2002 JCO Study of Orthodontic Diagnosis and Treatment Procedures, Part 2: Breakdowns of Selected Variables
The methodology and basic results of the 2002 JCO Study of Orthodontic Diagnosis and Treatment Procedures were covered in last month's article, along with trends across the four surveys conducted since 1986. The final two parts in this series will break down the usage of the most interesting diagnostic and treatment methods among three different groups of respondents--by number of years in practice, geographic region, and gross income level.
KEY TO GEOGRAPHIC REGIONS
NE = New England (CT, ME, MA, NH, RI, VT)
MA = Middle Atlantic (NJ, NY, PA)
SA = South Atlantic (DE, DC, FL, GA, MD, NC, SC, VA, WV)
ESC = East South Central (AL, KY, MS, TN)
ENC = East North Central (IL, IN, MI, OH, WI)
WNC = West North Central (IA, KS, MN, MO, NE, ND, SD)
MTN = Mountain (AZ, CO, ID, MT, NV, NM, UT, WY)
WSC = West South Central (AR, LA, OK, TX)
PAC = Pacific (AK, CA, HI, OR, WA)
Patient Demographics
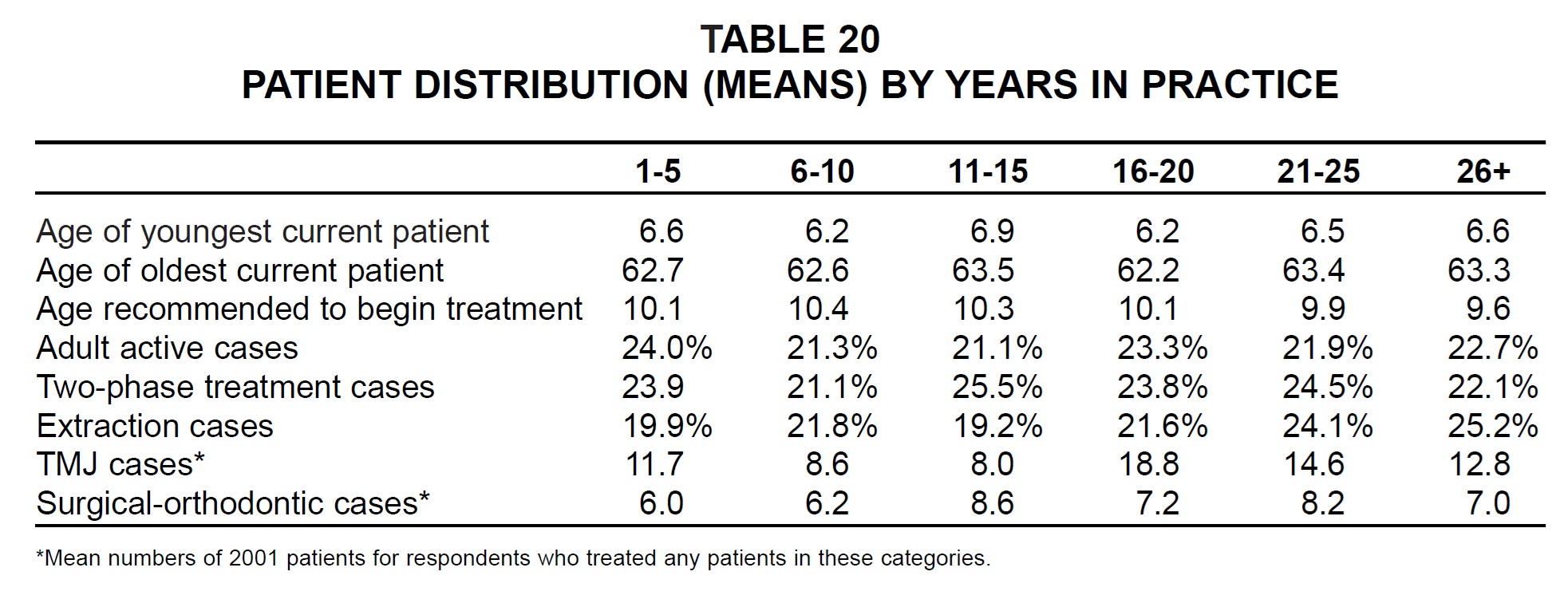
There was no noticeable difference in patient age by number of years in practice (Table 20). The newest practices reported the highest percentage of adult cases, and the oldest practices the highest percentage of extraction cases.
Similar articles from the archive:
- 1996 JCO Study of Orthodontic Diagnosis and Treatment Procedures, Part 2: Breakdowns of Selected Variables December 1996
- 1990 JCO Study of Orthodontic Diagnosis and Treatment Procedures, Part 2: Breakdowns of Selected Variables April 1991
- 1986 JCO Study of Orthodontic Diagnosisand Treatment Procedures Part 2 Selected Breakdowns October 1986
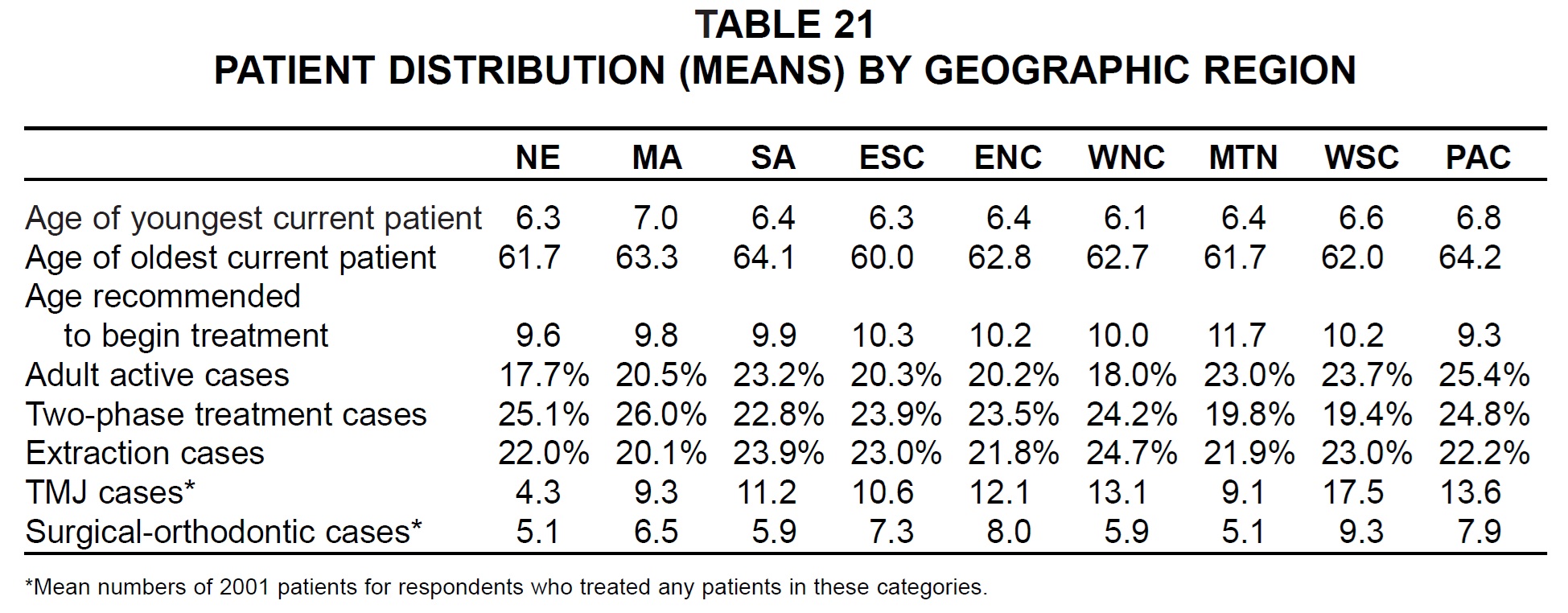
The mean age recommended to start treatment varied from a low of 9.3 years in the Pacific region to a high of 11.7 years in the Mountain region (Table 21). The highest percentage of adult patients was in the Pacific region, and the lowest in New England. Percentages of twophase patients ranged from 19.4% in the West South Central region to 26.0% in the Middle Atlantic. West North Central practices reported the highest mean percentage of extraction cases, and Middle Atlantic practices the lowest. The most TMJ and surgical-orthodontic patients were treated in the West South Central region, while New England orthodontists treated the fewest.
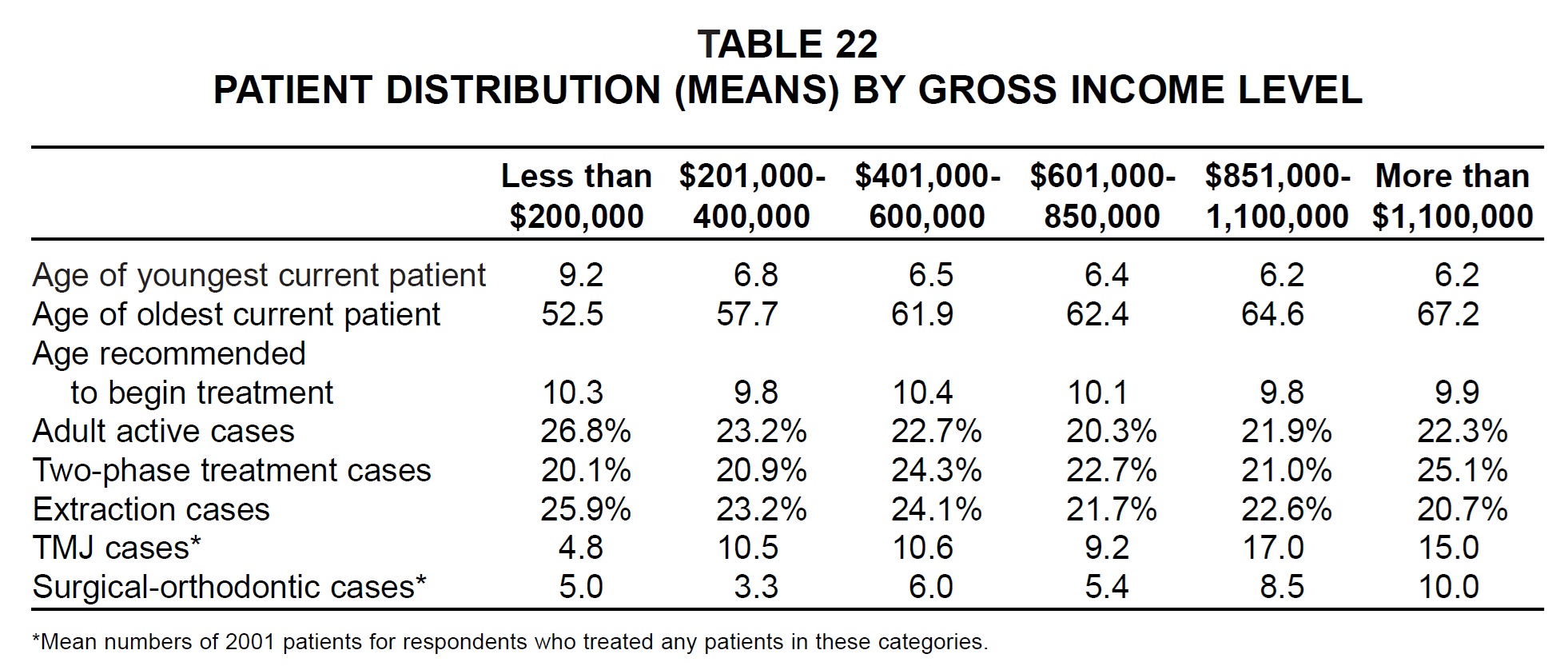
Respondents with the highest gross income reported both the youngest and the oldest patients (Table 22). Respondents with the lowest gross income showed the highest percentages of adult and extraction cases and the lowest percentages of two-phase cases. The largest practices treated the most TMJ and surgical-orthodontic patients.
Diagnostic Records
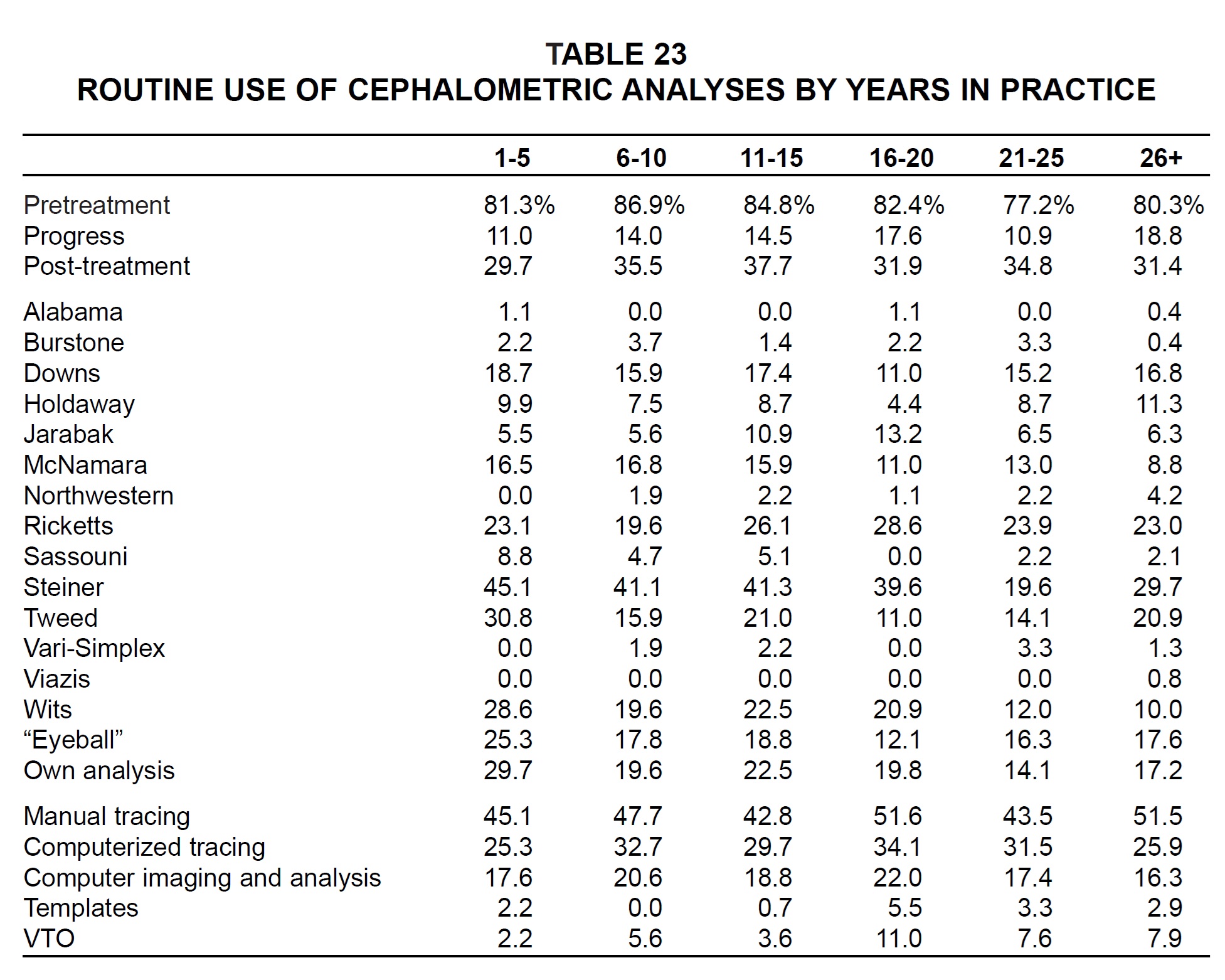
In general, the newest practices appeared to perform more different routine cephalometric analyses than older practices did (Table 23). The oldest practices were the least likely to use computerized tracings and imaging.
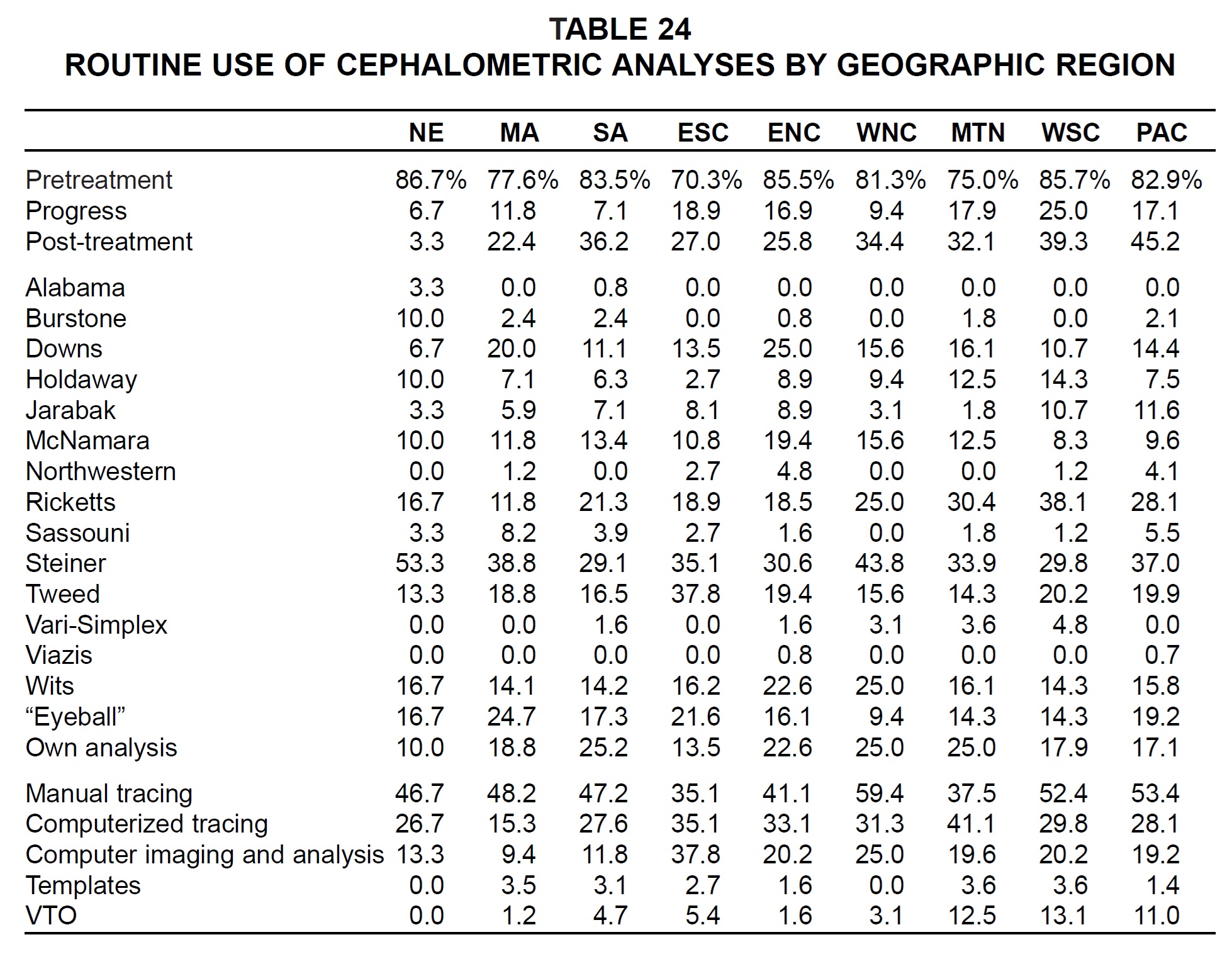
Regional differences could be seen in the use of many specific cephalometric analyses (Table 24). Of those used routinely by more than 10% of the respondents in any region, the Burstone and Steiner analyses were most popular in New England; the Downs and McNamara analyses in the East North Central region; the Jarabak analysis in the Pacific region; the Ricketts analysis in the West South Central region; the Tweed analysis in the East South Central region; and the Wits analysis in the West North Central region. Computerized tracings were performed most routinely by Mountain orthodontists, and computer imaging was used most by East South Central orthodontists.
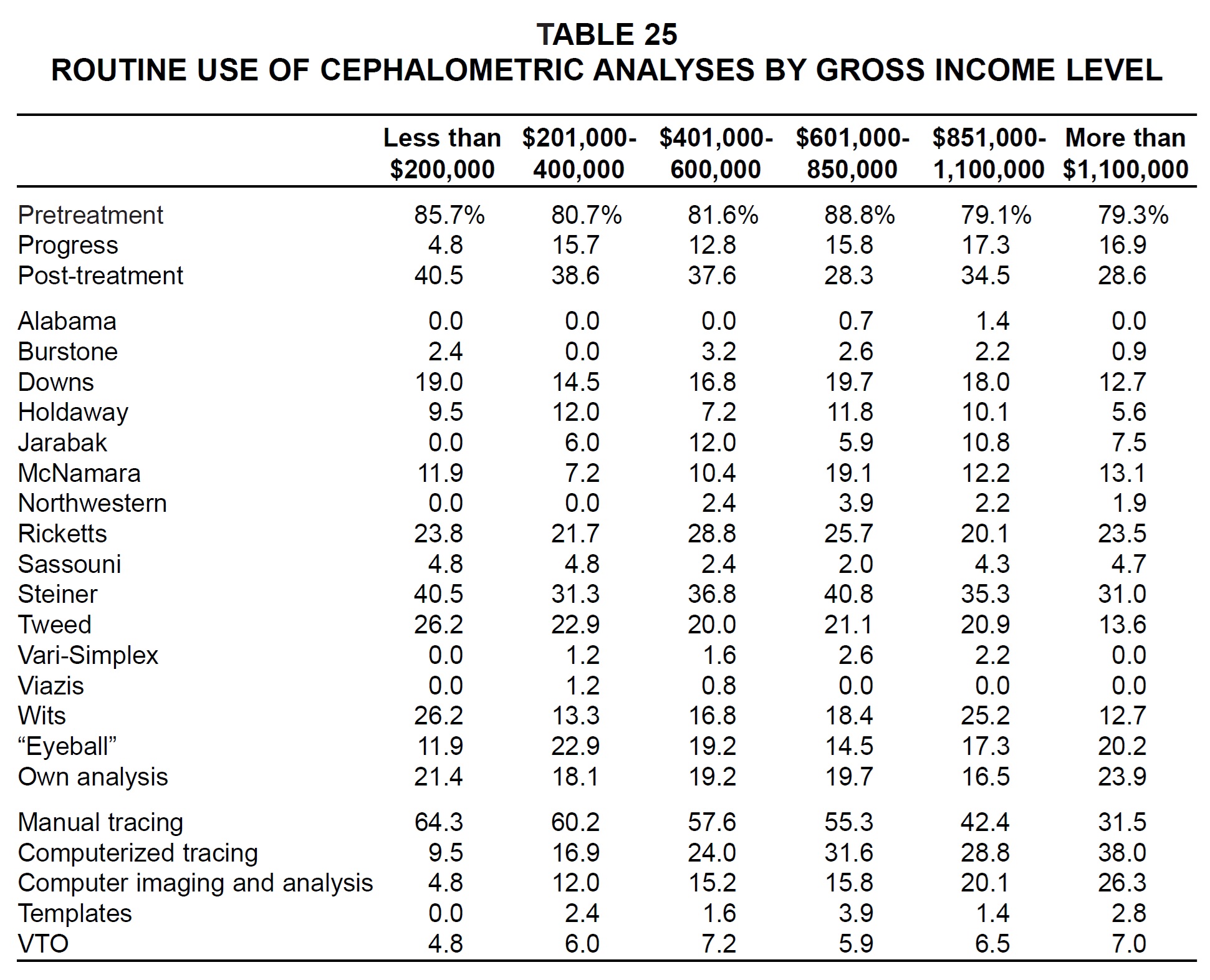
Practices with the highest gross income were the most likely to use their own analyses, computerized tracings, and computer imaging (Table 25). Practices with the lowest gross income performed the most routine post-treatment analyses, but the least routine progress analyses, and were the greatest users of the Tweed and Wits methods.
Fixed Appliances
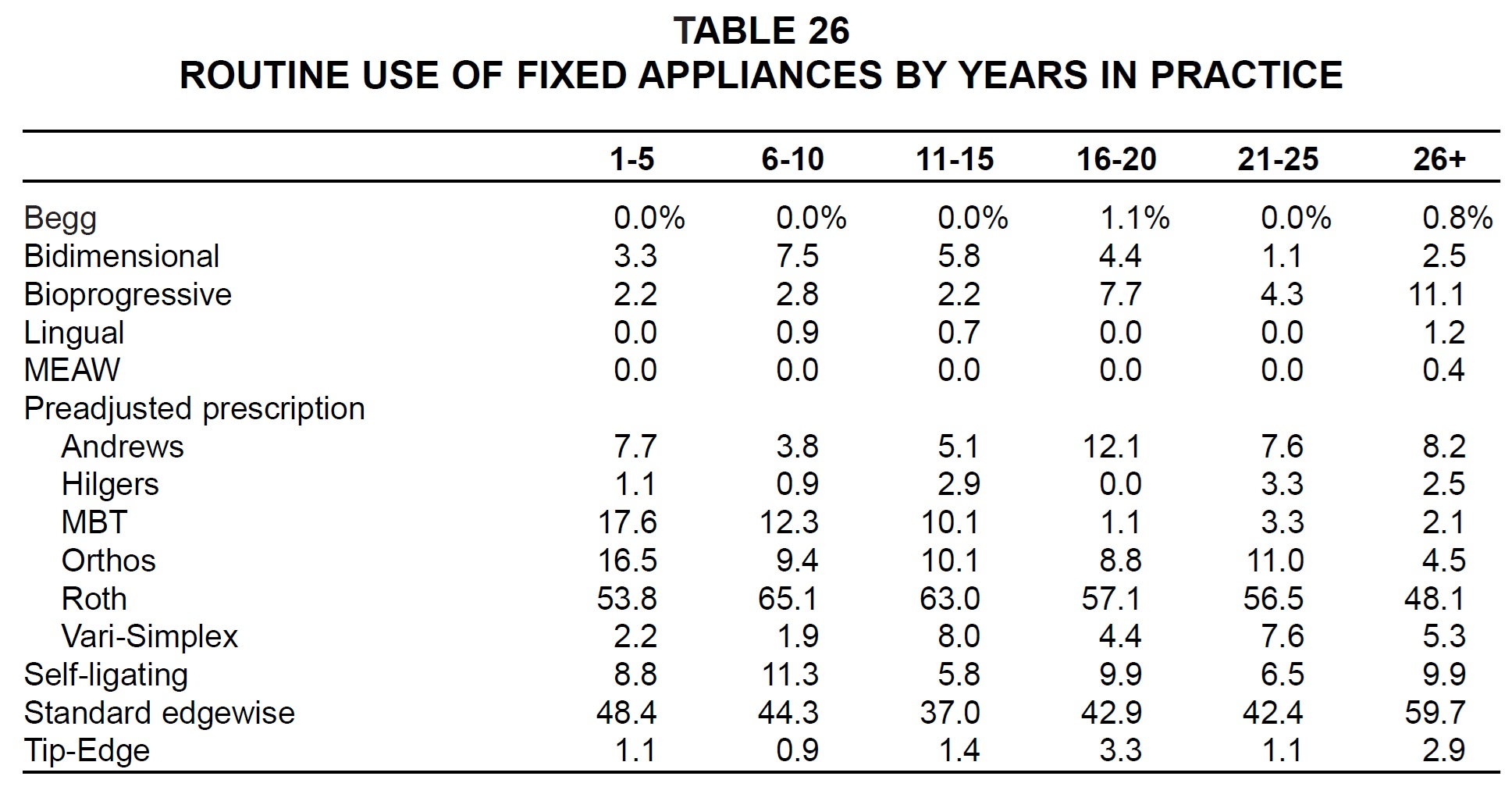
Respondents who had been in practice the longest were the most likely to use Bioprogressive, lingual, and standard edgewise appliances (Table 26). Among the preadjusted appliance prescriptions, MBT and Orthos were more popular among the newer practices, and the Roth prescription among those who had been in practice for six to 15 years.
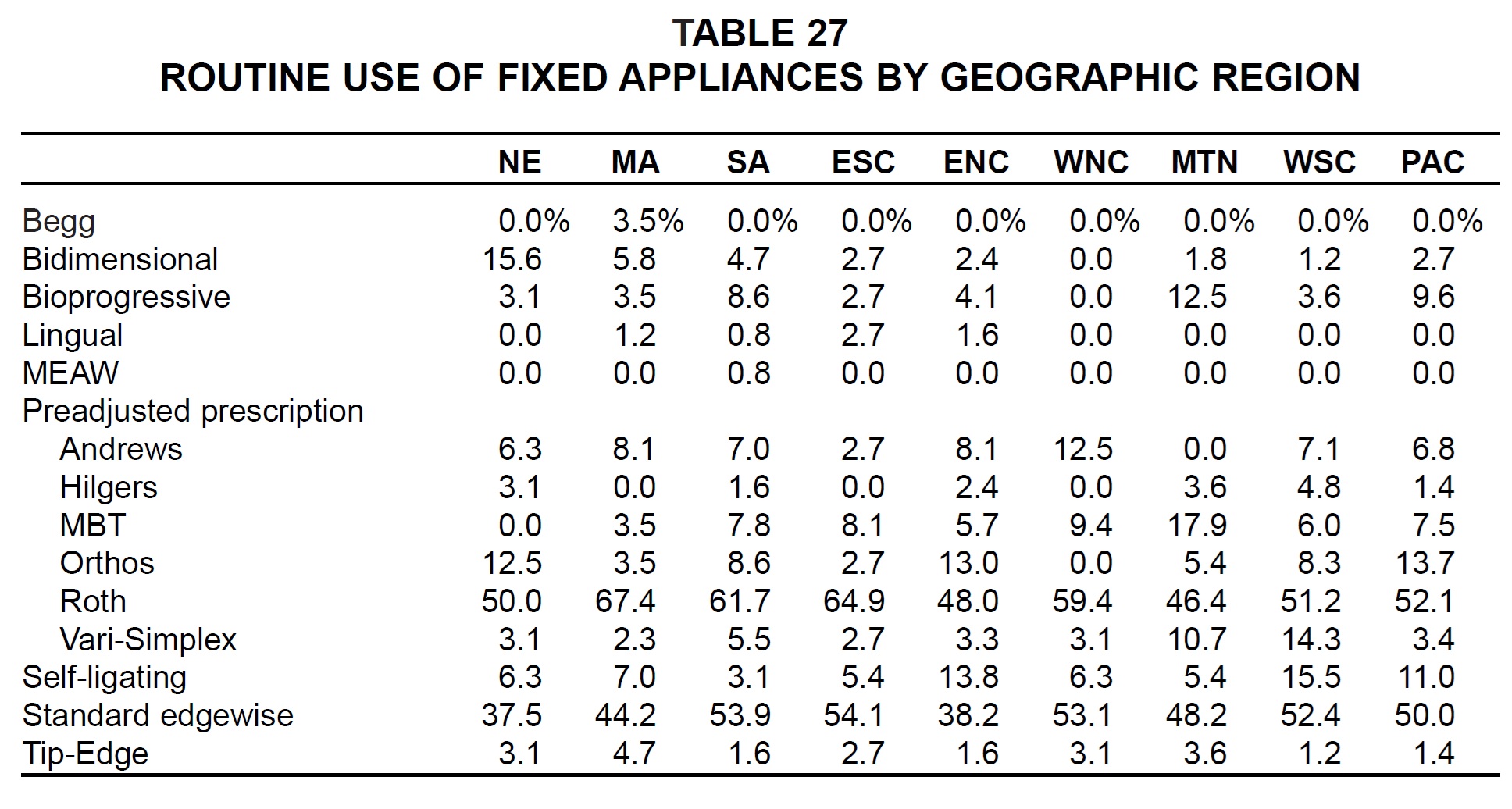
The only practices routinely using Begg appliances were in the Middle Atlantic region; the only routine users of the MEAW system were in the South Atlantic states (Table 27). Bidimensional appliances were most popular in New England; Bioprogressive and MBT in the Mountain region; lingual and standard edgewise in the East South Central region; Andrews in the West North Central region; Hilgers, Vari-Simplex, and self-ligating in the West South Central region; Orthos in the Pacific region; and Roth and Tip-Edge in the Middle Atlantic region.
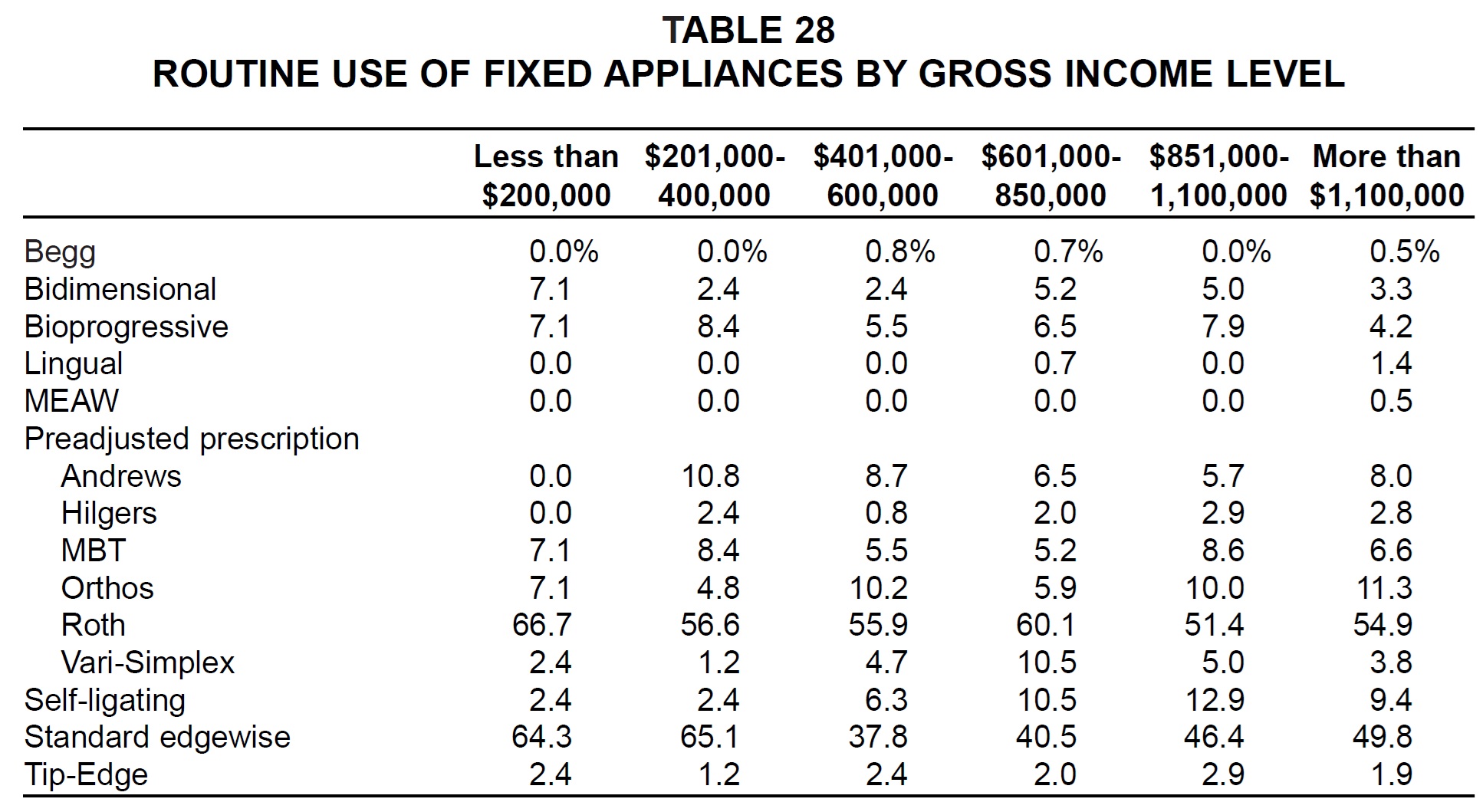
Generally speaking, respondents with lower gross income were more likely than others to use bidimensional, Roth-prescription, and standard edgewise appliances (Table 28). Larger practices were more likely to use lingual appliances, Hilgers and Orthos prescriptions, and self-ligating systems.
Brackets
The newest practices reported the highest percentages of ceramic, gold, and combination brackets, and were the most likely to use .022"slots (Table 29).
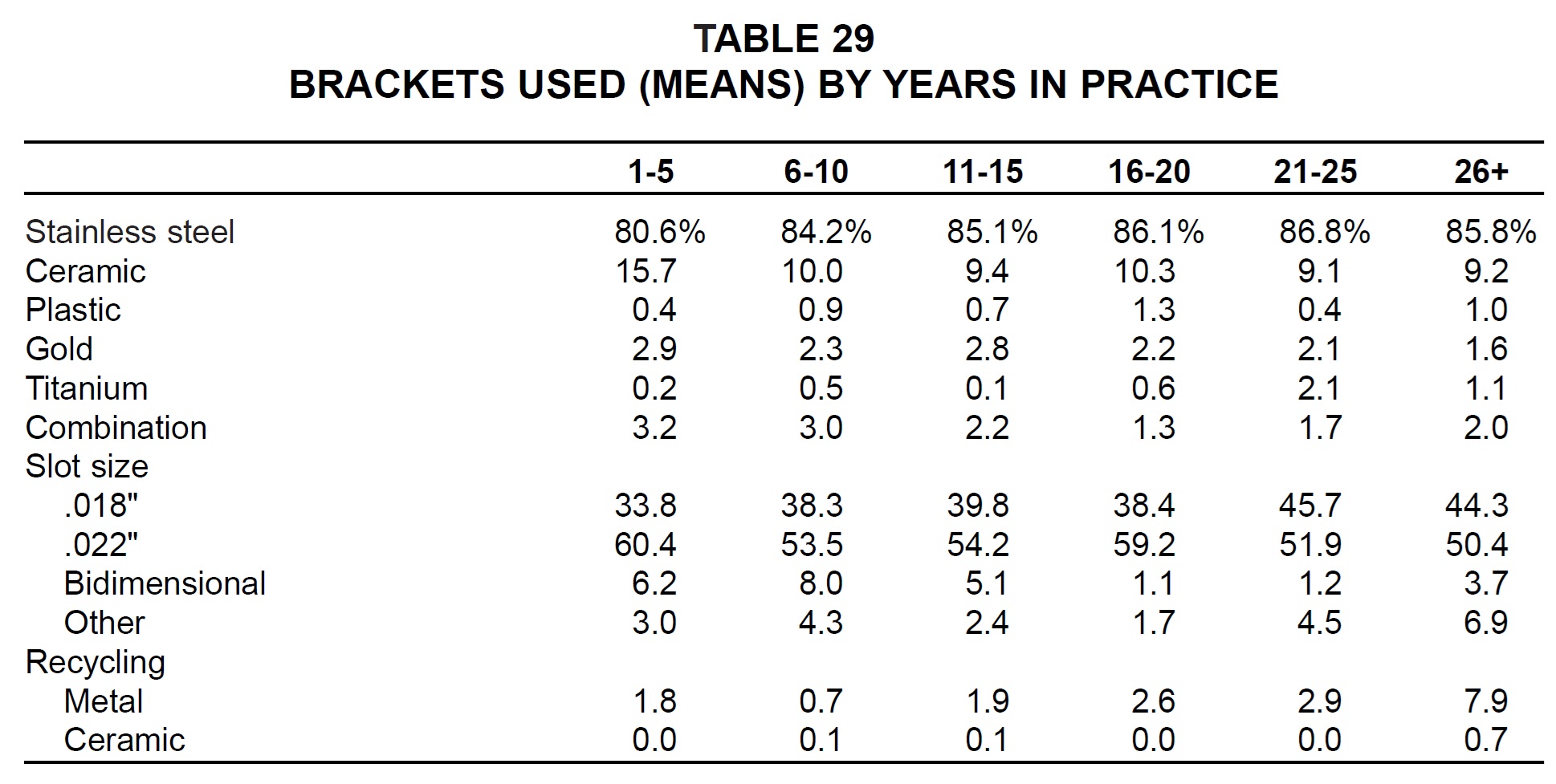
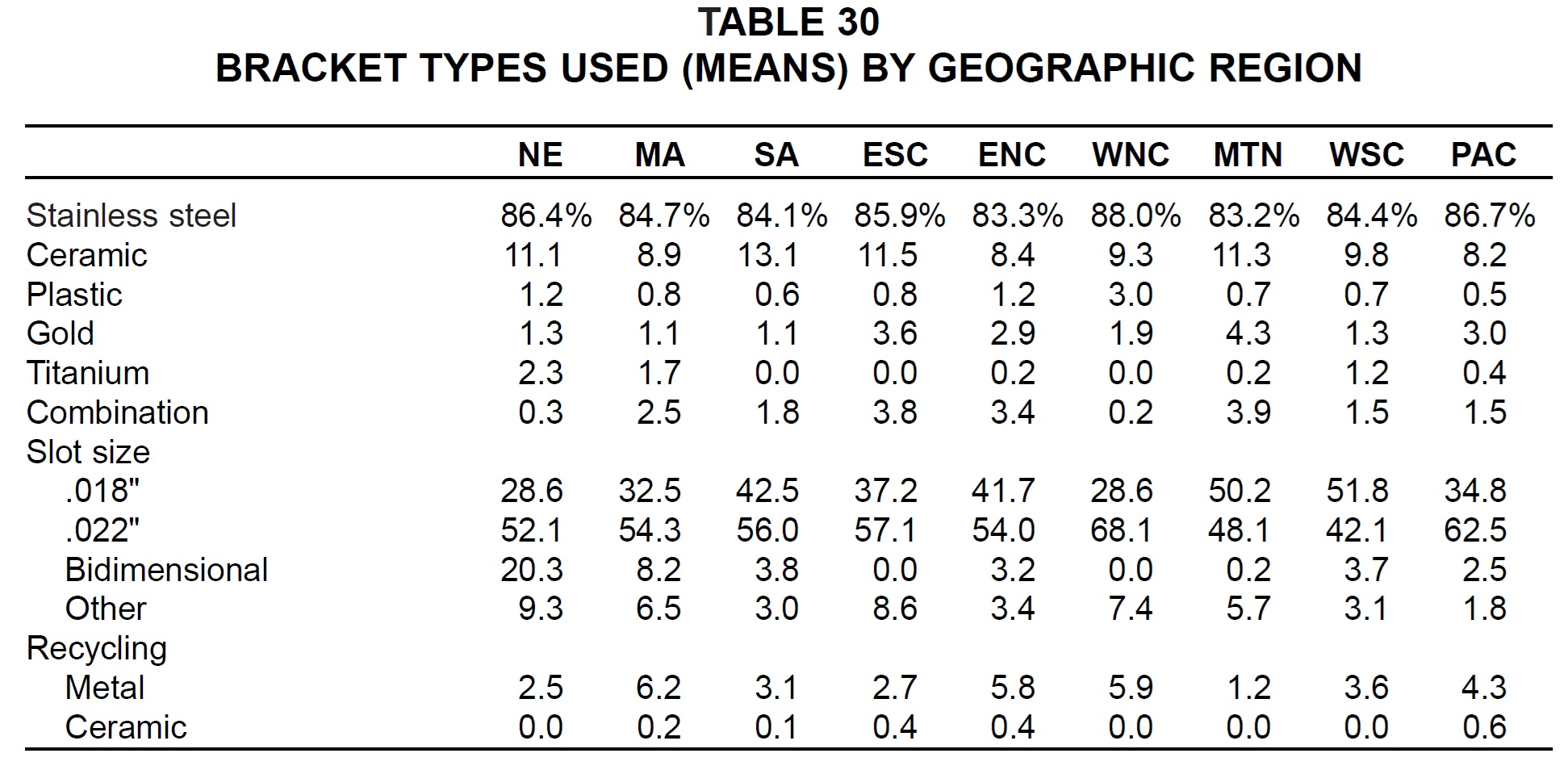
Older practices used more stainless steel and .018" brackets and did more recycling. Metal and plastic brackets were most popular in the West North Central area; ceramic brackets in the South Atlantic region; gold and combination brackets in the Mountain states; and titanium brackets in New England (Table 30). The .018" slot was used most in the West South Central and Mountain regions, the .022" slot in the West North Central and Pacific regions. The most recycling appeared to be done by Middle Atlantic, West North Central, and East North Central orthodontists, and the least by Mountain practitioners.
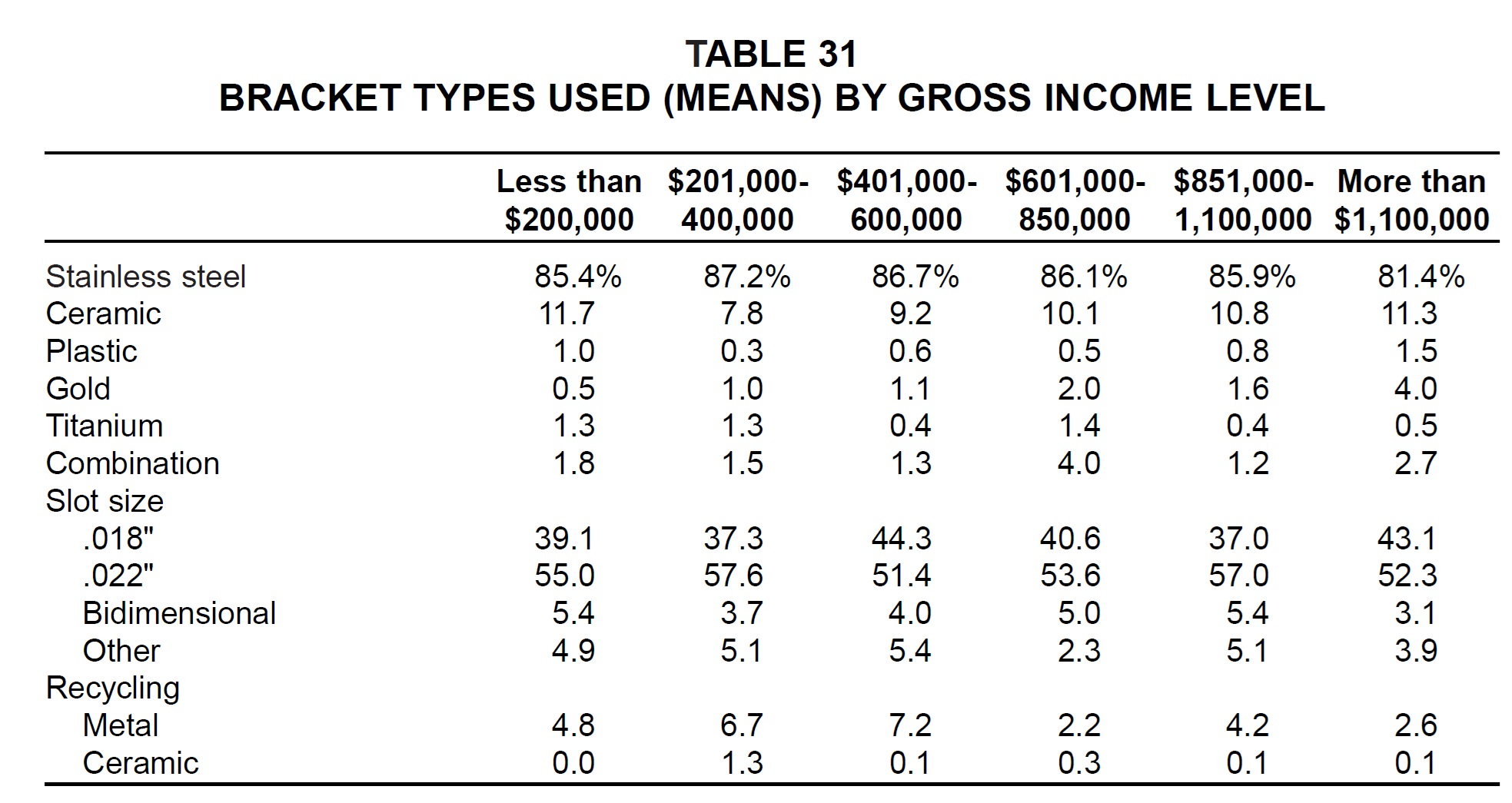
Middle-income practices tended to use more stainless steel brackets and fewer ceramic brackets than other respondents did, and they also recycled more of their metal brackets (Table 31). The highest-income practices used the most plastic and gold brackets.
Adhesives
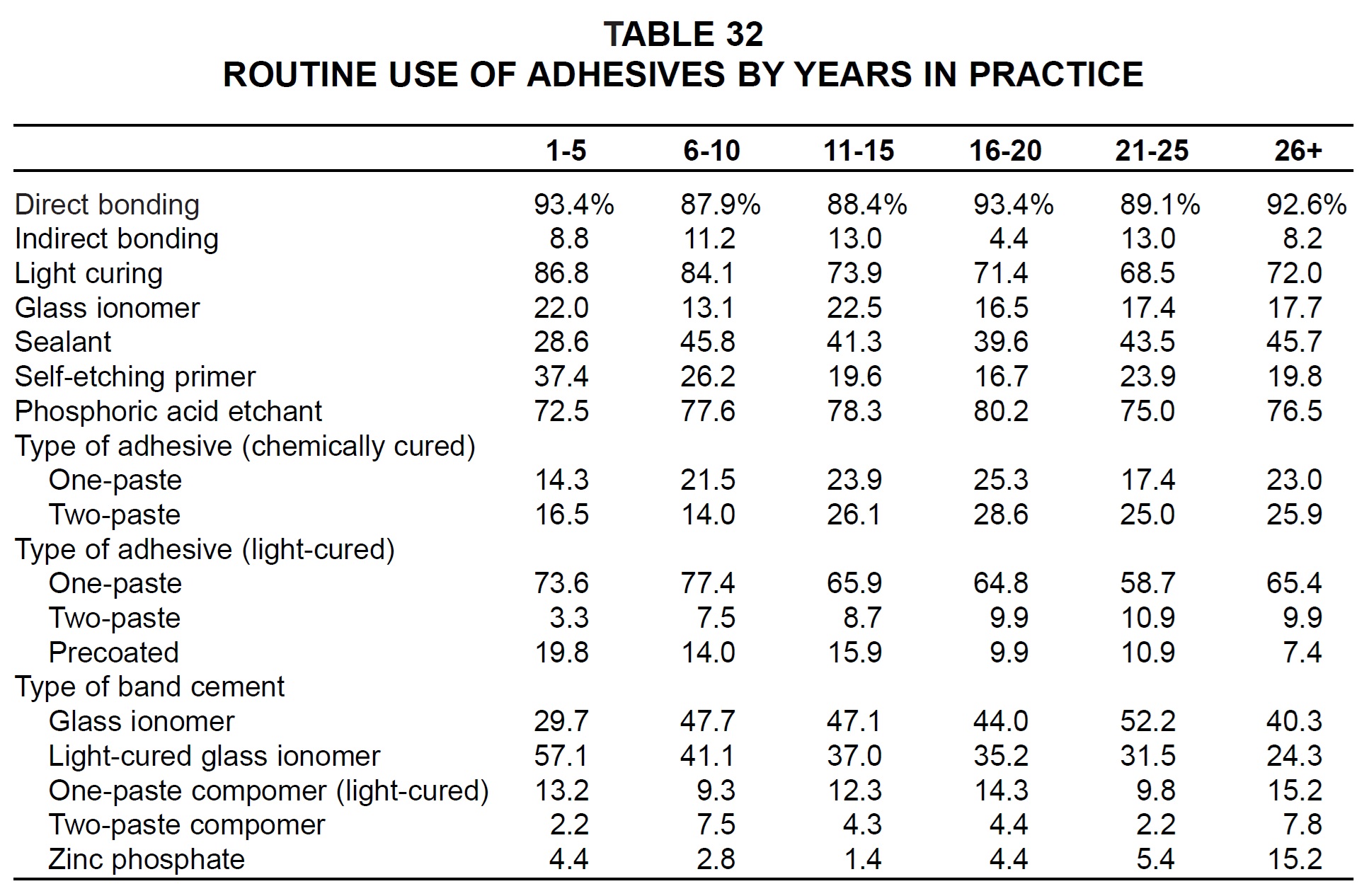
Light-cured adhesives, self-etching primers, and precoated brackets were used most routinely by the newest practices (Table 32). Among band cements, compomers and zinc phosphates were used most routinely by the oldest practices.
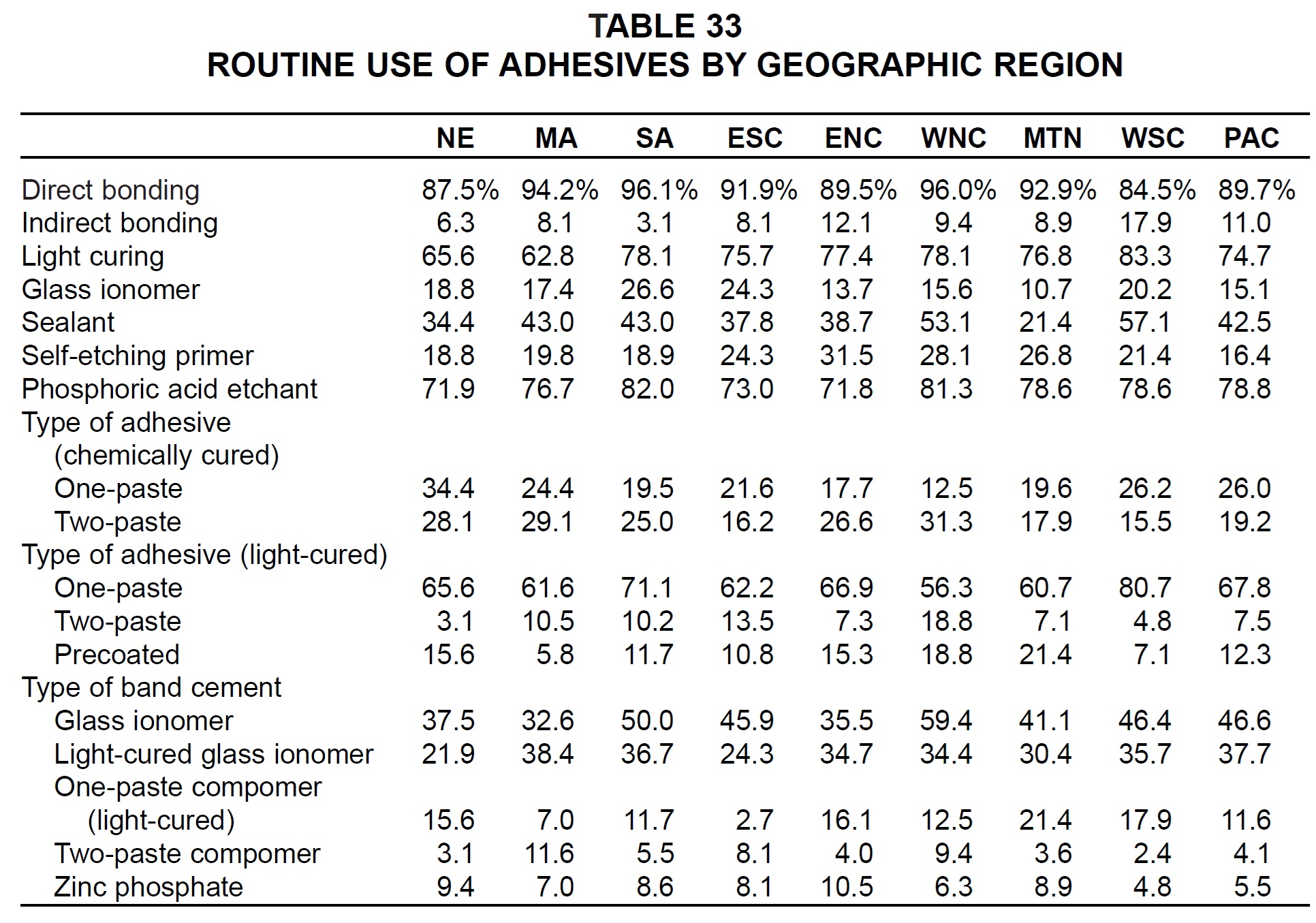
West South Central orthodontists were the most routine users of indirect bonding, light curing, and sealants (Table 33). Glass ionomer bonding adhesives were used most in the South Atlantic region, and light-cured glass ionomer cements in the Middle Atlantic States. Self-etching primers were most popular in the East North Central region, and precoated brackets and glass ionomer cements in the West North Central region.
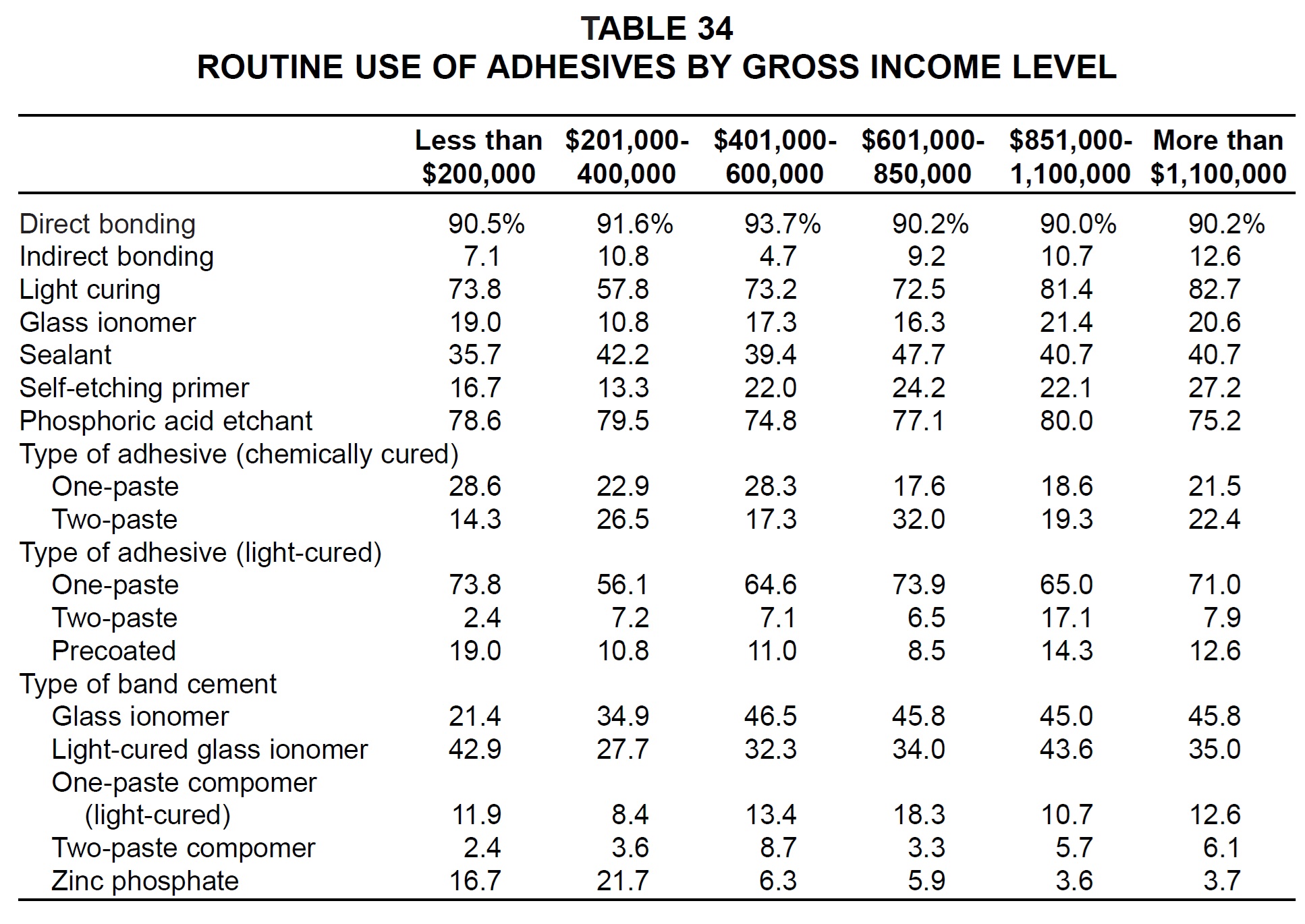
Practices with the highest gross incomes were the most likely to use indirect bonding, light curing, and self-etching primers (Table 34). Precoated brackets were used most by low-income practices, but adhesive usage in general did not seem to correlate with income level.
-
 DR. KEIM
DR. KEIM -
 DR. GOTTLIEB
DR. GOTTLIEB -
 DR. NELSON
DR. NELSON -
 MR. VOGELS
MR. VOGELS
Dr. Keim is Editor, Dr. Gottlieb is Senior Editor, and Mr. Vogels is Managing Editor of the Journal of Clinical Orthodontics, 1828 Pearl St., Boulder, CO 80302. Mr. Nelson is Director and Research Consultant, Nelson Associates, Nederland, CO.