.: Elements of a beautiful smile, N.M. Dent. J. 47:20-21, 1996.
- 40. Lombardi, R.E.: The principles of visual perception and their clinical application to denture esthetics, J. Prosth. Dent. 29:358-382, 1973.
- 41. Philips, E.: The anatomy of a smile, Oral Health 86:7-13, 1996.
- 42. Philips, E.: The classification of smile patterns, J. Can. Dent. Assoc. 65:252-254, 1999.
- 43. Yoon, M.E.; Jin, T.H.; and Dong, J.K.: A study on the smile in Korean youth, J. Kor. Acad. Prosthod. 30:259-270, 1992.
- 44. Johnson, D.K. and Smith, R.J.: Smile esthetics after orthodontic treatment with and without extraction of four first premolars, Am. J. Orthod. 108:162-167, 1995.
- 45. Janzen, E.K.: A balanced smile: A most important treatment objective, Am. J. Orthod. 72:359-372, 1977.
- 46. Paletz, J.L.; Manktelow, R.T.; and Chaban, R.: The shape of a normal smile: Implications for facial paralysis reconstruction, Plast. Reconstr. Surg. 93:784-789, 1994.
- 47. Benson, K.J. and Laskin, D.M.: Upper lip asymmetry in adults during smiling, J. Oral Maxillofac. Surg. 59:396-398, 2001.
- 48. Gibson, R.M.: Smiling and facial exercise, Dent. Clin. N. Am. 33:139-144, 1989.
- 49. Sarver, D.M. and Ackerman, J.L.: Orthodontics about face: The reemergence of the esthetic paradigm, Am. J. Orthod. 117:575-576, 2000.
- 50. Ackerman, J.L.; Proffit,W.R.; and Sarver, D.M.: The emerging soft tissue paradigm in orthodontic diagnosis and treatment planning, Clin. Orthod. Res. 2:49-52, 1999.
- 51. Ackerman, M.B.: Digital video as a clinical tool in orthodontics: Dynamic smile design in diagnosis and treatment planning, in 29th Annual Moyers Symposium, vol. 40, University of Michigan, Ann Arbor, 2003.
- 52. Lackey, A.D.: Examining your smile, Dent. Clin. N. Am. 33:133-137, 1989.
- 53. Moskowitz, M.E. and Nayyar, A.: Determinants of dental esthetics: A rationale for smile analysis and treatment, Compend. Cont. Ed. Dent. 16:1164-1166, 1995.
- 54. Morley, J. and Eubank, J.: Macroesthetic elements of smile design, J. Am. Dent. Assoc. 132:39-45, 2001.
- 55. Sabri, R.: Treatment of a Class I crowded malocclusion with an ankylosed maxillary central incisor, Am. J. Orthod. 122:557-565, 2002.
-
 DR. SABRI
DR. SABRI
Dr. Sabri is a Clinical Associate, Division of Orthodontics and Dentofacial Orthopedics, American University of Beirut Medical Center, and in the private practice of orthodontics in Beirut, Lebanon. Contact him at P.O. Box 16-6006, Beirut, Lebanon; e-mail: roysabri@dm.net.lb.