2002 JCO Study of Orthodontic Diagnosis and Treatment Procedures, Part 3: More Breakdowns of Selected Variables
The first article in this three-part series on the 2002 JCO Study of Orthodontic Diagnosis and Treatment Procedures (JCO, October 2002) presented the methodology and basic results of the survey, as well as trends since the first Treatment Study was conducted in 1986. In last month's installment and this concluding article, we break down the routine usage of the most important diagnostic and treatment methods according to number of years in practice, geographic region, and gross income level.
KEY TO GEOGRAPHIC REGIONS
NE = New England (CT, ME, MA, NH, RI, VT)
MA = Middle Atlantic (NJ, NY, PA)
SA = South Atlantic (DE, DC, FL, GA, MD, NC, SC, VA, WV)
ESC = East South Central (AL, KY, MS, TN)
ENC = East North Central (IL, IN, MI, OH, WI)
WNC = West North Central (IA, KS, MN, MO, NE, ND, SD)
MTN = Mountain (AZ, CO, ID, MT, NV, NM, UT, WY)
WSC = West South Central (AR, LA, OK, TX)
PAC = Pacific (AK, CA, HI, OR, WA)
Archwires
Similar articles from the archive:
- 1996 JCO Study of Orthodontic Diagnosis and Treatment Procedures, Part 3: More Breakdowns of Selected Variables January 1997
- 1990 JCO Study of Orthodontic Diagnosis and Treatment Procedures, Part 3: More Breakdowns of Selected Variables May 1991
- 1986 JCO Study of Orthodontic Diagnosisand Treatment Procedures Part 2 Selected Breakdowns October 1986
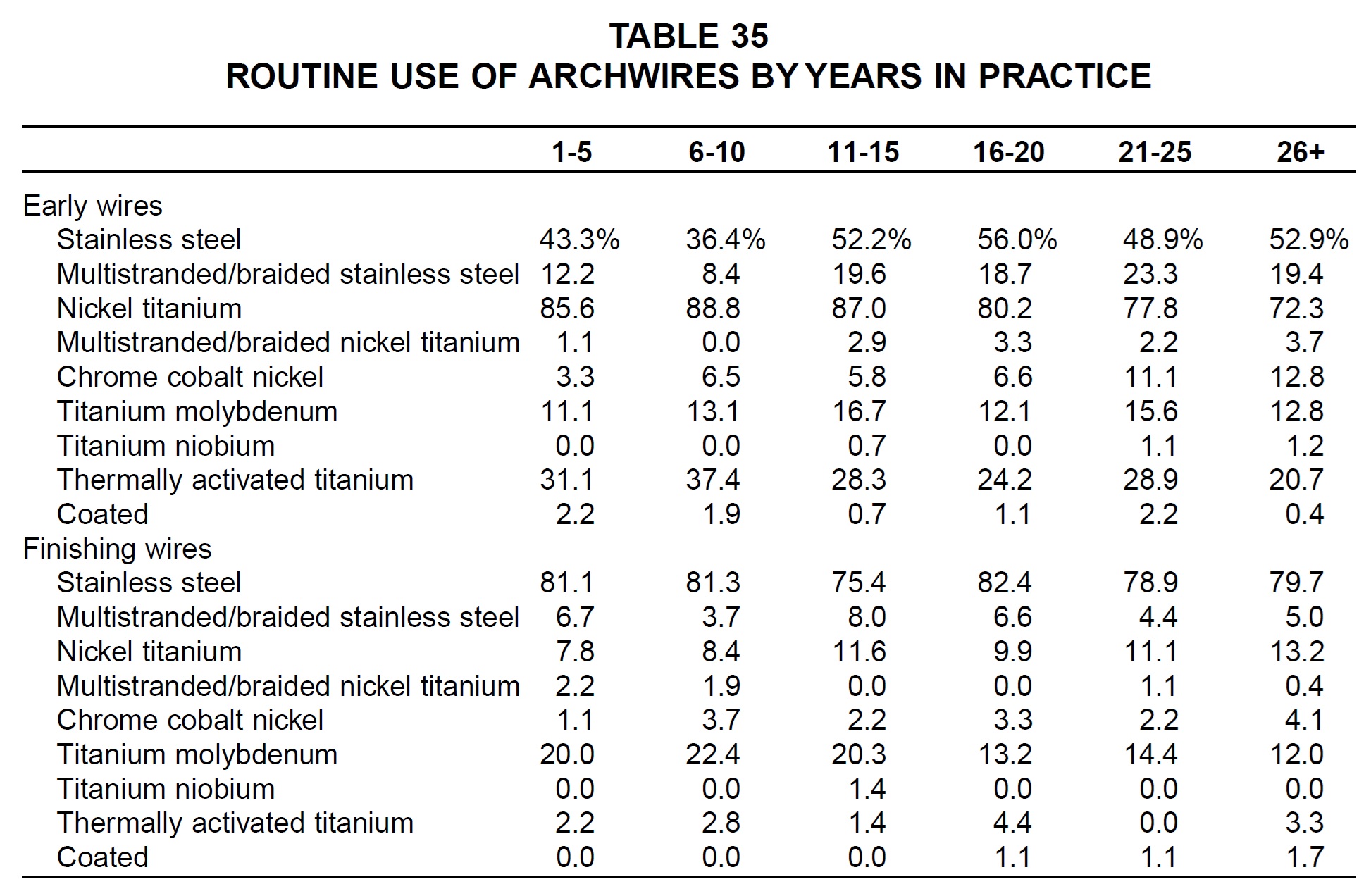
In general, the newer practices were more likely to use titanium alloys than stainless steel for initial archwires, with the opposite being true of older practices (Table 35). More than three-quarters of each age group used stainless steel finishing wires, but those who had been in practice less than 16 years used TMA finishing wires more routinely than others did. Older practices were more routine users of chrome cobalt nickel (Elgiloy) archwires in both stages of treatment.
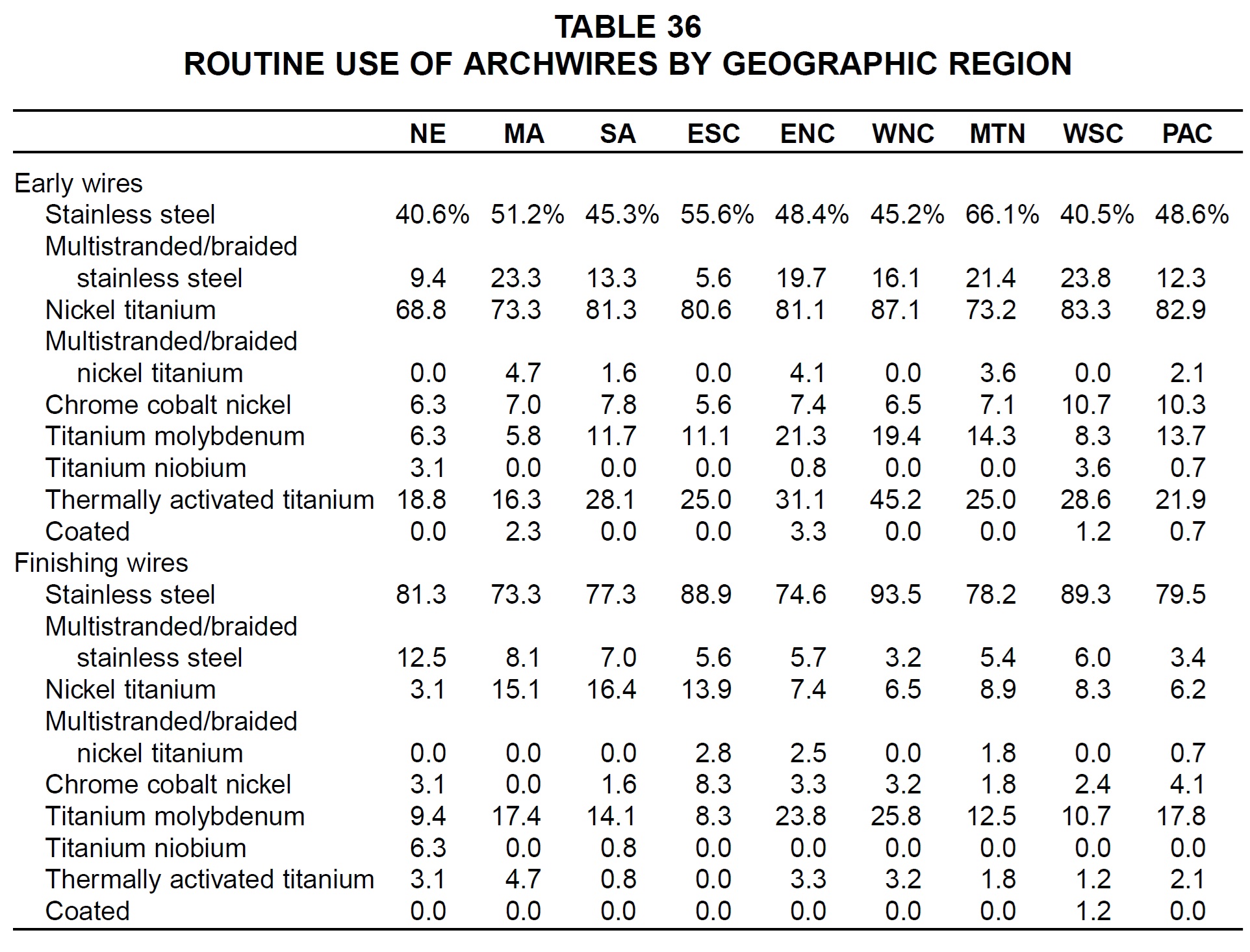
Stainless steel early archwires were used most routinely in the Mountain region, whereas nickel titanium and superelastic titanium early archwires were most popular in the West North Central region (Table 36). Multistranded and braided stainless steel early archwires were used most routinely in the West South Central and Middle Atlantic regions, and TMA early archwires in the East and West North Central regions. West North Central practices also reported the highest percentages of stainless steel and TMA finishing archwires. Multistranded and braided stainless steel finishing archwires were used most routinely in New England, and nickel titanium finishing archwires in the South and Middle Atlantic regions.
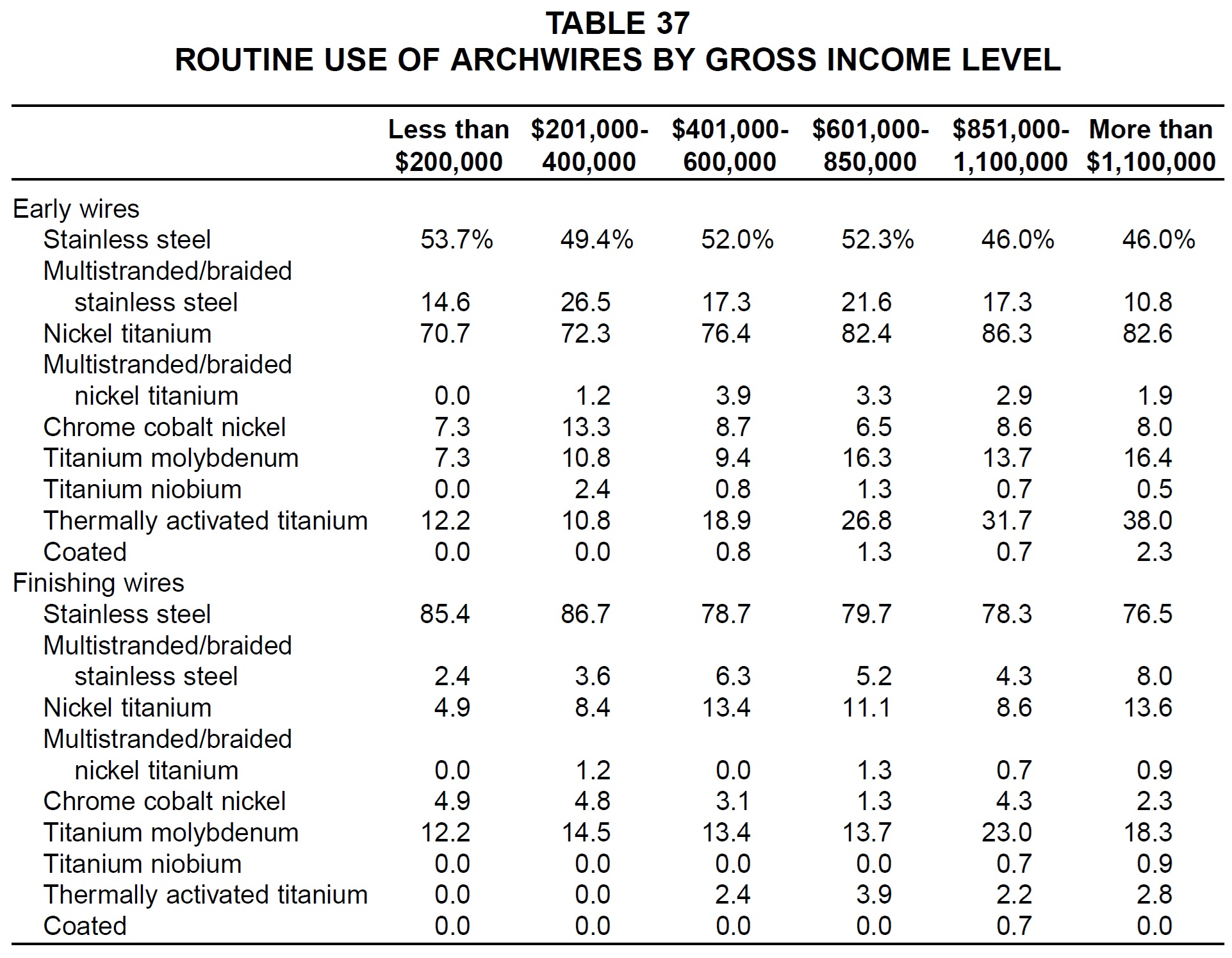
Respondents with higher gross income were more likely than others to use titanium alloys for both initial and finishing archwires (Table 37). Those with lower gross income were more likely to use stainless steel.
Removable and Functional Appliances
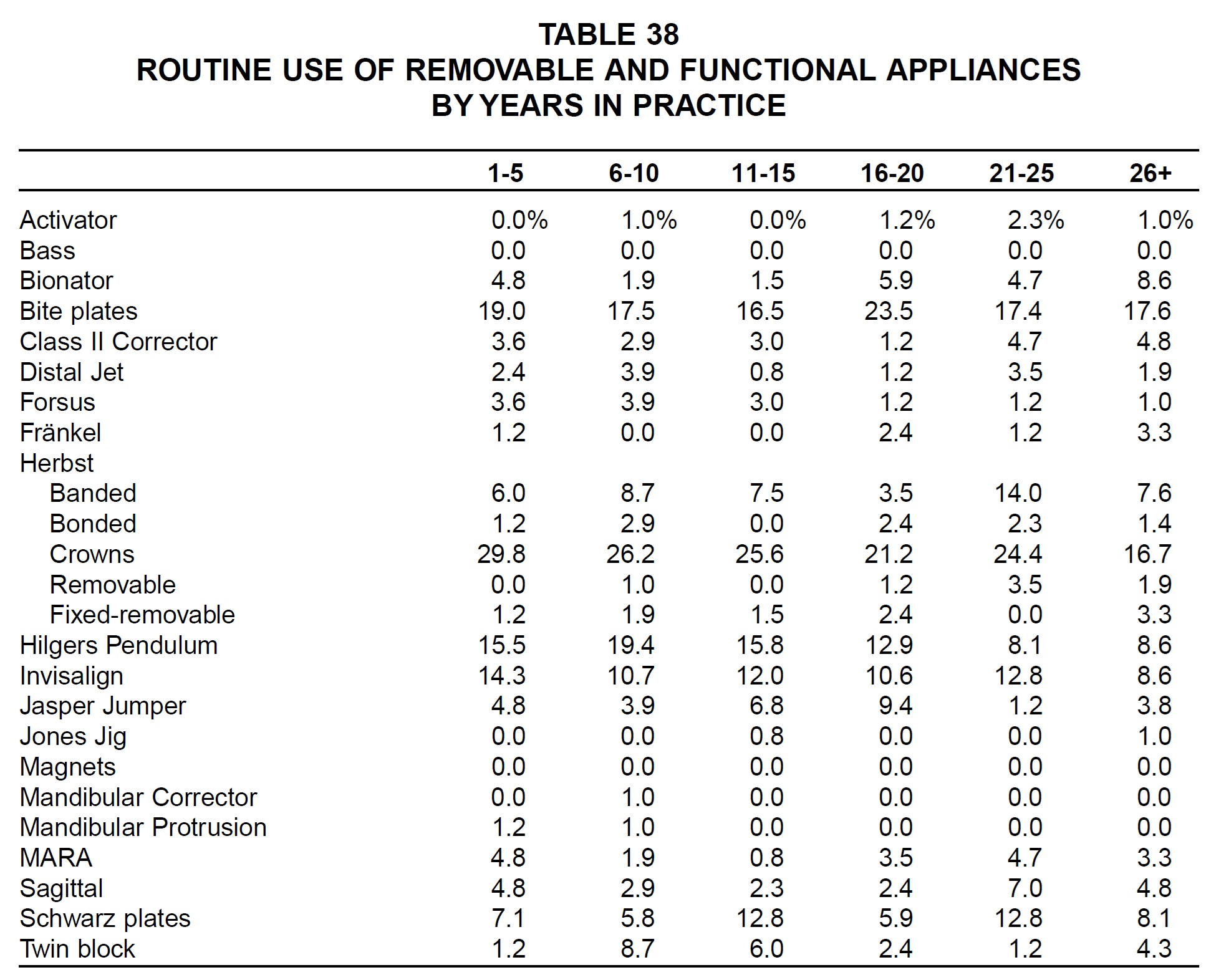
Among the removable and functional appliances surveyed, the newer practices were the more routine users of the Forsus appliance, Herbst with crowns, Hilgers Pendulum, Invisalign, Mandibular Corrector, Mandibular Protrusion Appliance, and MARA (Table 38). Older practices were the more routine users of the activator, bionator, Class II Corrector, Fränkel, removable and fixed-removable Herbsts, and sagittal appliance.
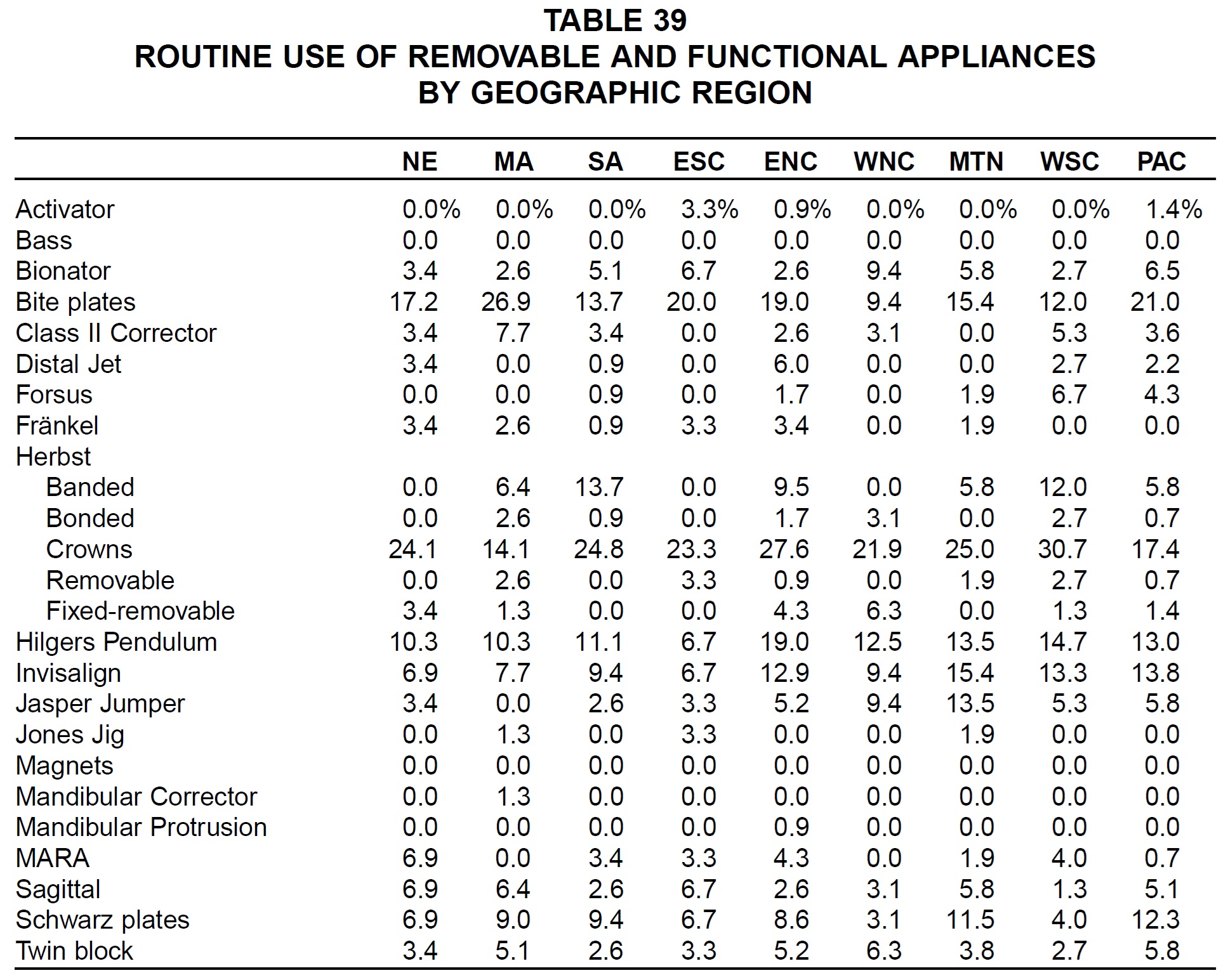
Regionally, the most routine users of the activator, removable Herbst, and Jones Jig were in the East South Central region; of the bionator, bonded and fixed-removable Herbsts, and twin block in the West North Central region; of biteplates, the Class II Corrector, and the Mandibular Corrector in the Middle Atlantic region; of the Distal Jet, Hilgers Pendulum, and Mandibular Protrusion Appliance in the East North Central region; of the Forsus appliance and Herbst with crowns in the West South Central region; of the banded Herbst in the South Atlantic region; of the Invisalign and Jasper Jumper in the Mountain region; of the MARA and sagittal appliances in New England; and of Schwarz plates in the Pacific region (Table 39).
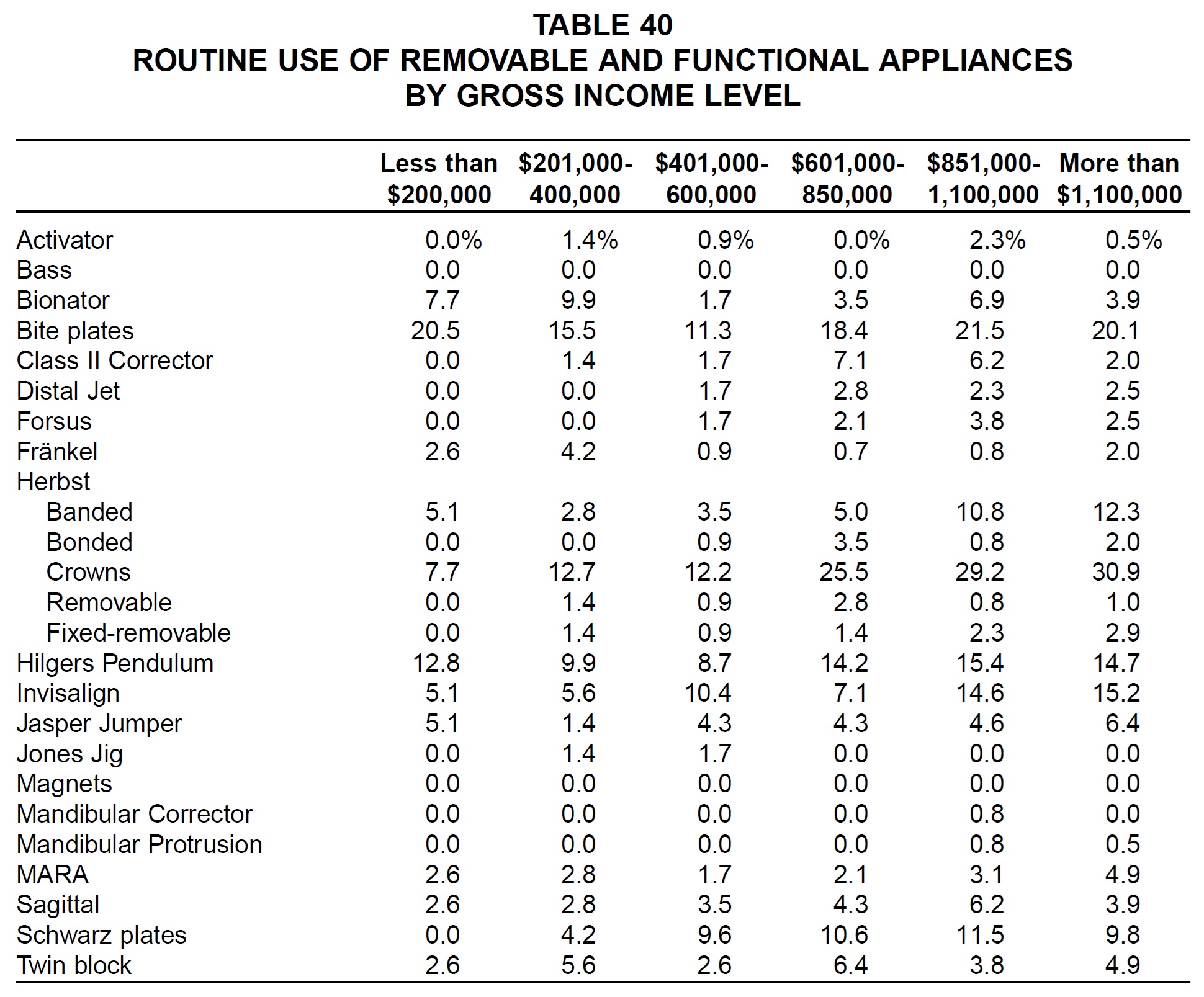
Many of the removable and functional appliances tended to be used more routinely in practices with higher gross income, including the Class II Corrector, Distal Jet, Forsus, Herbst, Hilgers Pendulum, Invisalign, Jasper Jumper, Mandibular Corrector, Mandibular Protrusion Appliance, and MARA (Table 40).
Headgear
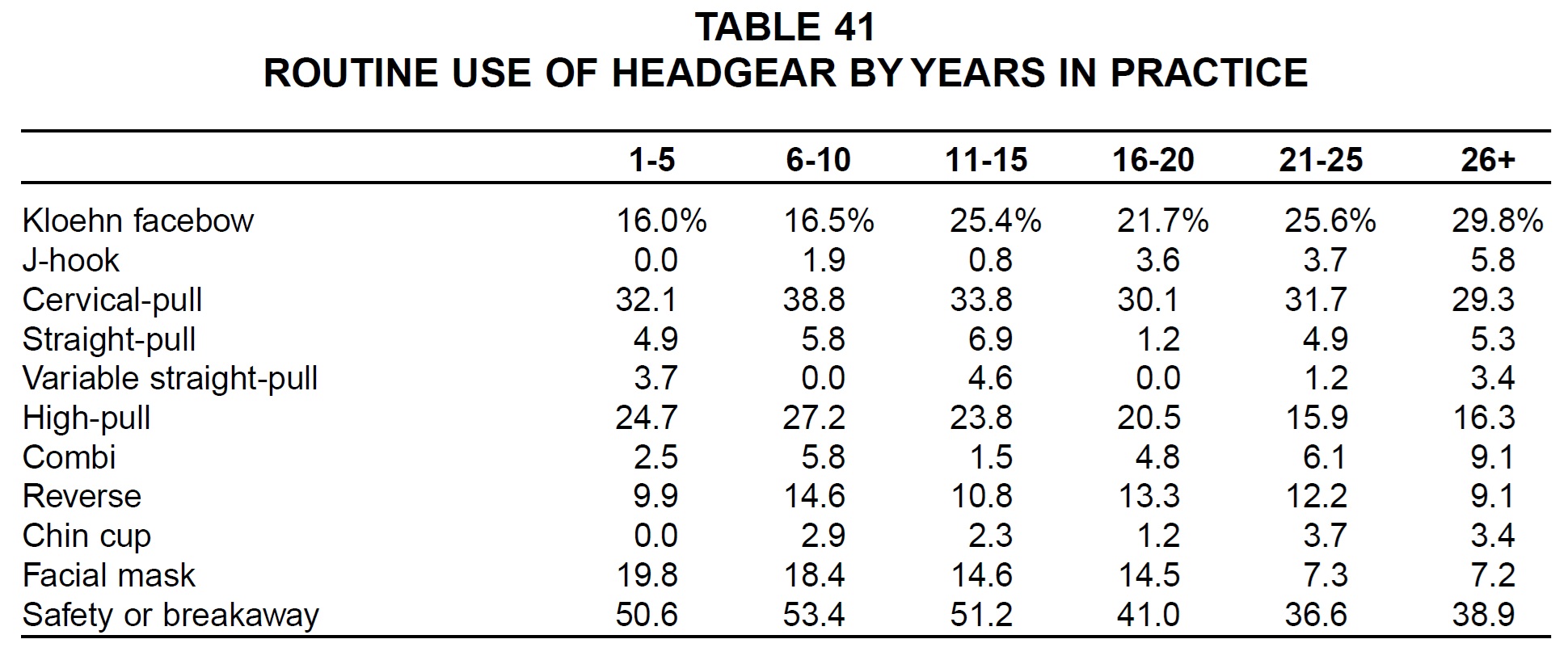
Respondents who had been in practice longer were more likely to use Kloehn facebows, J-hook headgear, and chin cups, while newer practices were more likely to use high-pull and reverse headgear, facial masks, and safety or breakaway devices (Table 41).
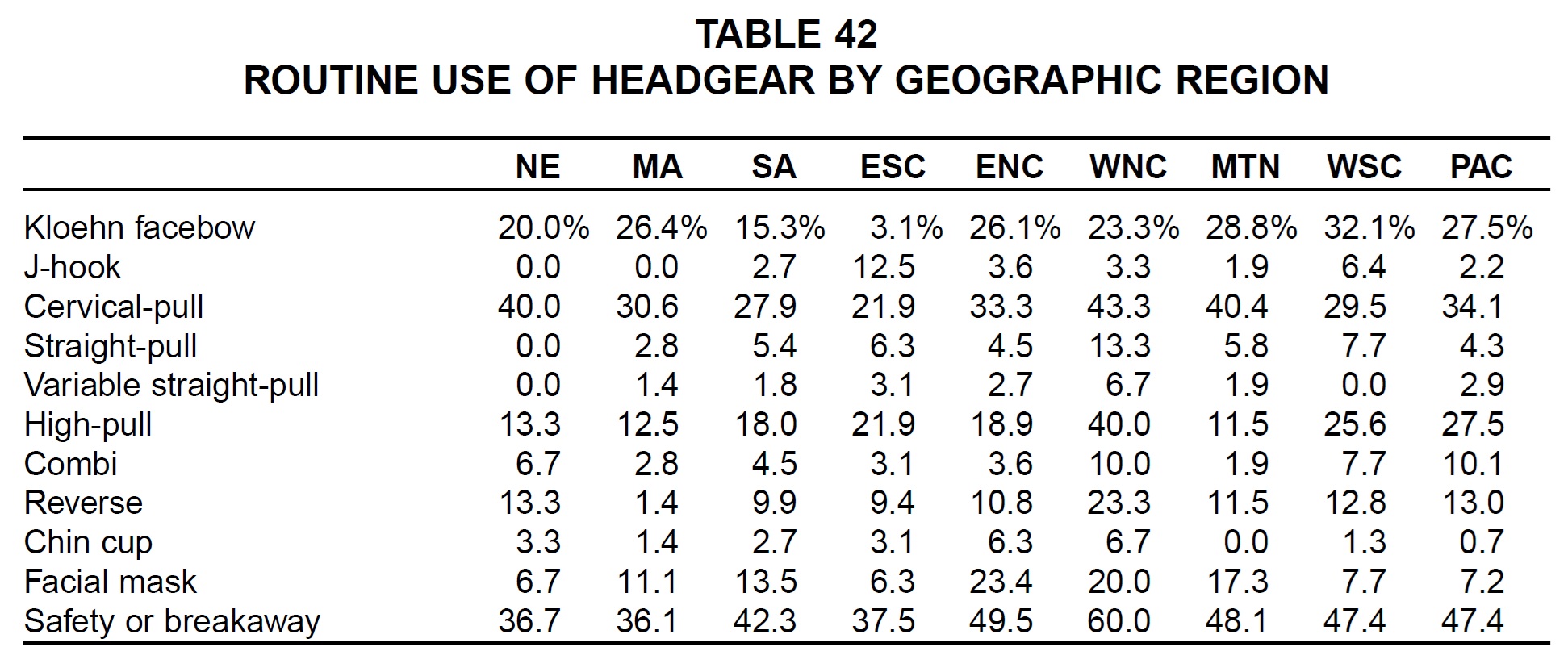
Kloehn facebows were used most routinely in the West South Central region (Table 42). East South Central orthodontists were the most frequent users of J-hook headgear and the least frequent users of Kloehn facebows. Reverse headgear, chin cups, and safety or breakaway devices were most routinely used in the West North Central region. Facial masks were most popular in the East North Central region.
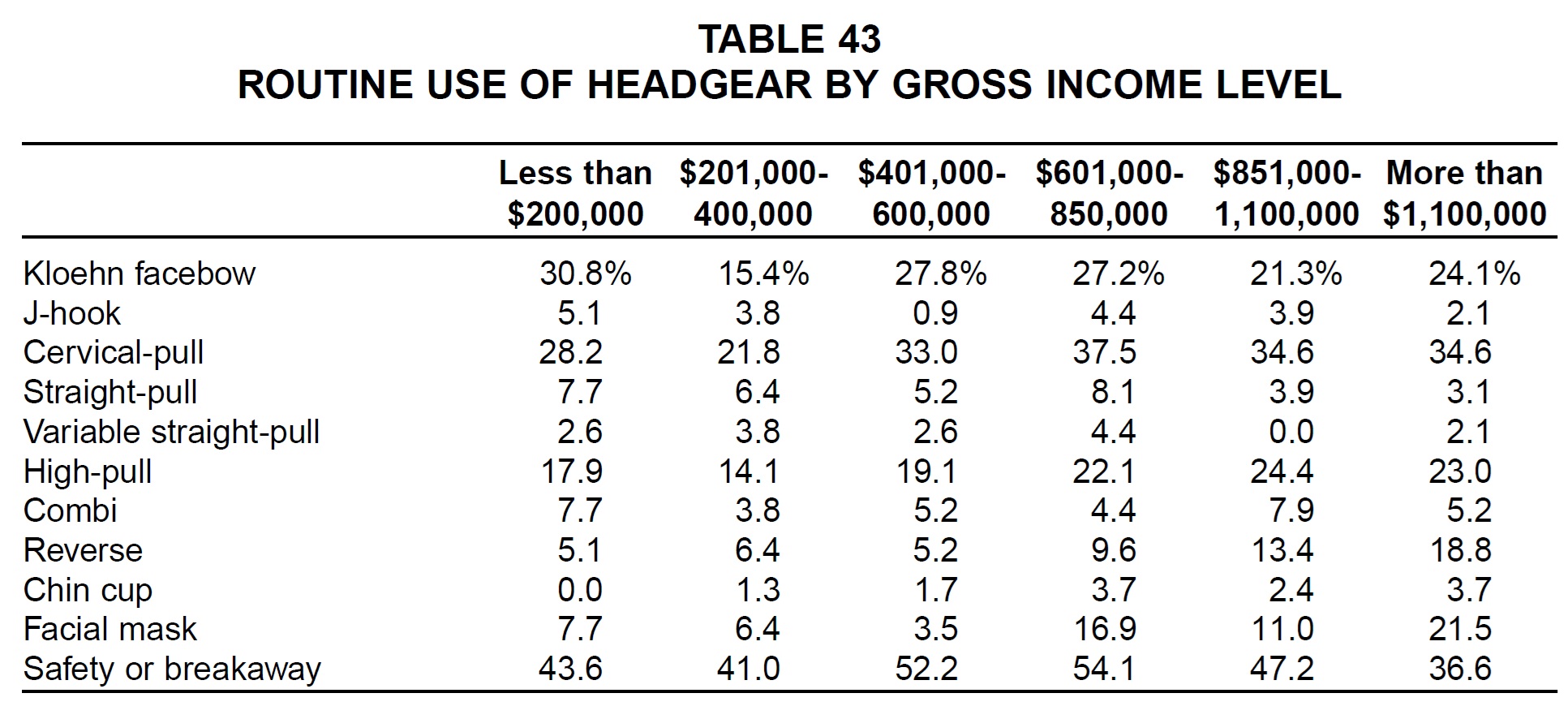
Practices with the lowest gross income were the most likely to use Kloehn facebows (Table 43). Larger practices were more likely to use high-pull and reverse headgear, chin cups, and facial masks.
Finishing Procedures
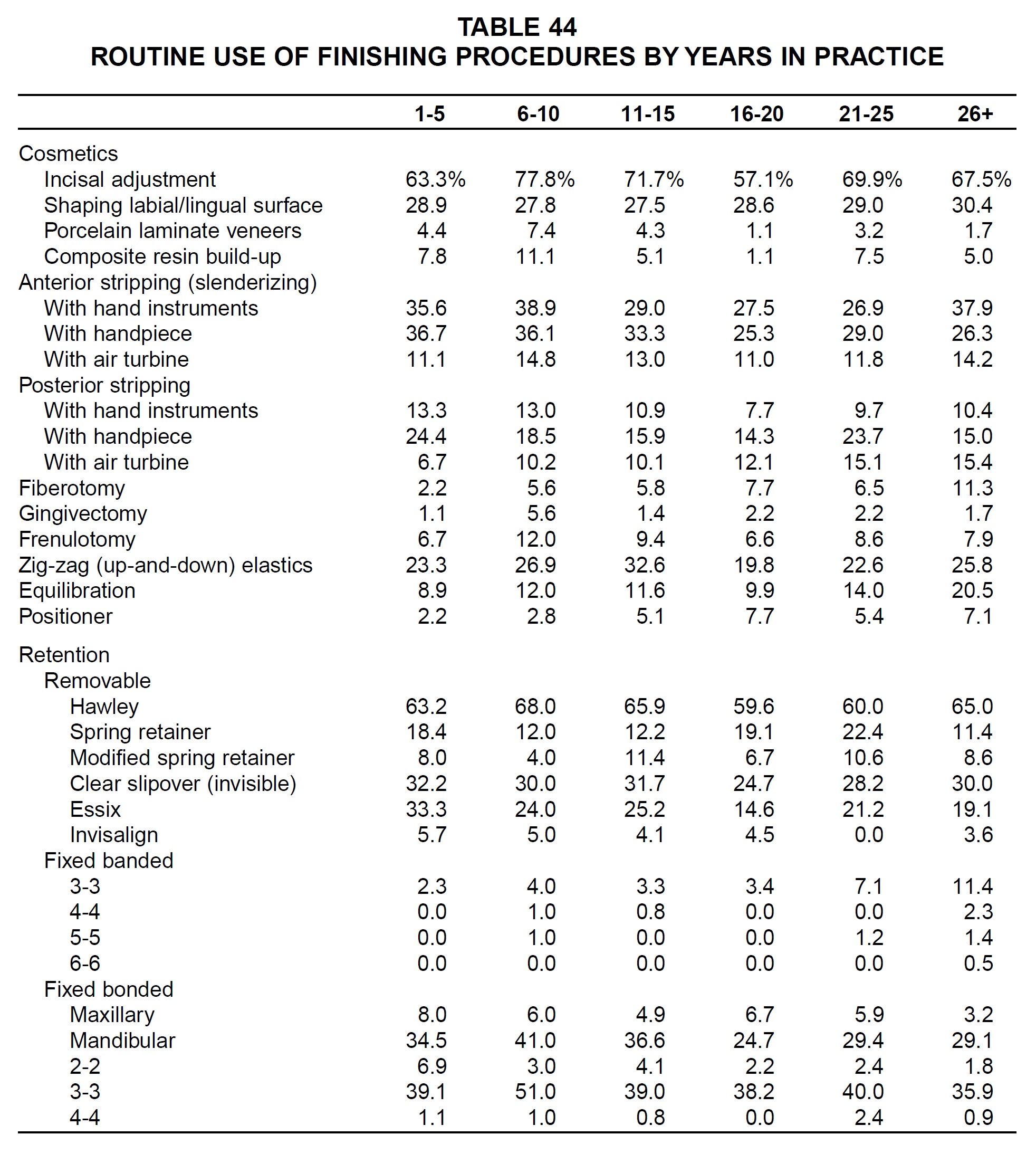
There was no discernible pattern in the use of cosmetic procedures or stripping by number of years in practice (Table 44). Older practices were somewhat more likely than others to routinely prescribe fiberotomies, equilibration, and positioners. "Invisible" types of retainers and fixed bonded retainers were clearly favored by the younger practitioners, while fixed banded retainers were used more routinely by older practitioners.
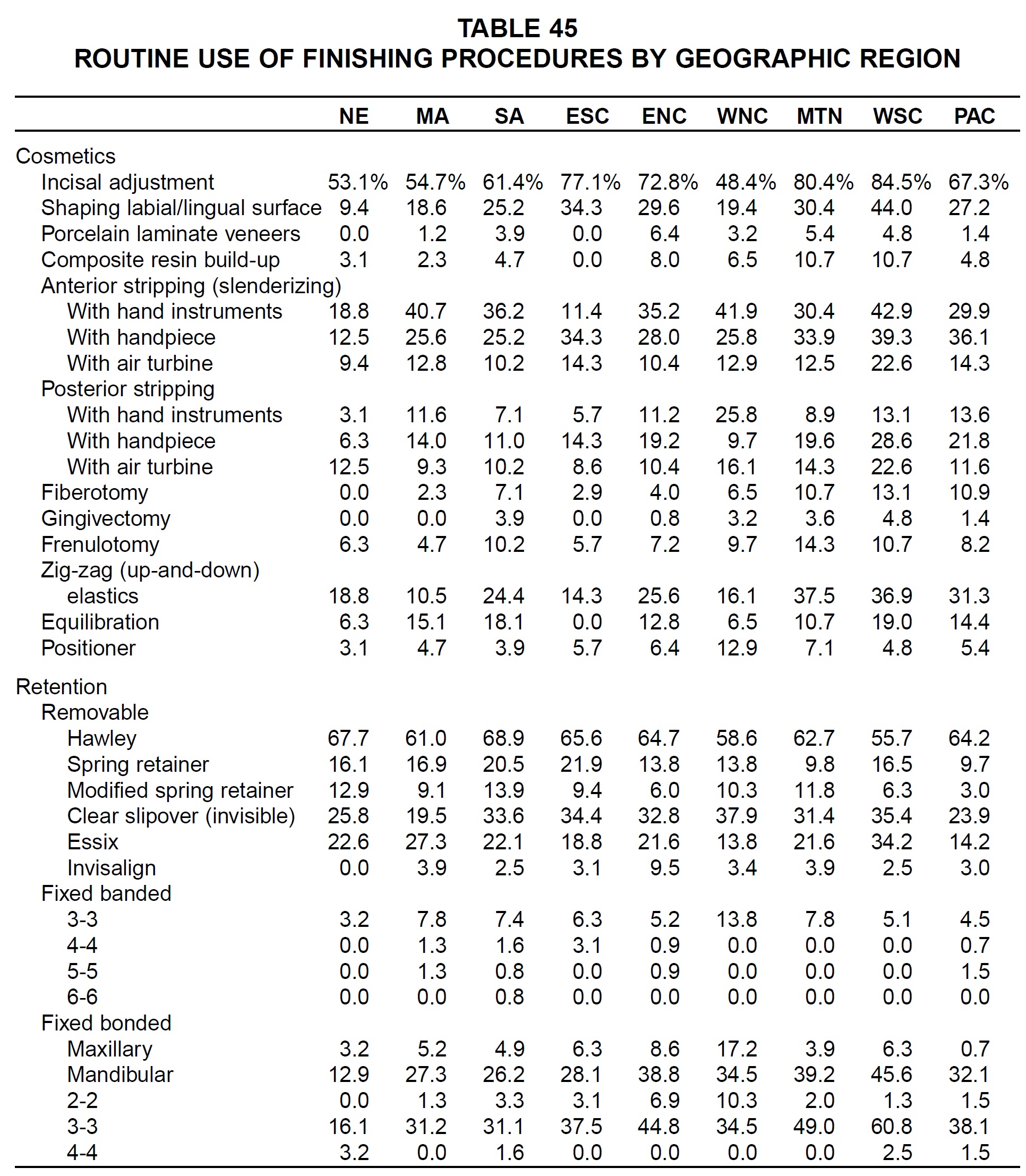
Cosmetic procedures and stripping were most routinely performed by West South Central area respondents and least routinely performed in New England (Table 45). Hawley and modified spring retainers were used most routinely in the South Atlantic region, spring retainers in the East South Central region, clear slipover and fixed banded retainers in the West North Central region, Essix and fixed bonded retainers in the West South Central region, and Invisalign retainers in the East North Central region.
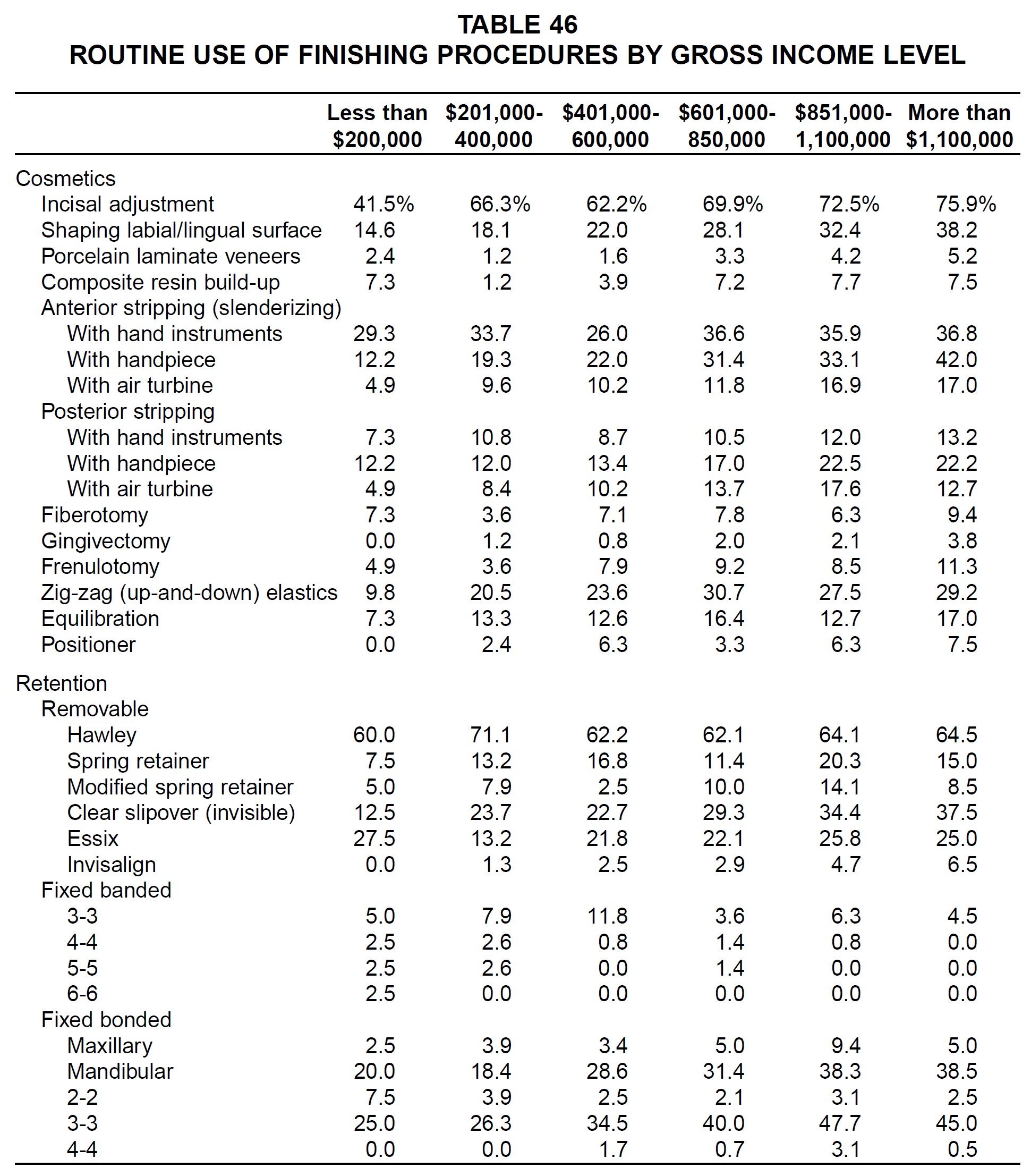
Routine use of every finishing procedure increased almost linearly with gross income (Table 46). The higher-income practices were also more likely to use clear slipover, Invisalign, and fixed bonded retainers, while lower-income practices were more likely to use Essix and fixed banded retainers.
Conclusion
Orthodontic diagnosis and treatment methods have not changed significantly over the 16-year-period covered by the JCO surveys. Nevertheless, several overall trends have emerged since 1986:
- Orthodontists are about five years older on average, and more than twice as many of them are women.
- Fewer diagnostic records are being taken on a routine basis.
- Many more orthodontists are using digital imaging and analysis.
- Nickel titanium alloys have replaced stainless steel as the material of choice for initial archwires.
- Light-cured adhesives have become much more popular than chemically cured composites.
- Fixed functional devices are used more routinely than removable appliances, and headgear use is declining.
- The percentage of patients treated with extractions is dropping.
- Cosmetic finishing procedures have become commonplace.
The next JCO Study of Orthodontic Diagnosis and Treatment Procedures may show a continuation of these trends, as well as the emergence of new technologies that at present can only be imagined.
-
 DR. KEIM
DR. KEIM -
 DR. GOTTLIEB
DR. GOTTLIEB -
 DR. NELSON
DR. NELSON -
 MR. VOGELS
MR. VOGELS
Dr. Keim is Editor, Dr. Gottlieb is Senior Editor, and Mr. Vogels is Managing Editor of the Journal of Clinical Orthodontics, 1828 Pearl St., Boulder, CO 80302. Dr. Nelson is Director and Research Consultant, Nelson Associates, Nederland, CO.