Stepwise Overjet Reduction with a Modified Twin-Block Appliance
The twin-block appliance, described by Clark in 1982, is currently the most popular functional appliance in the United Kingdom. Recent evidence suggests that it may also be considered the most successful in the treatment of Class II, division 1 malocclusions.1
The optimal amount of mandibular advancement for construction of the twin block has yet to be established. Although the bite registration is generally taken with the incisors in an edge-to-edge position, several authors have suggested that a more gradual advancement of the bite may provide a greater orthopedic effect with less incisor tilting in Class II, division 1 cases.2-4 Smaller increments of mandibular advancement also reduce tension in the craniomandibular musculature, thus improving patient comfort, speech, and compliance, and increasing the likelihood of correct appliance position being maintained during sleep.
Most functional appliances can only be reactivated by laboratory reconstruction or adjustments, or by time-consuming chairside additions of acrylic, with the accompanying risk of loose monomer in the intraoral cavity. A modified twin-block appliance allows controlled, stepwise bite advancements to be carried out easily at the chair.5 Advancement screws are incorporated in the maxillary appliance blocks and activated by the insertion of cylindrical acetal resin spacers of various thicknesses.
Similar articles from the archive:
Bite reactivations of as much as 7mm can be readily achieved using the standard 12mm advancement screws. For greater activations, the longer 16mm or 20mm screws may be required. We have used this system for as much as 12mm of stepwise advancement.
Case Report
A 12-year-old female presented with a severe overjet and crowding (Fig. 1). Clinical examination showed mandibular retrusion and a dolichofacial pattern with incompetent lip morphology. Mandibular protrusive and lateral excursive movements were limited.
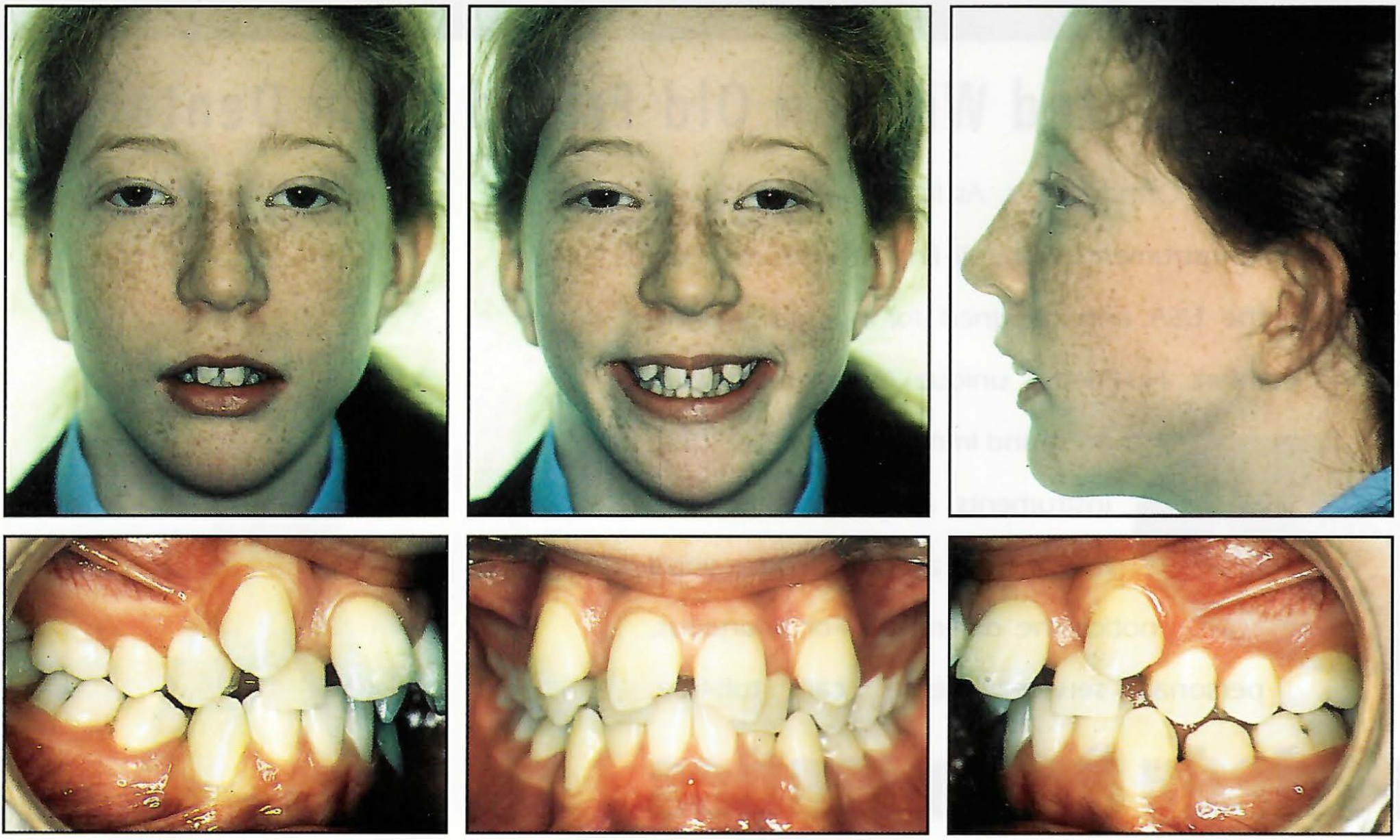
Fig. 1 12-year-old female patient before treatment.
The overjet was 12mm; the overbite was excessive, but incomplete. The buccal segments were slightly Class II on both sides. The maxillary arch showed severe crowding, with the canines buccally positioned and the lateral incisors palatally inclined. The mandibular arch had minimal crowding and showed previous loss of the first bicuspids. Cephalometric analysis confirmed a marked Class II dental relationship with mandibular retrusion and an excessive maxillomandibular plane angle (Fig. 2).
The treatment plan was as follows:
- Twin-block appliance with stepwise mandibular advancement to correct the overjet.
- Extraction of both maxillary first premolars.
- Placement of fixed appliances to align both arches.
Because of the patient's restricted mandibular protrusive movement, the appliance was constructed with a minimal bite advancement of 3mm (Fig. 3A). Reactivations were made by adding bilateral spacers of 3mm, 3mm, and 2mm to the maxillary appliance at six-to-eight-week intervals, until the overjet was reduced to zero (Fig. 3B). The longer, 16mm advancement screws were required for the final activation.
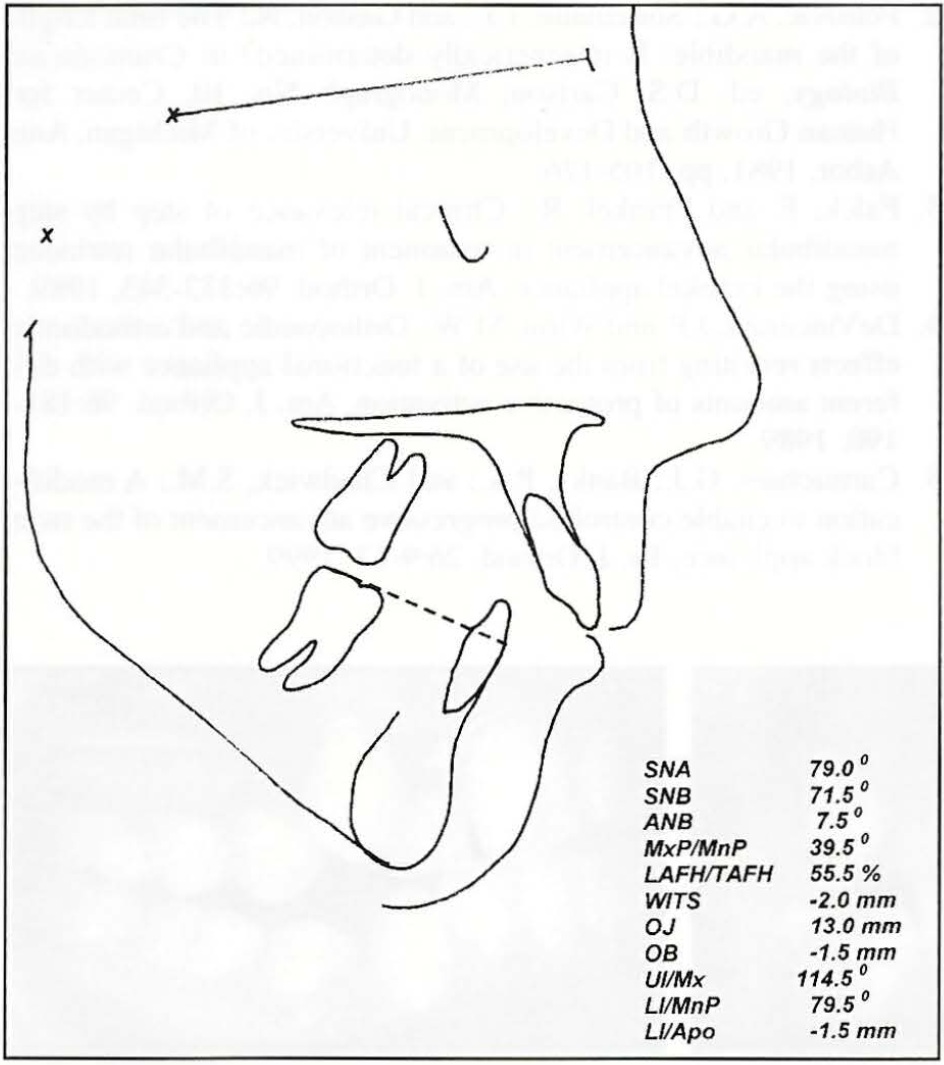
Fig. 2 Cephalometric tracing before treatment.
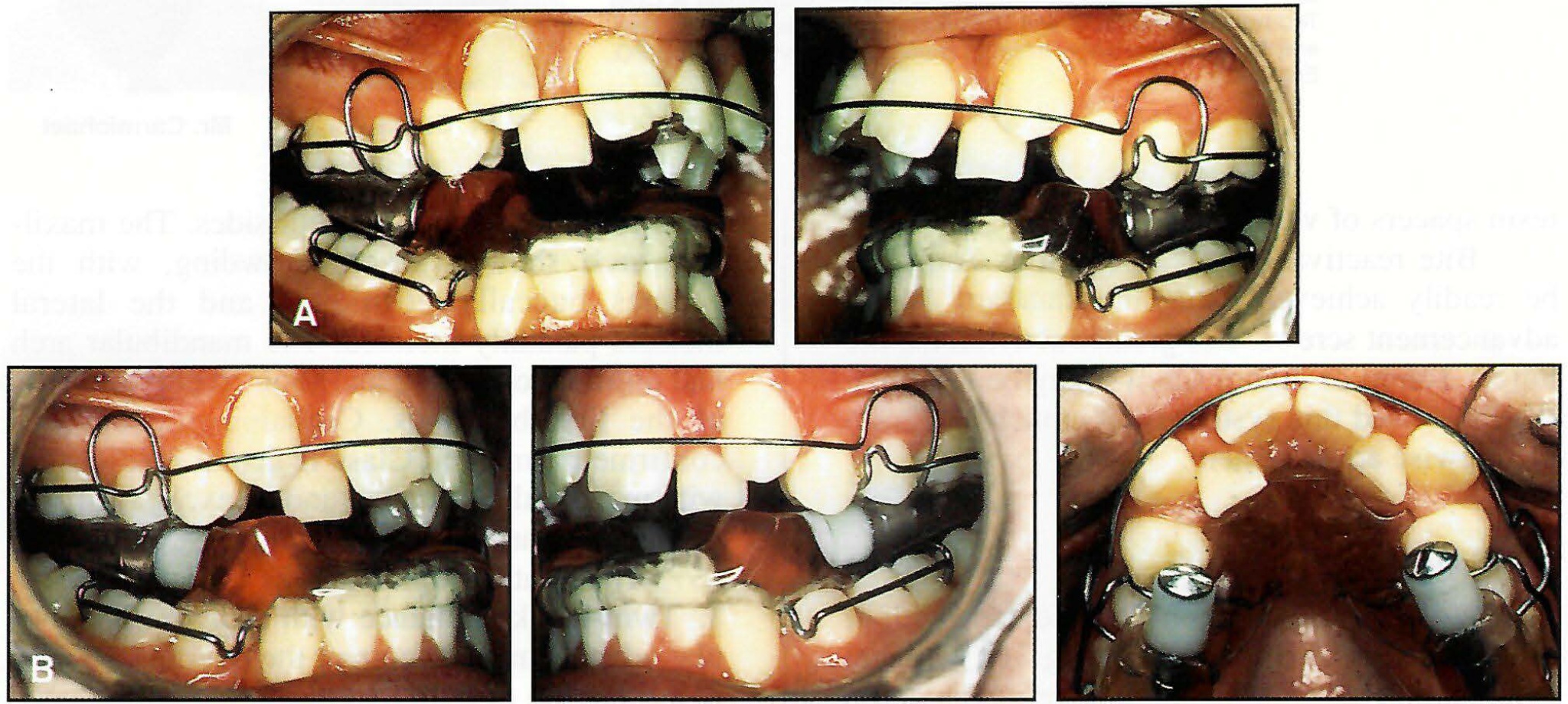
Fig. 3 A. Twin block with initial bite advancement of 3mm. B. After seven months of treatment, with further bite advancements made by adding spacers of 3mm, 3mm, and 2mm bilaterally.
The active twin-block appliance phase lasted seven months (Fig. 4).

Fig. 4 After seven months of twin-block therapy.
Full-time wear was continued for two more months, during which the maxillary first bicuspids were extracted. Preadjusted Roth .022" appliances were then placed. Fixed appliances were removed after 17 months, for a total active treatment time of 24 months (Fig. 5). Upper Hawley and lower fixed multistranded retainers were then delivered.
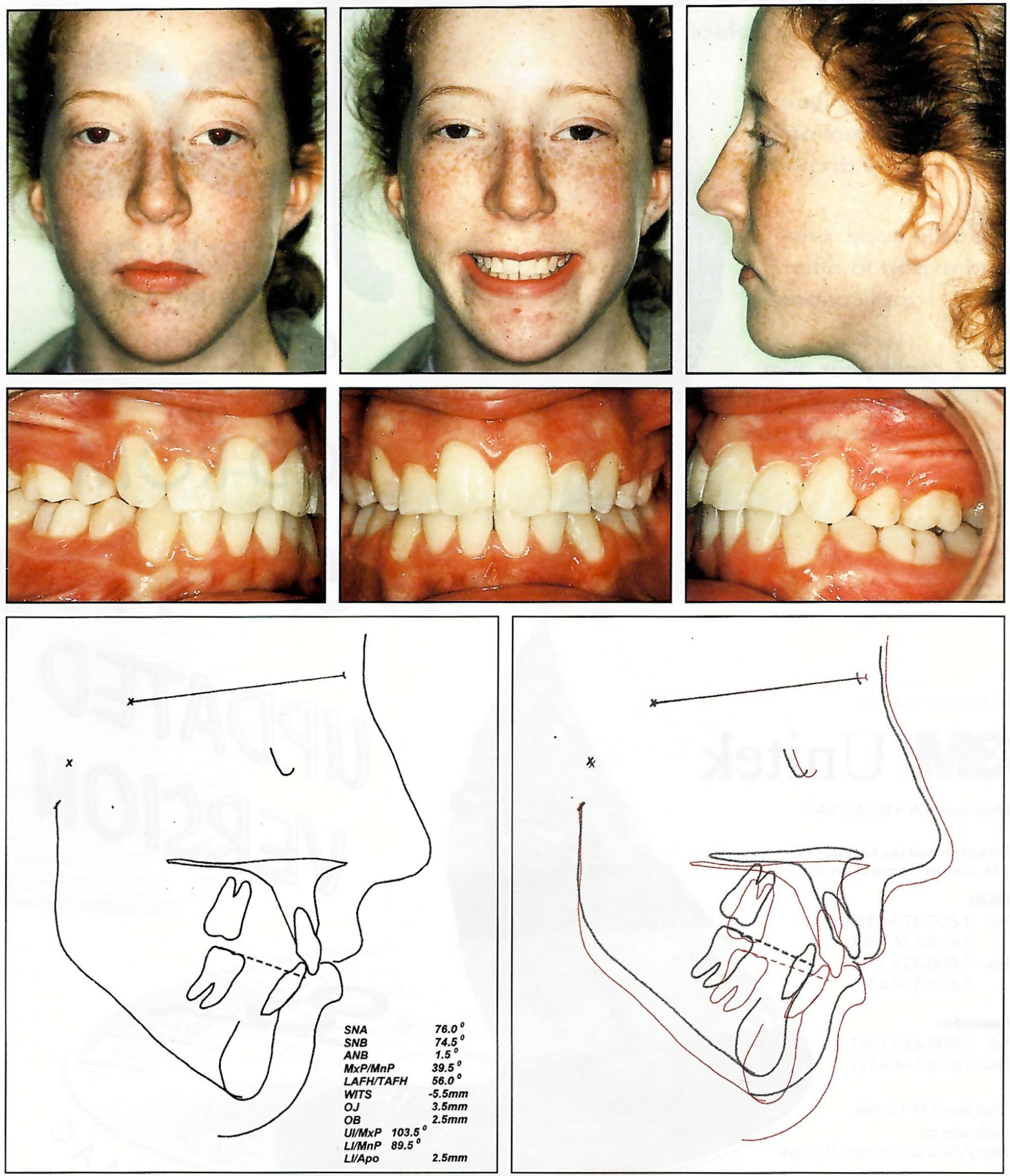
Fig. 5 After 17 months of fixed appliance therapy.
Discussion
A number of prospective twin-block patients are unable to posture into an edge-to-edge position for the construction bite. The patient with a dolichofacial pattern shown here could achieve only 3mm of bite advancement, but required 12mm of overjet reduction. Modification of the twin block allowed chairside reactivations with minimal inconvenience to staff and patient. Conventional twin-block appliances would have required several reactivations by chairside addition of acrylic or by laboratory reconstruction.
A fully adjustable functional appliance has definite advantages in the treatment of patients with severe overjets or limited ability to posture the mandible forward. Commercial manufacture is currently being investigated, and it is hoped that the system will become widely available in the near future.
REFERENCES
- 1. Chadwick, S.M.; Banks, P.A.; and Wright, J.L.: The use of myofunctional appliances in the UK: A survey of British orthodontists, Dent. Update 25:302-308, 1998.
- 2. Petrovic, A.G.; Stutzmann, J.J.; and Gasson, N.: The final length of the mandible: Is it genetically determined? in Craniofacial Biology, ed. D.S. Carlson, Monograph No. 10, Center for Human Growth and Development, University of Michigan, Ann Arbor, 1981, pp. 105-126.
- 3. Falck, F. and Fränkel, R.: Clinical relevance of step by step mandibular advancement in treatment of mandibular retrusion using the Fränkel appliance, Am. J. Orthod. 96:333-343, 1989.
- 4. DeVincenzo, J.P. and Winn, M.W.: Orthopaedic and orthodontic effects resulting from the use of a functional appliance with different amounts of protrusive activation, Am. J. Orthod. 96:181-190, 1989.
- 5. Carmichael, G.J.; Banks, P.A.; and Chadwick, S.M.: A modification to enable controlled progressive advancement of the twin block appliance, Br. J. Orthod. 26:9-13, 1999.
-
 DR. BANKS
DR. BANKS -
 GAVIN CARMICHAEL, LOTA, MIMPT
GAVIN CARMICHAEL, LOTA, MIMPT
Mr. Carmichael is Chief Technician, Maxillofacial and Orthodontic Department, Burnley General Hospital, Casterton Avenue, Burnley, Lancashire BB10 2PQ, England.