JCO Interviews Dr. Homer W. Phillips on Bonding, Part 2
DR. GOTTLIEB How often do you experience bond failure?
DR. PHILLIPS Today it's pretty rare. We had a horrendous failure rate in the early years of bonding when techniques and materials weren't as good. For the last three years, we have had an exceptionally low failure rate, but one that any orthodontist could equal. It's simply a matter of following the proper procedures and, perhaps, knowing where not to bond.
DR. GOTTLIEB What are situations that shouldn't be bonded?
DR. PHILLIPS Any place where the bracket is going to be in traumatic occlusion. If we can't place a bracket so that it will be out of occlusion, either by contouring the bracket or by positioning it farther gingivally than usual, we simply don't put a bracket on until conditions will permit it to be out of occlusion.
DR. GOTTLIEB What do you do if you put a bracket on and then find that it is in traumatic occlusion?
DR. PHILLIPS The first thing we do after removing the transfer tray is to see if there is interference anywhere. If there is, we use a diamond wheel in a high speed air rotor and equilibrate the bracket or tube, but not the tooth, to get the bracket out of occlusion.
DR. GOTTLIEB Is it a problem in this regard that you do not have occluding models in the laboratory phase?
DR. PHILLIPS If it is a full bonding, we do have an opposing model and we do use the models to check for occlusal interferences. When we take a sectional impression, we look in the mouth with the teeth in occlusion to see if a bracket can be placed in the customary position, which is basically the middle third of the clinical crown. If it can be placed there without interfering with the occlusion, we send the impression to the lab with instructions to bond to such and such a tooth. If, on the other hand, we feel there is a real need to have a particular bracket on and we see that we can't put it I n the usual place, we will put a note on our prescription to our laboratory technician to place this bracket farther gingivally or toward the distal; and we always have the ability to grind away part of the bracket if it still interferes. If we have to grind away too much, we simply remove it and place a new one in a different position.
DR. GOTTLIEB Apart from traumatic occlusion, you feel that the bonding adhesives available today are quite adequate for all normal chewing requirements?
DR. PHILLIPS We have instances, due to the forces of occlusion, when a patient will come in with a bracket pad still firmly attached to the tooth, but with the bracket or tube gone. The weld has failed, rather than the attachment of the base to the tooth. With present adhesives and proper technique, we don't need more bond strength. We've got all we want.
DR. GOTTLIEB What do you consider to be the latest and best in bracket bases?
DR. PHILLIPS As adhesives have become better, the base has been able to be made smaller, since you don't need as much surface for adequate clinical bond strength. The base in widest use today is the solid foilbacked bracket with mesh attached to it, either welded or soldered. GAC's photoetched bases are an excellent surface, too. Smallness is helpful cosmetically, and in avoiding occlusal interferences. But, perhaps the most significant feature of small bases is their potential for more precise contouring to the enamel surface. The adhesives we use are more apt to contain voids, if they are applied in thick layers. The closer fitting the bracket pad, the less chance for voids in the adhesive that tend to cause it to fracture more easily. So, there is good reason to contour the bracket pad for close adaptation to the tooth surface.
Another point is that if you don't have a deep thickness of material at the edge of the pad, such as occurs using too flat a base on a convex tooth, there is going to be less area for plaque accumulation. Beyond that, if you are using Lee's Unique or Ormco's System I, that rely on a co-mingling of components-- an A,B,A sandwich-- you simply will not get as uniform a polymerization if there is a great thickness of material. So, contouring is important and very easy to achieve with the small present-day bases.
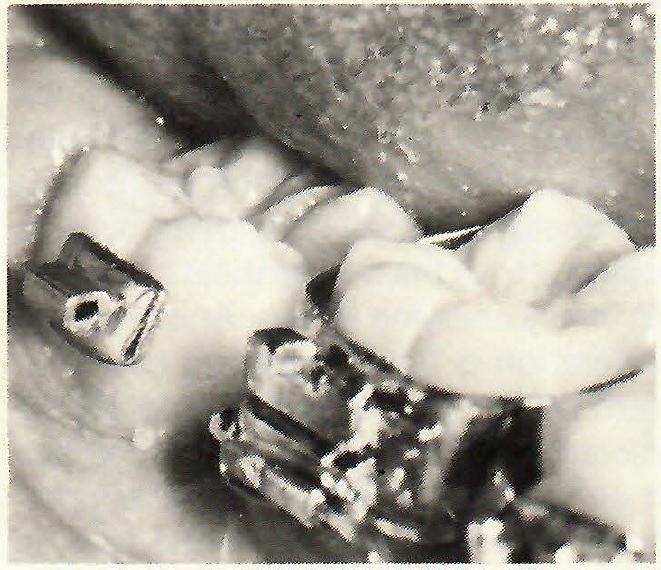
[show_img]462-jco-img-0.jpg[/show_img] Setup showing small bracket bases.DR. GOTTLIEB Do you feel that adaptation of bases is more precise using an indirect technique?
DR. PHILLIPS Yes, because in bonding indirectly, it is much easier to see if the base is well contoured before you put adhesive on it.
DR. GOTTLIEB Is there room for more improvement in bases?
DR. PHILLIPS Ideally, a base would offer as much retention for the adhesive per surface area as the enamel does. That is not the case right now, and the weak link in the bonding system is the interface between the adhesive and the bracket base. Yet, something has to be the weakest link. I don't think it is a special problem that orthodontists and the industry have to address particularly, because the bases we have now will definitely hold up to the usual orthodontic force, with the possible exception of headgear therapy.
DR. GOTTLIEB Do plastic brackets have a place in your practice?
DR. PHILLIPS Unless they are reinforced, in my view, plastic brackets are unacceptable for routine edgewise orthodontics. They are satisfactory for short term orthodontics or in situations where tooth movement is limited or where both patient and doctor agree that they don't mind changing brackets every three to five months due to wear and tear and discoloration. Unless there is a metal slot, such as the Tella-Tech bracket has, plastic brackets are just not satisfactory, in my view, because the bracket slot wears and distorts.
DR. GOTTLIEB What do you think of the cosmetic potential of plastic brackets?
DR. PHILLIPS That is their one reason for being, as far as I am concerned, and they are excellent for a few months.
DR. GOTTLIEB Do you find that patients favor them on occasion?
DR. PHILLIPS Many adult patients definitely favor them. When I start an adult patient, if they ask about "invisible" braces, we show them what they are and point out the drawbacks. If they insist on it, I will use plastic brackets, but I also tell them that we may have to change to metal brackets for part of their treatment. In fact, they may want us to do so, because when they discolor enough, many adults in my practice come to feel that they really don't look nice after all and they are happy to settle for metal brackets. I have very few patients in my practice with other than metal brackets, but this is not to say what we are doing now is what we will be doing a year or two from now.
DR. GOTTLIEB Do you ever use bands?
DR. PHILLIPS We use bands routinely on upper and lower first molars. We routinely bond second molars. Other than some transfer cases, I have no patients with bands other than on the four first molars. I would modify that to say that I do have a few patients with porcelain jacket crowns and I use bands for them. It is possible to bond to porcelain with such materials as Den-Mat, but this can present a problem at debonding, unless the jacket is to be replaced.
DR. GOTTLIEB Are the first molars banded because you use headgear?
DR. PHILLIPS That's correct as far as the upper molars are concerned. I have not found it practical to use bonded attachments with headgear, because you can't depend clinically on the patient being sufficiently careful. With everyday orthodontics, you are going to have attachments come off with headgear to bonded tubes.
DR. GOTTLIEB The leverage is great.
DR. PHILLIPS That's right. So, we see no reason to try. We think we are going to come out far ahead in time-saving with less breakage, if we use molar bands with headgear.
DR. GOTTLIEB Why do you use molar bands on the lower arch?
DR. PHILLIPS We use first molar bands in the lower arch simply because, for most of my patients, the first molar attachment is the last one in the arch during most of their treatment. The most distal attachment in the mouth is the one that is closest to the fulcrum of the temporomandibular joint and is going to receive the strongest occlusal forces. If anything is apt to come off, it's the one farthest back, due to heavy chewing forces. Another consideration is that if a patient comes in with any attachment loose other than a molar tube, we may elect not to replace it at that appointment. If it is a molar tube, I nearly always feel that it must be replaced immediately. I just can't live with anything more than a very minimal breakage rate. Later in treatment when we include second molars, we always bond them. I can't tell you how many years it has been since I have banded a second molar.
DR. GOTTLIEB In part is that because of the ease of access with bonds as opposed to bands?
DR. PHILLIPS Yes. It is so easy to bond a second molar, particularly with an indirect technique, that I really can't think of a good reason for doing it any other way. Precise positioning is very easy to achieve with a one-tooth template. You can put a tube on a tooth when perhaps only a third to a half of the buccal surface is available. In years past, we used to defer putting attachments on second molars because they had not erupted enough, but we just don't think about that any more. We take a sectional alginate impression and the next time we see the patient, we put on a tube or four tubes-- whatever the case happens to need-- without a special appointment.
DR. GOTTLIEB Is access to the template a problem in bonding second molars?
DR. PHILLIPS No. Looking at the template on the model tells me exactly what it should look like when I have it in the right place in the mouth. For convenience in reaching back to the second molar area, we simply stick a scaler into the silicone tray to facilitate placing it that far back in the mouth. Holding one finger on the tray, the scaler is removed, and we continue to hold the tray with the one finger until the adhesive has set, timing it with a stopwatch.
DR. GOTTLIEB How much eruption is enough to bond to, on a second molar for example?
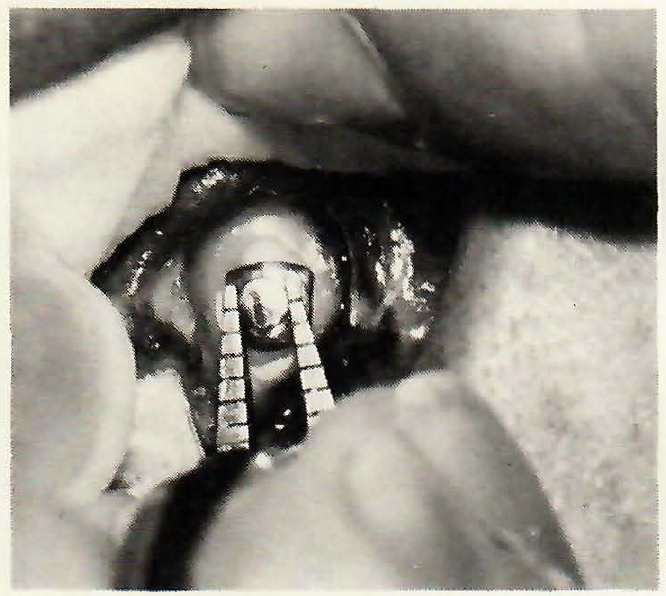
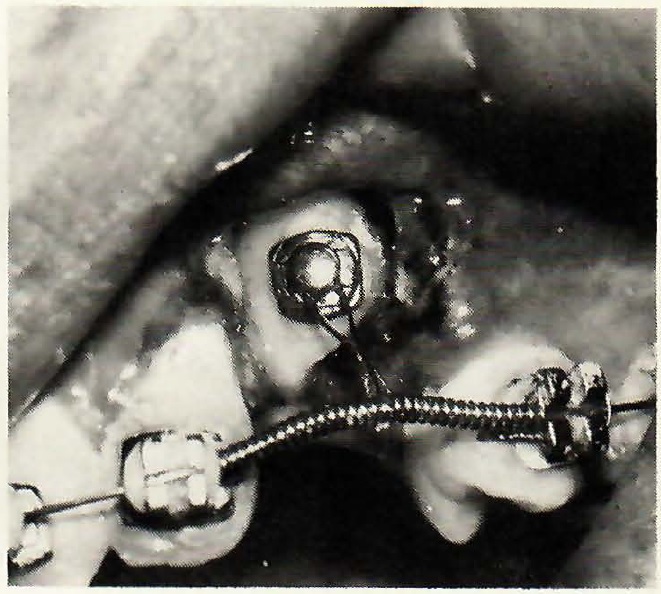
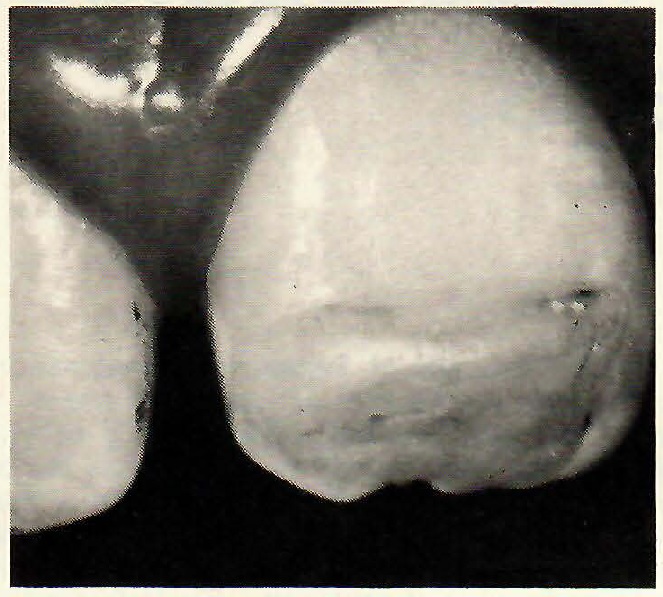
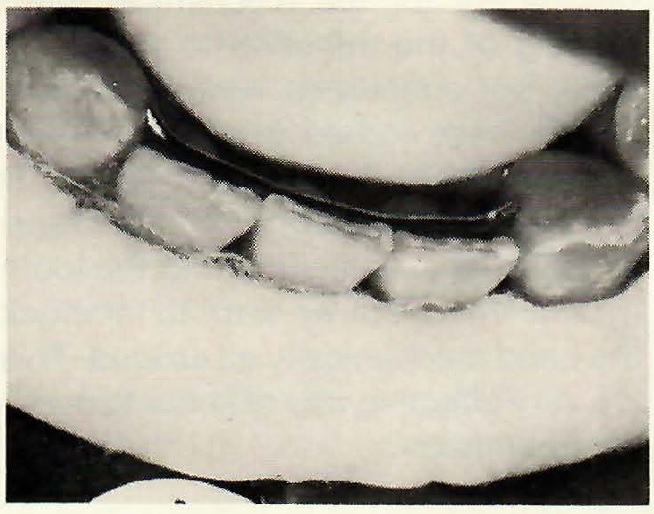
DR. PHILLIPS On some second molars there may not be much buccal surface available. I use an American Orthodontics tube that is only 2mm long on teeth that are not erupted enough to accommodate a standard buccal tube. This allows us to get the tooth into pretty good position very early in treatment. Incidentally, because we know that we are going to put attachments on virtually all second molars, we use only convertible tubes on the first molars, so that we can convert them to brackets, both upper and lower.
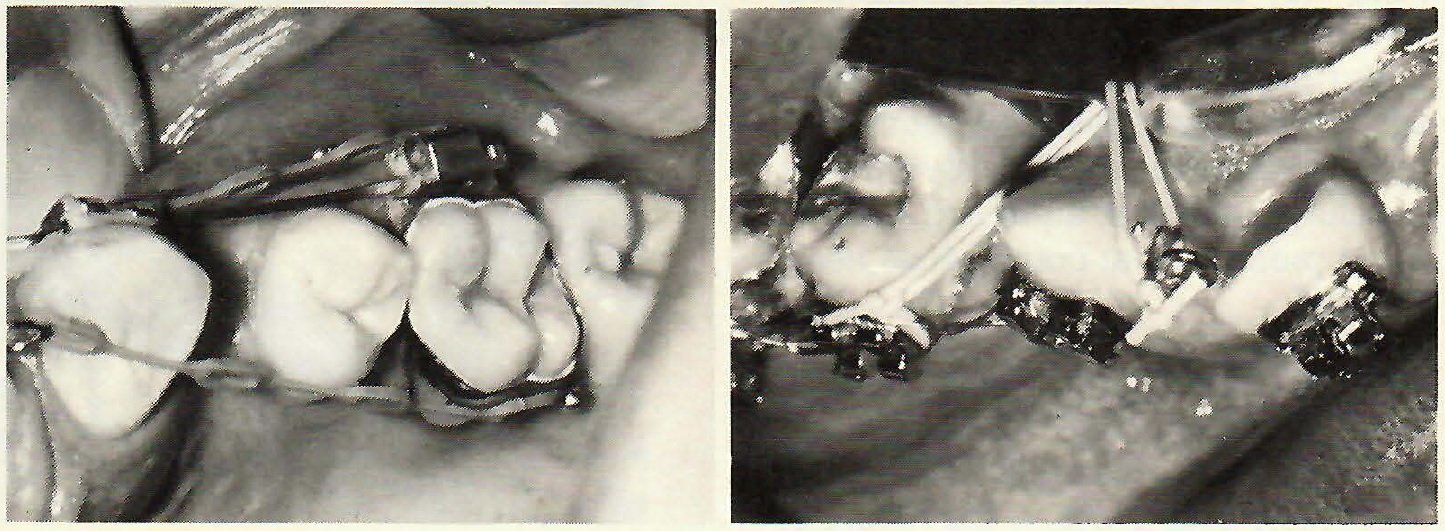
[show_img]462-jco-img-1.jpg[/show_img] Taking the impression. [show_img]462-jco-img-2.jpg[/show_img] The impression. [show_img]462-jco-img-4.jpg[/show_img] Tray in place. [show_img]462-jco-img-5.jpg[/show_img] Second molar attachment bonded.DR. GOTTLIEB Do you ever do any direct bonding?
DR. PHILLIPS We do some direct bonding. We bond all lingual attachments directly and we will occasionally -- maybe three times a month-- bond an incisor or cuspid bracket directly on a tooth that was not fully erupted, or is in such a position that we did not want to bond it initially, or if we are replacing a bonding failure.
DR. GOTTLIEB What decides you to go direct in those instances?
DR. PHILLIPS If the tooth is very easily accessible and not particularly malshaped or malpositioned, we'll bond directly. It is generally in a situation where we consider the precise positioning of the attachment to be the least critical part of the whole operation, such as with a lingual button or hook. In unusual places, such as the occlusal surface of an impacted tooth, we bond directly.
DR. GOTTLIEB Do you place labial and lingual attachments in the same tray at the same time?
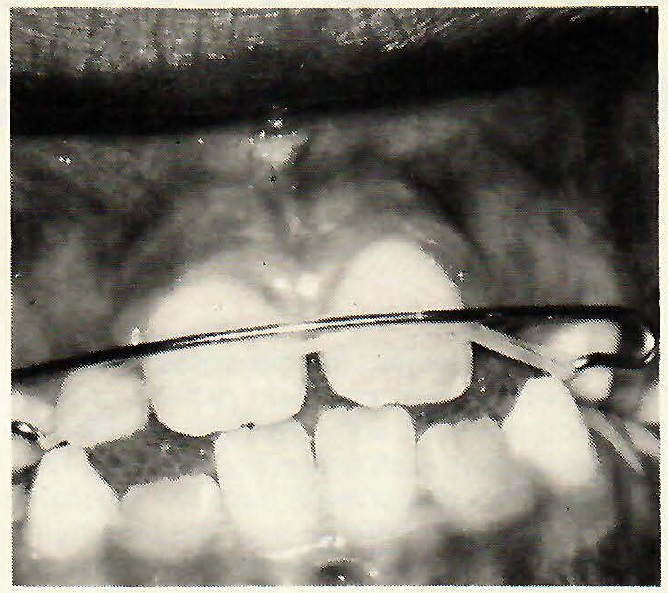
DR. PHILLIPS We do it occasionally, but not routinely. When we do it, we score the tray down the middle to make it even more flexible labiolingually to avoid smearing the adhesive. When it is smeared, we have to clean it off, and I'd just as soon not have to. We routinely bond lingual attachments directly.
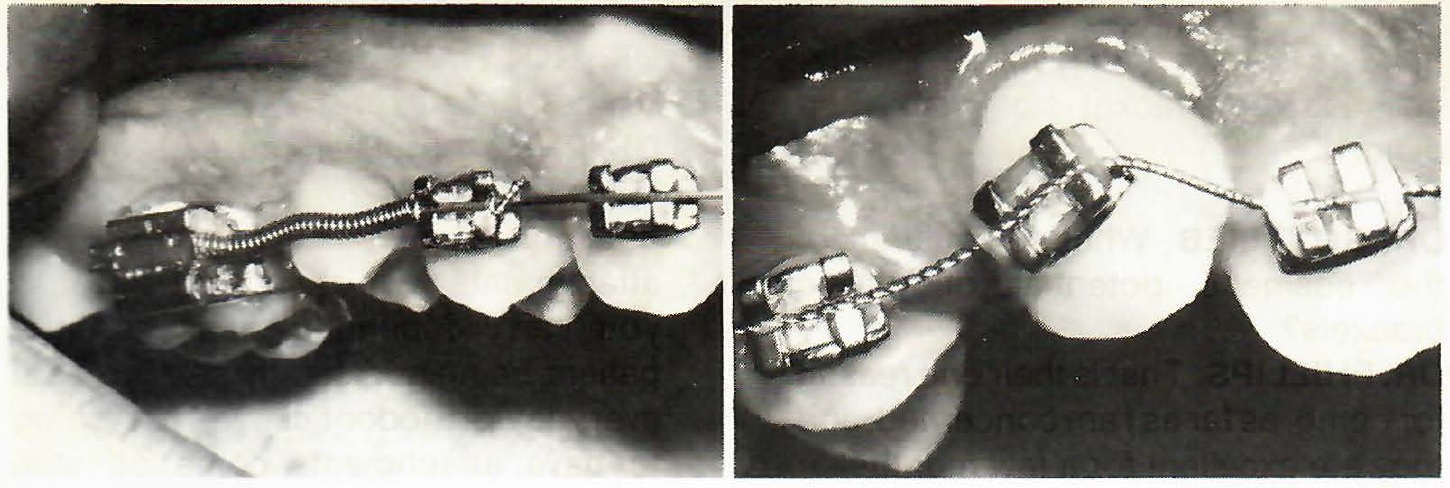
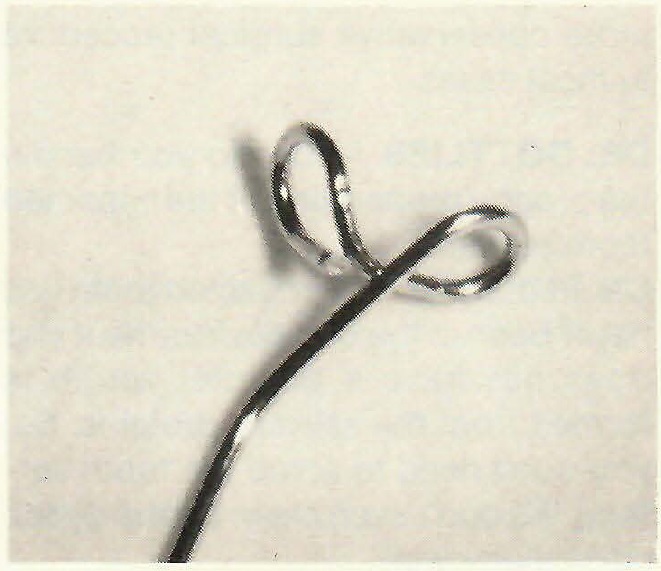
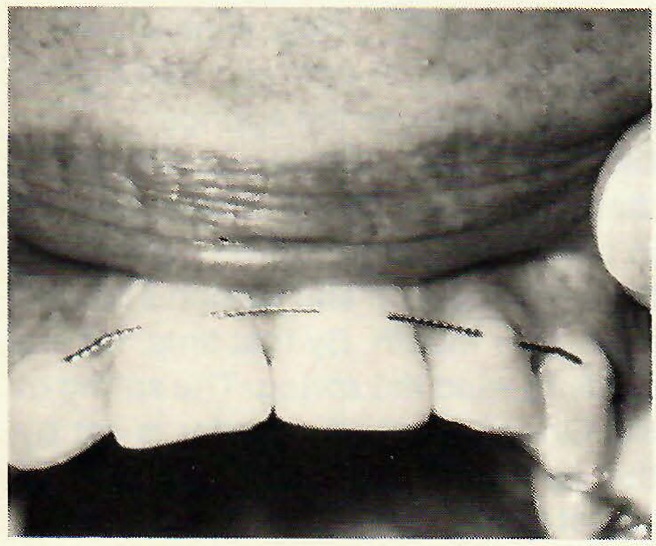
[show_img]462-jco-img-6.jpg[/show_img] Tray scored for bonding labially and lingually. [show_img]462-jco-img-7.jpg[/show_img] Figure-8 hook.DR. GOTTLIEB What kind of lingual attachments do you use?
DR. PHILLIPS Any place where we formerly placed a lingual button to attach an elastic thread or ligature wire, we now make a little figure-8 hook of .016 wire and bond that. The two loops of the figure-8 are at right angles to each other. If there is not room on the lingual of a rotated tooth to bond a button or hook, we place the hook on the mesial, rotate the tooth, remove the hook, and close the space. We do not hesitate to place the hook anywhere the occlusion will permit. We can form it in a minute or less and custom-fit it. The hook fits in places where a commercially made button would not fit or not fit well.
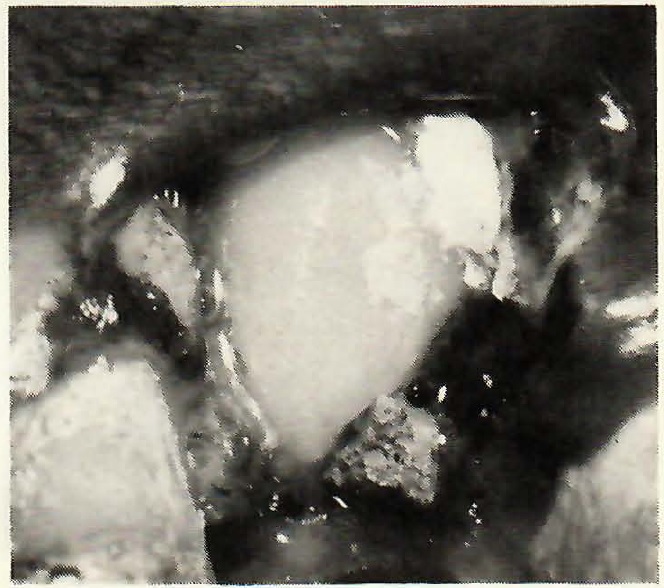
[show_img]462-jco-img-8.jpg[/show_img] Figure-8 hook in action.DR. GOTTLIEB Do you routinely bond to all impacted teeth?
DR. PHILLIPS Yes, and direct bonding has a strong application with impacted teeth. We routinely bond to impacted teeth that have been exposed. We have not ligated or pinned an impacted tooth for several years. Bonding allows a more conservative surgical procedure in most cases.
DR. GOTTLIEB How do you handle the prophy preparation of the impacted tooth surface?
DR. PHILLIPS The impacted tooth has never been in the oral environment and does not have a pellicle, which is formed from the salivary proteins. So, you don't need to scrub the tooth surface. We don't even clean off the debris particularly well.
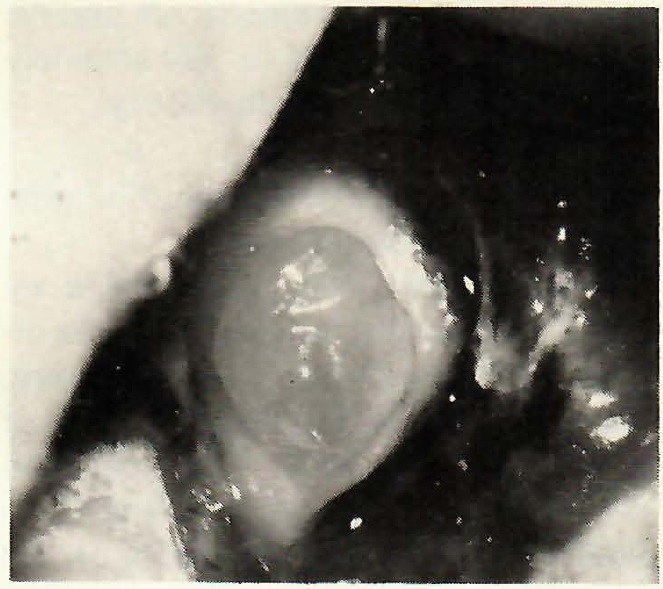
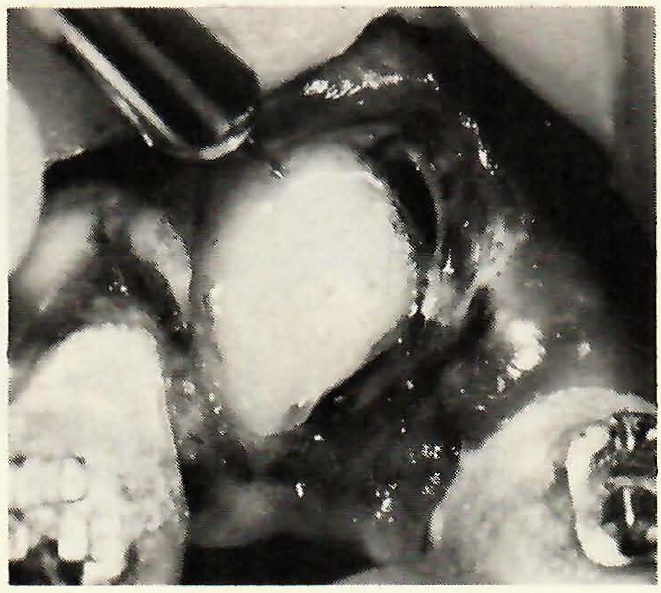
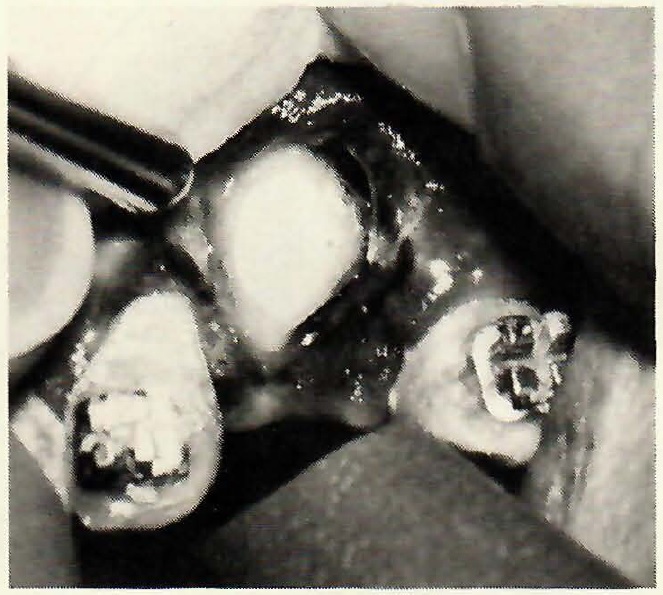
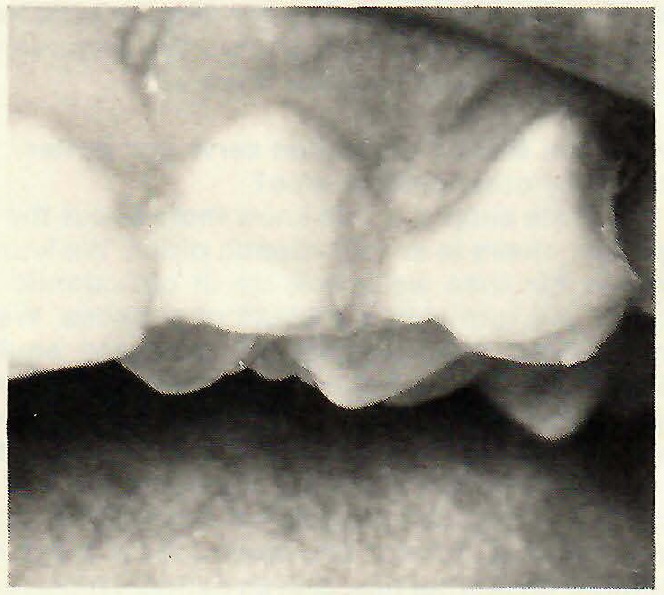
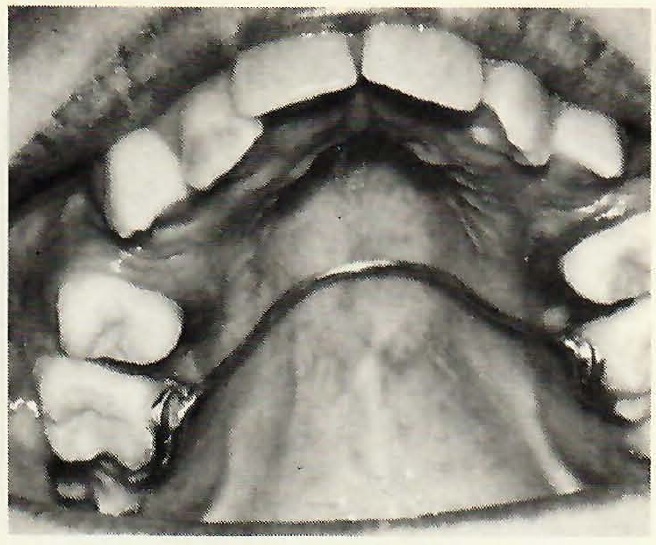
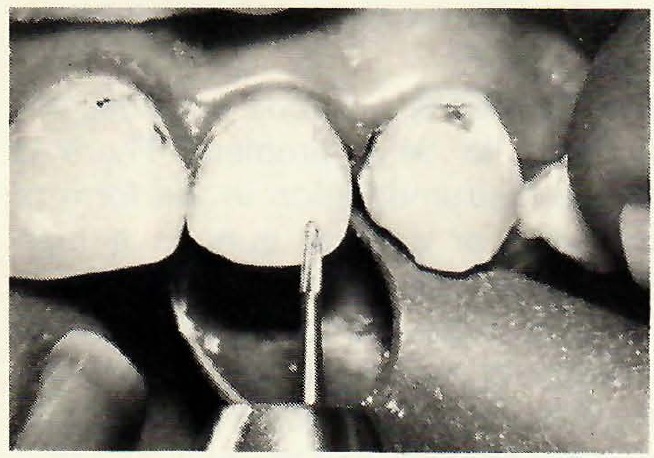
[show_img]462-jco-img-9.jpg[/show_img] Impacted tooth exposed. [show_img]462-jco-img-10.jpg[/show_img] Gel applied. [show_img]462-jco-img-11.jpg[/show_img] Gel rinsed off.DR. GOTTLIEB Could you describe the bonding technique you use for an impacted cuspid?
DR.PHILLIPS In the first place, I try to be present at the surgery, to see the location of the tooth and to see that tissue is removed to my satisfaction. I generally have the patient come to the office about a week after surgery, with the periodontal pack in place. I remove the pack, place the acid gel, wash it off, and go through our sealant and adhesive system procedures. The etching gel is much preferable to a liquid in this area, because these teeth are pretty well in a hole. The gel can be placed exactly where you want it on the tooth surface and not onto the soft tissue, particularly if you use a syringe to dispense the gel. We get such an excellent etch on these teeth, because they have not been exposed to the oral environment. Also, we don't worry about flash in such cases until later,when we have moved the tooth to a more accessible position. We are very careful during the air-drying step to avoid pressure that could cause hemorrhage.
DR. GOTTLIEB What other uses do you make of bonding?
DR. PHILLIPS I use it for retention of removable appliances. If the nature of the spring or clasp and the shape of the teeth would tend to dislodge a removable appliance, we build a bulge of adhesive on the tooth surface to create an undercut for the clasp or spring to make the appliance firm and comfortable for the patient. We use a similar device to position an elastic over a flared incisor and also to rotate teeth. We place a little adhesive on the tooth where we want a little extra pressure.
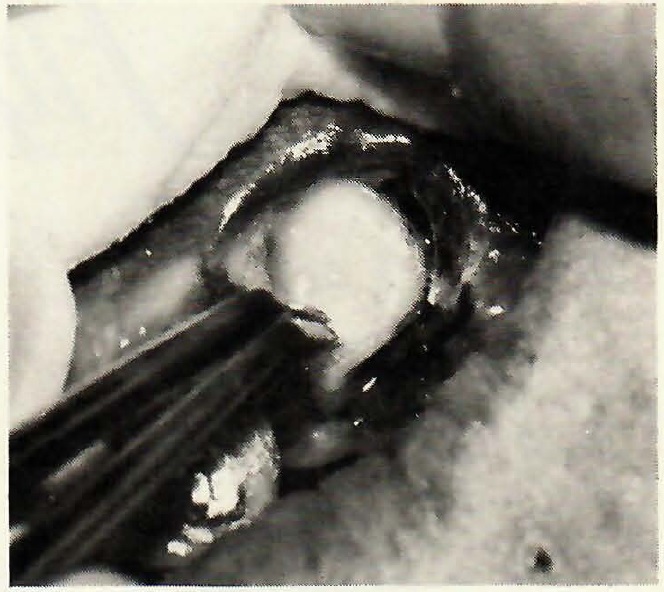
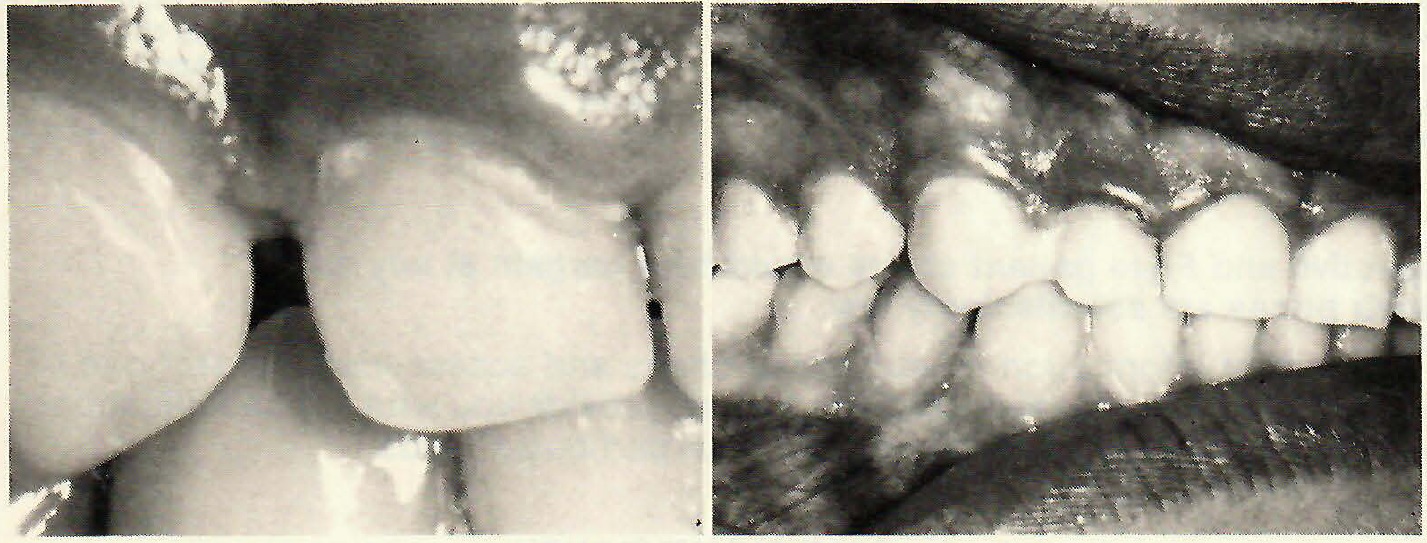
[show_img]462-jco-img-12.jpg[/show_img] Etched surface dried. [show_img]462-jco-img-13.jpg[/show_img] Sealant applied. [show_img]462-jco-img-15.jpg[/show_img] Attachment placed. [show_img]462-jco-img-16.jpg[/show_img] Bonded attachment tied in.DR. GOTTLIEB The appliance is made from an impression of the untreated surface and then the bulge is added?
DR. PHILLIPS That's correct. It puts a little extra push at that point. We also use the adhesive to build out the contour of small teeth to close diastemas due to tooth size discrepancy. For example, for a small lateral incisor that will be built out with a jacket following treatment, we build out during treatment with adhesive to close the space. It stabilizes the area and looks somewhat better than the gap between the teeth.
If a headgear patient has a band come off more than once, we bond it.
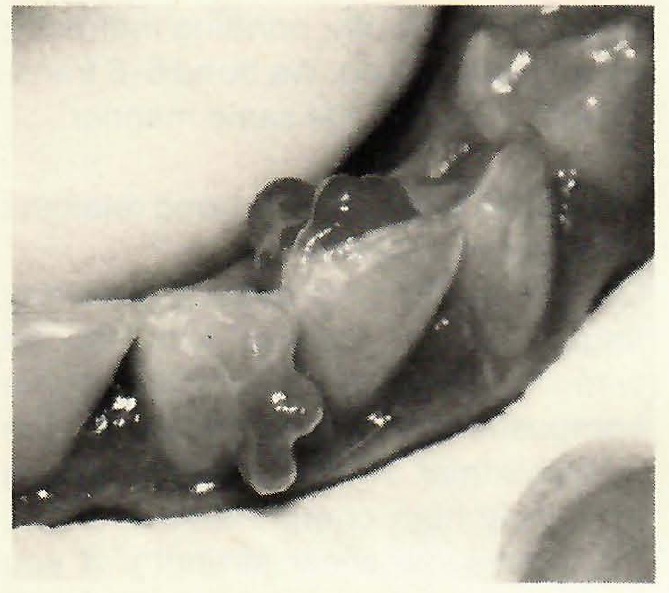
[show_img]462-jco-img-17.jpg[/show_img] Retention ledge of adhesive. [show_img]462-jco-img-19.jpg[/show_img] Retention bulge of adhesive. [show_img]462-jco-img-20.jpg[/show_img] Elastic engaged on retention ledge. [show_img]462-jco-img-21.jpg[/show_img] Retainer clasp engaging retention bulge. [show_img]462-jco-img-22.jpg[/show_img] Diastema closed with adhesive.DR. GOTTLIEB What is your technique for that?
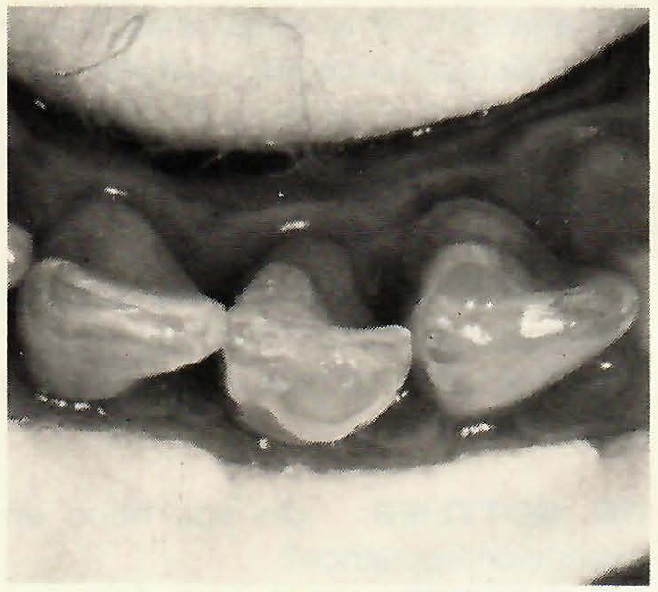
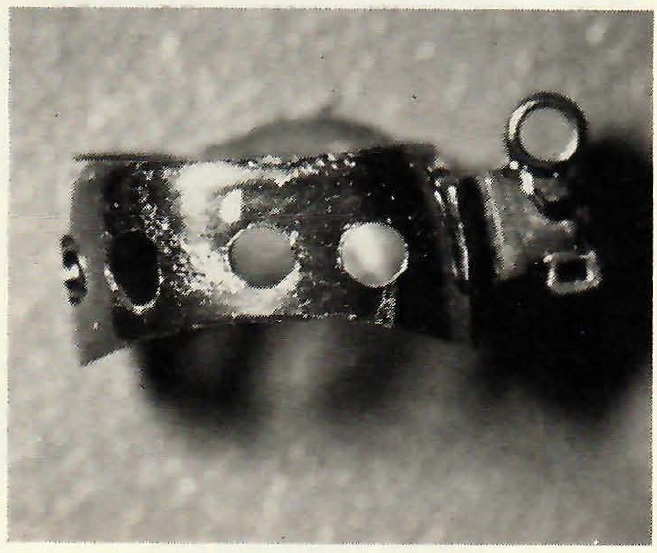
DR. PHILLIPS We make as many holes as we have room for all around the band with a half-round carbide bur in a high speed handpiece; carefully, because it is a slippery surface and you can hurt your finger. We etch the tooth surfaces we can reach and bond by conventional technique directly. We don't try to do this indirectly. There is no need.
[show_img]462-jco-img-23.jpg[/show_img] Etching selected tooth areas. [show_img]462-jco-img-24.jpg[/show_img] Adhesive bulges applied. [show_img]462-jco-img-25.jpg[/show_img] Positioner exerts pressure on adhesive bulges. [show_img]462-jco-img-26.jpg[/show_img] Band prepared for bonding.DR. GOTTLIEB You perforate the interproximal part of the band?
DR. PHILLIPS Yes, because the perforations are for the mechanical interlocking of the adhesive to the band. We're not concerned with whether or not we have etched the interproximal tooth surface. The basic retention is from the buccal and lingual etched surfaces as far as attachment to the tooth is concerned, but we want to interlock the band mechanically all around. This is a very effective way of keeping headgear bands on.
DR. GOTTLIEB Are these bonded bands trouble to remove?
DR. PHILLIPS In most cases, you can remove them with conventional band removing plier technique. If one is particularly stubborn, you can section it with a bur and remove it that way.
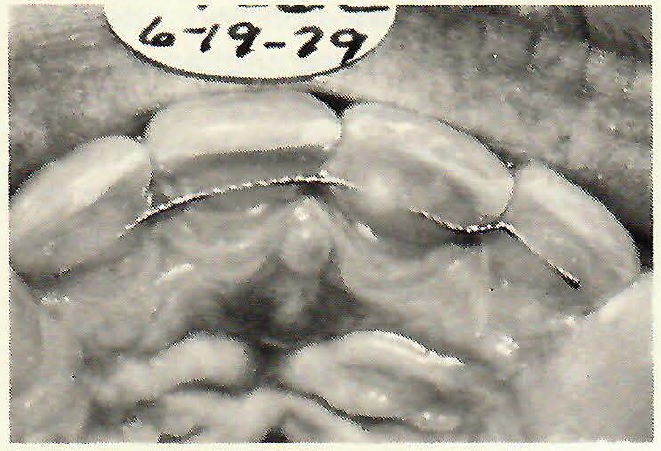
DR. GOTTLIEB Do you bond lower 3-3 lingual retainers?
DR. PHILLIPS Yes, and we do it indirectly. We fit the wire to the teeth on the model, make a small bend in each end of the wire where it will overlay the lingual aspect of the cuspid teeth, make a mound of adhesive that completely covers the lingual surface, then make an overlay tray and transfer the whole thing to the mouth, bonding indirectly, as we routinely do. We bond 6-6 transpalatal arches in the same manner.
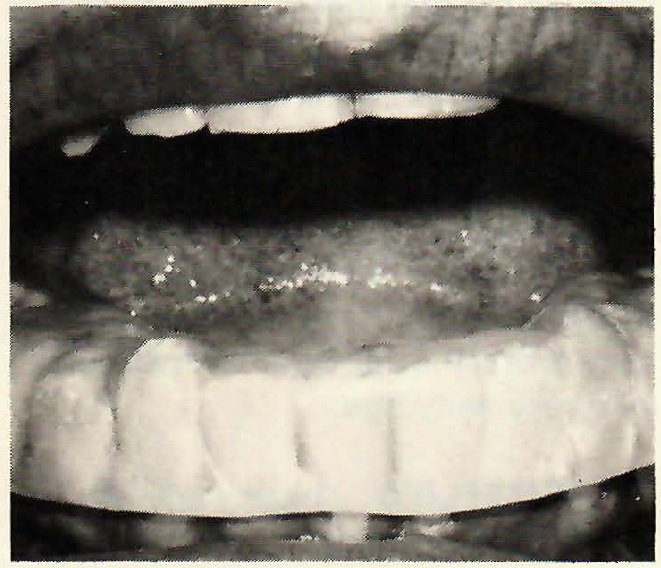
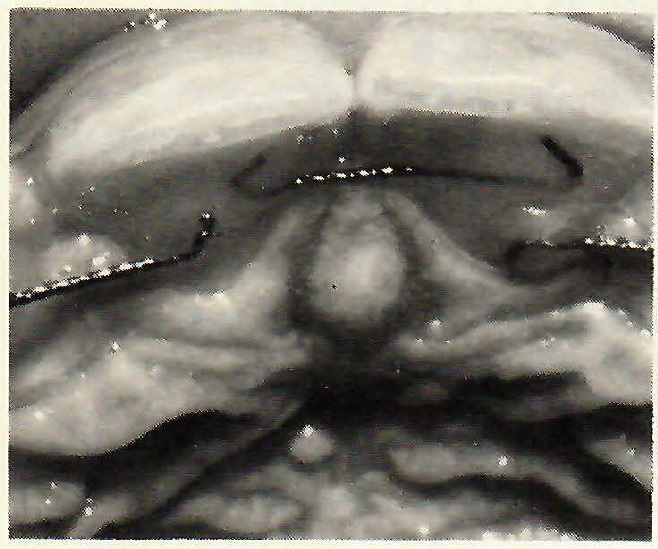
[show_img]462-jco-img-27.jpg[/show_img] Bonded lower lingual retainer. [show_img]462-jco-img-28.jpg[/show_img] Bonded transpalatal arch.DR. GOTTLIEB Do you bond retainers for maxillary teeth?
DR. PHILLIPS We make a maxillary lingual bonded retainer with braided wire. You have to be careful that the composite does not extend across the interproximal. These materials have an extremely high compressive strength, but pretty low shear strength. If you bond across the interproximal areas, the material will fracture. You also have to be aware of the occlusion. You can't do this if the lower incisors are going to bite against it. An alternative way we do this is with separate pieces of wire, one piece holding the centrals together and another for the central-to-lateral on each side.
DR. GOTTLIEB Do you go to the labial side if you can't bond the lingual?
DR. PHILLIPS You can. Of course, it is not as esthetic.
DR. GOTTLIEB Do you bond an expansion appliance?
DR. PHILLIPS Yes. I think there are significant advantages to doing it in this fashion, and we have been doing these for at least five years. The advantages include the fact that they are simple to fabricate and no tooth separation or band fitting is required. Beyond that, the entire buccal segment can be firmly encased in the acrylic, which I feel results in less alveolar bending and gives you as stable an attachment as you could possibly have. Another advantage is that the appliance can be placed at a very early age.
DR. GOTTLIEB How early an age would you consider?
DR. PHILLIPS My philosophy for expansion appliances is that if there is a skeletal crossbite that requires palatal expansion, you can't do it too early. The patient has to be emotionally able to handle it. No matter how short the clinical crowns, you can bond this appliance. You make it from one impression, with no further contact with the patient until the day you put it on. So, this is a very atraumatic way to construct and place an expansion appliance.
[show_img]462-jco-img-29.jpg[/show_img] Upper lingual bonded retainer. [show_img]462-jco-img-30.jpg[/show_img] Alternate upper lingual bonded retainer. [show_img]462-jco-img-32.jpg[/show_img] Upper labial bonded retainer.DR. GOTTLIEB Does the fact that the entire posterior occlusal surfaces are covered create any special problems?
DR. PHILLIPS I don't think so. No matter how expansion appliances are constructed, within a day or two the occlusion is destroyed anyway. The appliance is only in place 3 to 5 weeks at most, and in that length of time I'm not concerned with any permanent bite opening. It just doesn't seem to be a problem.
DR. GOTTLIEB What kind of spring do you prefer in the expansion appliance?
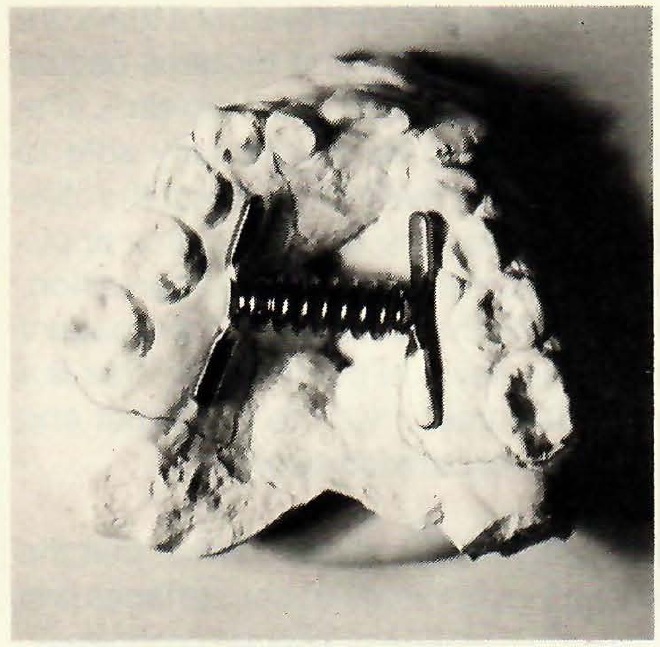
DR. PHILLIPS We use a spring-loaded expander called a Minne Expander. We adapt the bars on each end of the spring to the lingual surfaces of the teeth, as if we were going to solder them to bands. Then you can make the acrylic tray that covers all the posterior teeth, either by a pepper and salt technique or with a Biostar machine or vacuum-forming machine. After removing the appliance from the model, we perforate the acrylic trays because we are only looking for mechanical retention here. We're not concerned with whether there is any chemical bonding between the adhesive and the acrylic.
DR. GOTTLIEB How much etching do you do?
DR. PHILLIPS You have to be careful not to have more bonding retention than you want. These appliances have tremendous retention on deciduous and adult teeth. In fact, with fully erupted adult teeth, we etch only the buccal and lingual surfaces. If you etch the entire crown, you would simply have to carve the entire appliance off with a bur. If you only etch the buccal and lingual, you can generally break the appliance off in pieces, using posterior band removing pliers.
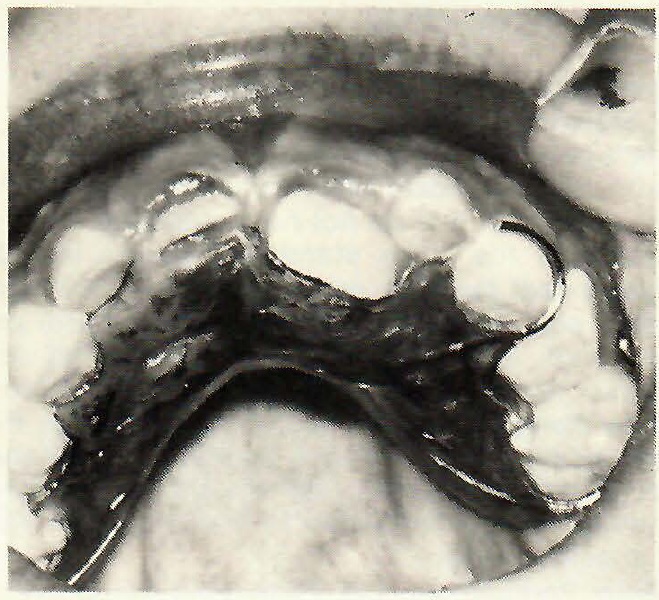
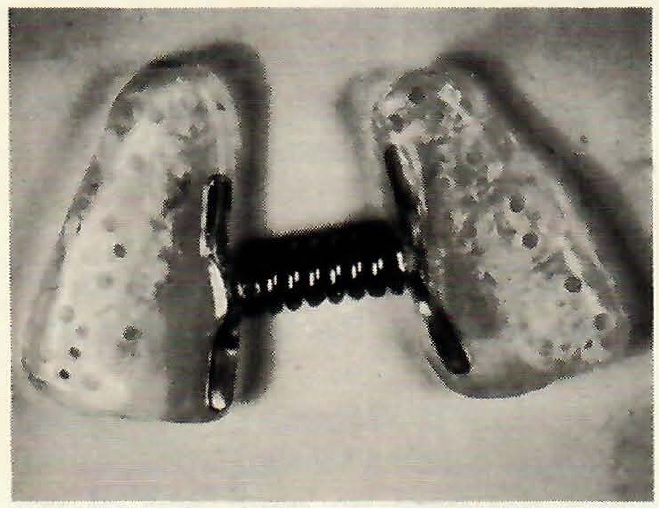
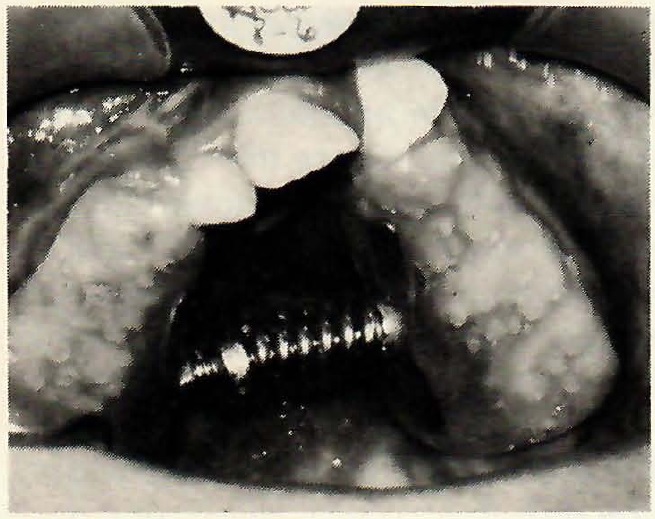
[show_img]462-jco-img-34.jpg[/show_img] Minne Expander on model. [show_img]462-jco-img-35.jpg[/show_img] Finished expansion appliance. [show_img]462-jco-img-36.jpg[/show_img] Bonded expansion appliance.DR. GOTTLIEB On deciduous teeth you do etch the occlusal?
DR. PHILLIPS Yes. On deciduous teeth or any teeth with extremely short clinical crowns, say a crown height of only 1mm, we do etch the occlusal surface.
DR. GOTTLIEB In such cases, do you use the same adhesive, or a more lightly filled one?
DR. PHILLIPS We use Concise, but in this case, we mix it in a proportion that gives us 3 to 4 minutes setting time, so that we have plenty of time to fill both halves of the appliance and seat it properly.
DR. GOTTLIEB How soon after the adhesive has set can you make your first adjustment in the springs?
DR. PHILLIPS We rarely wait more than 10 minutes. We hold the appliance in place for 5 minutes and then we let the patient get up and stretch a bit and rinse their mouth. By that time, we are ready to wind the spring. The spring of the Ormco Minne Expander is set by the operator. The patient does not adjust this spring. The patient comes to the office once a week and the doctor winds the spring. I prefer it, because I have control and it also gives me an opportunity to observe the patient at weekly intervals.
DR. GOTTLIEB What is you opinion about recycling and reusing metal brackets?
DR. PHILLIPS Probably 25% or 30% of metal brackets can be reused. The majority of brackets are damaged either during treatment or during the debonding procedure; so most of them are not usable more than one time. If, under strong magnification, the bracket slot appears undistorted and the bracket base and mesh are still in good shape, I see no reason not to use them at least one more time.
DR. GOTTLIEB What is your procedure for recycling brackets?
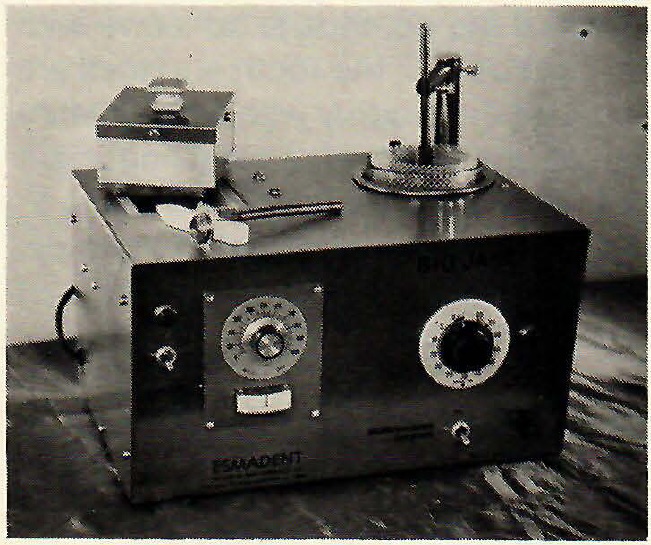
DR. PHILLIPS First of all, we put the brackets in separate containers at the time of debonding, to avoid having to sort them later. Following removal from the mouth, we burn off the composite in the Esmadent Big Jane unit. Then we clean the bracket in the ultrasonic cleaner solution and place them in the polishing part of the Big Jane unit. The brackets that we do recycle appear to be very satisfactory.
[show_img]462-jco-img-37.jpg[/show_img] "Big Jane" reconditioner and polisher.DR. GOTTLIEB Many orthodontists tell me that bonding attachments isn't the problem, but that debonding is. Do you feel the same way about debonding?
DR. PHILLIPS I don't consider debonding to be a problem. There is ample instrumentation in the form of diamond or carbide burs in a high speed air rotor, to remove composite from the tooth. Of course, this must be done with care to avoid marring the tooth surface. Debonding involves getting the bracket and the bulk of adhesive off the teeth and then polishing the tooth surfaces following that.
DR. GOTTLIEB What do you use to accomplish the first part?
DR. PHILLIPS In the early days of debonding, we still had a debanding mentality and tried using typical band removing pliers, which didn't work so well. We were putting tremendous stresses on the teeth in that way. Although I never saw it happen, I was concerned about fracturing a cusp or an incisal edge. We now know that the simplest way to get brackets off is to use a shearing type of instrument, such as a ligature cutter, with the blades held flat against the tooth surface. As a rule, this causes fracture within the adhesive and the bracket comes off very easily. I feel that good debonding starts with proper bonding. If the bonding adhesive has been put on only in the required amount, there simply isn't as much to take off and the problem is simplified to begin with.
DR. GOTTLIEB After popping the bracket off as you described, how do you handle the adhesive that still remains on the tooth?
DR. PHILLIPS Much of the remainder can be removed with the same shearing type instrument. These are made with blades at various angles to facilitate removal in various quadrants. Depending on the type of adhesive and the quantity, some of it can be removed with a hand scaler, but this is quite difficult with the harder materials. My preference, following the use of the ligature cutter, is a straight fissure carbide bur in a high speed handpiece, turned rather slowly at 100,000 to 150,000 rpm. The specific bur that I prefer is a #1157 which has a rounded tip rather than a truncated tip and no sharp edges at the end of the cylinder which might scratch the teeth.
DR. GOTTLIEB Do you use the bur in a wet field or a dry field?
DR. PHILLIPS We generally do this in a dry field. We place a cotton roll in the area where we are working and dry the teeth. We prefer to use air directed at the working site as a coolant, rather than using a water spray. A water spray would be more effective as a coolant, but would obscure the view. So, we work with a dry field. This requires using a high speed vacuum, because the bur turning at that speed turns the composite into dust, which the vacuum takes away.
DR. GOTTLIEB Does the carbide bur work better in a dry field?
DR. PHILLIPS I'm not sure of that. My reason for working in a dry field is strictly for visibility. I want to see precisely what I am doing.
[show_img]462-jco-img-38.jpg[/show_img] Carbide bur used In debonding. [show_img]462-jco-img-39.jpg[/show_img] Pumicing following debonding.DR. GOTTLIEB Do you use loupes at this stage?
DR. PHILLIPS I do. I find that I can see things with loupes that I can't see any other way. The nearest thing to it is when you enlarge slides with a projector. You see things that you simply do not see clinically. With loupes, you find what you thought was good bonding with no flash, actually does have flash. And, you can remove composite with a bur more carefully. There is no bur that cannot scar tooth enamel, but if you do this step carefully, there is a minimum of scarring and it removes the material quite rapidly.
DR. GOTTLIEB And then you polish?
DR. PHILLIPS Right. Following removal of the composite adhesive with the carbide bur, the tooth surfaces are pumiced thoroughly with a prophylactic instrument. This is a most important and necessary step if you are trying to end with a very smooth tooth surface. My object is to leave the surface at least as good as it was to begin with.
DR. GOTTLIEB Is that evaluation of the finished surface with a loupe or with the naked eye?
DR. PHILLIPS With a loupe.
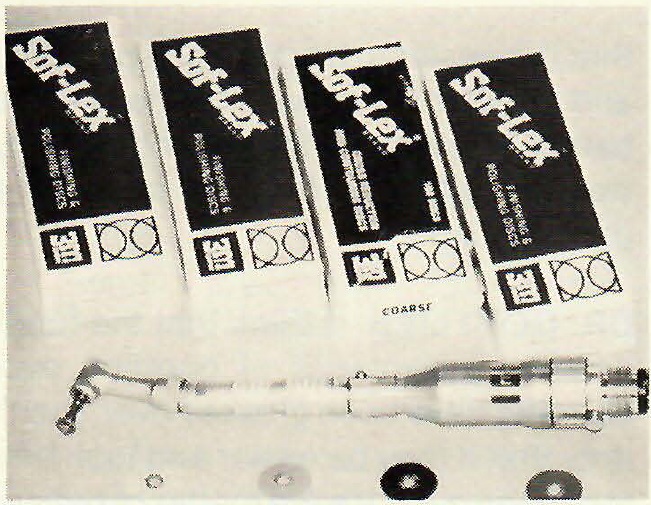
[show_img]462-jco-img-40.jpg[/show_img] Soflex discs used following pumicing.DR. GOTTLIEB Does the pumicing conclude the debonding process?
DR. PHILLIPS The teeth generally look pretty good following the pumicing, but a step beyond that must be taken if you are looking for the most highly polished tooth surface you can get, especially on flat incisor teeth. That step is to use a series of finishing discs in a low speed contrangle handpiece.
DR. GOTTLIEB Which discs do you use?
DR. PHILLIPS The ones we have found most effective for this purpose are the 3M Soflex Disc Series which comes in 4 grits--coarse, medium, fine, and superfine. If you are looking for the best surface, you can't take shortcuts here. You must use all four discs. You have to program yourself to the fact that you are going to have to take these steps, if you want the best surface you can make. It almost takes more time talking about it than it does to do it. It takes about three minutes for the four upper incisors and I think I owe it to the patient to spend those three minutes. The teeth will look nicer and will be more plaque free.
DR. GOTTLIEB These discs are too fine to take the place of the pumice, I would gather.
DR. PHILLIPS Well, yes and no. The pumicing does things that a disc can't do because of better access of a prophy cup versus a disc. You can't do the interproximal surfaces as well with the discs alone as you can with the pumice followed by the discs. We have tried many combinations and find that pumicing followed by the full four-disc series results in the best surface. We've used various polishing pastes. We've used rubber wheels. We've used mounted points. We always come back to the method I described. It will leave a very highly polished surface in a very short period of time.
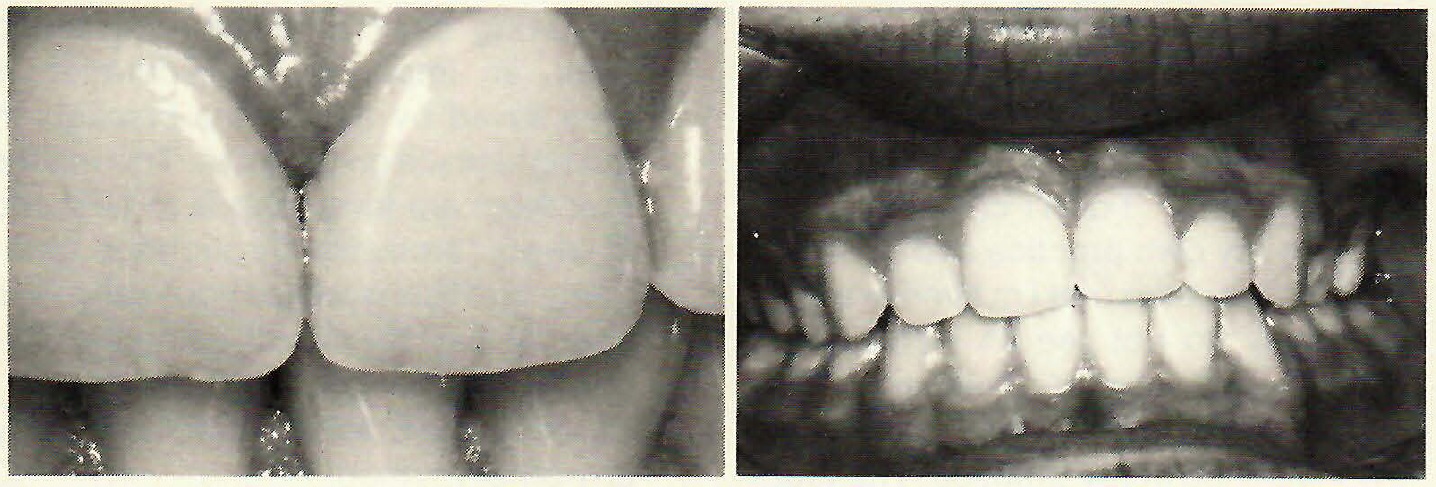
[show_img]462-jco-img-41.jpg[/show_img] Following debonding procedures.DR. GOTTLIEB Do you consider decalcification to be much of a problem with bonding?
DR. PHILLIPS As far as I am concerned, the only significant problem that remains in bonding is decalcification around the bracket pad. The key to avoiding it is good oral hygiene, but not all patient are excellent brushers. The next best thing to routine good home care is office fluoride treatments. At our bonding appointments, we routinely give a fluoride treatment immediately following bracket placement, and we urge the use of a fluoride gel as part of home care. I am looking for a system that will protect even the poor brusher from decalcification. I am working with such a system at present, which shows promise of greatly reducing the amount of decalcification suffered by poor brushers.
DR. GOTTLIEB Are you much concerned about decalcification under the bracket, due to voids or seepage?
DR. PHILLIPS No. We don't have that as a rule. The sealant isn't exposed to air under the bracket, so it does polymerize totally there. Beyond that, it's a matter of knowing how much adhesive to put on and examining it carefully after we've bonded. If there is a gap somewhere, we've got a mistake we can correct right then.
DR. GOTTLIEB A question was raised whether removing the interproximal protection of bands resulted in increased- interproximal caries. Is that still an issue?
DR. PHILLIPS I don't consider it an issue. In my own practice and in other bonding practices that I'm familiar with, we simply do not see an increase in interproximal decay compared to banded cases. There is an extremely low incidence in my practice. The fact that it is easier to brush is one part of it, and another is that we don't have loose bands or bands with cement partially washed out being left on a tooth for a period of time.DR. GOTTLIEB I think that the fundamental advantages of bonding over banding have been glossed over. It isn't only that it may be easier and look better. To my mind it's the matter of patient comfort, and getting rid of separation, band fitting, and the thickness of interproximal band material. To me, these alone would justify bonding, without any of the other factors involved.
DR. PHILLIPS They would indeed, and we could add not having to be concerned about closing band spaces and the ability to take bite wing x-rays at any time during treatment to check for interproximal decay without removing the appliance. There are many advantages to the patient and the orthodontist, but the main one would have to be patient comfort.
DR. GOTTLIEB Most orthodontists who bond favor a direct technique over an indirect one. They say that indirect takes more time and is no more accurate.
DR. PHILLIPS Certainly the overall time is greater using an indirect technique, but chair time for the patient and the doctor is much reduced. In addition to saving chair time during bonding itself, an important consideration is time saved by having the brackets in the right place on the teeth. This means that there are fewer bends to be made in every archwire throughout treatment, and this is where you really save time. At least for myself, using the indirect technique that I have described, I cannot place brackets as accurately by any other method.