Effective Vertical Control of the Entire Maxillary Arch with a Palatal TAD-Supported Appliance
Vertical control is of critical importance in orthodontic treatment, especially for patients with hyperdivergent growth patterns.1 Treatment mechanics are more likely to extrude the posterior segments in these patients, owing to their weaker bite forces and reduced masticatory muscle volumes.2 Leveling a steep occlusal plane with preadjusted brackets in a hyperdivergent patient may result in differential moments and extrusive forces on the molars.3
Proper diagnosis of the vertical growth pattern and avoidance of extrusive mechanics are the keys to maintaining the profile and sagittal relationship in such a case. Various adjunctive treatment modalities, including high-pull headgear and vertical holding appliances, have been used to control vertical growth of the maxilla and prevent downward and backward rotation of the mandible.4-7 More recently, the introduction of temporary anchorage devices (TADs) has expanded the boundaries of tooth movement. Intrusion of maxillary molars and posterior buccal segments with skeletal anchorage can promote counterclockwise rotation of the mandible, increased chin projection, a more esthetic soft-tissue profile, and improved lip-incisor and occlusal relationships.
When selecting the biomechanical system for TAD-based intrusion, it is important to consider such occlusal characteristics as contacts, occlusal plane divergence, and the presence or absence of open bite. For balanced intrusion, the line of force application should pass through the center of resistance (CR) of the unit being intruded, whether a single tooth or an entire segment. Finite element analysis of posterior segmental intrusion (first premolars through second molars) showed that placing two buccal and two palatal mini-implants in the interproximal bone between the premolars and molars in each segment produced the least amount of tipping and canting.8 On the other hand, adding mini-implants not only increased patient discomfort and pain, but also increased the likelihood of mini-implant failure. Replacing the palatal mini-implants with one or two palatal arches resulted in varying degrees of buccolingual and mesiodistal tipping. In another study reporting successful treatment of growing hyperdivergent patients with TADs, maxillary posterior segmental intrusion was effected by using two palatal mini-implants and a rapid palatal expander (RPE) to prevent lingual tipping.9 The mandible was rotated forward and soft- and hard-tissue convexities were reduced, leading to the conclusion that growing hyperdivergent patients benefited from intrusion or relative intrusion (controlling the vertical dimension), depending on the amount of growth remaining.
Similar articles from the archive:
- Surgical-Orthodontic Correction of Skeletal Class III Malocclusion with Vertical Maxillary Excess December 2016
- CASE REPORT Surgical-Orthodontic Treatment of Class II Malocclusion with Maxillary Vertical Excess June 2009
- Biomechanical Considerations in the Correction of Anterior Open Bite with Maxillary Skeletal Plates January 2015
The possibility of modifying the line of force application during treatment—that is, applying separate forces of different magnitudes and directions to the molar and premolar areas—and incorporating the anterior segment to achieve full-arch intrusion with a minimum number of mini-implants has rarely been addressed. This article documents the management of maxillary vertical growth by intrusion of the entire maxillary dentition to achieve forward rotation of the mandible, increased chin projection, and reduced incisor display.
Case Report
A 14-year-old female presented with the chief complaint of crowding (Fig. 1). She had a mildly convex facial profile with excessive lower anterior facial height and obtuse nasolabial and mentolabial angles, as well as a consonant smile arc with 1mm of gingival display in smiling. Intraoral examination found a 3mm overjet, a 1mm overbite at the incisor level, 2mm of open bite in the canine regions, and Class I molar and canine relationships.

Fig. 1 14-year-old female patient with excessive lower anterior facial height, hyperdivergent growth pattern, and Class I molar and canine relationships before treatment.
Cephalometric analysis indicated a slightly convex hard-tissue profile and mildly hyperdivergent growth pattern (Table 1). Vertically, the mandibular plane angle was slightly increased, and the distances from the upper and lower incisor apices to the palatal and mandibular planes were excessive. The upper and lower incisor inclinations were normal.

Treatment started with leveling and alignment of both arches, using an archwire sequence from .014" nickel titanium to .019" × .025" nickel titanium. Full-time vertical seating elastics were prescribed in the canine to premolar and incisor regions to achieve an ideal overbite. Moderate compliance with the elastics improved as treatment progressed.
Upper and lower .016" × .022" TMA* archwires were inserted prior to the finishing phase. After 17 months of treatment, we noted an increased gingival display in smiling (3mm), lip incompetency (4mm of lip separation at rest), mentalis muscle strain, and a retrusive chin position (Fig. 2).

Fig. 2 A. After 17 months of leveling and alignment, showing excessive incisor and gingival display, increased interlabial gap, and reduced chin projection, with adequate occlusal relationships. B. Superimposition of pretreatment (black) and progress (blue) cephalometric tracings, confirming backward mandibular rotation and reduced chin prominence.
The lateral cephalometric superimposition showed incisor extrusion and clockwise rotation of the mandible due to vertical growth of the maxilla and slight extrusion of the molars during treatment. The clockwise mandibular rotation had increased the interlabial gap and convexity of the facial profile and reduced the chin projection. After reevaluation, the treatment objectives were to reduce the gingival display and interlabial gap, thus improving smile esthetics, as well as to reduce lower anterior facial height by counterclockwise mandibular rotation and control of maxillary vertical growth.
Two possible treatment modalities were presented to the patient and her mother. The first option was a combination of orthodontics and orthognathic surgery to address the vertical skeletal problem, using a Le Fort I osteotomy to impact the maxilla and a genioplasty for chin advancement. The major concerns with this approach were its cost and the risks associated with surgery. The alternative was to use TADs to intrude the maxillary dentition, reducing gingival display and encouraging forward mandibular rotation. The family was opposed to orthognathic surgery and accepted the second option.
After obtaining informed consent, we placed two 1.8mm × 8mm mini-implants** in the palatal shelves, along a line extending between the first and second premolars and adjacent to the midpalatal suture (Fig. 3A). A customized appliance was designed with four power arms fabricated from .040" stainless steel wire and soldered to O-caps.** The appliance was affixed to the mini-implant heads using glass ionomer cement,*** and the maxillary posterior teeth were splinted with an .019" × .025" stainless steel archwire. From the lingual aspect, the appliance also included a Hyrax† screw soldered to the first-molar bands, occlusal rests on the second molars, and two rigid bars extending anteriorly with pads bonded to the first and second premolars. Buttons were bonded to the lingual aspects of both upper canines, and bilateral intrusive forces of 150-200g were applied with elastomeric chains from the power arms to the hooks on the appliance and the canine buttons (Fig. 3B,C).
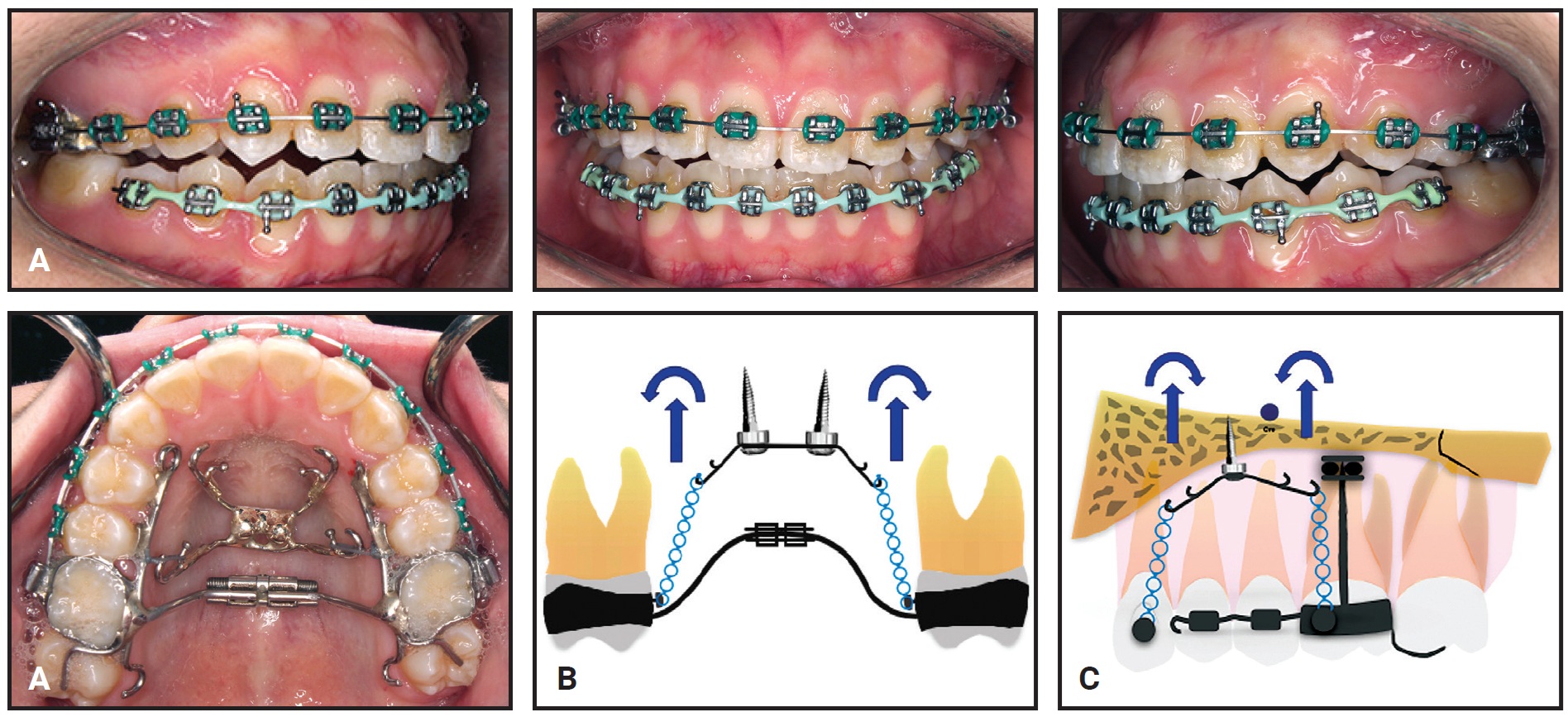
Fig. 3 A. Customized splint for maxillary dentition provides skeletal anchorage for intrusion. B. Intrusive forces and moments generated tend to constrict maxillary arch. C. Intrusive forces and moments generated tend to tip maxillary arch. Anterior force on canines intrudes incisors and reduces gummy smile simultaneously with posterior intrusion.
A smooth progression of maxillary intrusion was obtained by titrating the anterior or posterior intrusive forces as needed to control the occlusal plane (Fig. 4).
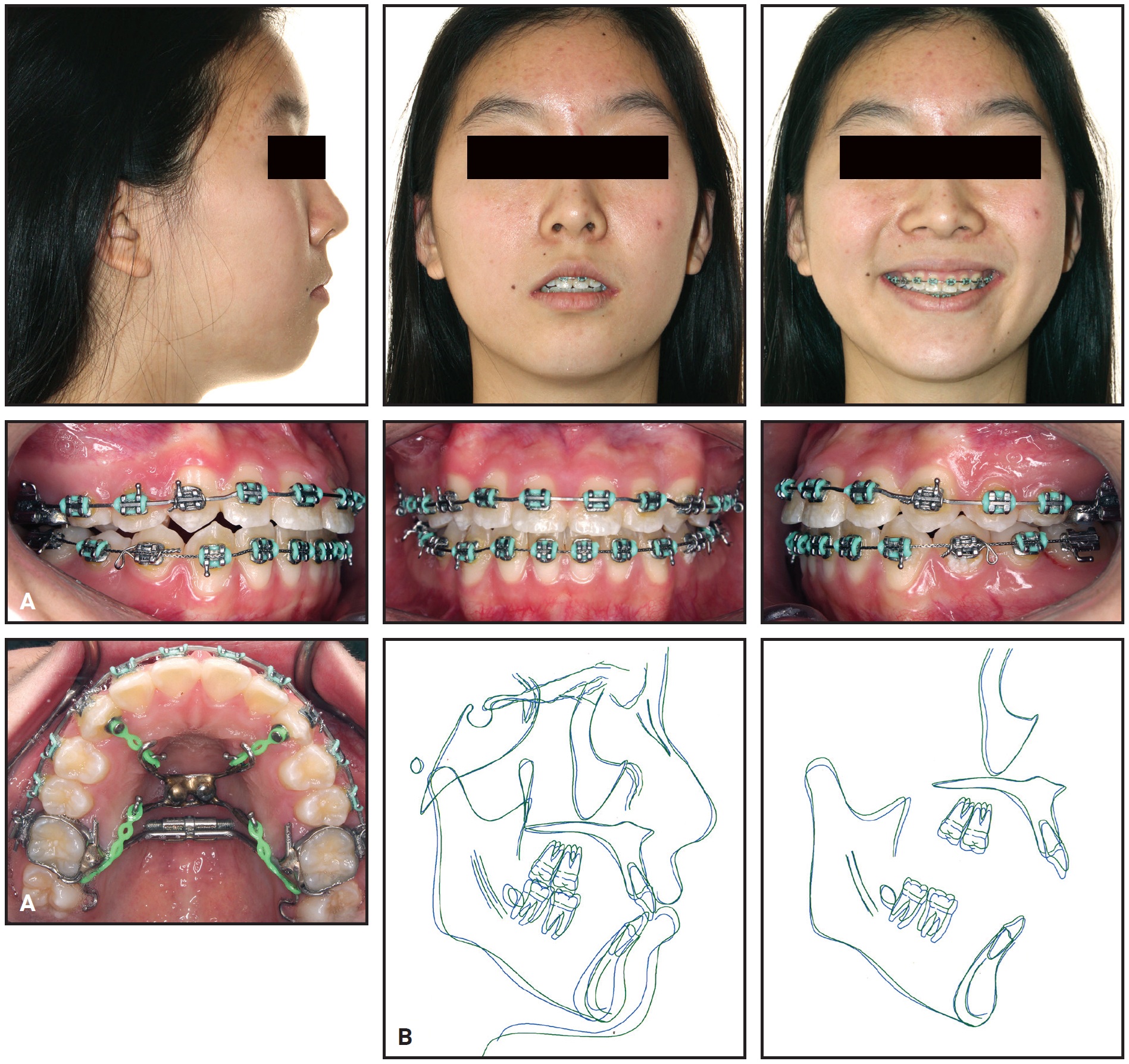
Fig. 4 A. After eight months of intrusion. B. Superimposition of pre-intrusion (blue) and post-intrusion (green) cephalometric tracings.
About 14 months later, 20° of labial crown torque was added to the upper canines to compensate for the torque changes that had occurred during intrusion. The finishing phase was completed using .017" × .025" TMA archwires, with the occlusal rests and extension arms cut off to allow settling of the occlusion.
After 42 months of treatment, the appliances were debonded and the mini-implants were removed (Fig. 5A).
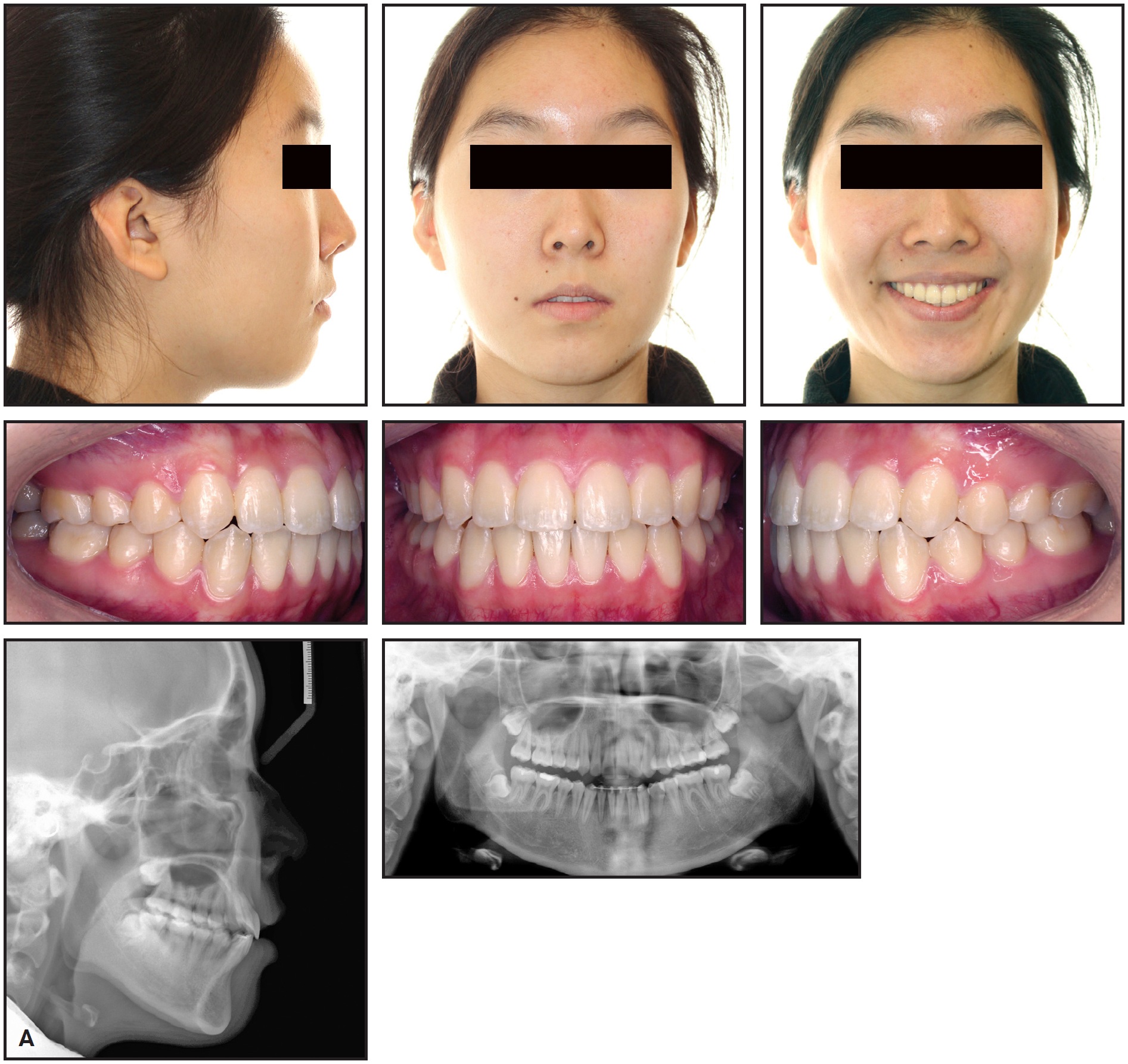
Fig. 5 A. Patient after 42 months of treatment (continued in next image).
A lower 3-3 lingual retainer was bonded, and a vacuformed upper retainer was delivered.
Post-treatment records showed a significant improvement in smile esthetics, correction of the excessive gingival display, reduction of the interlabial gap, and an increase in chin projection. Ideal overjet and overbite were achieved, and the Class I canine and molar relationships were maintained. The panoramic radiograph demonstrated adequate root parallelism with no evidence of substantial apical root resorption. Cephalometric analysis confirmed the increased chin prominence (Pg-NA perp) and reduced mandibular plane angle (MP-SN) due to counterclockwise rotation of the mandible after maxillary intrusion (Table 1). The distance from the upper molars and incisors to the nasal floor was reduced, and the upper and lower incisor inclinations were maintained.
Treatment with the customized appliance resulted in significant intrusion of the maxillary dentition and control of maxillary vertical growth, with counterclockwise rotation of the mandible and improvements in pogonion and soft-tissue chin position (Fig. 5B). The vertical growth of the ramus contributed to extrusion of the lower molars and incisors.
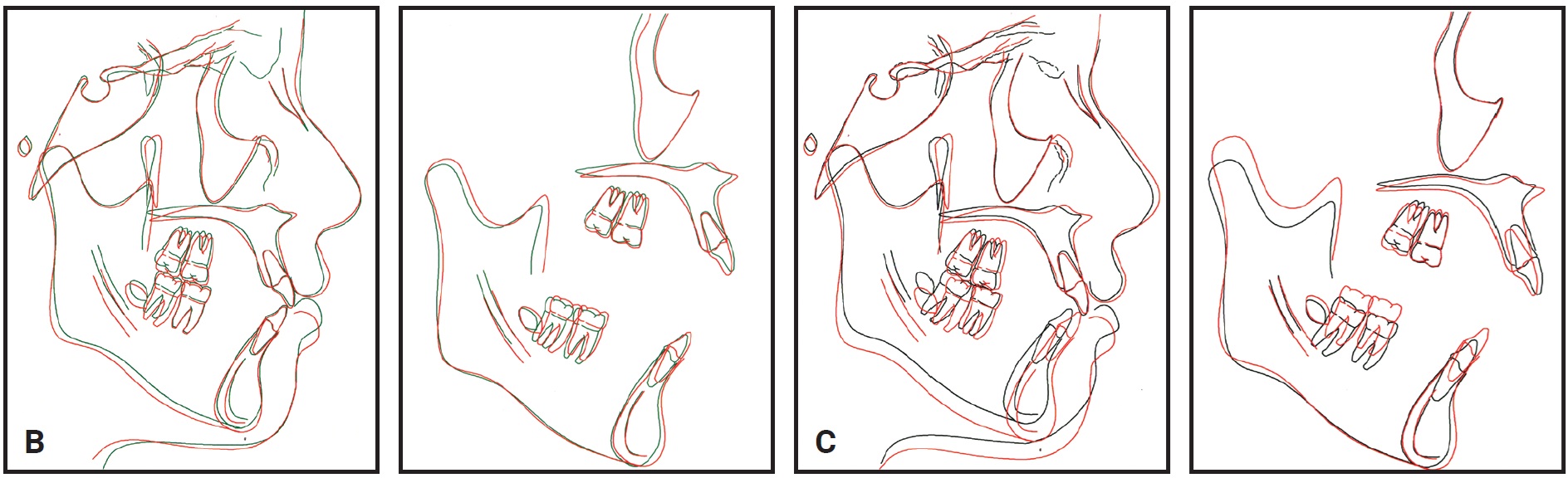
Fig. 5 (cont.) B. Superimposition of post-intrusion (green) and post-treatment (red) cephalometric tracings. C. Superimposition of pretreatment (black) and post-treatment (red) cephalometric tracings.
The vertical growth of the ramus contributed to extrusion of the lower molars and incisors.
Discussion
This case—a Class I malocclusion with a mildly hyperdivergent growth tendency—did not appear to be complex at first. After 17 months of leveling and alignment, however, we observed significant vertical growth of the maxilla, extrusion of the maxillary dentition, and clockwise rotation of the mandible due to an unfavorable growth pattern and extrusive mechanics. The increased vertical dimension resulted from extrusion of the lower premolars and molars after the lower curve of Spee had been leveled with continuous archwires. Extrusion of the upper and lower anterior teeth and the increased gingival display were attributable to two factors: elevated palatal cusps on the upper posterior teeth following arch expansion and concomitant vertical forces created by elastics intended to prevent bite opening. Since vertical ramal growth was insufficient to compensate for backward rotation of the mandible, the cumulative side effects of the mechanics required a modified treatment approach. Intrusion of the entire maxillary arch was incorporated into the treatment plan to encourage forward mandibular autorotation and to address the lip incompetency and excessive gingival display in smiling.
Buccal or palatal TADs have been used to support intrusion of the posterior teeth and correction of anterior open bite, especially in adult patients.10,11 From a biomechanical perspective, to intrude the entire maxillary dentition, the appliance design should allow the application of force vectors of different magnitudes in multiple directions. In this case, the cemented appliance with power arms and the modified RPE with hooks for force application provided the versatility and rigidity needed to achieve full-arch intrusion with only two palatal TADs.
The modified RPE was specifically designed to consolidate the upper right and left posterior segments and to prevent lingual tipping of the upper molars and premolars during intrusion. An RPE provided more stiffness and rigidity than a transpalatal arch would, considering the force required to intrude the full dentition. The expansion screw was a safety mechanism to mitigate any lingual tipping caused by the intrusive forces. In this patient, because some maxillary expansion was achieved with the archwires during leveling and alignment, no further expansion was needed during the intrusion phase.
The hooks of the customized appliance were positioned anteriorly and posteriorly to the CR of the maxillary dentition to counteract the moments generated by the applied forces, thus preventing any steepening of the occlusal plane during intrusion. Since the line of action of the intrusive force was lingual to the CR of the anterior teeth, labial crown torque was added to the archwires at the level of the canines to maintain their buccolingual inclination throughout treatment. A similar design, involving a rigid lingual arch splinted to all the upper teeth, was successfully used by Hong and colleagues to treat a gummy smile in an adult patient (except that the initial alignment was performed with clear aligners, rather than fixed appliances).12
In our case, the effective treatment changes resulted from a combination of maxillary intrusion, using the custom-designed appliance, and favorable vertical growth of the ramus. Cephalometric superimposition of the pre- and post-intrusion phases showed substantial intrusion of the entire maxillary dentition (Fig. 4B). About 3.4mm of incisor intrusion reduced the incisor display by 3mm; a 1.7mm intrusion of the first and second molars reduced the mandibular plane angle (MP-SN) by 1.9° and the facial convexity by 1.6° (Table 1). As a result of the mandibular autorotation, the bony chin projection increased by 3.8mm (Pg-NA perp). The positive orthopedic effects of intrusion in this case were similar to those reported by Buschang and colleagues.9 The results were maintained during the finishing stage by avoiding extrusive mechanics and emphasizing vertical control of the molars. Despite the significant amount of vertical growth during treatment, the mandibular plane angle, incisor display, and vertical molar position relative to the nasal floor were basically unchanged. This maxillary vertical control resulted in anterior positioning of the chin point.
The mandibular molars were not intruded in this case, but their vertical position was controlled with a rigid archwire. Regional superimposition of the mandible showed significant extrusion of the lower molars and incisors into the interocclusal space created by the vertical growth of the ramus and the intrusion of the maxillary molars. It has been suggested that intrusion of both upper and lower molars is necessary in patients with severe open bites.9,13 In this patient, however, because eruption of the upper molars was controlled during treatment, the entire compensatory eruption of the posterior teeth occurred in the mandibular arch. Moreover, since a successful outcome was observed after maxillary intrusion, the lower molars did not need to be intruded or maintained with skeletal anchorage. A more notable projection of the mandible, in conjunction with less maxillary molar intrusion, might have been achieved with the incorporation of mandibular TADs.
Soft-tissue changes following maxillary intrusion resulted in a significant enhancement of this patient’s smile esthetics. Lip incompetency was improved by the counterclockwise rotation of the mandible, and gingival display was reduced as the upper anterior teeth were intruded. In a non-growing patient, any long-term soft-tissue relapse after intrusion would be expected to be clinically insignificant.14
Conclusion
This case demonstrates that close monitoring of vertical growth during orthodontic treatment can play a pivotal role in achieving esthetic treatment results. Intrusion of the entire maxillary dentition using palatal TADs can be a viable treatment option to address the skeletal and soft-tissue problems associated with a hyperdivergent growth pattern.
FOOTNOTES
- *Trademark of Ormco Corporation, Orange, CA; www.ormco.com.
- **Unitek, trademark of 3M, Monrovia, CA; www.3M.com.
- ***Fuji ORTHO, trademark of GC America, Alsip, IL; www.gcamerica.com.
- †Registered trademark of Dentaurum, Inc., Newtown, PA; www.dentaurum.com.
REFERENCES
- 1. Gkantidis, N.; Halazonetis, D.J.; Alexandropoulos, E.; and Haralabakis, N.B.: Treatment strategies for patients with hyperdivergent Class II Division 1 malocclusion: Is vertical dimension affected? Am. J. Orthod. 140:346-355, 2011.
- 2. Ingervall, B. and Minder, C.: Correlation between maximum bite force and facial morphology in children, Angle Orthod. 67:415-422, 1997.
- 3. Ross, V.A.; Isaacson, R.J.; Germane, N.; and Rubenstein, L.K.: Influence of vertical growth pattern on faciolingual inclinations and treatment mechanics, Am. J. Orthod. 98:422-429, 1990.
- 4. Chung, C.H.; Tadlock, L.P.; Barone, N.; Pangrazio-Kulbersh, V.; Sabott, D.G.; Foley, P.F.; Trulove, T.S.; Park, J.H.; and Dugoni, S.A.: Common errors observed at the American Board of Orthodontics clinical examination, Am. J. Orthod. 152:139-142, 2017.
- 5. Deberardinis, M.; Stretesky, T.; Sinha, P.; and Nanda, R.S.: Evaluation of the vertical holding appliance in treatment of high-angle patients, Am. J. Orthod. 117:700-705, 2000.
- 6. Lee, J.; Miyazawa, K.; Tabuchi, M.; Kawaguchi, M.; Shibata, M.; and Goto, S.: Midpalatal miniscrews and high-pull headgear for anteroposterior and vertical anchorage control: Cephalometric comparisons of treatment changes, Am. J. Orthod. 144:238-250, 2013.
- 7. Sankey, W.L.; Buschang, P.H.; English, J.; and Owen, A.H. III: Early treatment of vertical skeletal dysplasia: The hyperdivergent phenotype, Am. J. Orthod. 118:317-327, 2000.
- 8. Cifter, M. and Sarac, M.: Maxillary posterior intrusion mechanics with mini-implant anchorage evaluated with the finite element method, Am. J. Orthod. 140:233-241, 2011.
- 9. Buschang, P.H.; Carrillo, R.; and Rossouw, P.E.: Orthopedic correction of growing hyperdivergent, retrognathic patients with miniscrew implants, J. Oral Maxillofac. Surg. 69:754-762, 2011.
- 10. Deguchi, T.; Kurosaka, H.; Oikawa, H.; Kuroda, S.; Takahashi, I.; Yamashiro, T.; and Takano-Yamamoto, T.: Comparison of orthodontic treatment outcomes in adults with skeletal open bite between conventional edgewise treatment and implant-anchored orthodontics, Am. J. Orthod. 139:S60-68, 2011.
- 11. Reichert, I.; Figel, P.; and Winchester, L.: Orthodontic treatment of anterior open bite: A review article—Is surgery always necessary? Oral Maxillofac. Surg. 18:271-277, 2014.
- 12. Hong, R.K.; Lim, S.M.; Heo, J.M.; and Baek, S.H.: Orthodontic treatment of gummy smile by maxillary total intrusion with a midpalatal absolute anchorage system, Kor. J. Orthod. 43:147-158, 2013.
- 13. Alsafadi, A.S.; Alabdullah, M.M.; Saltaji, H.; Abdo, A.; and Youssef, M.: Effect of molar intrusion with temporary anchorage devices in patients with anterior open bite: A systematic review, Prog. Orthod. 17:9, 2016.
- 14. Marzouk, E.S. and Kassem, H.E.: Long-term stability of soft tissue changes in anterior open bite adults treated with zygomatic miniplate-anchored maxillary posterior intrusion, Angle Orthod. 88:163-170, 2018.
-
 DR. AZAMI
DR. AZAMI -
 DR. NANDA
DR. NANDA -
 DR. URIBE
DR. URIBE
Dr. Azami is a former resident, Dr. Nanda is Professor Emeritus, and Dr. Uribe is an Associate Professor, Postgraduate Program Director and Division Chair, and Charles J. Burstone Endowed Professor, Division of Orthodontics, Department of Craniofacial Sciences, University of Connecticut School of Dental Medicine, Farmington, CT. E-mail Dr. Uribe at furibe@uchc.edu. Dr. Nanda is an Associate Editor and Dr. Uribe is a Contributing Editor of the Journal of Clinical Orthodontics.