JCO Interviews Dr. Lennart Wieslander on Dentofacial Orthopedics: Headgear-Herbst Treatment in the Mixed Dentition
JCO has asked Dr. Bjorn Zachrisson, a member of the JCO Contributing Editors Board and Chairman of the Orthodontic Department at the University of Oslo, Norway, to interview some leading European orthodontists. This interview is the first in the series.
Dr. Wieslander is Professor and Chairman, Orthodontic Department, University of Basel, Switzerland.
DR. ZACHRISSON Lennart, has the orthopedic effect of treatment always been an important consideration?
DR. WIESLANDER Dr. Angle believed in stimulation of growth and in the possibility of achieving great changes in maxillary and mandibular morphology.1 However, after the introduction of cephalometric roentgenology, it was thought for many years that orthodontic treatment could generally only influence the dentoalveolar area of the maxilla and mandible.2DR. ZACHRISSON So when did we start to include the possibility of orthopedic change in treatment planning?
DR. WIESLANDER Ever since activator treatment was introduced in Europe, there has been reason to speculate on the possibility of influencing mandibular growth in Class II cases.3-15 In the U.S., it was in the late '50s that some investigations on headgear therapy in the mixed dentition demonstrated an effect on the base of the maxilla.16-18 In my own study at the University of Washington,19 which was published in 1963, we evaluated patients treated with Kloehn headgear. The findings indicated that changes in the development of the entire craniofacial complex seemed to be possible.
DR. ZACHRISSON That study of yours is one of the most commonly cited papers in the orthodontic literature. Could you briefly outline what you were able to show?
DR. WIESLANDER In Figure 1 you can see a schematic picture of a group of Class II patients treated with the Kloehn type of headgear in the mixed dentition compared to a control group.The illustration is taken from our followup study published several years later.20 The mean changes can be described as follows:
The force applied to the maxilla in a distal direction produced a change in growth pattern with a subsequent more posterior and slightly more inferior position of the maxilla. As a result of this, the ANB angle was reduced (3°) due to posterior movement of Point A and the PTM. There was a clockwise rotation of the pterygoid plates and probably also of the base of the sphenoid bone. The posterior movement of the pterygomaxillary fissure (2mm) appeared to be due to the combined effect of the rotation and a resorption on the anterior surface of the pterygoid plate. The maxillary molars were in a more posterior position (5mm) in the treated group as a result of a change in direction of growth of the maxilla (2mm) in combination with distal tooth movement within the dentoalveolar area (3mm). The change in position of the maxillary molars produced a clockwise rotation of the mandible, with an increase in the mandibular plane angle (1.5º).
DR. ZACHRISSON In Norway, we have used your headgear findings as treatment guidelines for several years. Do you think there is any major difference in orthopedic thinking between the U.S. and Europe today?
DR. WIESLANDER Several new treatment methods have been introduced in the past 10 years. Some appliances with a combination headgear and activator effect are accepted in both the U.S. and Europe for correction of skeletal deviations in the mixed dentition.21-23 The orthopedic effect of the Frankel appliance seems to have become accepted to a similar degree in America and Europe.24-27
DR. ZACHRISSON Lennart, are you of the opinion that it is possible to stimulate mandibular growth?
DR. WIESLANDER My feelings are that a change in the amount and direction of growth is clearly proven in animal experiments.28-40 Some studies on children treated with activator-type appliances showed a statistically significant increase in mandibular length. However, until a few years ago there was little evidence of the possibility of stimulating condylar growth in human beings.
DR. ZACHRISSON Why is there no proof of increased mandibular growth in some thorough activator studies?
DR. WIESLANDER Variation in appliance construction is certainly one factor. In a cephalometric study of patients treated with the conventional type of Andresen activator, Lennart Lagerstrom and I were not able to register any increase in mandibular length as compared to a control group.41 Other appliance designs may give a better response. In my opinion, the fact that most activators are used only at night is most important, because of the possibility that the occlusion may reverse the treatment effect during the day. That is one reason for the headgear-Herbst treatment that we use in severe Class II malocclusions in the early mixed dentition.
DR. ZACHRISSON Luder15 has recently indicated that the height of the construction bite is of great importance for determining the orthopedic response. Do you agree?
DR. WIESLANDER Yes, because he finds more change in the position of the mandible when he uses a construction bite that will keep the mandible in a more constant anterior position during the use of the appliance. However, we have not experimented with different heights of the construction bite in our Herbst cases.
DR. ZACHRISSON Your most recent work on the combined headgear-Herbst appliance has
produced some of the most strikingly favorable profile changes that I have seen in children with retrusive mandibles. I would like to go into some details of this approach. First, who was Herbst?
DR. WIESLANDER Emil Herbst was the first professor and chairman of an orthodontic department in Europe. He was born in Bremen, Germany, was a famous orthodontist, and was very active in his field in the beginning of this century. His clinical and scientific experience is well documented in his books.42 Among his appliances is the Herbst-Schanier, which is the telescoping arm system that Herbst developed to protrude the lower jaw in Class II cases.
DR. ZACHRISSON It has been a long time since it was introduced. Why has his appliance not been used more frequently?
DR. WIESLANDER The introduction of intermaxillary elastics in the U.S. and functional jaw orthopedics in Europe provided orthodontists with other means for treatment of Class II malocclusions. The Herbst approach was simply forgotten. The honor of having reintroduced it goes to Hans Pancherz of Malmo, Sweden. He treated a group of Class II malocclusions in the early permanent dentition, and documented the effect of that treatment in several publications around 1980.43-46 More recent contributions have been made by Langford,47,48 Howe and McNamara,49,51and Clements and Jacobson.50 Those authors have also discussed some clinical aspects of using this appliance.
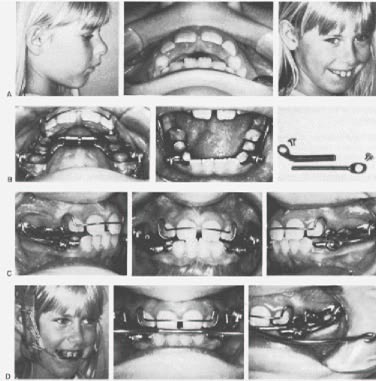
DR. ZACHRISSON Could you describe your treatment procedure with the headgear-Herbst appliance?
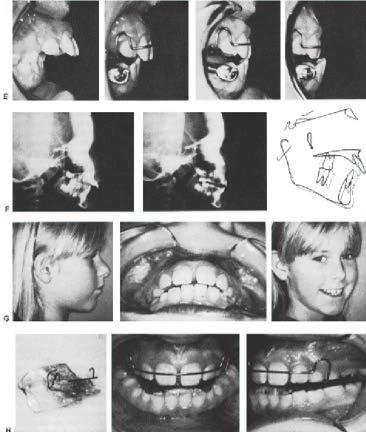
DR. WIESLANDER We like to treat severe Class II malocclusions in the early mixed dentition. Our approach is shown in detail in Figure 2. Upper and lower splints are cast in Vitallium (Fig. 2B). We have also tried plastic splints that are less expensive. The splints are bonded to the permanent first molars and to the deciduous molars and cuspids. The mandible is jumped to a normal Class I molar relationship with the Herbst telescoping arms at the start of treatment (Fig. 2C). A headgear is worn against the upper splint at night (Fig. 2D).
The mandible is progressively jumped forward in small additional increments (Fig. 2E). By adding a piece of tubing on the telescoping arms on each side, one can jump the mandible to an end-to-end relationship after eight weeks. A second piece of tubing is added in another eight weeks to place the mandible in a slightly protrusive position. After six months of active treatment, the telescoping arms are removed, and the most retruded position of the mandible is tested. If the patient is still biting in a normal Class I molar relationship after one week, the case is retained with an activator for six to 12 months. The mandible is jumped forward to an end-to-end incisor relationship in the construction bite of the activator. At the end of the retention period, the activator is used every other night, then every third night, and finally once a week until good stability is achieved.
DR. ZACHRISSON Could you describe the changes you find after headgear-Herbst treatment in the mixed dentition, for comparison to your headgear findings in Figure 1?
DR. WIESLANDER In Figure 3 you see a schematic picture of the effect of active treatment in comparison to an untreated control group.52 The average change in the sagittal relationship of the
maxillary and mandibular incisors after active treatment was 7½ mm. This was the result of a 3mm posterior effect on the maxilla and a 4½ mm anterior effect on the mandible.
DR. ZACHRISSON How much of the change is orthopedic and how much is tooth movement?
DR. WIESLANDER We find a combination of tooth movement and orthopedic changes. In the maxilla, about half of the treatment effect was due to posterior change in maxillary basal bone. There was a significant effect on the mandible in all patients. This was mostly due to an anterior change in position of the base of the mandible, and slightly due to labial movement of the lower incisors. There was a significant increase in mandibular length. The distance from condylion to gnathion increased 2mm more in the treated group than in the control group. Furthermore, the angle between the ramus and the corpus increased about 2°, and the condyle was positioned 1½ mm more anteroinferiorly after treatment. In studying mandibular joint x-rays, we found the supra-condylar space had not increased. It is, therefore, tempting to speculate on an appositional growth process in the fossa, resulting in an anteroinferior transformation of the fossa following jumping of the mandible. Stimulation of mandibular growth, change in mandibular morphology, and an anterior transformation of the glenoid fossa would be some factors to explain the overall picture of anterior mandibular development.
DR. ZACHRISSON Which are the most favorable considerations in relation to treatment with the Herbst appliance?
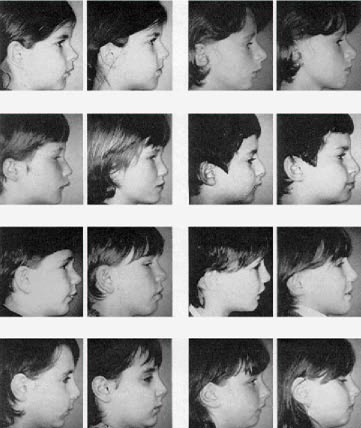
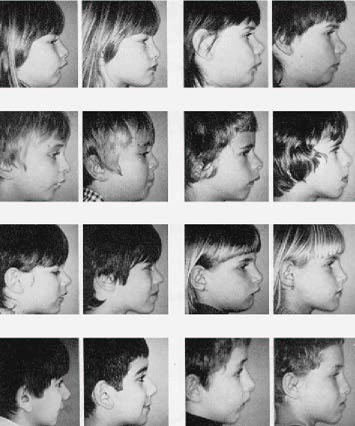
DR. WIESLANDER The fact that we do not need the usual patient cooperation and that we get a treatment effect in all cases are important considerations. Furthermore, we seem to be able to get an increased treatment effect because the appliance is worn 24 hours a day. Extraoral photographs taken before and after active treatment of every person in our group of patients are shown in Figure
DR. ZACHRISSON Lennart, I still think that the profile change in some of your photographs is indeed encouraging. I have not seen anything as impressive with any type of functional appliance in those difficult cases with markedly retrusive mandibles. If your results remain stable, my feeling is that your method is preferable to the removable types of functional appliances. But how do your findings compare with those of Pancherz?
DR. WIESLANDER There are differences in patient age and appliance design between our studies. Pancherz treated a group of patients in the permanent dentition, while our group was in the mixed dentition. Furthermore, the sagittal discrepancy pretreatment was more pronounced in our patients. The average ANB angle was 9.2°, as compared to 5.5° in the Pancherz group. In addition to the Herbst appliance that Pancherz used, we included a headgear. Our findings are similar, but it is possible to find some differences in treatment effect.
Pancherz found an average increase of 1.2° in SNB during treatment that appeared to be fairly stable during the post-treatment period of 12 months. We found an average increase in SNB of 2.9° during active treatment, but a relapse of about 1° ten months later. It is likely that the difference in
age between our groups is a factor to consider in relation to treatment response. However, we both found a 2mm increase in mandibular growth as measured from condylion to gnathion in the treated group. As far as the effect of treatment on the maxilla is concerned, Pancherz reported a reduction of 0.7° in SNA; however, that was not evident after the post-treatment period. In our group, the average reduction of SNA was 1°, and the effect of treatment on the base of the maxilla appeared stable during the post-treatment period. Perhaps the addition of headgear was the reason for the difference.
DR. ZACHRISSON Is the pubertal growth spurt important in treatment timing?
DR. WIESLANDER There is reason to believe that orthopedic treatment is more effective the younger the patient is. Sutural remodeling may be related to the maturity of the skeleton. Furthermore, research from Bjork, Woodside, and Ekstrom53 has shown that the growth potential in the early mixed dentition is as favorable or even better than in the pubertal age groups. It is possible that the slight difference in treatment effect between my group and Pancherz' group could be explained by the difference in age between the groups.
DR. ZACHRISSON So you would like to start treatment as early as possible in severe Class II cases?
DR. WIESLANDER Yes. Esthetics, possible trauma, and poor function are also factors that favor early treatment.
DR. ZACHRISSON What do you mean by early treatment? Which age group is most favorable for a headgear-Herbst appliance?
DR. WIESLANDER It is very important to start in the early mixed dentition. We need anchorage for the splints from the first molars and from the deciduous molars and cuspids. Six months of treatment around 8 years of age is a common approach. Later on, the resorption of the deciduous roots complicates appliance construction because of anchorage problems.
DR. ZACHRISSON Is it possible to transfer all the forces from the dentoalveolar area to basal bone?
DR. WIESLANDER No, we found that in spite of a splint covering the whole maxillary arch, posterior movement was evident in both the dentoalveolar area and in basal bone. The ratio was about 50:50, and it seems to be difficult to avoid an effect of treatment on the dentoalveolar area.
DR. ZACHRISSON I recently listened to presentations by Kokich and Shapiro from Seattle. In clinical experiments, they purposely ankylosed deciduous canines to obtain solid anchorage for improved orthopedic effects. The ankylosed teeth provided excellent anchorage. Would you consider such an approach for improving the orthopedic effect in headgear-Herbst treatment?
DR. WIESLANDER We have tried this approach in two cases we started recently. We ankylosed the upper deciduous canines by extraction, elimination of the periodontium, and replantation. Wehope to get more orthopedic effect on the maxilla, but we do not yet know if there are any side effects to be considered.
DR. ZACHRISSON Is the amount of force important in relation to the effect of treatment?
DR. WIESLANDER There is probably a correlation between the amount of force and the effect of treatment. One reason for the dramatic effect of treatment in animal experiments could be the heavy forces used. With the whole dental arch as anchorage in a patient, we can increase extraoral forces against the maxilla to 1,000-1,500 grams on each side.
DR. ZACHRISSON Do you recommend heavy forces in orthopedic treatment?
DR. WIESLANDER In our clinical experiments with the headgear-Herbst appliance, we thought in the beginning that it was important to use very heavy forces against the maxilla. However, we found that we got too much distal tooth movement and we have decreased the extraoral force to 500-1,000 grams on cases started more recently.
DR. ZACHRISSON How important is the headgear in this combination?
DR. WIESLANDER Jumping the mandible with the telescoping arms has a slight tipping effect on the maxillary splint. By using a highpull headgear with short outer arms, we feel that the tipping tendency is counteracted. So we use the headgear not only to try to increase the orthopedic effect, but also to try to improve the treatment result.
DR. ZACHRISSON That would be similar to the way Stockli and Teuscher use the headgear in the Zurich activator approach?
DR. WIESLANDER Yes, but I think we use forces of greater magnitude.
DR. ZACHRISSON When you described your treatment procedure, you mentioned a progressive jumping of the mandible to increase the effect on growth. How important is the reactivation of the appliance?
DR. WIESLANDER A muscular functional component seems to be an important influence on mandibular growth. The correlation between condyilar growth and lateral pterygoid muscle activity was a constant finding in the animal studies of McNamara32 and Petrovic and Stutzmann.34 It was proven that increased activity of this muscle was correlated with increased condylar growth. In later research, they have suggested that it might rather be the tension in the posterior part of the condylar capsule--caused by the activity of the lateral pterygoid muscle--that may be responsible for increased condylar growth. Important studies have shown that the activity of this muscle and the resultant tension of structures in the posterior part of the capsule decreased after a maximum level of activity six to eight weeks after the start of treatment.31,33 A constant reactivation may, therefore, be important in obtaining a maximum condylar growth response.
DR. ZACHRISSON At the recent meeting of the Pacific Coast Society of Orthodontists in San Francisco, Woodside reported that he achieved no statistically significant increase in mandibular length with the Herbst appliance in humans or monkeys. Is there a plausible explanation for the differences between Woodside's findings and yours?
DR. WIESLANDER There are some differences between Woodside's patients and the patients in our group. The cases we have treated are three to four years younger, which may be an important factor; I do not think that Woodside included a retention period in his experiment; and, furthermore, the progressive jumping is important. If I understood Woodside correctly, he used the Herbst approach on cases that had previously shown a poor reaction to conventional treatment. That may also explain the difference in treatment reaction between our patients. It is very good that Woodside is pointing at possible negative effects of Herbst treatment, because it is easy to become too enthusiastic. We must follow our cases several years out of retention to acquire more knowledge about the treatment effect.
DR. ZACHRISSON You mentioned that anterior transformation of the glenoid fossa could help explain the type of mandibular movement. However, you could also simply have displaced the condyle anteriorly out of the fossa, which I assume would create instability or a dual bite. Would you comment on this?
DR. WIESLANDER We found the condyle position was 1½ mm more anteroinferior as a result of treatment. However, we could not find a statistical difference in the supracondylar space before and after active treatment. This was interpreted as an anterior transformation of the glenoid fossa. The double contour found on several of the mandibular joint x-rays may also verify this finding. Lindahl and Hollender,54 in studying condylar fractures, have found that an anteroinferior adaptation and a double contour appear to a greater extent the younger the patient is.
DR. ZACHRISSON Are any pretreatment procedures necessary?
DR. WIESLANDER In cases with upper laterals in a palatal position, it is necessary to correct the incisors before the mandible can be jumped forward. However, it is important that this pretreatment procedure not last more than a couple of months, so that we do not lose time for the start of the headgear-Herbst treatment.
DR. ZACHRISSON Are there any complications during active treatment, such as caries or loosening?
DR. WIESLANDER There are usually few complications. In the beginning, when we were using bands, we had problems with breakage that we are not finding with splints. We find a slight gingival irritation upon removal of the splints; but it is reversible, and normal gingival conditions return shortly after active treatment. If patients open too wide, the telescoping arms may come out of the tubes, but the patients learn to push them back again.
DR. ZACHRISSON What are the important details to watch for at the end of active treatment?
DR. WIESLANDER In several cases, we find that the molars are not in contact after removal of the appliances. It is important to keep the vertical dimension intact until the molars have settled. Otherwise, the mandible is forced in a posterior direction because of the incisal guidance. Sometimes, in addition to the activator, we use a bite plate during the day for a few months until the molars have settled.
DR. ZACHRISSON Are there any contraindications to treatment due to morphology?
DR. WIESLANDER In most severe Class II cases, we find a combination of maxillary protrusion
and mandibular retrusion. In cases where the malocclusion is caused by pure maxillary protrusion, it may be unfavorable to jump the mandible forward.
DR. ZACHRISSON How about high angle cases?
DR. WIESLANDER If the mandibular plane angle does not increase when the mandible is protruded, high angle cases are not necessarily contraindicated.
DR. ZACHRISSON Is there no risk of future temporomandibular joint problems?
DR. WIESLANDER Woodside55 and Tonge, Heath, and Meikle38 have found some evidence of possible degenerative changes in the condylar area in animal experiments with the Herbst appliance in the permanent dentition. However, the findings may be reversible. We found no functional disturbances in our treated patients. It is possible that cases treated in the early mixed dentition have a better prognosis than cases with a later treatment start. In my opinion, treatment with the Herbst appliance is contraindicated on patients whose growth period is over.
DR. ZACHRISSON How about the long-term stability of the treatment results?
DR. WIESLANDER We found some relapse tendencies during the retention period. There was an average increase in overjet of about 2mm in the first group of patients treated. However, with somemodifications in the wear time of the activator during retention, as described in the treatment procedure, it appears possible to reduce these relapse tendencies. The cases must be followed several years out of retention before a more definite answer can be given.
DR. ZACHRISSON Is there reason to believe that conventional mixed dentition treatment is old-fashioned? Are you introducing a new treatment philosophy?
DR. WIESLANDER No, there are many roads to Rome. However, the usual attempt is to improve the relationship between the maxilla and mandible with appliances used over a long period of time, trying to gradually guide the direction and amount of growth in a favorable way. An early intensive orthopedic treatment--attempting to establish a normal occlusion directly, and then letting growth and adaptation adjust to this normal occlusion and function--may be an alternative. In the future, perhaps it may be possible to think of this new approach for cases in which orthopedic changes are important. It would avoid long treatment time in the mixed dentition, and a correction could then be followed by a passive period for several years until further dentoalveolar adjustments may become necessary in the permanent dentition.
DR. ZACHRISSON Lennart, on behalf of all JCO readers, I would like to thank you very much for the time and effort you have devoted to sharing your many years of experience in the field of dentofacial orthopedics.