Esthetic Factors Involved in Anterior Tooth Display and the Smile: Vertical Dimension
Several mistakes are commonly made during orthodontic treatment of both routine and difficult cases, especially when it comes to the patient's display of the dentition in rest position, normal conversation, and full smile. The purpose of this article is to discuss some new concepts of the desirable characteristics of tooth display during normal conversation and smiling, and to provide guidance on how to analyze esthetic factors by viewing the patient from the front. It will emphasize the need for age-related goals in orthodontics, as well as the benefits of individual variation within different facial types. A subsequent article will deal with the transverse dimension.
Evaluating Esthetics from the Front
Esthetics, which is derived from the Greek word for "perception", deals with beauty and the beautiful. It has two dimensions: objective and subjective.1 Objective (admirable) beauty is based on consideration of the object itself, implying that the object possesses properties that make it unmistakably praiseworthy. Subjective (enjoyable) beauty is a quality that is value-laden, relative to the tastes of the person contemplating it.1,2 Careful technique in dentistry should lend objective esthetics (admirable beauty) to the entire orofacial complex, involving unity, form, structure, balance, color, function, and display of the dentition.1 On the other hand, the creation of subjective beauty may enhance cosmetic value.1,2
Similar articles from the archive:
In an extensive discussion of the principles of visual perception and their clinical applications to denture esthetics, Lombardi pointed out that detailed esthetic judgments can only be made by viewing patients from the front, in conversation, facial expressions, and smiling3 (Fig. 1A). The dentist's view from above and behind the patient is skewed, differing substantially from the "true" perception of the patient in a mirror or by other people during normal social activities (Fig. 1B,C).
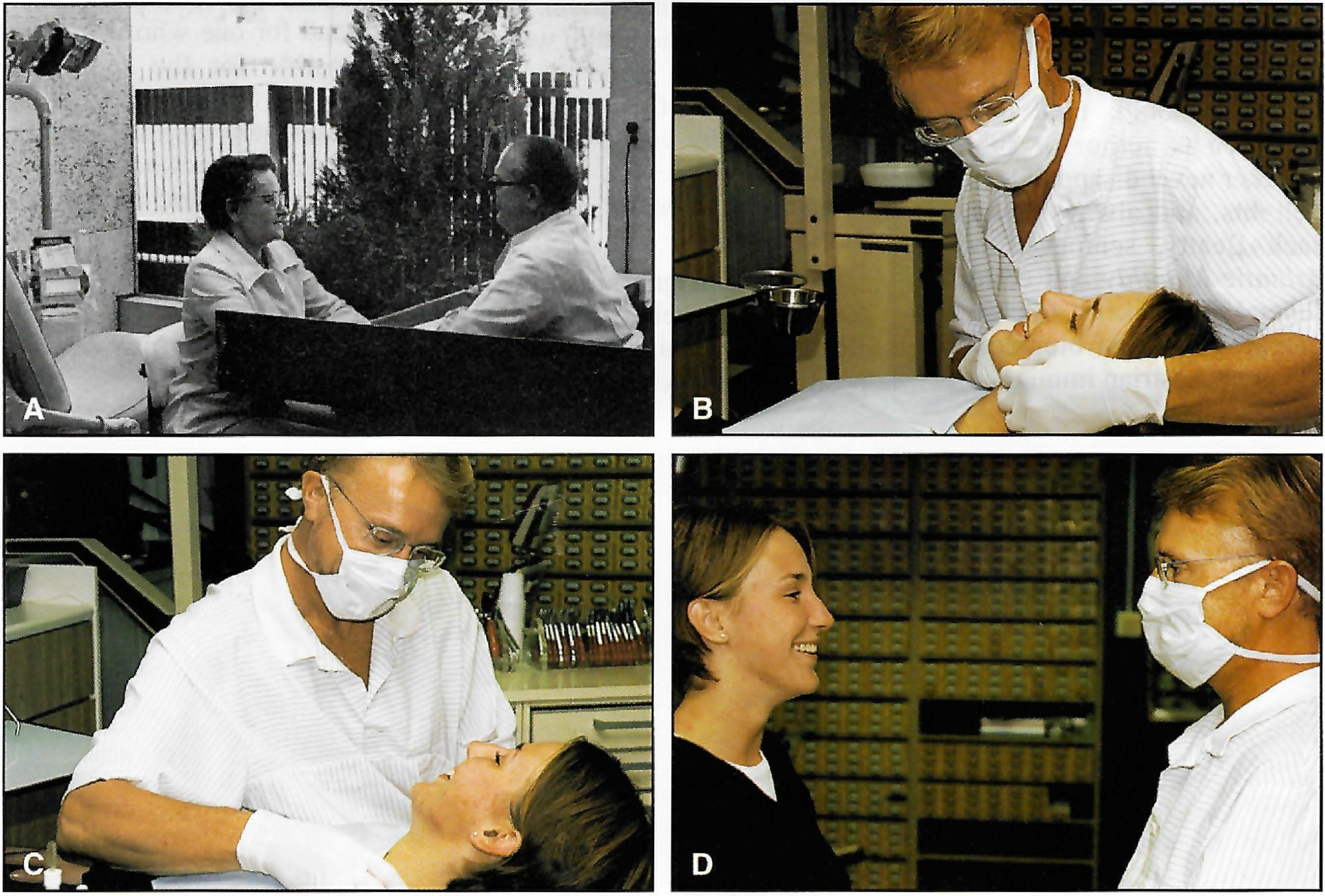
Fig. 1 A. Nondental situation cited by Lombardi3: viewing patient from front for esthetic evaluation before making denture. B,C. Positions unsuitable for evaluating esthetics. D. Viewing patient from front to obtain realistic impression of esthetic features.
For example, it is impossible to gain adequate information on such details as dentofacial midline alignment and right-left symmetry of canine and premolar torque unless the patient is observed directly from the front. Therefore, it is fundamentally important that esthetic factors such as the following be analyzed by sitting or standing in front of the patient (Fig. 1D):
- Crown lengths of maxillary and mandibular incisors.
- Incisal edge contours (before and after recontouring by grinding).
- Axial inclinations of all maxillary and mandibular incisors.
- Midlines (upper, lower, labial, and facial).
- Crown torque (canines, premolars, and molars on both sides).
- Smile line (rest position and full smile).
- Right-left symmetry of crown shapes and sizes and gingival margin levels.
After carefully studying these features, the orthodontist can make the required finishing archwire bends and perform any other esthetic procedures needed.
Smile Type
In visual evaluation of the full smiles of 454 dental and dental hygiene students, age 20 to 30, from the Los Angeles area, Tjan and colleagues found that 11% had a high smile, revealing the complete cervicoincisal length of the maxillary incisors and a contiguous band of gingiva.4 An average smile, revealing 75-100% of the maxillary incisors, was found in 69% of this population, and a low smile, displaying less than 75% of the maxillary incisors, in 20%.
Lip coverage of the maxillary incisors tends to increase with age, and therefore the percentage of high smiles may be greater among younger age groups5,6 and smaller among older adults.7 There is also a sex difference in smile type: low smile lines are a predominantly male characteristic, and high smile lines predominantly female.4
Maxillary Incisal Curve and Lower Lip
The Tjan survey also revealed that 85% of the students had a maxillary incisal curve parallel to the inner contour of the lower lip, 14% showed a straight rather than a curved line, and 1% had a reverse smile line4 (Fig. 2).
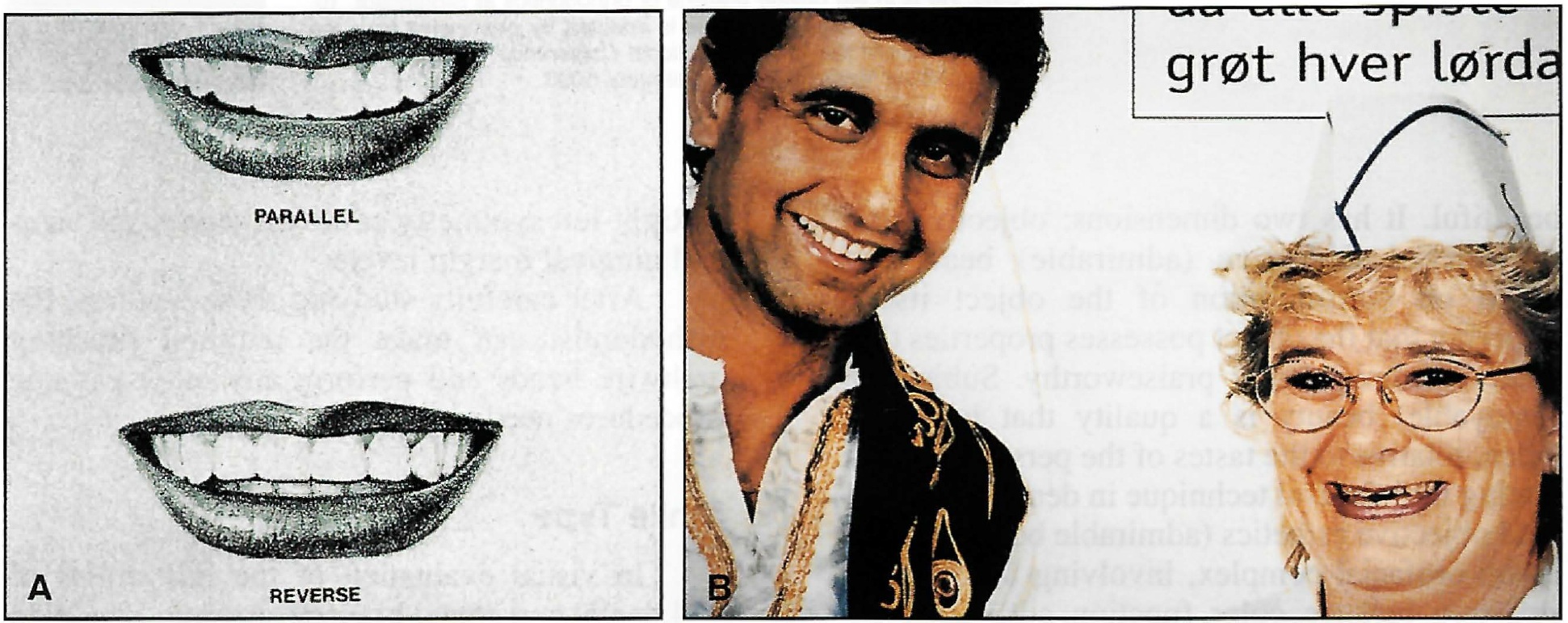
Fig. 2 A. Parallel and reverse curves of maxillary incisors relative to lower lip (reprinted by permission4). B. Norwegian advertisement demonstrating attractive and less attractive smiles. Male model has maxillary incisor curve parallel to lower lip and displays only maxillary teeth. Female model has reverse incisor curve and exposes less of maxillary teeth and more of mandibular teeth.
Since parallelism is the "normal" finding in untreated persons, it would seem to be an optimal goal for objective beauty in all kinds of esthetic oral rehabilitations,6,7 including orthodontic (Fig. 3A,B) and orthodontic-prosthetic treatment8 (Fig. 3C,D).

Fig. 3 A,B. Improvement in parallelism between maxillary incisor curve and lower lip contour with orthodontic treatment of adult female. C,D. Similar improvement in another adult female with Class 11, division 2 malocclusion and abraded incisors. Orthodontic treatment was supplemented with four porcelain laminate veneers (courtesy of Dr. S. Toreskog, Sweden).
A straight or reverse smile line may contribute to a less attractive facial appearance.3,8 In addition, the reverse curve is often associated with marked abrasive wear of the maxillary incisors (Figs. 2B and 4A).

Fig. 4 Importance of vertical dimension in beautiful smile. A. Adult female with uncompensated attrition. B. After restorative treatment by Dr. M.R. Mack of Fort Lauderdale, FL. Note physiologic positioning with improved lip form, smile, and facial proportions (reprinted by permission8). C. Female patient with little maxillary incisor display. D. Dramatic esthetic improvement after surgical inferior repositioning of maxilla and treatment by Dr. P.K. Turley of Los Angeles (reprinted by permission13).
Vertical Position of the Incisors
Normal Age Changes
Peck and colleagues recently measured maxillary incisor exposure, at rest position and full smile, in a sample of 15-year-old males and females5 (Table 1). Vig and Brundo reported a gradual decrease in maxillary incisor exposure for each increase in age group from under 30 to over 607 (Table 2).

Mandibular incisor display showed a corresponding increase. In fact, the amount of mandibular incisor display after age 60 was approximately equal to the amount of maxillary incisor display before age 30 (see Fig. 6).
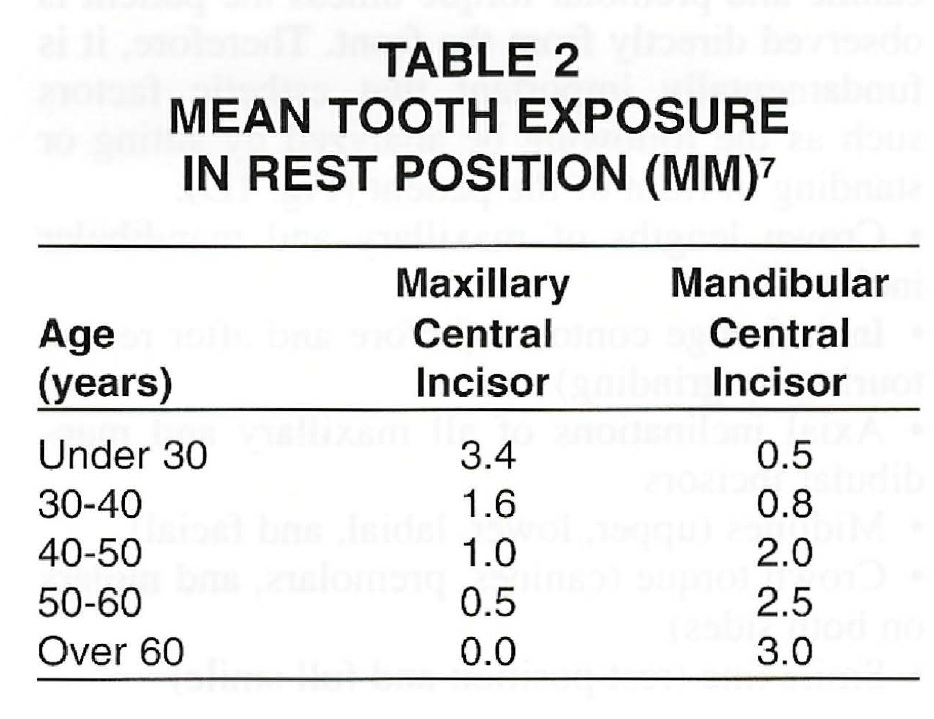
This progressive change is caused by the effects of gravity on upper and lower lip positions. The sagging of the perioral soft tissue is partly due to the natural flattening, stretching, and decreasing elasticity of the skin.10 Display of the maxillary incisors during normal conversation thus indicates youth, while display of only the mandibular incisors indicates age. The importance of the vertical dimension in tooth display has been demonstrated in prosthetic dentistry8,9 and in orthognathic surgery involving inferior maxillary repositioning (Fig. 4).
Sexual Dimorphism
Several studies have found significant sex differences in anterior tooth display.5-7 Generally, females have significantly more maxillary and less mandibular tooth exposure than males at all ages (Table 1). In an adult sample, Vig and Brundo found almost twice as much maxillary anterior tooth display with the lips at rest in women (3.4mm) as in men (1.9mm).7The men displayed much more of the mandibular incisors (1.2mm to .5mm). As noted above, a high smile type is twice as prevalent in women.5,6 The reason for this dimorphism remains largely unexplained.
Standardized Extraoral Photography
A standardized procedure for recording tooth display in rest position and full smile, in conjunction with the standard full-face, three-quarter, and profile views, will help the clinician avoid undesirable treatment effects on the smiles of older patients. Estimates of method errors using double determinations show mean differences and standard deviations consistent with expectations.5,6 Potential errors are immense, as dramatized by Burstone's data on the interlabial gap in adolescents: in centric occlusion the lip gap was 1.8mm (S.D. 1.2mm), but in rest position the gap was 3.7mm (S.D. 1.6mm).15
Each patient should be coached and asked to achieve the same lip position at least twice in succession before a photograph is taken (Table 3).5,6 A short video sequence will be helpful in demonstrating rest position, normal conversation, and smiling. Most people are able to attain reasonably reproducible lip positions.
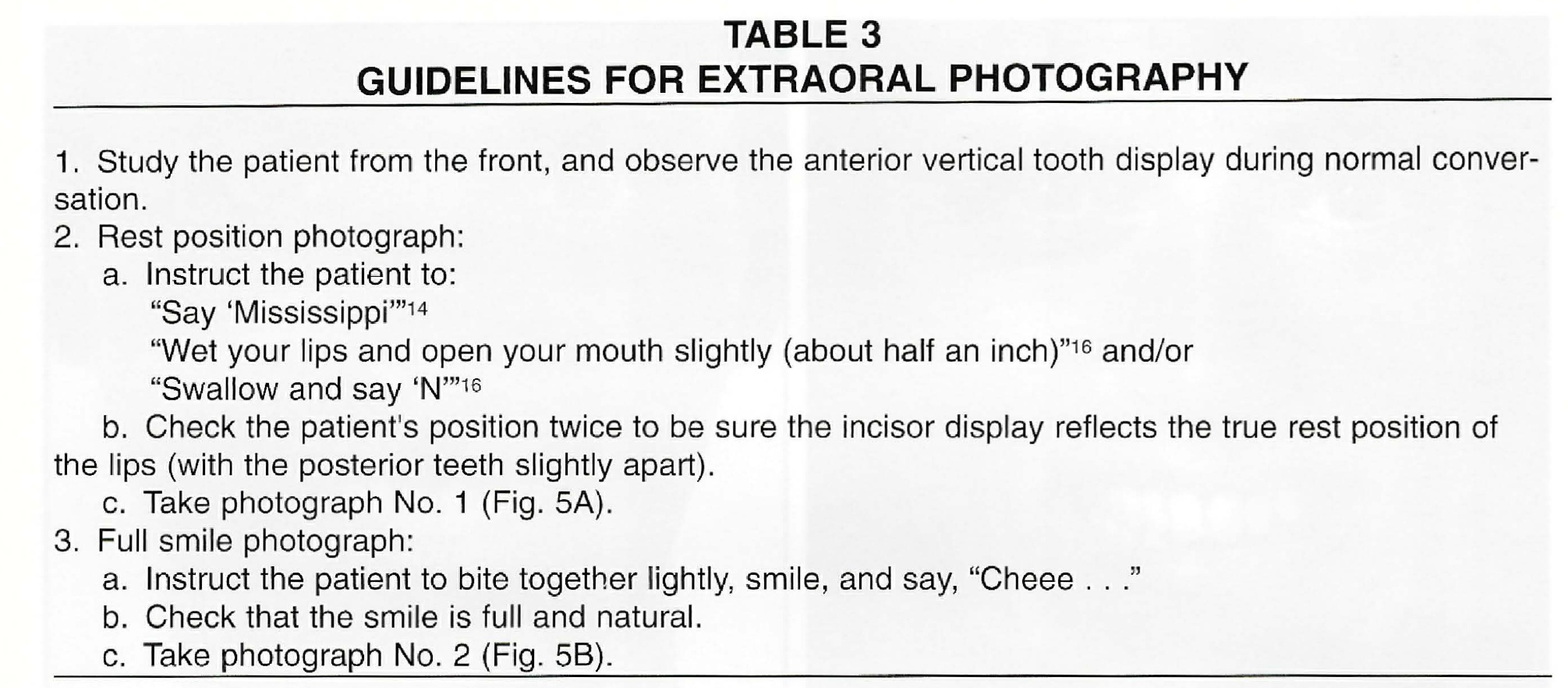
In rest position the teeth should be slightly apart, and the perioral soft tissue and mandibular posture must both be unstrained. At full smile the teeth should be lightly closed (Fig. 5).

Fig. 5 Extraoral photographs recommended for routine evaluation of anterior tooth display and smile. A. Rest position (teeth slightly apart). B. Full smile (teeth lightly closed).
The optimal vertical reference position for the maxillary incisal edge in orthodontic treatment planning is with relaxed lips (Fig. 6). Useful information can be obtained when the patient is observed in normal conversation. The full smile will not provide the same information, partly because of high individual variability in upper lip movement from rest position to full smile. This movement ranges from 2mm to 12mm, with an average of 7-8mm, and is not correlated with age.16
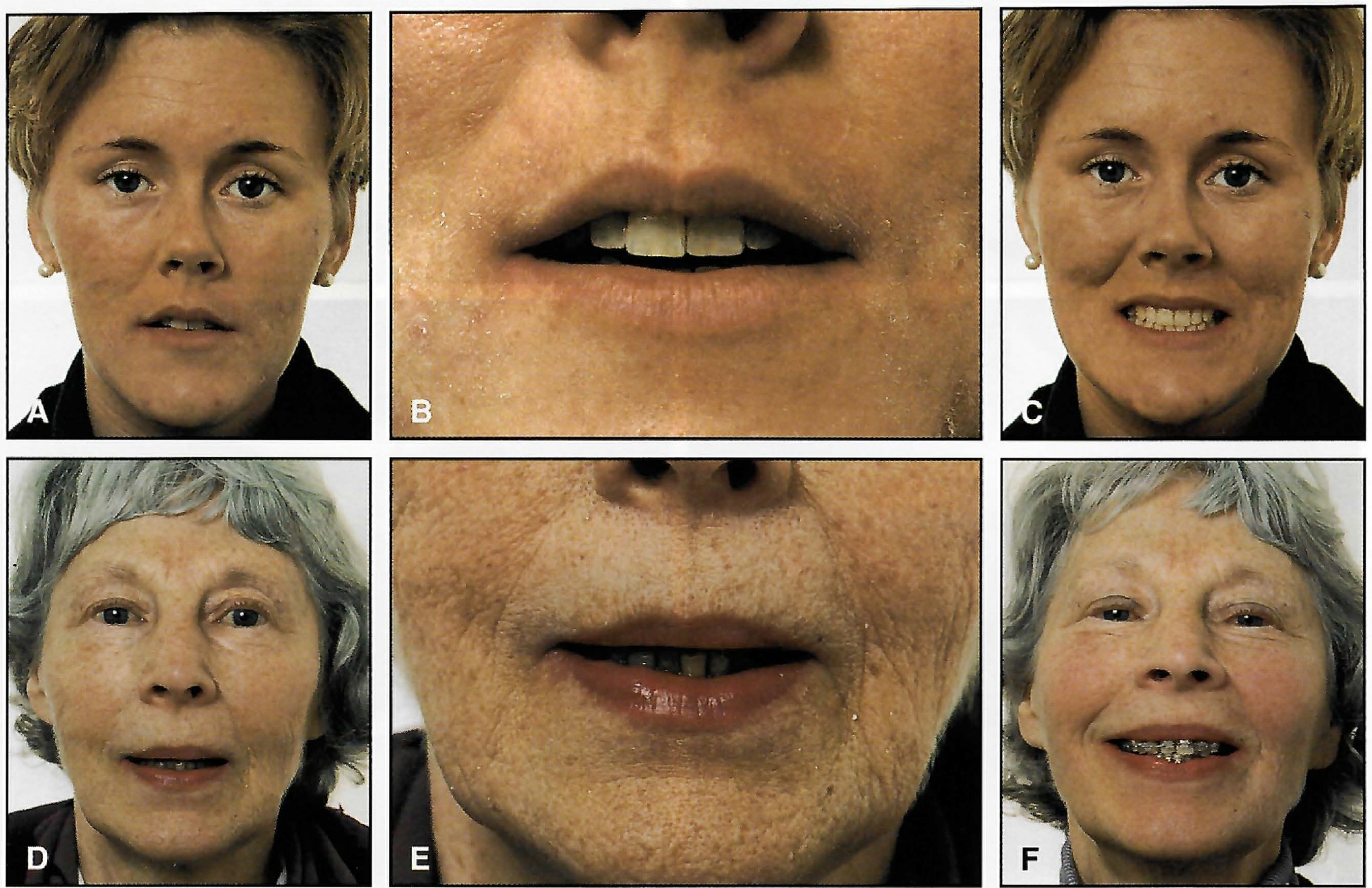
Fig. 6 Age changes in vertical tooth display during normal conversation, demonstrated by female patients ages 25 and 65. In rest position (A-8, D-E), young woman shows only maxillary incisors, whereas older woman shows only mandibular incisors. In maximum smile (C,F), vertical tooth display is similar.
The smile is apparently formed in two stages, the first raising the lip to the nasolabial fold, and the second involving further superior raising of the lip and the fold by three muscle groups.5 Nearly everyone, irrespective of age, will display the maxillary incisors nicely on maximum smiling, even if only the mandibular incisors are visible during conversation (Fig. 6).
Clinical Implications for Low and Average Smile Types
The correction of deep overbite can be accomplished by various combinations of intrusion of the anterior teeth and extrusion of the posterior teeth.17 From the esthetic perspective, a serious mistake commonly made in orthodontic practice is "overintrusion" of the maxillary incisors (Figs. 7 and 8). In most deep overbite cases, this will tend to hide the maxillary anterior teeth behind the upper lip in normal conversation. Such a mistake can go undetected by the orthodontist unless the patient's tooth display and smile are analyzed from the front. With increasing age and concomitant drooping of the upper lip,7 an unesthetic anterior tooth display may worsen.
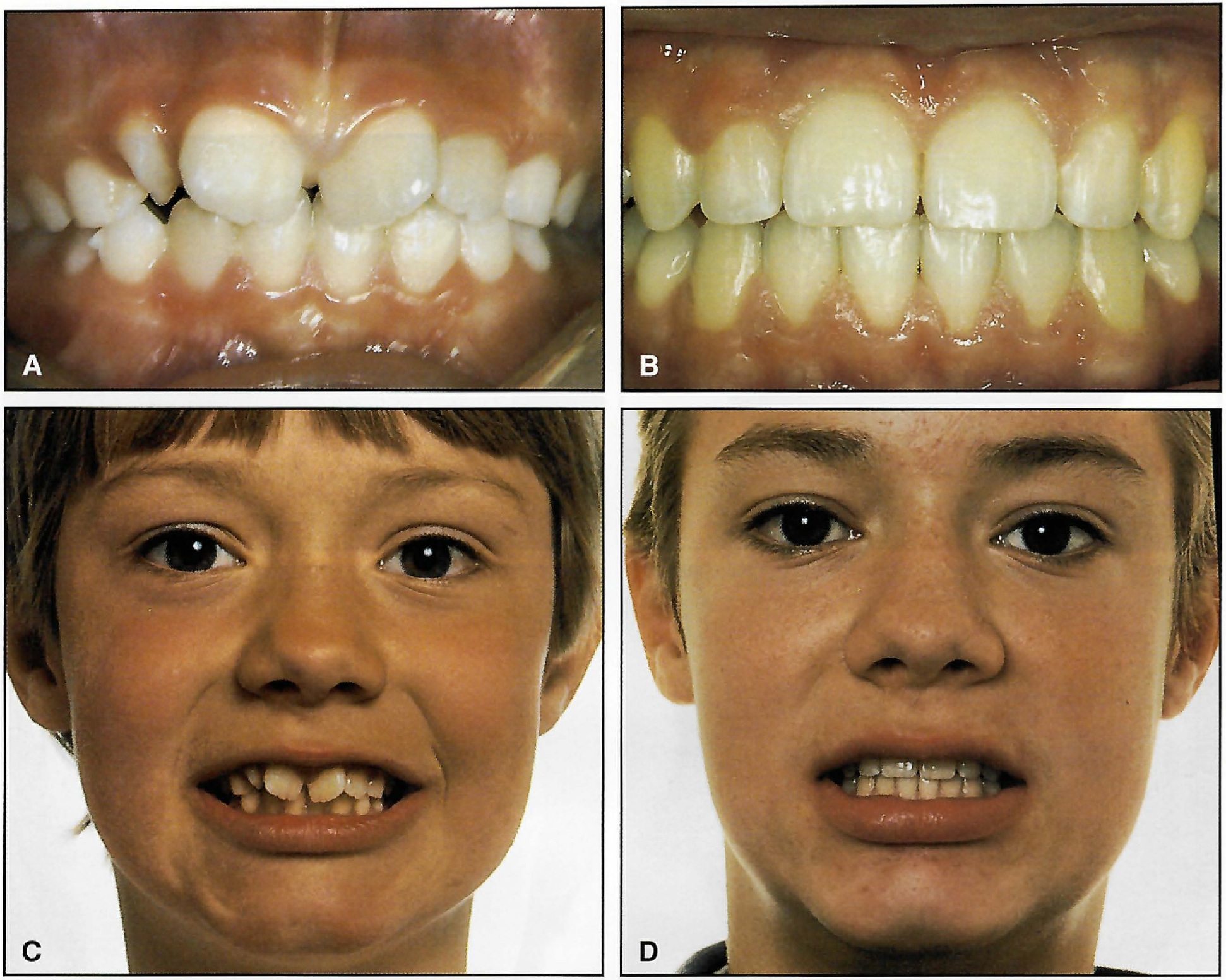
Fig. 7 Young male patient with severe anterior crowding before (A,C) and after (B,D) orthodontic treatment. Note undesirable esthetic result after overintrusion of maxillary incisors, and straight incisal curvature in relation to lower lip.
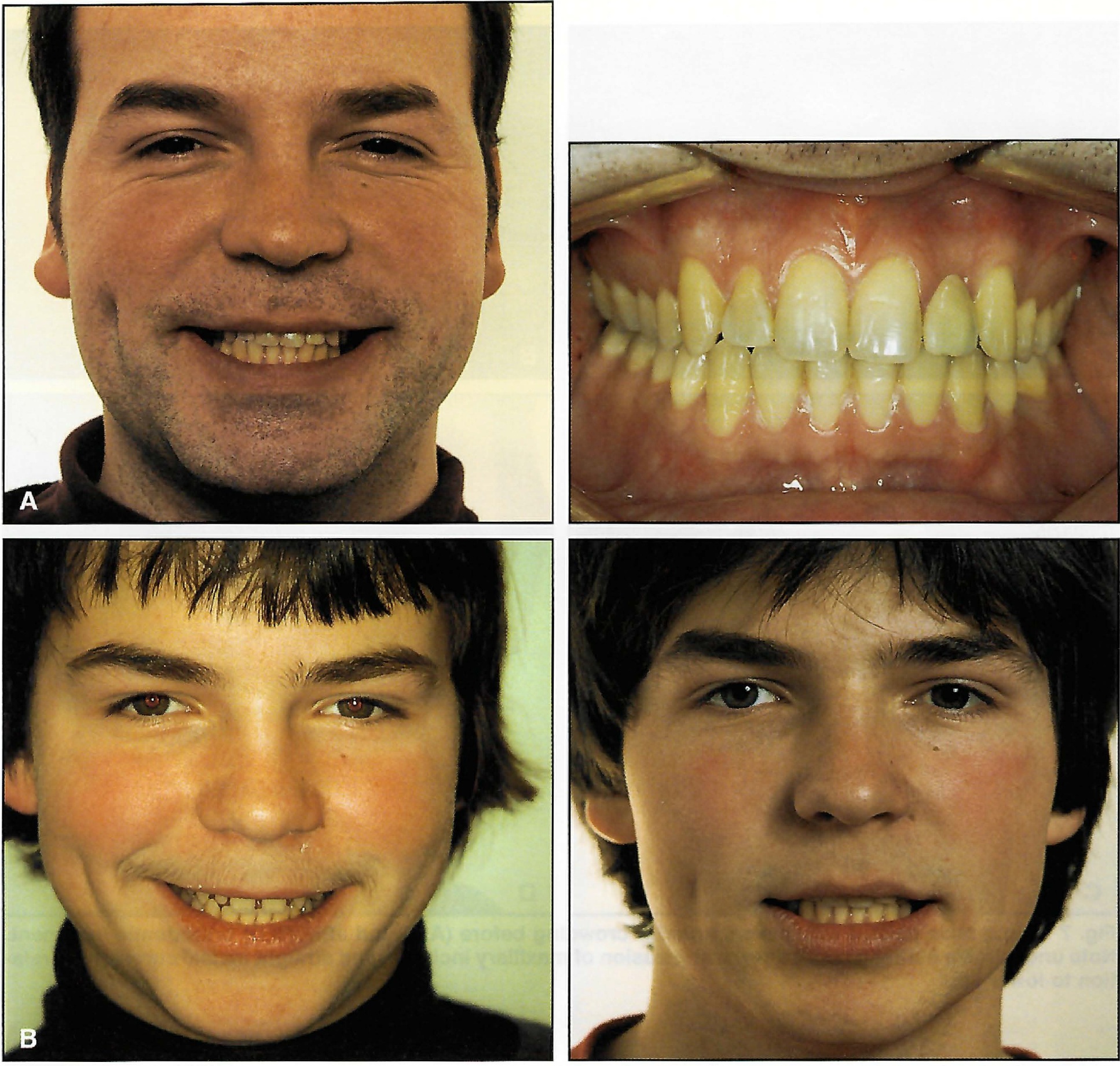
Fig. 8 A. Esthetically undesirable long-term result in 30-year-old male 15 years after orthodontic treatment. Too much of mandibular incisors and too little of maxillary incisors are displayed. B. Pre- and post-treatment records from 1981 and 1983, respectively, show maxillary incisors were intruded.
The maxillary incisors should be moved in the vertical direction that improves their relationship to the resting lip position, and the tooth-to-lip position should be monitored constantly throughout treatment. In some deep overbite cases, this may actually mean extrusion rather than intrusion of the maxillary incisors.18,19 In most orthodontic patients, except those with marked "gummy" smiles, active intrusion of the maxillary incisors is undesirable.
The best treatment strategy in the majority of deep overbite cases is to actively intrude the mandibular incisors, using double tubes on the mandibular first molars and continuous or segmented base arches17 or utility arches20 (Fig. 9). In a young patient with a short lower face, extrusion of the posterior teeth might correct a deep overbite, but the stability of such correction is uncertain, especially with less-than-adequate growth during and after treatment.17
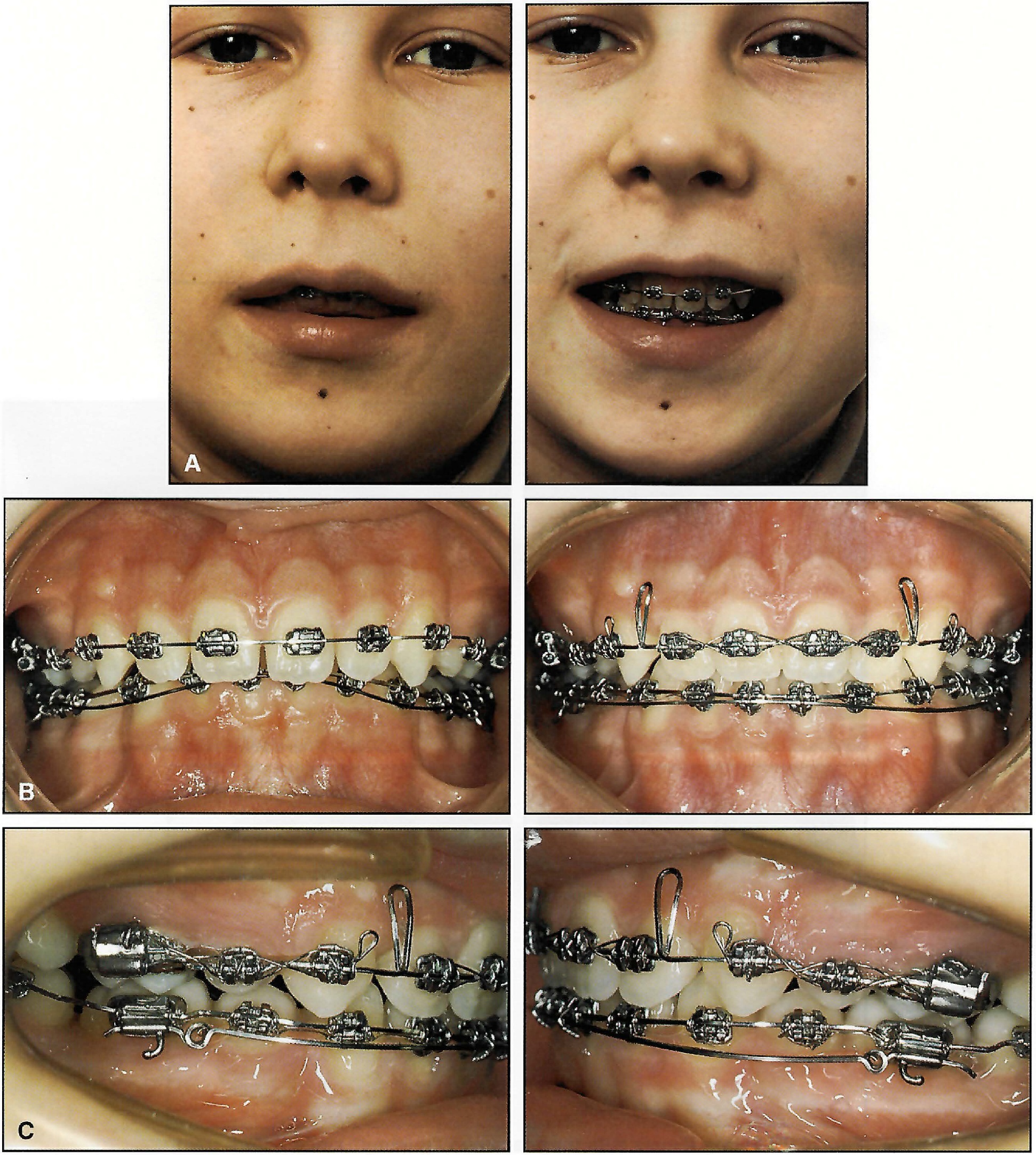
Fig. 9 Young male patient with deep overbite. A. Rest position and smile photographs indicate that maxillary incisors should not be intruded. B. Mandibular incisor intrusion. C. Continuous base arch from double tubes on mandibular first molars.
Another common mistake in orthodontic finishing is to create a straight (or even reverse) maxillary incisal curve relative to the smile line (Fig. 7B,D). Parallelism of the incisal curve and the inner contour of the lower lip in smiling may seem difficult to produce. In practice, however, this appearance can readily be achieved if the maxillary central incisors are symmetrically positioned .5-1mm longer than the lateral incisors21 (Figs. 3B,C and 4B,D). If the lower lip shows a marked curvature in smiling, the distoincisal edges of the maxillary central incisors can be ground slightly without affecting functional occlusion12 (Fig. 3B).
It is particularly undesirable to combine maxillary incisor overintrusion with a straight arrangement of these teeth. Figure 7 shows a young patient who received what Lombardi calls a "denture mouth".3
Clinical Implications for High Smile Types
The "gummy" smile, which can be defined as 2mm or more of maxillary gingival exposure in full smiling (Figs. 10 and 11), has provoked considerable interest and concern among clinicians.5,6,18,19,23,26 Its biological mechanism appears to involve the combined effects of anterior vertical excess, an increased muscular capacity to raise the upper lip in smiling, and associated factors such as excessive interlabial gap at rest and excessive overjet and overbite.9 Surprisingly, upper lip length, clinical crown height of the incisors, and mandibular and palatal plane angles do not appear to relate to the gingival smile line.5 The sexual dimorphism in smile types indicates that females are twice as likely as males to have gummy smiles.4-6,27
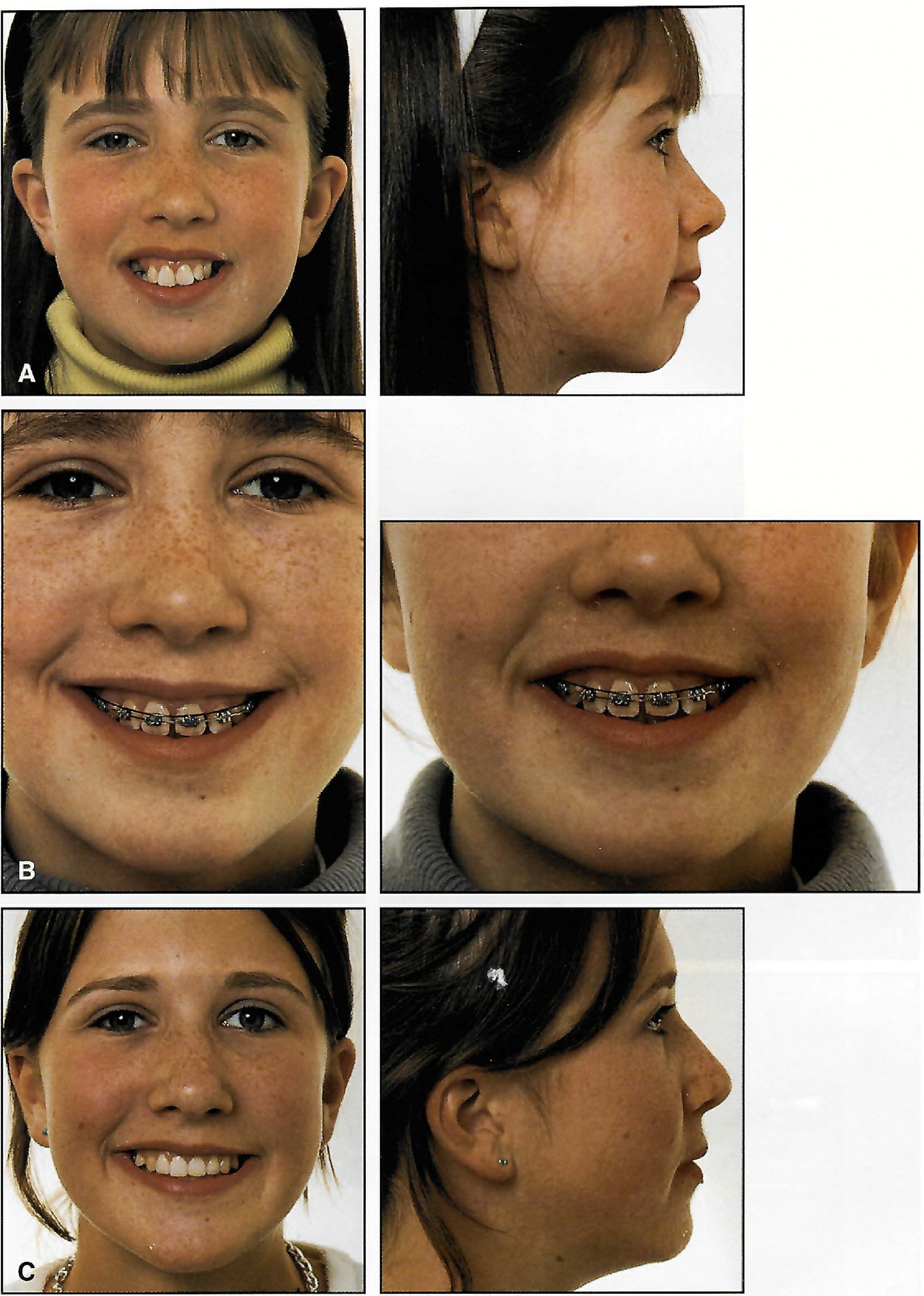
Fig. 10 A. Young female with long face and "gummy" smile before treatment. B. After extraction of four premolars, maxillary incisors actively intruded with base arch, which was maintained during most of treatment. C. Esthetic improvement in smile and facial appearance.

Fig. 11 A. Young female with long face and pronounced "gummy" smile before treatment. B. High smile line remaining after active maxillary incisor intrusion. C. Labial gingivectomies over six anterior teeth, using "adult" excisions, with frenum relocated and sutured. D. Healing of gingiva after one week and after four months. E. Acceptable tooth display and smile. Further improvement can be expected with normal aging.
A different treatment philosophy is needed for patients with high lip lines than for those with average or low smile types. Active maxillary incisor intrusion should be the goal in this category of patients. Treatment alternatives include various combinations of orthodontic, periodontal, and surgical therapy.5,22,26
Intrusion base arches or utility arches may succeed in reducing a gummy smile orthodontically in some cases (Fig. 10). Such treatment can produce a remarkable change in facial appearance.19 Selective intrusive and restorative techniques can also be used to improve the final esthetic result in patients with fractured or overerupted and abraded incisors.22,28
In other instances, gingival display can be eliminated by a simple gingivectomy (Fig. 11) or surgical crown lengthening with removal of crestal alveolar bone.22,26,29 Such procedures are particularly indicated in cases with altered passive eruption, excessive gingival margins, and short clinical crowns, because they will expose more of the anatomical crowns. When crestal alveolar bone is removed during surgical crown lengthening, the gingival margin will stabilize within six months at about 3mm from the new bone level.29
The type of gingival surgery depends on the relationship between the alveolar bone crest and the cementoenamel junction. At the end of orthodontic treatment, a labial gingivectomy to the bottom of the clinical pocket may produce a net gain of 1mm or more in crown length, or about half the probing length30,31 (Fig. 11). The gingivectomy is especially useful in eliminating the accumulation of hyperplastic gingiva often associated with fixed appliance therapy. Wennström has demonstrated that even if the gingivectomy is extended into the alveolar mucosa, the regenerated tissue will still be normal gingiva with keratinized epithelium.32 When a local labial gingivectomy is performed on an adult, the cut should be reduced mesiodistally to eliminate the risk of interdental recession31 (Fig. 11C).
Treatment of the most severe gummy smiles may require maxillary superior repositioning surgery (Le Fort I osteotomy), along with reduction of the associated vertical maxillary excess.5 This approach does have limitations, however, since the upper lip may be considerably shortened.33-35
It should be mentioned that some marginal gingival display in smiling is not as objectionable to lay people as orthodontists and oral surgeons might imagine. Peck and colleagues remarked that in the 1989 Miss America pageant, five of the 51 contestants had conspicuous gummy smiles.5 Furthermore, because of the gradual drooping of the lips over time, there is reasonable evidence that a gummy smile will diminish with age.7 Orthodontists should therefore look on a moderately gummy smile as an acceptable anatomical variation well within the usual range of lip-tooth-jaw relationships, especially for women.5,6
Conclusion
This discussion of some esthetic factors involved in tooth display in normal conversation and smiling has emphasized the following clinical guidelines:
- Study the patient from the front to make a reliable esthetic evaluation.
- Routinely take extraoral photographs that record the pre- and post-treatment tooth display with the lips at rest.
- Be careful not to overintrude the maxillary incisors in a patient with average or low smile type.
- Establish an age-appropriate vertical anterior tooth display in rest position and normal conversation.
- Provide a curve of the maxillary incisors that is parallel to the inner contour of the lower lip in smiling.
- Reduce excessive gingival exposure in a long-faced patient by active maxillary incisor intrusion coupled, if necessary, with labial gingivectomies.
REFERENCES
- 1. Nash, D.A.: Professional ethics and esthetic dentistry, J. Am. Dent. Assoc. 115:7E-9E, 1988.
- 2. Pogrel, M.A.: What are normal esthetic values? J. Oral Maxillofac. Surg. 49:963-969, 1991.
- 3. Lombardi, R.E.: The principles of visual perception and their clinical application to denture esthetics, J. Prosth. Dent. 29:358-382, 1973.
- 4. Tjan, A.H.L. and Miller, G.D.: The JGP: Some esthetic factors in a smile, J. Prosth. Dent. 51:24-28, 1984.
- 5. Peck, S.; Peck, L.; and Kataja, M.: The gingival smile line, Angle Orthod. 62:91-100, 1992.
- 6. Peck, S.; Peck, L.; and Kataja, M.: Some vertical lineaments of lip position, Am. J. Orthod. 101:519-524, 1992.
- 7. Vig, R.G. and Brundo, G.C.: The kinetics of anterior tooth display, J. Prosth. Dent. 39:502-504, 1978.
- 8. Mack, M.R.: Vertical dimension: A dynamic concept based on facial form and oropharyngeal function, J. Prosth. Dent. 66:478-485, 1991.
- 9. Mack, M.R.: Perspective of facial esthetics in dental treatment planning, J. Prosth. Dent. 75:169-176, 1996.
- 10. Peck, S. and Peck, H.: The aesthetically pleasing face: An orthodontic myth, Trans. Eur. Orthod. Soc. 47:175-185, 1971.
- 11. Rosen, H.M. and Ackerman, J.L.: Porous black hydroxyapatite in orthognathic surgery, Angle Orthod. 61:185-191, 1991.
- 12. Kokich, V.G. and Spear, F.M.: Guidelines for managing the orthodontic-restorative patient, Semin. Orthod. 3:3-20, 1997.
- 13. Turley, P.K.: Orthodontic management of the short face patient, Semin. Orthod. 2:138-152, 1996.
- 14. Johnston, L.E.: Personal communication, 1997.
- 15. Burstone, C.J.: Lip posture and its significance in treatment planning, Am. J. Orthod. 53:262-284, 1967.
- 16. Kokich, V.G. and Spear, F.: Interdisciplinary treatment: The key to managing implants and dentofacial esthetics, precongress course, European Orthodontic Society, Valencia, Spain, June 1997.
- 17. Shroff, B.; Yoon, W.M.; Lindauer, S.J.; and Burstone, C.J.: Simultaneous intrusion and retraction using a three-piece base arch, Angle Orthod. 67:455-462, 1997.
- 18. Mackley, R.J.: An evaluation of smiles before and after orthodontic treatment, Angle Orthod. 63:183-190, 1993.
- 19. Mackley, R.J.: "Animated" orthodontic treatment planning, J. Clin. Orthod. 27:361-365, 1993.
- 20. Ricketts, R.M.; Bench, R.W.; Gugino, C.F.; Hilgers, J.J.; and Schulhof, R.J.: Bioprogressive Therapy, RMO, Denver, 1979.
- 21. Brisman, A.S.: Esthetics: A comparison of dentist's and patient's concepts, J. Am. Dent. Assoc. 100:345-352, 1980.
- 22. Kokich, V.G.: Esthetics: The orthodontic-periodontic-restorative connection, Semin. Orthod. 2:21-30, 1996.
- 23. Hulsey, C.M.: An esthetic evaluation of lip-teeth relationships present in the smile, Am. J. Orthod. 57:132-144, 1970.
- 24. Janzen, E.K.: A balanced smile--a most important treatment objective, Am. J. Orthod. 72:359-372, 1977.
- 25. Kokich, V.: Esthetics and anterior tooth position: An orthodontic perspective, Part I: Crown length; Part II: Vertical position; Part III: Mediolateral relationships, J. Esth. Dent. 5:19-23, 174-178, 200-207, 1993.
- 26. Garber, D.A. and Salama, M.A.: The aesthetic smile: Diagnosis and treatment, Periodontol. 2000 11:18-28, 1996.
- 27. Rigsbee, O.H.; Sperry, T.P.; and BeGole, E.A.: The influence of facial animation on smile characteristics, Int. J. Adult Orthod. Orthog. Surg. 3:233-239, 1988.
- 28. Kokich, V.G.; Nappen, D.L.; and Shapiro, P.A.: Gingival contour and clinical crown length: Their effect on the esthetic appearance of maxillary anterior teeth, Am. J. Orthod. 86:89-94, 1984.
- 29. Brägger, U.; Lauchenauer, D.; and Lang, N.P.: Surgical lengthening of the clinical crown, J. Clin. Periodontol. 19:58-63, 1992.
- 30. Monefeldt, I. and Zachrisson, B.U.: Adjustment of clinical crown height by gingivectomy following orthodontic space closure, Angle Orthod. 47:256-264, 1977.
- 31. Zachrisson, B.U.: Orthodontics and periodontics, in Clinical Periodontology and Implant Dentistry, 3rd ed., ed. J. Lindhe, T. Karring, and N.P. Lang, Munksgaard, Copenhagen, 1997, pp. 741-793.
- 32. Wennström, J.L.: Regeneration of gingiva following surgical excision: A clinical study, J. Clin. Periodontol. 10:287-297, 1983.
- 33. Rosen, H.M.: Lip-nasal aesthetics following Le Fort I osteotomy, Plast. Reconstr. Surg. 81:171-179, 1988.
- 34. Proffit, W.R. and Phillips, C.: Adaptations in lip posture and pressure following orthognathic surgery, Am. J. Orthod. 93:294-302, 1988.
- 35. Sarver, D.M. and Weissman, S.M.: Long-term soft tissue response to Le Fort I maxillary superior repositioning, Angle Orthod. 61:267-276, 1991.
-
 DR. ZACHRISSON
DR. ZACHRISSON
Dr. Zachrisson is a Contributing Editor of the Journal of Clinical Orthodontics and a Professor of Orthodontics at the University of Oslo. He is in the private practice of orthodontics at Stortingsgt. 10, 0161 Oslo, Norway. This article is adapted by permission from the Proceedings of the 11th International Conference for Orthodontists, Verlag Neuer Merkur, Munich, Germany, 1998.