CASE REPORT
Nonsurgical Treatment of Anterior Crossbite in a Cleft Lip and Palate Patient Using a Fan-Type Rapid Palatal Expander and Fixed Appliances
Surgical treatment of cleft lip and palate starts at an early age with cheiloplasty (3 months old) and palatoplasty (10-12 months old), followed in the early mixed detention by alveolar bone grafting. These surgical procedures can help achieve esthetic objectives but may hamper maxillary transverse and sagittal growth. That usually results in maxillary retrusion and incisor retroclination, often creating a Class III malocclusion and anterior crossbite.1,2 Additionally, there is a greater tendency toward a hyperdivergent pattern.3
In cleft lip and palate patients, the maxillary transverse deficiency is often more pronounced in the anterior region, affecting the intercanine width. A fan-type rapid palatal expander (RPE) has been suggested because of the differential opening of the screw in the anterior region, which can avoid side effects such as molar tipping and posterior expansion.4,5
This report demonstrates the benefits of a fan-type RPE in nonsurgical treatment of a young patient with a skeletal Class III malocclusion and anterior crossbite who had previously undergone surgery to repair a cleft lip and palate.
Diagnosis and Treatment Planning
A 13-year-old male presented with the chief complaint of a crooked bite (Fig. 1). The patient had undergone surgical corrective procedures for cleft lip and palate during childhood. He exhibited scar tissue on the upper left lip from the lip-repair surgery, additional scar tissue in the palatal region, left nasal-wing asymmetry, and elevation of the left nasal wing in smiling. The patient was in the permanent dentition, showing a Class I molar relationship, an anterior crossbite with a –5mm overjet, and a maxillary arch-length discrepancy of 7mm. The maxillary midline was deviated to the right, and the mandibular midline to the left. Severe crowding and retroclination of the upper incisors and buccal displacement of the upper right canine were also observed.
Similar articles from the archive:
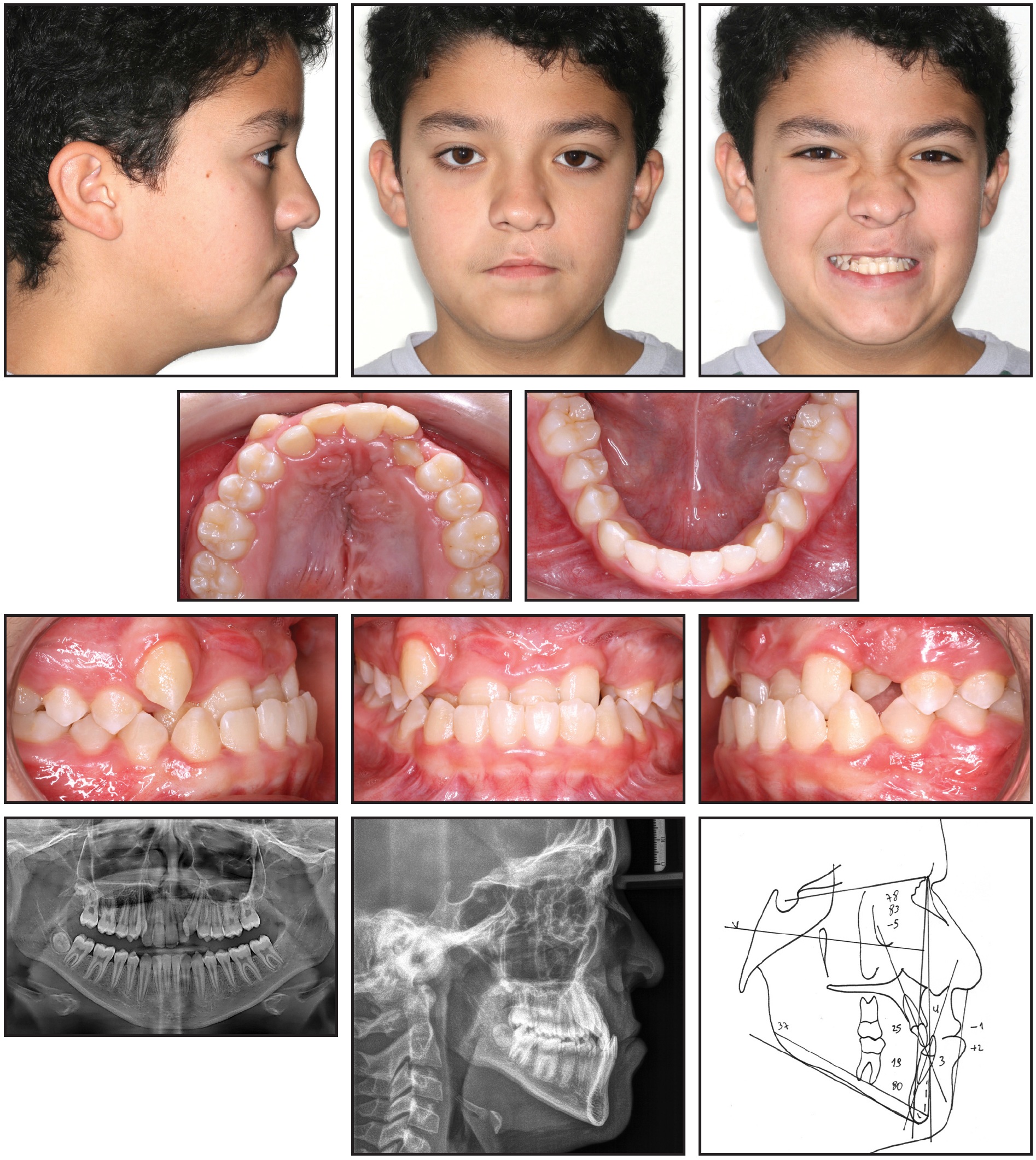
Fig. 1 13-year-old male patient with skeletal Class III pattern, dolichofacial tendency, maxillary and mandibular midline deviations, anterior crossbite with –5mm overjet, severe crowding and retroclination of maxillary incisors, and buccal displacement of upper right canine before treatment.
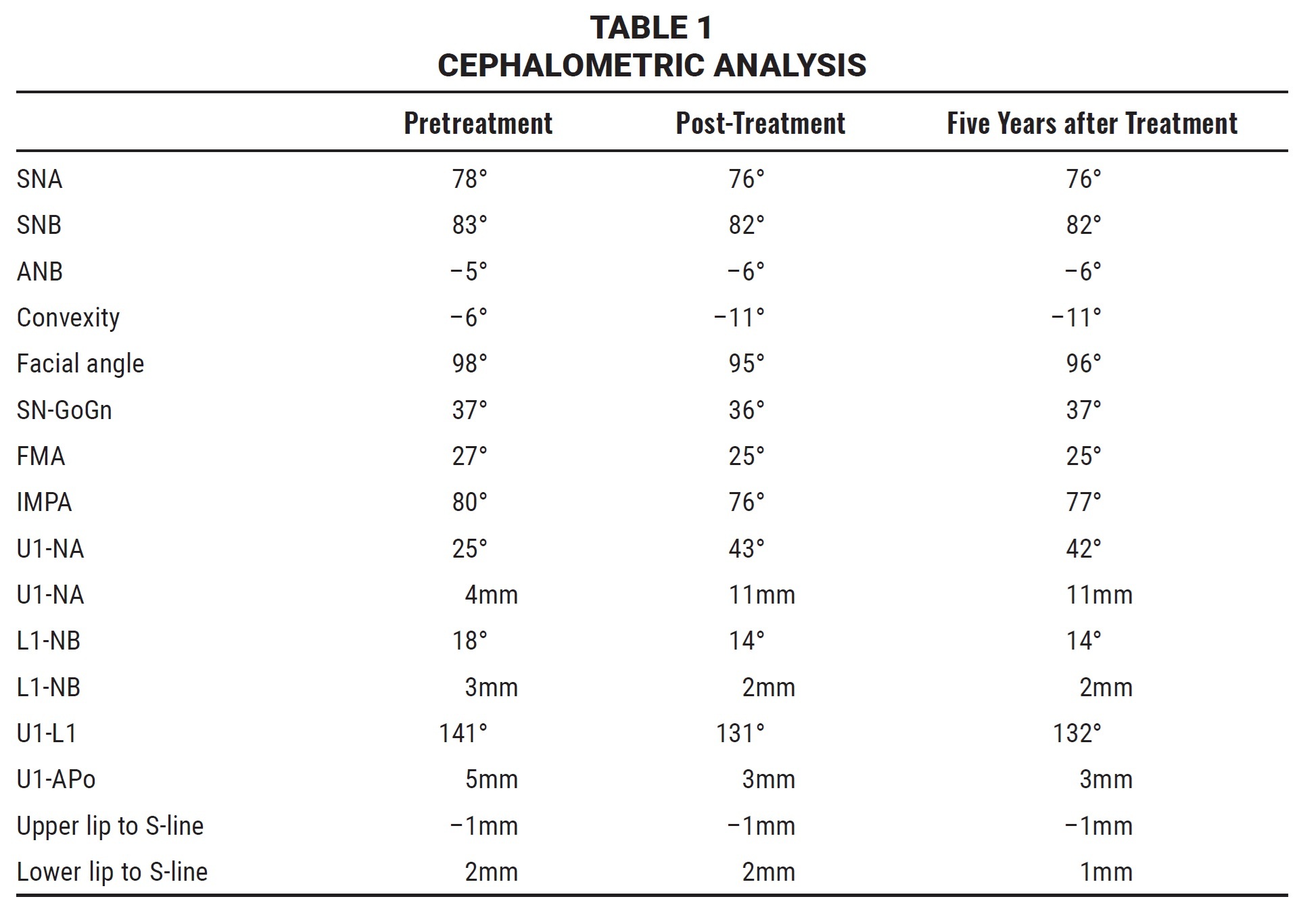
The panoramic radiograph revealed short upper central- and lateral-incisor roots and absence of the left third-molar germs. Cephalometric analysis (Table 1) indicated a skeletal Class III malocclusion (ANB = –5°), a retropositioned maxilla (SNA = 78°), and a forwardly displaced mandible (SNB = 83°). The patient also had a dolichofacial growth pattern (SN-GoGn = 37°), with well-positioned upper incisors (U1-NA = 25°, 4mm) and retroclined lower incisors (L1-NB = 18°, IMPA = 80°).
Treatment objectives were to correct the anterior transverse maxillary deficiency, resolve the anterior crossbite, improve facial balance, and establish an ideal occlusion.
The first option was to delay orthodontic treatment until the patient had finished growing, but this would have had a negative effect on his quality of life during adolescence.6 In addition, the malocclusion would likely have worsened, making surgical maxillary advancement imperative. A second option was to perform immediate orthodontic nonextraction treatment to improve the patient’s facial esthetics and to balance maxillomandibular growth, notably the lip relationship. The parents and the patient opted for this second alternative.
Treatment Progress
A banded fan-type RPE with an acrylic cover was prescribed to promote expansion of the anterior maxilla, where the transverse deficiency was more pronounced (Fig. 2A). The appliance was activated .5mm per day for 21 days until overcorrection of the posterior teeth was achieved (Fig. 2B). At that point, the expansion screw was fixed in place for six months of passive retention.
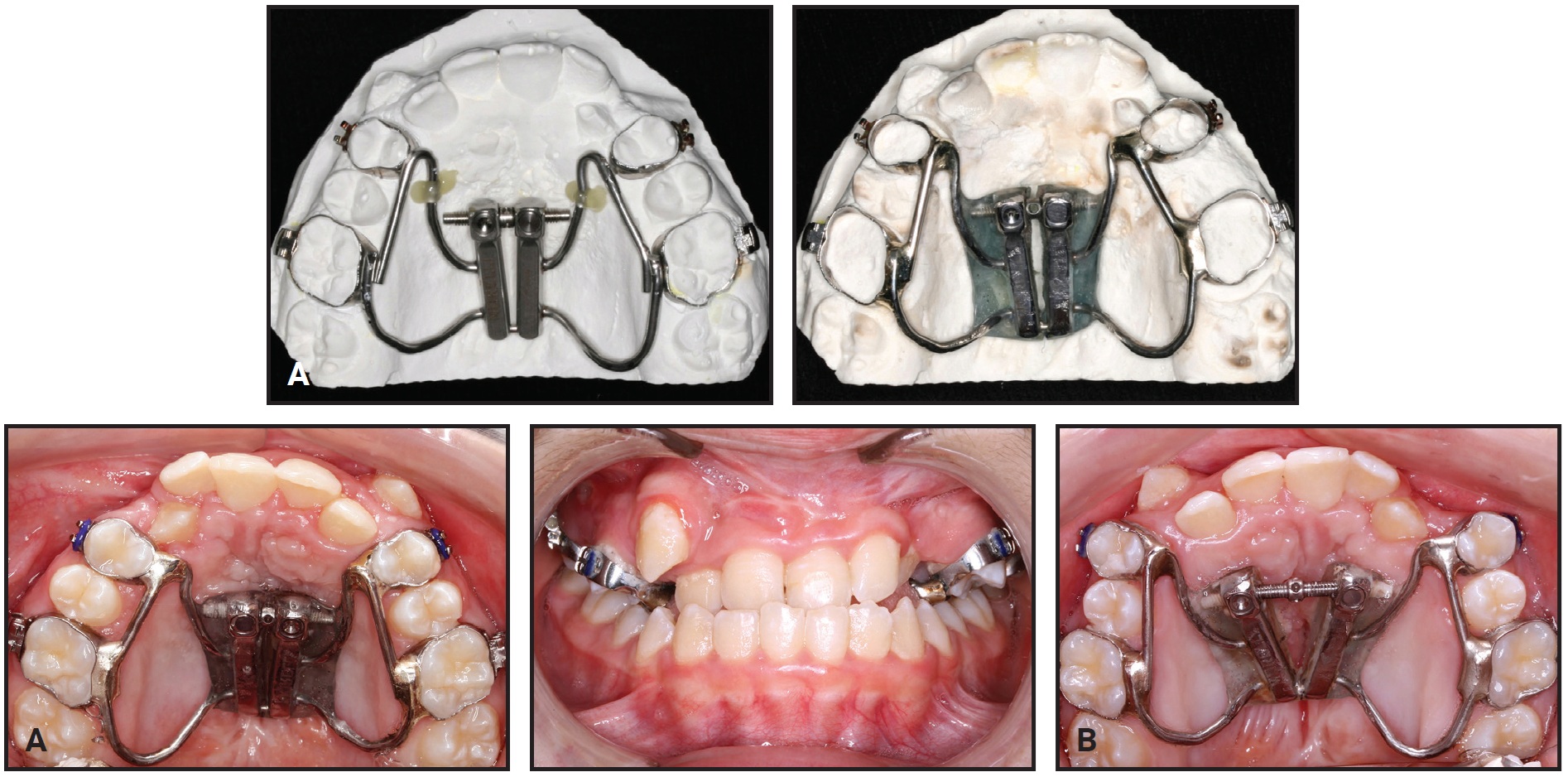
Fig. 2 A. Fan-type rapid palatal expander (RPE) inserted in maxillary arch. B. RPE activated .5mm per day for 21 days to achieve overcorrection of posterior teeth.
Once the active expansion was completed, .022" × .028" standard edgewise brackets were bonded in the maxillary arch, and an .014" nickel titanium archwire was placed from the upper left first molar to right central incisor (Fig. 3).

Fig. 3 After 21 days of active expansion, .022" × .028" standard edgewise brackets bonded in maxillary arch, and .014" nickel titanium archwire placed from upper left first molar to right central incisor.
The archwire sequence continued with .016", .018", and .020" stainless steel archwires. When the .020" archwire was in place, the maxillary midline shift was addressed with elastomeric chains (Fig. 4). The lower canines and premolars were bonded, and the lower first and second molars were banded for leveling and alignment of the posterior teeth with sectional mechanics to avoid proclination of the lower incisors. The lower archwire sequence involved .016", .018", and .020" stainless steel wires.
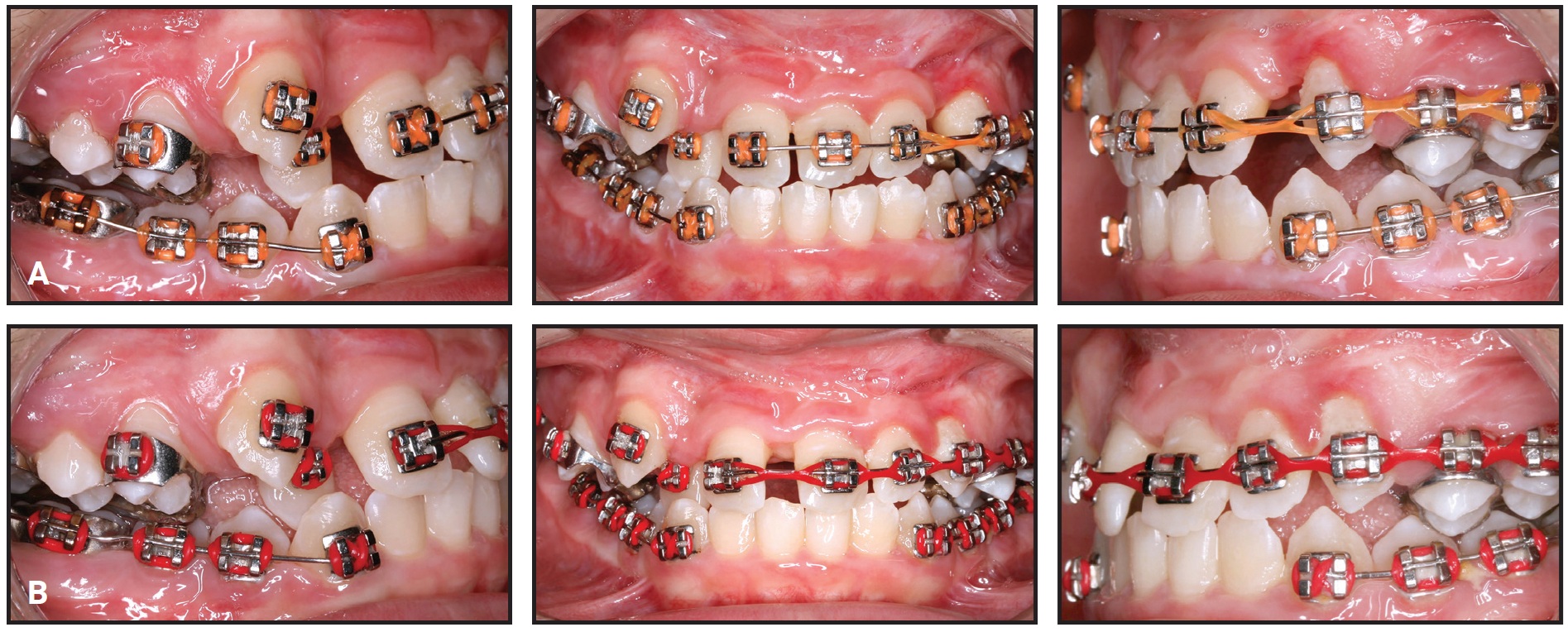
Fig. 4 A. After five months of treatment, .020" maxillary archwire inserted, with elastomeric chains added to address midline shift. Lower posterior teeth leveled and aligned with sectional mechanics to avoid proclination of lower incisors. B. After seven months of treatment, .019" × .025" upper and .020" segmented lower stainless steel archwires in place.
After the maxillary midline correction, an .012" nickel titanium upper archwire was placed from first molar to first molar. The archwire sequence then progressed to .016", .018", and .020" nickel titanium and .019" × .025" stainless steel, with 1st-, 2nd-, and 3rd-order bends placed in the finishing wire. Maxillary incisor torque was increased to compensate for the anterior crossbite. In the mandibular arch, brackets were bonded to the incisors, but a full archwire was not placed until the upper archwire reached .019" × .025" stainless steel (Fig. 5). Temporary miniscrews were inserted between the upper and lower right first molars and second premolars, and a sliding jig was used to distalize the lower right posterior teeth and correct the mandibular midline shift.
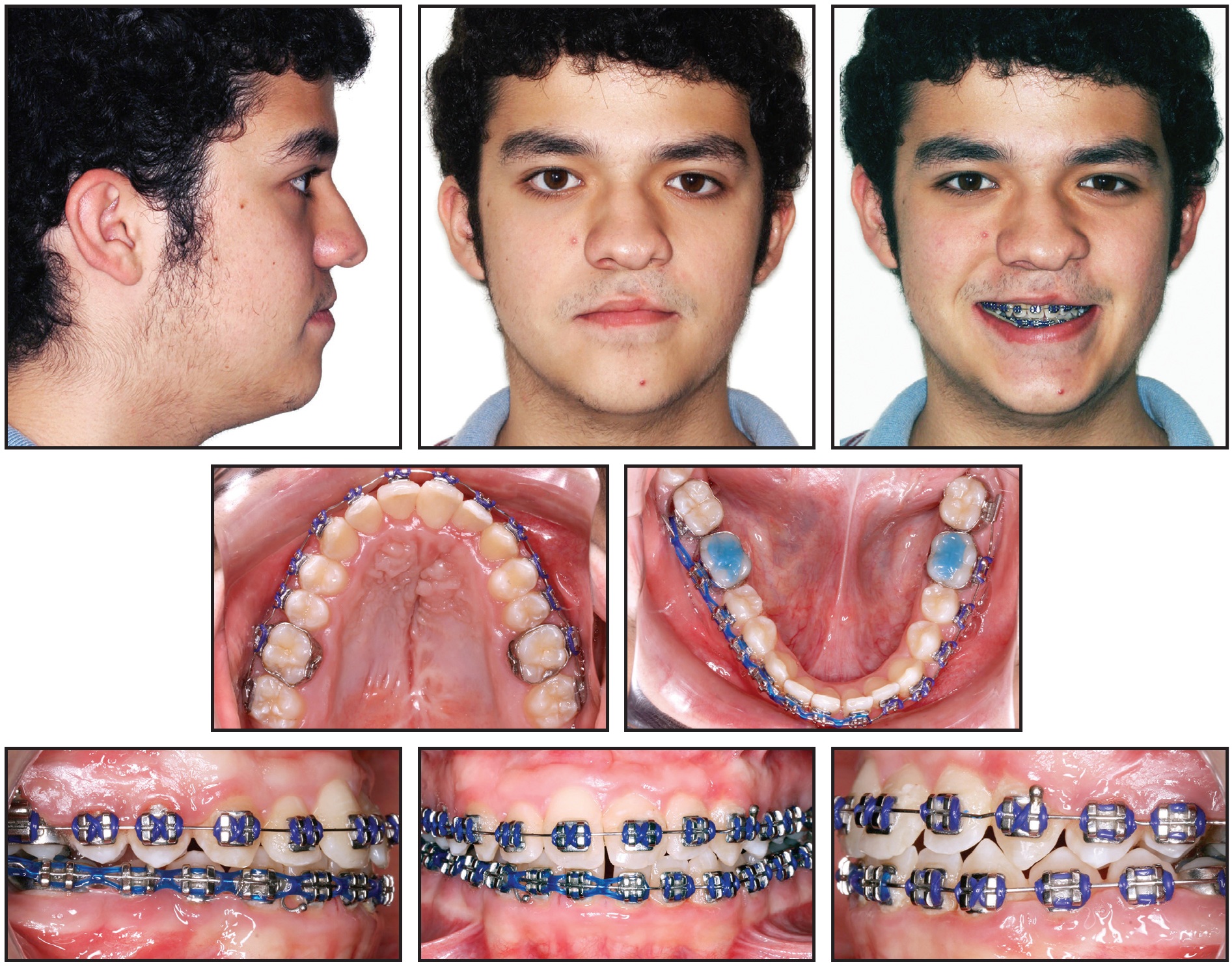
Fig. 5 After 22 months of treatment, .019" × .025" stainless steel archwires in place.
The sliding jig was removed after the midline correction, and the patient then wore settling elastics for intercuspation. Total treatment time was four years (Fig. 6A and 6B).
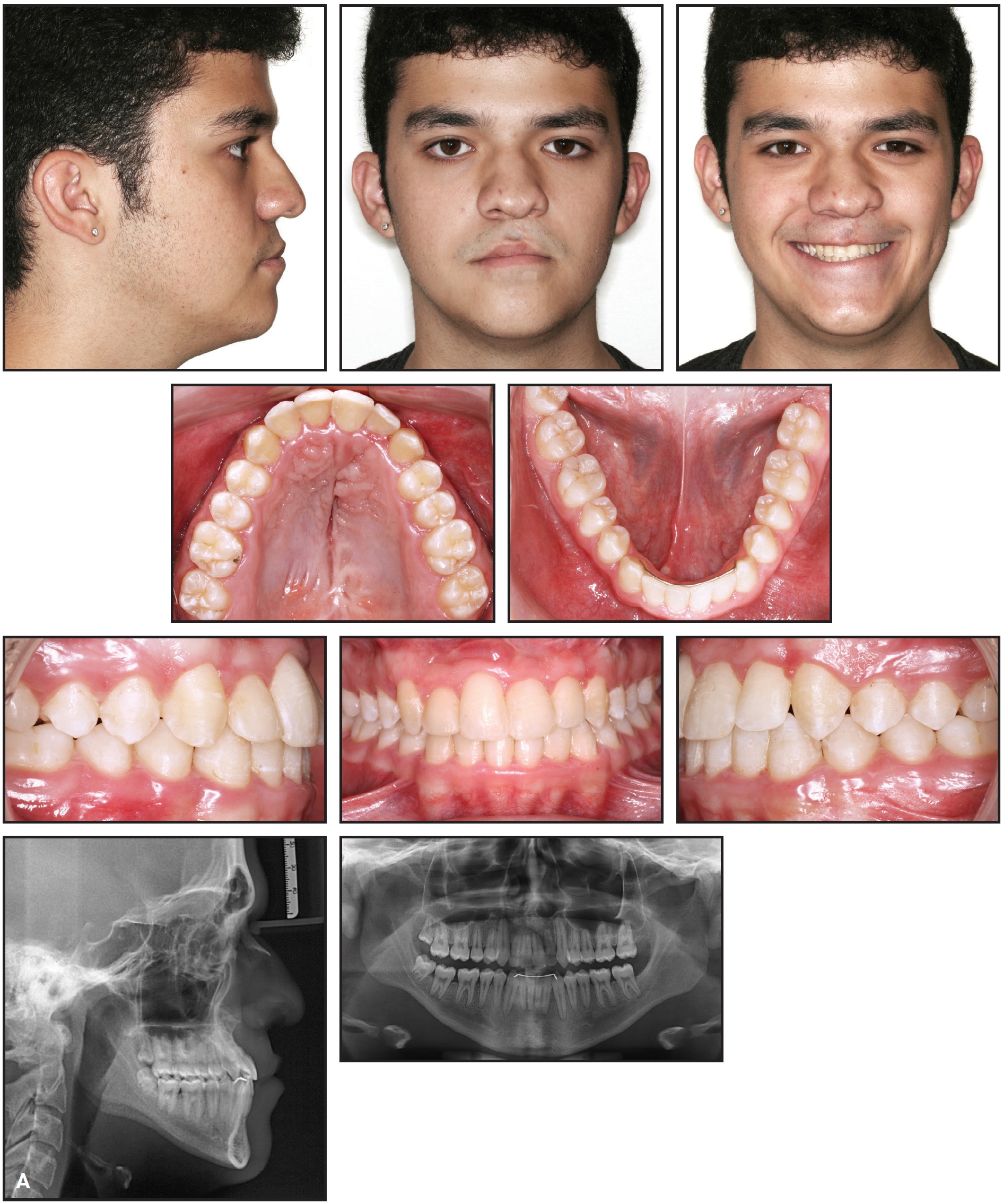
Fig. 6 A. Patient after four years of treatment (continued in next image).
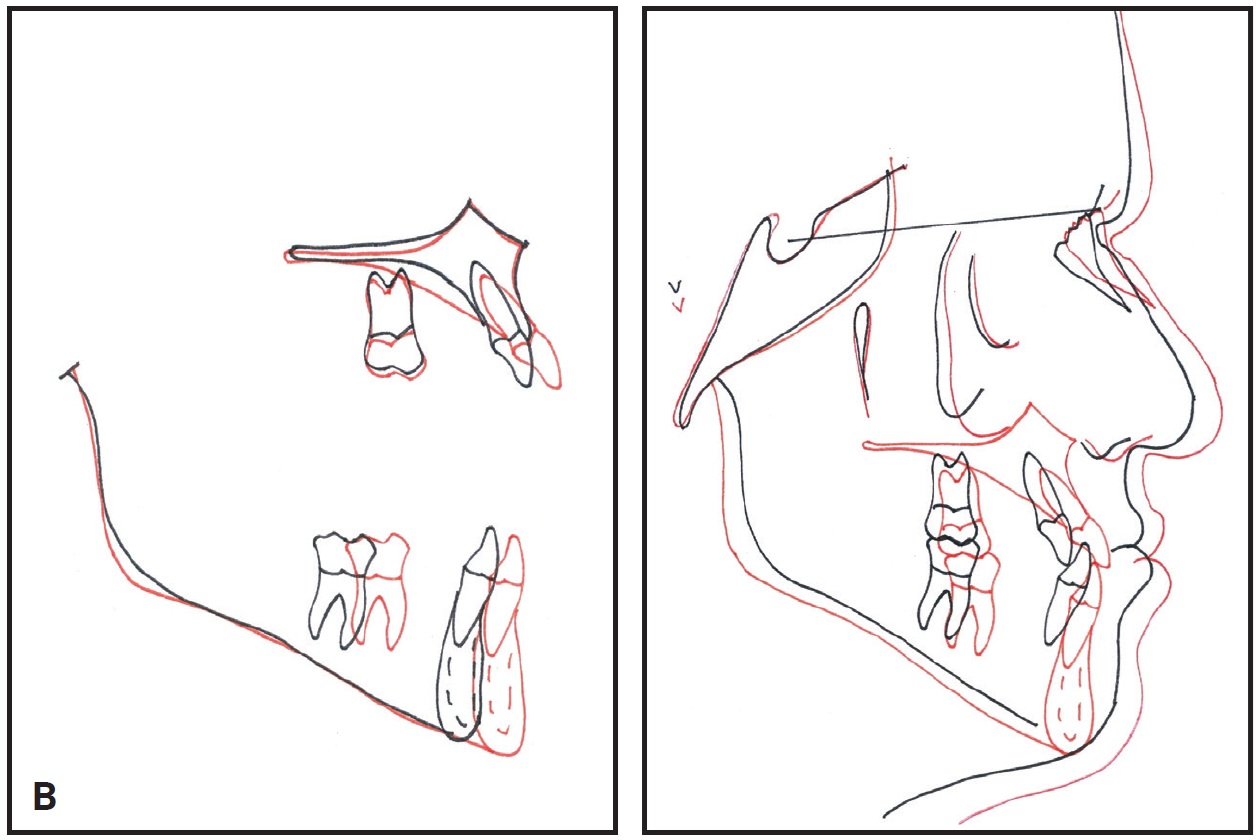
Fig. 6 (cont.) B. Superimposition of pretreatment (black) and post-treatment (red) cephalometric tracings.
A mandibular 3-3 lingual retainer wire was bonded. A wraparound retainer was used in the upper arch full-time for the first year, at night only for the next six months, and on alternating days for the subsequent six months, for a total of two years.
Treatment Results
After four years of treatment, Class I molar and canine relationships were obtained, and the anterior crossbite, midline shifts, overjet, and overbite were corrected. The anterior transverse expansion resulted in a more pleasant smile. Facial esthetics were improved, and the concave profile was balanced.
The panoramic radiograph evidenced root parallelism and confirmed the absence of the left third molars and root resorption of the upper central incisors. Cephalometric analysis (Table 1) demonstrated the effects of treatment: the skeletal Class III relationship (ANB = −6°) and the vertical pattern (SN-GoGn = 36°) were maintained, while the upper incisors were proclined and protruded (U1-NA = 43°, 11mm).
Five years after treatment, the facial and occlusal results were maintained (Fig. 7).
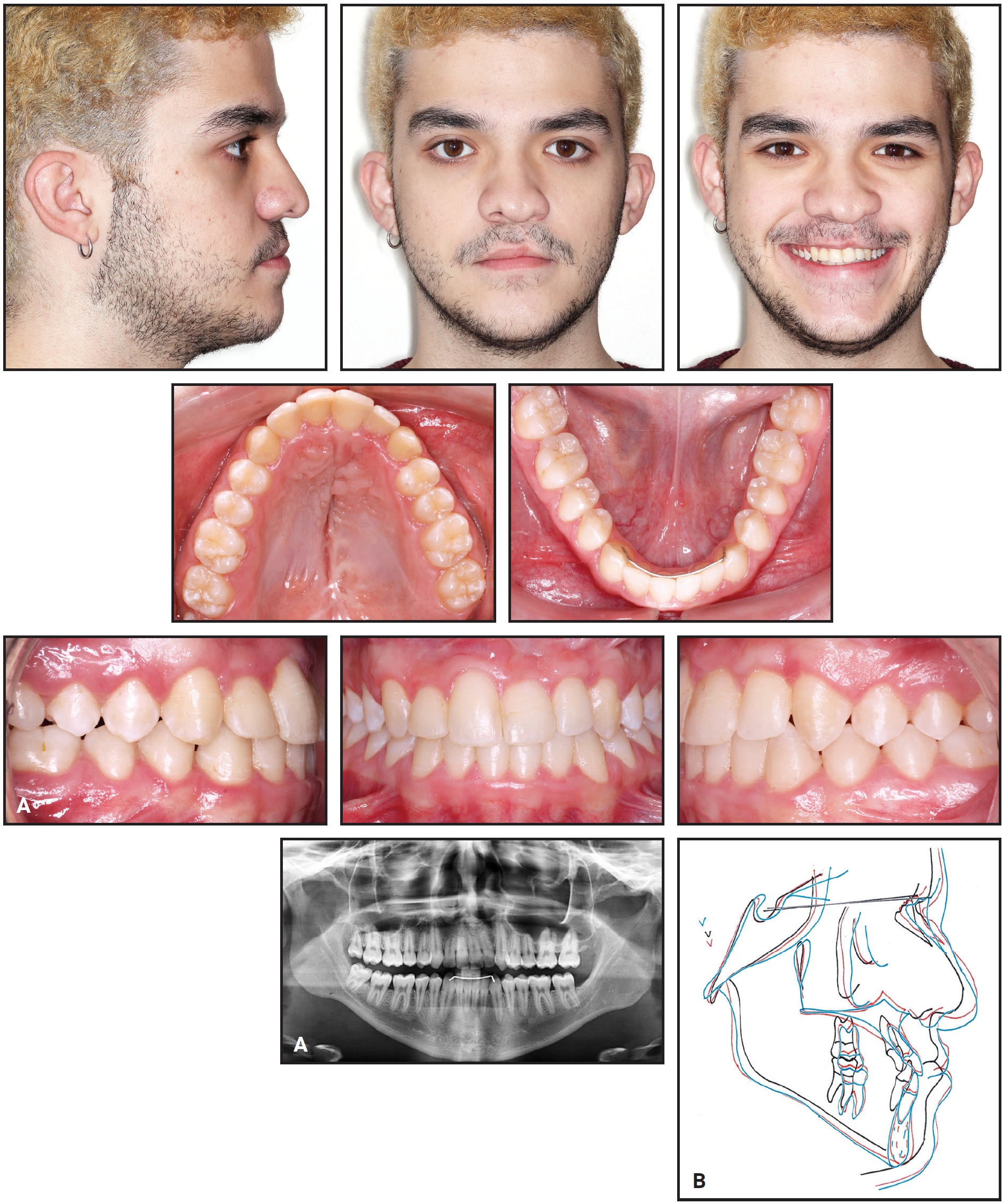
Fig. 7 A. Patient five years after treatment. B. Superimposition of pretreatment (black), post-treatment (red), and five-years-post-treatment (green) cephalometric tracings.
Discussion
In a patient with unilateral cleft lip and palate, the skeletal anterior crossbite and maxillary anterior transverse deficiency can be attributed more to the surgically repaired lip than to the surgically repaired palate, because the pressure exerted by the scar tissue of the lip causes atresia of the premaxilla.7 The maxillary bone fails to grow normally and tends to narrow, which affects its relationship with the mandibular basal bone over time.8 A conventional Hyrax* expander is unsuitable for such a case, in which a posterior crossbite is not present and only the premaxilla is affected.1,7 A fan-type palatal expander produces a more V-shaped opening in the anterior region,5,9 with the further advantages of moving the maxilla downward and forward and increasing labial tipping of the incisors.4
This report shows how such effects, typically associated with a fixed appliance, can be used in compensatory treatment of a young patient in the permanent dentition. Significant expansion was achieved, palatal root torque of the upper incisors was accentuated, and the lower incisors were retracted to normalize the overjet while the patient was still growing. Additionally, there was no clockwise rotation of the mandible, and the patient’s vertical growth pattern was not accentuated.
An estimated 20-60% of the patients who visit cleft palate centers in North America will eventually need orthognathic surgery for maxillary advancement.10 That option would have corrected the sagittal maxillomandibular discrepancy in our case, but the patient and parents declined surgical treatment. Considering the patient’s age and lack of posterior crossbite, the orthodontic compensation of the anterior teeth facilitated anterior correction and helped to improve facial balance. No alterations occurred in the intermaxillary relationship (ANB = −6°), and the results remained stable over time, as seen in the five-year follow-up.
Patients with unilateral cleft lip and palate tend to present upper incisors with an unfavorable crown-root ratio, which could be caused by either short roots or long crowns; in such cases, both sides (cleft and noncleft) are affected,11 making orthodontic treatment more challenging. Because of this biological limitation, a substantial amount of upper-incisor tip and torque was needed in our case, leading to apical root resorption.
These patients also tend to have shorter and more retrusive upper lips and more protrusive lower lips—a pattern that usually worsens with growth, exacerbating the facial imbalance.12 In the present case, the upper lip position was maintained by proclination and protrusion of the upper incisors.
FOOTNOTES
- *Registered trademark of Dentaurum, Inc., Newtown, PA; www.dentaurum.com.
REFERENCES
- 1. Capelloza Filho, L.; Normando, A.D.; and da Silva Filho, O.G.: Isolated influences of lip and palate surgery on facial growth: Comparison of operated and unoperated male adults with UCLP, Cleft Palate Craniofac. J. 33:51-56, 1996.
- 2. Silva Filho, O.G.; Valladares Neto, J.; Capelloza Filho, L.; and de Souza Freitas, J.A.: Influence of lip repair on craniofacial morphology of patients with complete bilateral cleft lip and palate, Cleft Palate Craniofac. J. 40:144-153, 2003.
- 3. Seo, Y.J.; Park, J.W.; Kim, Y.H.; and Baek, S.H.: Initial growth pattern of children with cleft before alveolar bone graft stage according to cleft type, Angle Orthod. 81:1103-1110, 2011.
- 4. Çörekçi, B. and Göyenç, Y.B.: Dentofacial changes from fan-type rapid maxillary expansion vs traditional rapid maxillary expansion in early mixed dentition, Angle Orthod. 83:842-850, 2013.
- 5. Figueiredo, D.S.; Bartolomeo, F.U.; Romualdo, C.R.; Palomo, J.M.; Horta, M.C.; Andrade Jr., I.; and Oliveira, D.D.: Dentoskeletal effects of 3 maxillary expanders in patients with clefts: A cone-beam computed tomography study, Am. J. Orthod. 146:73-81, 2014.
- 6. Ruiz-Guillén, A.; Suso-Ribera, C.; Romero-Maroto, M.; Gallardo, C.; and Peñacoba, C.: Perception of quality of life by children and adolescents with cleft lip/palate after orthodontic and surgical treatment: Gender and age analysis, Prog. Orthod. 22:10, 2021.
- 7. Long, R.E. Jr.; Semb, G.; and Shaw, W.: Orthodontic treatment of the patient with complete clefts of lip, alveolus, and palate: Lessons of the past 60 years, Cleft Palate Craniofac. J. 37:533.3-533.13, 2000.
- 8. Lacerda Filho, R.H.W.; Ramos, T.B.; Lacerda Filho, V.V.L.; Chaves, A.M.B.; Furtado, P.G.C.; and Ozawa, T.O.: Facial growth changes induced by orthodontic treatment in patients with unilateral cleft lip and palate, J. Craniofac. Surg. 29:1495-1500, 2018.
- 9. Doruk, C.; Bicakci, A.A.; Basciftci, F.A.; Agar, U.; and Babacan, H.: A comparison of the effects of rapid maxillary expansion and fan-type rapid maxillary expansion on dentofacial structures, Angle Orthod. 74:184-194, 2004.
- 10. Hathaway, R.; Daskalogiannakis, J.; Mercado, A.; Russell, K.; Long, R.E. Jr.; Cohen, M.; Semb, G.; and Shaw, W.: The Americleft study: An inter-center study of treatment outcomes for patients with unilateral cleft lip and palate, Part 2: Dental arch relationships, Cleft Palate Craniofac. J. 48:244-251, 2011.
- 11. Al-Jamal, G.A.; Hazza’a, A.M.; and Rawashdeh, M.A.: Crown-root ratio of permanent teeth in cleft lip and palate patients, Angle Orthod. 80:1122-1128, 2010.
- 12. Moreira, I.; Suri, S.; Ross, B.; Tompson, B.; Fischer, D.; and Lou, W.: Soft-tissue profile growth in patients with repaired complete unilateral cleft lip and palate: A cephalometric comparison with normal controls at ages 7, 11, and 18 years, Am. J. Orthod. 145:341-358, 2014.
-
 DR. PITHON
DR. PITHON -
 DR. REYES
DR. REYES -
 DR. MOTA-JÚNIOR
DR. MOTA-JÚNIOR -
 DR. CASTILHOS
DR. CASTILHOS -
 DR. TANAKA
DR. TANAKA
Dr. Pithon is a Professor, Southwest Bahia State University, Jequié, Bahia, Brazil. Dr. Reyes is a Professor, Department of Periodontology and Oral Implantology, Pontificia Universidad Católica Madre y Maestra, Santo Domingo, Dominican Republic. Dr. Mota-Júnior is a Professor, Juiz de Fora Federal University, and in the private practice of orthodontics in Juiz de Fora, Minas Gerais, Brazil. Dr. Castilhos is a student and Dr. Tanaka is a Professor, Graduate Dentistry Program, School of Life Sciences, Pontifícia Universidade Católica do Paraná, 1155 R. Imaculada Conceição, 80215-901 Curitiba, Paraná, Brazil. E-mail Dr. Tanaka at tanakaom@gmail.com.
