DIAGNOSTIC CHALLENGE #1
Part 2
In this monthly column, Contributing Editors Gayle Glenn, DDS, MSD, and Shawn L. Miller, DMD, MMSc, present a case to challenge your diagnosis and treatment-planning skills. The initial records for this case were introduced in the previous issue. Here, Dr. Glenn and Dr. Miller discuss how the case was treated.
Courtesy of University at Buffalo
Similar articles from the archive:
Diagnosis
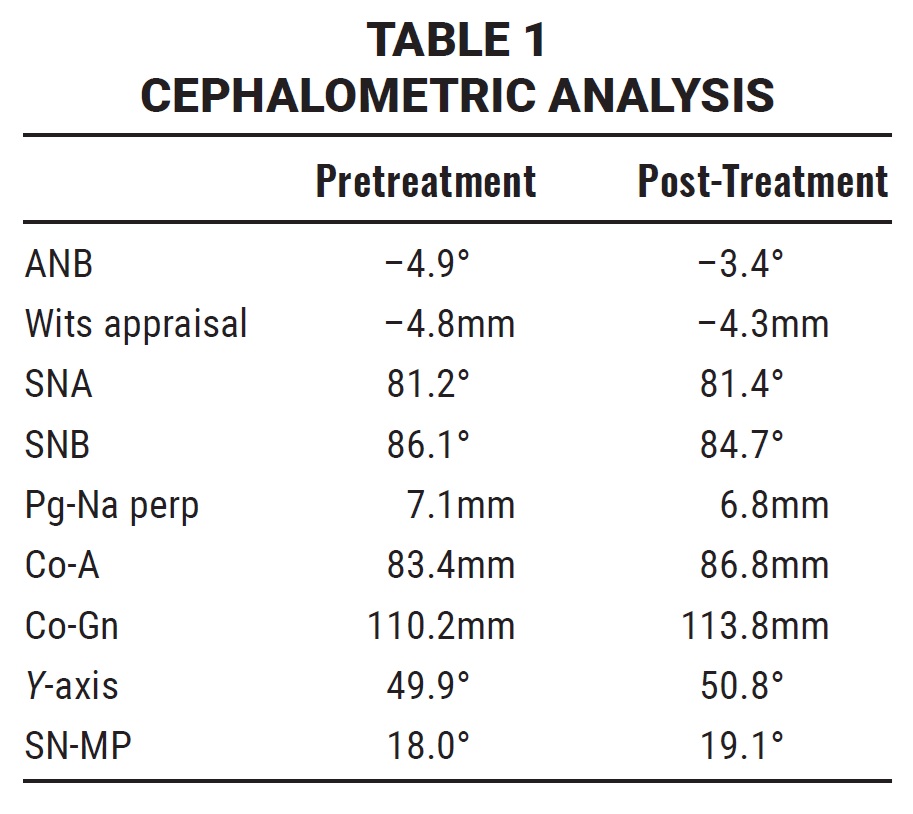
The patient presented with a skeletal Class III malocclusion, a hypodivergent growth pattern, and diminished lower anterior facial height. The smile arc was nonconsonant, with 70% incisal display in smiling. The maxillary midline was deviated 1.5mm to the right of the facial midline, and the mandibular midline was deviated 1.5mm to the left. An anterior crossbite was present at the upper right lateral incisor and from the upper left central incisor to the canine; due to premature contact at the incisors, a 2.5mm anterior functional shift between centric relation and maximum intercuspation was observed. The upper and lower right lateral incisors demonstrated grade 2 mobility. A 1.1mm Bolton discrepancy was attributable to a mandibular excess (Fig. 1A and 1B).

Fig. 1A Initial records (continued in next image).
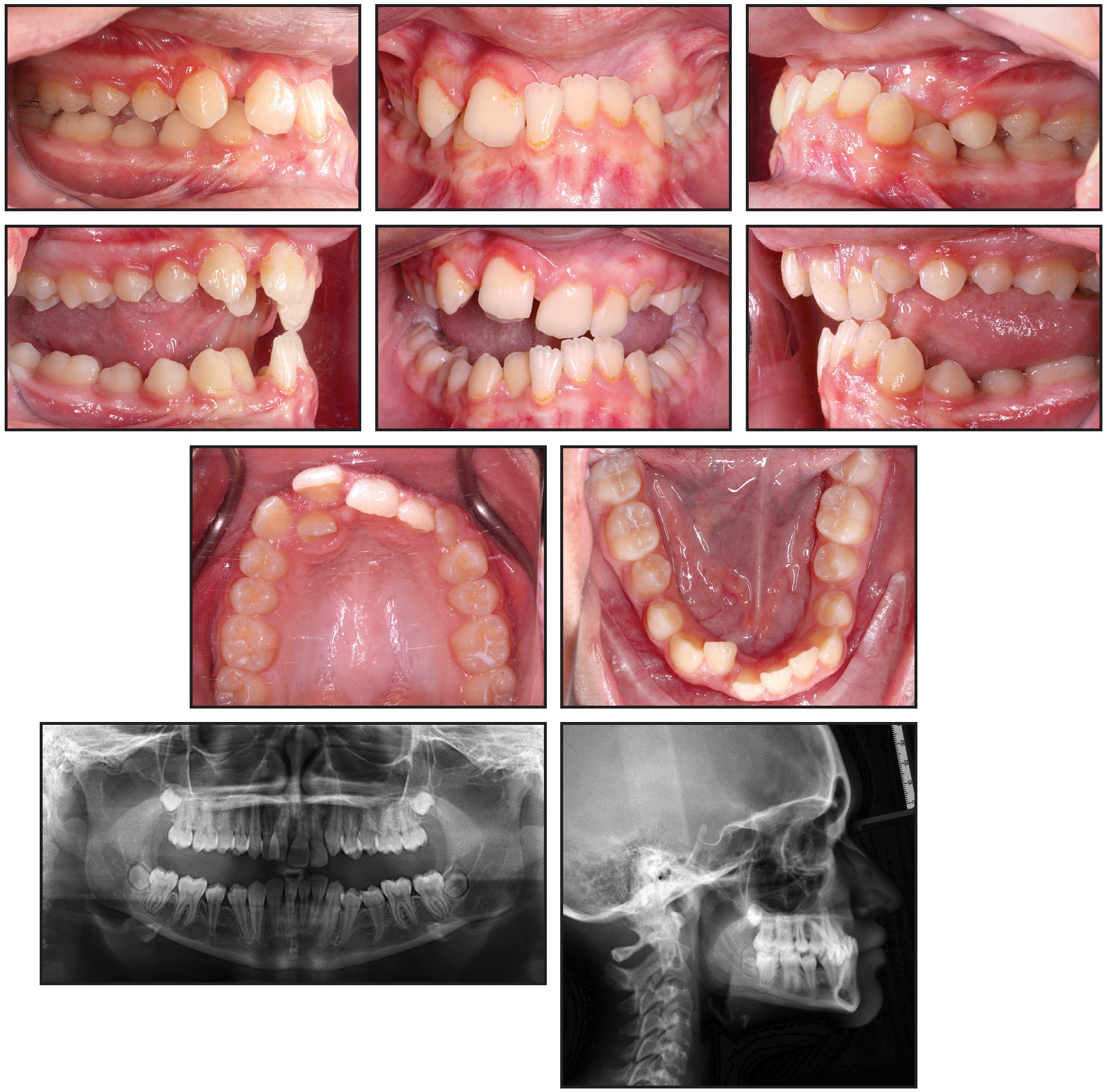
Fig. 1 (cont.) Initial records.
Bilateral Class III molar relationships were present, along with a Class I canine relationship on the right; the canine relationship on the left could not be determined. The upper and lower incisors were retruded and retroclined. A severe deep bite (10.7mm) and negative overjet (–2.4mm) were noted. The curve of Wilson was exaggerated, as was the curve of Spee (5.5mm). Moderate crowding was present in the upper arch; the lower arch was tapered, with mild crowding.
Treatment
Objectives: Eliminate functional shift, correct midline deviation, achieve normal overjet and overbite, establish Class I molar and canine relationships, level curve of Spee, and improve smile esthetics while maintaining profile.
Plan: Nonsurgical, nonextraction treatment with .022" MBT*-prescription brackets, fixed posterior bite block for bite jumping, and fixed anterior bite plate to correct deep bite.
- Fixed posterior bite block installed with bands on upper first molars and metal extension arms to premolars. Upper arch bonded from canine to canine, excluding upper right lateral incisor.
- After correction of functional shift, posterior bite block removed. Patient scanned for fabrication of fixed anterior bite plate with bands on upper first molars. Bite plate installed; upper premolars and lower arch bonded.
- Sequence of .014"-.018" round and .016" × .022" rectangular nickel titanium archwires used for leveling and alignment.
- Archwires changed to .016" × .022" stainless steel, with open coils at upper lateral incisors to open space; after space opening, .014" nickel titanium overlay wires added to align upper lateral incisors.
- Vertical Class III box elastics (¼", 6oz) worn 22 hours per day from upper premolars to lower canines and first premolars to extrude premolars, level curve of Spee, obtain Class I molar and canine relationships, and achieve ideal overjet and overbite.
- Arch coordination, finishing, and detailing performed.
- Hawley retainers delivered for both arches, with anterior bite plate added to upper retainer.
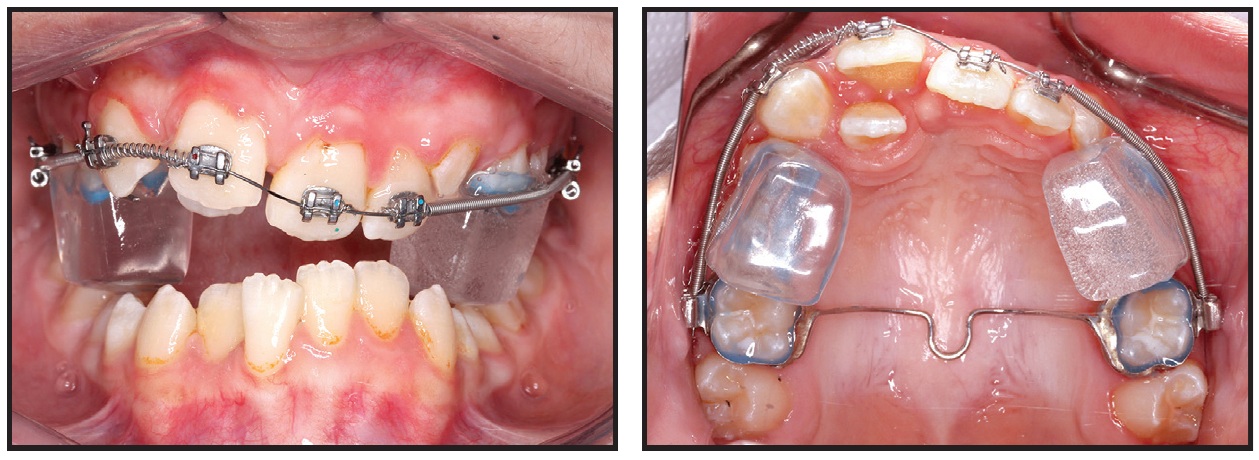
Fig. 2 Progress records. Posterior bite block in place.
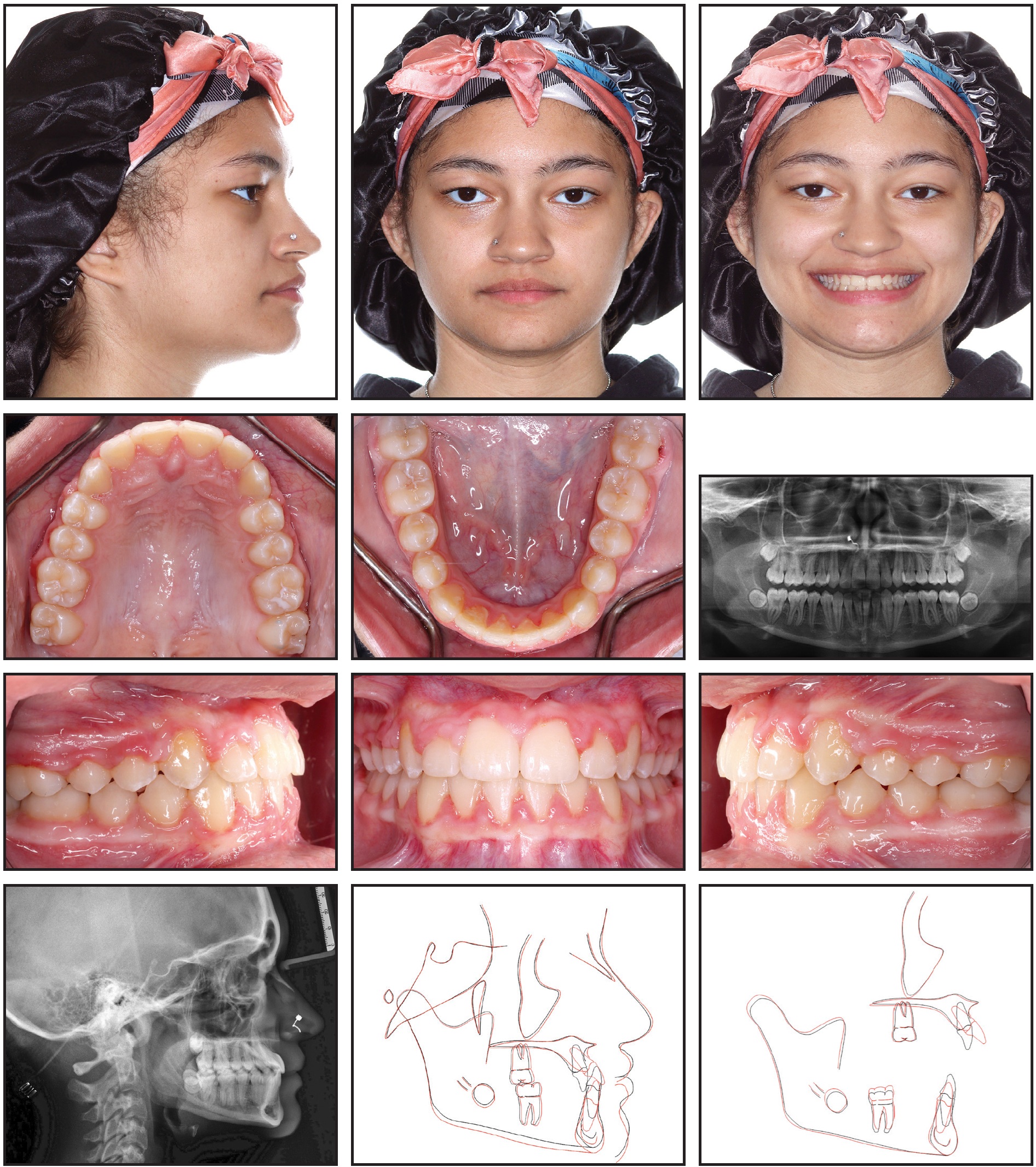
Fig. 3 Final records.
Discussion
This case illustrates two critical orthodontic concepts: first, from a diagnostic standpoint, the importance of recognizing a functional shift between centric relation and maximum intercuspation, and second, from a treatment standpoint, the need to properly manage the vertical dimension.
If an anterior crossbite is present, we should assume there is a functional shift unless proven otherwise. An in-person clinical examination is required for diagnosis. Functional shifts are essential to recognize for treatment planning, yet they are sometimes missed even by astute clinicians. In this case, without the anterior shift, nonsurgical treatment would have been nearly impossible.
The treatment plan and mechanics must be carefully designed to achieve the soft-tissue, skeletal, and dental treatment objectives. Here, the vertical dimension was managed with fixed posterior bite blocks, followed by a fixed anterior bite ramp and sequential segmented fixed appliances (Fig. 2). This approach required good patient compliance, but it successfully addressed the deep overbite, leveled the curve of Spee, increased the lower face height, and allowed for clockwise mandibular rotation.
Because of the traumatic malocclusion, it was inadvisable to wait until growth was complete to perform orthognathic surgery, although early surgery with maxillary premolar extractions could have yielded ideal esthetic results. Because of the curve of Wilson at the outset, another option could have involved maxillary expansion to produce skeletal rather than dentoalveolar changes. Other alternatives, such as lower-arch extractions or distalization with skeletal anchorage, would have made it extremely challenging to level the curve of Spee and increase the posterior vertical dimension.
The use of an upper Hawley retainer with an anterior bite plate should discourage post-treatment deepening of the overbite. Nevertheless, undesirable changes could be caused by late mandibular growth. The patient and parents should be informed of that possibility, which might require retreatment with surgery in adulthood.
This case illustrates the favorable esthetic and functional outcomes that can be achieved when all factors align appropriately (Fig. 3). Well done!
SLM & GG
If you have a case you'd like to see featured in the Diagnostic Challenge, please follow these guidelines and use our submissions system. Go to our About page for more information on how to submit articles to JCO.
FOOTNOTES
- *Registered trademark of Solventum, St. Paul, MN; www.solventum.com.
-
 DR. HAMIDUDDIN
DR. HAMIDUDDIN -
DR. WARUNEK
-
DR. GLENN
-
DR. MILLER
Dr. Hamiduddin was a Resident and Dr. Warunek is Clinical Assistant Professor and Orthodontics Research Director, Orthodontic Department, University of Buffalo School of Dental Medicine, Buffalo, New York. Dr. Hamiduddin is now in Private Practice, 1827 Jeffersonian Drive, Vienna, VA, 22182. E-mail her at aliyyah.hamiduddin@gmail.com. Dr. Miller and Dr. Glenn are Contributing Editors to the Journal of Clinical Orthodontics.