CASE REPORT
Segmental Mechanics with T-Loop Springs for Management of Ectopic Canines and Severe Crowding
Because highly displaced canines are frequently associated with crowding, a nonextraction approach may result in proclination of the anterior teeth, with detrimental effects on the soft-tissue profile. To resolve the crowding and achieve stable results, an extraction approach is often chosen, using either frictional or frictionless mechanics, depending on the needs of the patient, to close the resulting spaces. Since frictionless mechanics with customized, precalibrated springs and other space-closure assemblies can enable greater control over tooth movement,1 it has become an integral part of segmented-arch approaches to extraction treatment.2,3
The T-loop retraction spring is particularly useful for canine repositioning because it provides precise control over tooth movement and avoids the effects of friction between archwire and brackets. The spring consists of a T-shaped loop, an anterior (alpha) arm, and a posterior (beta) arm. Tooth movement can be managed in three dimensions by adjusting different parts of the loop to change the horizontal and vertical force vectors delivered by the beta arm.4 Differential moments are produced either by changing the angulations of the preactivation (gable) bends or by positioning the spring off center to adjust the relative lengths and, hence, the magnitudes of forces generated by the alpha and beta arms.5-7
This article outlines the use of segmental mechanics with T-loop springs after premolar extractions in a patient with ectopic canines and severe crowding.
Diagnosis and Treatment Plan
A 17-year-old female presented with the chief complaint of forwardly positioned upper teeth (Fig. 1). The profile was convex, with a retrusive chin, lip incompetence, and a marked tooth-size/archlength discrepancy in both arches.
Similar articles from the archive:
- ALIGNER CORNER Treatment of a Class II, Division 1 Malocclusion and Ectopic Canines with Invisalign Mandibular Advancement and the Bootstrap Technique March 2025
- Effective Torque Correction for Buccally Erupted Ectopic Canines February 2024
- CASE REPORT Management of an Ectopic Lower Canine by Autotransplantation and Orthodontic Treatment November 2016

Fig. 1 17-year-old female patient with highly displaced upper right canine, ectopic lower right canine, and severe crowding before treatment.
The molar relationships were Class I on the left and end-on Class II on the right. Both archforms were ovoid, with severe crowding. The upper right canine was highly displaced, positioned between the upper right lateral incisor and first premolar. The lower right canine was ectopic, and the lower right lateral incisor was palatally displaced, potentially explaining a 3mm lower dental midline deviation to the right. The overjet was excessive, but the overbite was within the normal range.
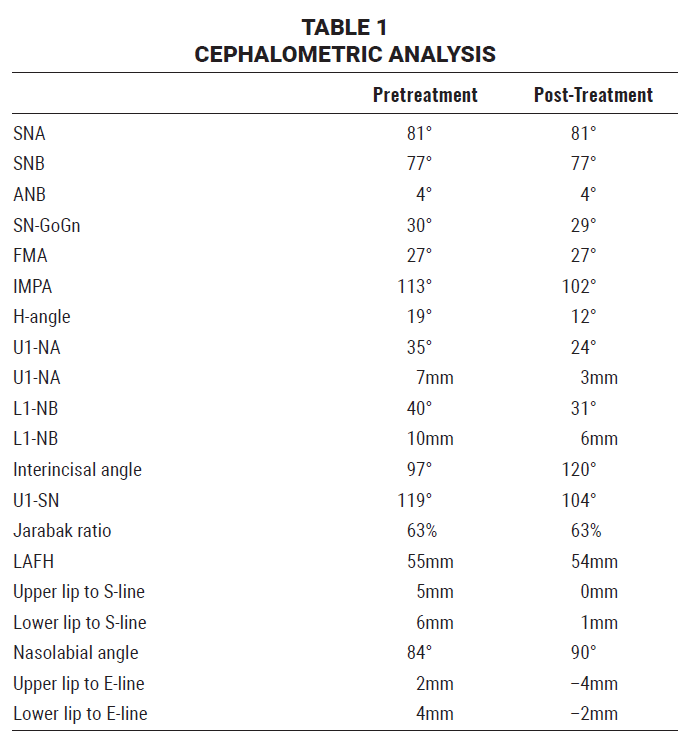
The panoramic radiograph confirmed the presence of all four third molars, with normal levels of alveolar support. Cephalometric analysis showed a skeletal Class I relationship with a normodivergent growth pattern (Table 1). Both the upper and lower incisors were proclined. The H-angle (19°) indicated protrusive upper and lower lips and a retrusive chin position. The nasolabial angle was acute, and the mentolabial sulcus was diminished.
Treatment objectives were to resolve the crowding and align the teeth, achieve an ideal overjet and a Class I molar relationship on the right, and improve the facial appearance. Because of the severe crowding, both proposed treatment options included extraction of the four first premolars. The first alternative would have combined the extractions with an anterior segmental osteotomy, due to the patient’s thin alveolus, followed by a genioplasty to address the retrusive chin. In the second approach, extractions would be followed by full retraction of the anterior teeth to close the spaces; if there was no improvement in the facial profile at that point, we would proceed with micro-implant-supported en masse distalization of both arches. To avoid surgery, the patient selected the second alternative.
Treatment Progress
Before orthodontic treatment began, the patient was referred to an oral surgeon for extraction of all first premolars. Since the upper and lower incisors were proclined and the canines were ectopic, a continuous archwire would have led to unwanted intrusion of the anchor units and roundtripping of the incisors. Therefore, a two-step retraction was planned: after all four canines were retracted with segmental T-loop springs, the incisors would be retracted.
Preadjusted .022" appliances were bonded to all the canines, and the first molars were banded. Four T-loop springs were fabricated from .017" × .025" TMA* wire, with 15° alpha activation bends and 30° beta activation bends, and inserted into the molar bands and canine brackets, closer to the posterior segments for better anchorage (Fig. 2).
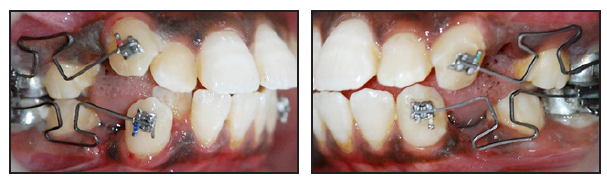
Fig. 2 Four T-loops placed for canine retraction.
The springs were reactivated every eight weeks over the next four months, resulting in 4mm of retraction. Distal tipping and mesial-out rotation of the lower right canine were attributed to insufficient alpha and antirotation bends. Therefore, further reactivation of the lower right T-loop was discontinued.
After four months, the canine retraction of was complete (Fig. 3); all four canines displayed good root parallelism, except for the lower right. Elastomeric chains were placed to relieve mild anterior spacing.

Fig. 3 After four months of treatment, canine retraction completed and anterior retraction initiated.
The rest of the teeth were bonded for the next stage of treatment. The continuous archwire sequence began with .014" nickel titanium, using passive lacebacks on the canines to prevent mesial tipping, and proceeded to .018" × .025" copper nickel titanium, with the ligatures tightened for anterior retraction.
After 13 months of treatment, the archwires were replaced with .019" × .025" stainless steel, with additional torque on lower right canine to improve its position, and the remaining spaces were closed with elastomeric chains. To correct the end-on molar relationship, Class II elastics (5⁄16", 6oz) were worn on the right side.
After a total active treatment time of 18 months (Fig. 4), all appliances were removed. Because the patient was satisfied with the improvements in her facial profile and occlusion, she declined a genioplasty; en masse distalization was deemed unnecessary, although removal of the third molars was recommended. Upper and lower circumferential wraparound retainers were delivered for one year of full-time wear and nighttime wear thereafter.

Fig. 4 After 18 months of treatment, before debonding.
Treatment Results
Class I canine and molar relationships were obtained on both sides, resulting in an improved occlusion with good anterior and canine guidance (Fig. 5). Adequate lip seal was established, along with improvements in the nasolabial angle and lip protrusion.

Fig. 5 Patient after treatment, showing well-aligned canines and incisors and improvement in soft-tissue profile.
The canine and premolar roots were parallel on the panoramic radiograph. Cephalometric analysis confirmed an improvement in the soft-tissue profile (Table 1). As documented in previous studies, retraction of the incisors produced beneficial changes in the lip positions,8,9 resulting in a good lip seal, as well as posterior movement of the soft tissue over points A and B,10 leading to an improved nasolabial angle. The upper anterior teeth were ideally inclined, and the inclination of the lower incisors improved significantly; although they remained proclined, no further treatment was considered necessary, given the position of the lower lip and the normalized overjet and overbite. Gingival health was good overall, and the occlusion remained stable after treatment.
Discussion
The T-loop spring, introduced in 1960 by Stoner,11 is an effective device for frictionless mechanics.12 The loop’s position in the interbracket space can be adjusted to produce differential moments: a more anterior placement increases the alpha moment, while a more posterior placement increases the beta moment. As noted by Burstone and Koenig,13 the height and dimensions of the loop also affect the moment-to-force ratio; the loops used in the present case were therefore bent to Burstone’s specifications. To fabricate the spring, TMA wire is recommended because of its excellent mechanical properties and good formability, as well as a lower load-deflection rate than with stainless steel.14
When incorporated with archwires for en masse retraction, T-loops deliver a regulated force system to the teeth, thus improving predictability, as long as the position of the loop and angulations of the bends are properly designed to deliver the forces required for adequate anchorage. This need for precision is a known disadvantage of the T-loop spring: small differences in its positioning or fabrication can produce significant effects,15 as demonstrated by the undesirable rotation and tipping of the lower right canine observed in our patient. T-loop springs can also cause vertical side effects such as extrusion of the posterior teeth; a transpalatal arch can be incorporated to improve vertical control of the molars and thus limit this side effect.
Alternatives to the T-loop spring include the PG spring, developed by Gjessing,16 and the closed helical loop. An advantage of the PG spring is that it does not require activation bends, since it generates a moment-to-force ratio of 8.0-9.1:1 to promote canine retraction. In addition, the use of PG springs avoids the inefficient sequence of tipping, bodily movement, and root uprighting often required with T-loops. Nevertheless, PG springs are fabricated from stainless steel, which exerts a higher load-deflection rate than TMA, while T-loops deliver force levels closer to those required for canine translation.17 In comparison to closed helical loops, T-loops also exert less force but an increased moment-to-force ratio after 1mm of activation, as noted in a finite element analysis by Chacko and colleagues.18
In the present case, the combination of premolar extractions and segmental mechanics with T-loop springs successfully resolved the bimaxillary protrusion and crowding while avoiding the roundtripping that would occur with continuous mechanics, demonstrating the advantages of this approach.
FOOTNOTES
- *Registered trademark of Ormco, Brea, CA; www.ormco.com.
REFERENCES
- 1. Burstone, C.J.: The segmented arch approach to space closure, Am. J. Orthod. 82:361-378, 1982.
- 2. Burstone, C.J.: Rationale of the segmented arch, Am. J. Orthod. 48:805-822, 1962.
- 3. Burstone, C.J.: The mechanics of the segmented arch techniques, Angle Orthod. 36:99-120, 1966.
- 4. Faulkner, M.G.; Lipsett, A.W.; El-Rayes, K.; and Haberstock, D.L.: On the use of vertical loops in retraction systems, Am. J. Orthod. 99:328-336, 1991.
- 5. Burstone, C.J. and Hanley, K.J.: Modern Edgewise Mechanics and the Segmented Arch Technique, Department of Orthodontics, University of Connecticut School of Dental Medicine, Farmington, CT, 1985.
- 6. Sachdeva, R.C.: A study of force systems produced by TMA T'loop retraction springs, thesis, University of Connecticut, Storrs, CT, 1985 (www.academia.edu/72110535/A_Study_of_Force_Systems_Produced_by_TMA_T_loop_Retraction_Springs).
- 7. Manhartsberger, C.; Morton, J.Y.; and Burstone, C.J.; Space closure in adult patients using the segmented arch technique, Angle Orthod. 59:205-210, 1989.
- 8. Kusnoto, J. and Kusnoto, H.: The effect of anterior tooth retraction on lip position of orthodontically treated adult Indonesians, Am. J. Orthod. 120:304-307, 2001.
- 9. Solem, R.C.; Marasco, R.; Guiterrez-Pulido, L.; Nielsen, I.; Kim, S.H.; and Nelson, G.: Three-dimensional soft-tissue and hard-tissue changes in the treatment of bimaxillary protrusion, Am. J. Orthod. 144:218-228, 2013.
- 10. Baik, W.; Choi, S.H.; Cha, J.Y.; Yu, H.S.; and Lee, K.J.: Comparison of soft tissue changes between incisor tipping and translation after premolar extraction, Kor. J. Orthod. 52:42-52, 2022.
- 11. Stoner, M.M.: Force control in clinical practice: I. An analysis of forces currently used in orthodontic practice and a description of new methods of contouring loops to obtain effective control in all three planes of space, Am. J. Orthod. 46:163-186, 1960.
- 12. Babacan, H.; Kiliç, B.; and Biçakçi, A.: Maxillary canine-first premolar transposition in the permanent dentition, Angle Orthod. 78:954-960, 2008.
- 13. Burstone, C. and Koenig, H.A.: Optimizing anterior and canine retraction, Am. J. Orthod. 70:1-19, 1976.
- 14. Maia, L.G.; de Moraes Maia, M.L.; da Costa Monini, A.; Vianna, A.P.; and Gandini, L.G. Jr.: Photoelastic analysis of forces generated by T-loop springs made with stainless steel or titanium-molybdenum alloy, Am. J. Orthod. 140:e123-e128, 2011.
- 15. Kuhlberg, A.J. and Burstone, C.J.: T-loop position and anchorage control, Am. J. Orthod. 112:12-18, 1997.
- 16. Gjessing, P.: Controlled retraction of maxillary incisors, Am. J. Orthod. 101:120-131, 1992.
- 17. Karanth, D. and Shetty, V.S.: Canine retraction by sectional arch technique: Comparison of characteristics between T loop retraction spring and PG retraction spring, J. Ind. Orthod. Soc. 35:17-27, 2002.
- 18. Chacko, A.; Tikku, T.; Khanna, R.; Maurya, R.P.; and Srivastava, K.: Comparative assessment of the efficacy of closed helical loop and T-loop for space closure in lingual orthodontics—A finite element study, Prog. Orthod. 19:14, 2018.
-
 DR. MALIK
DR. MALIK -
 DR. MAHINDRA
DR. MAHINDRA
Dr. Malik is an Assistant Professor, Department of Dentistry, Government Dental College and Hospital, Near Panchakki Road, Aurangabad, Maharashtra, India E-79; e-mail: mayankamalik97@gmail.com. Dr. Mahindra is a Professor and Head of Department, Department of Dentistry, Government Dental College and Hospital, and in private practice in Aurangabad, India.
