CASE REPORT
Herbst Appliance Supported by Four Miniscrews
The Herbst* appliance is considered one of the most reliable fixed functional devices for treating Class II malocclusions without the need for patient compliance. It efficiently advances the mandible, achieving substantial and stable results in a high percentage of cases.1-13 The Herbst is also well accepted by patients14-16: O’Brien and colleagues showed that patients are more likely to cooperate with Herbst treatment than with a Twin Block.**11
Advantageous skeletal effects of Herbst treatment include enhancement of sagittal mandibular growth, anterior displacement of the mandibular arch, reduction of sagittal maxillary growth, posterior displacement of the maxillary arch, and TMJ remodeling.13,17 On the other hand, the appliance’s dental effects—proclination of the mandibular incisors and palatal inclination of the upper incisors—tend to limit the potential for mandibular advancement.18,19
To combat these side effects, several modifications of the original Herbst design have been proposed.20,21 As far as we know, however, only the concomitant use of skeletal anchorage has effectively controlled lower incisor flaring.14-23 This case report demonstrates the use of four temporary anchorage devices (TADs) to mitigate the adverse dental effects of the Herbst appliance while correcting a Class II malocclusion.
Diagnosis and Treatment Plan
A 12-year-old male was referred by his dentist for orthodontic consultation. Clinical examination found a convex profile with a retrusive chin, excessive nasolabial angle, symmetrical mandible, and incompetent lips (Fig. 1).
Similar articles from the archive:
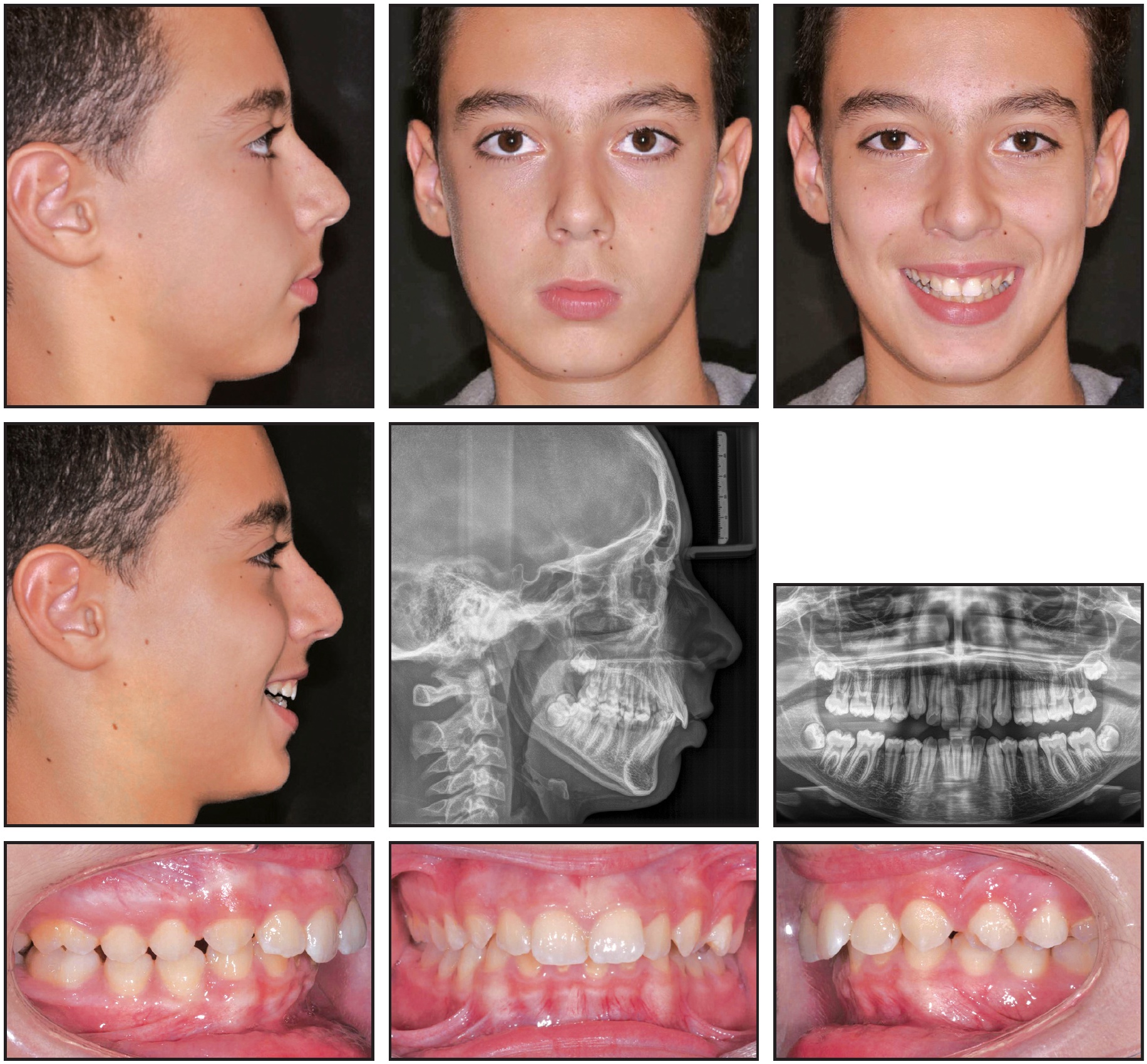
Fig. 1 12-year-old male patient with retrusive chin, incompetent lips, skeletal Class II malocclusion, and palatally inclined upper incisors before treatment.
A half-unit molar and canine Class II relationship on the right side and a full first-molar and half-unit Class II canine relationship on the left had resulted in a scissor bite in the left premolar area. The panoramic radiograph showed the presence of all permanent teeth with normal interdental bone levels.
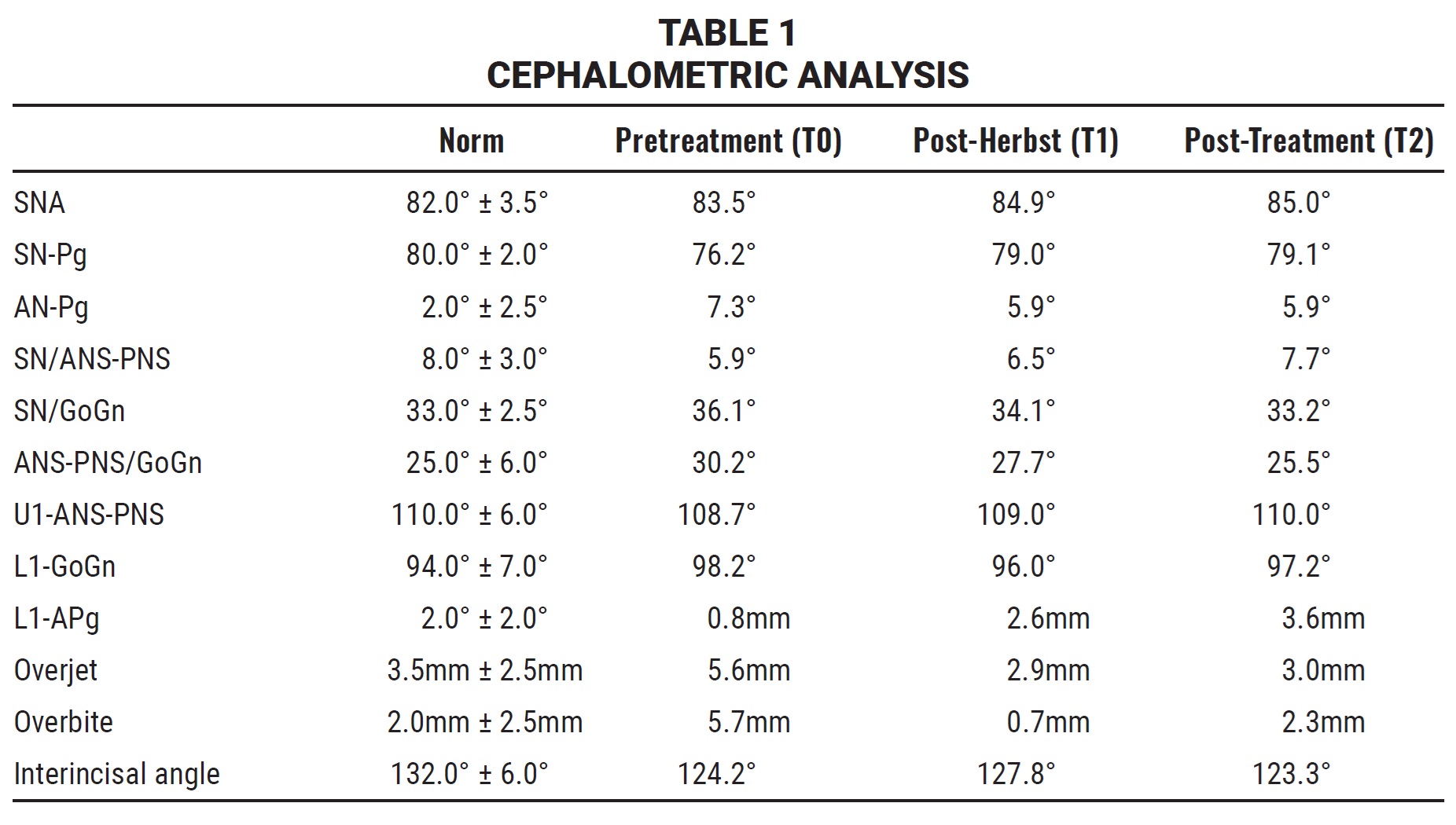
Cephalometric analysis indicated a skeletal Class II malocclusion with a long face, a short ramus, slightly palatally inclined maxillary incisors, and a protrusive inclination of the mandibular incisors relative to the mandibular symphysis (Table 1). The overjet and overbite were excessive.
Treatment goals were to improve facial esthetics, reduce the lower third of the face, and improve the mandibular projection and lip incompetence while converting the Class II dental relationship to a Class I. Because of the patient’s convex profile, the treatment strategy would incorporate mechanics to enhance mandibular advancement.
One proven method for treating a Class II patient with a retrusive mandible involves Class II elastics attached to miniscrew implants and connected by elastic power chain to a full-size stainless steel archwire.24,25 We rejected this option, however, because the patient could not guarantee adequate compliance with intermaxillary elastics. Another alternative was to expand the maxilla and align the dentition, with the expectation of surgery upon completion of growth, but the patient was not able to delay treatment. Based on the patient’s facial features, the best choice seemed to be a bite-jumping appliance that would encourage mandibular protraction while limiting the adverse effects traditionally associated with pushing force vectors.18,19
Treatment Progress
Preadjusted .022" × .028" brackets*** were placed in the upper arch, and an .014" nickel titanium archwire was used to correct the upper incisor inclination and the scissor bite (Fig. 2). After five months of treatment, a Herbst appliance with four 1.4mm × 6mm TADs† (H4T) was placed (Fig. 3). In the lower arch, one miniscrew was inserted between the right first permanent molar and second premolar and the other between the left first and second premolars. Auxiliary buttons were bonded to the buccal surfaces of the canines, and elastic chains were attached to the miniscrews to retrocline the lower incisors and promote mandibular protraction. In the upper arch, a miniscrew was inserted between the first and second premolars on each side, and elastic chains were attached between the miniscrews and an .018" × .022" stainless steel archwire for vertical control.

Fig. 2 .022" × .028" brackets*** placed in upper arch.
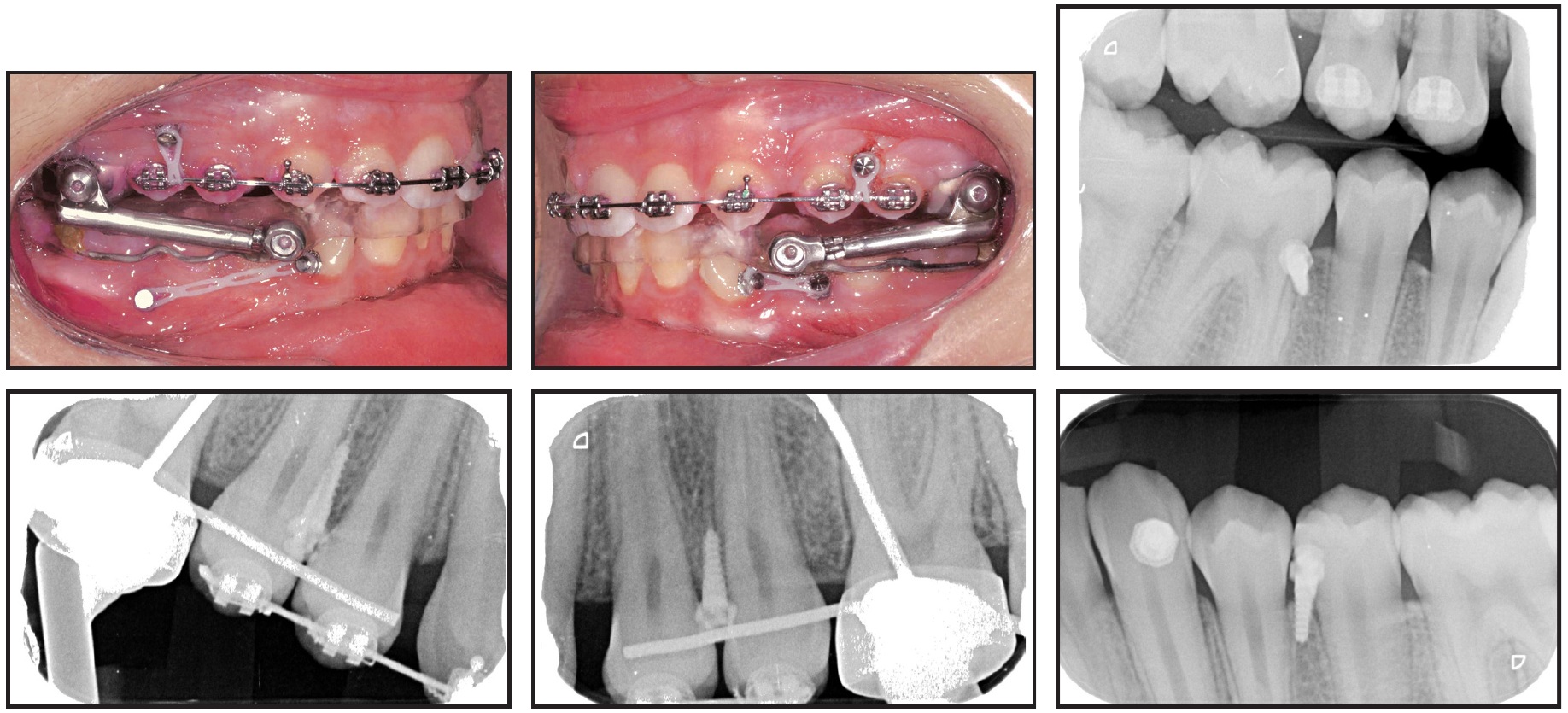
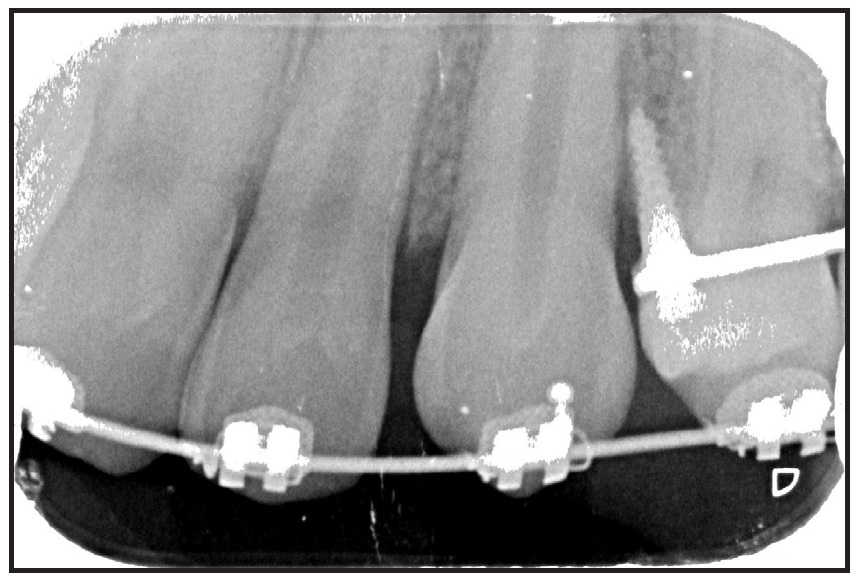
Fig. 4 Failed upper left TAD replaced after 11 days with TAD between canine and first premolar.
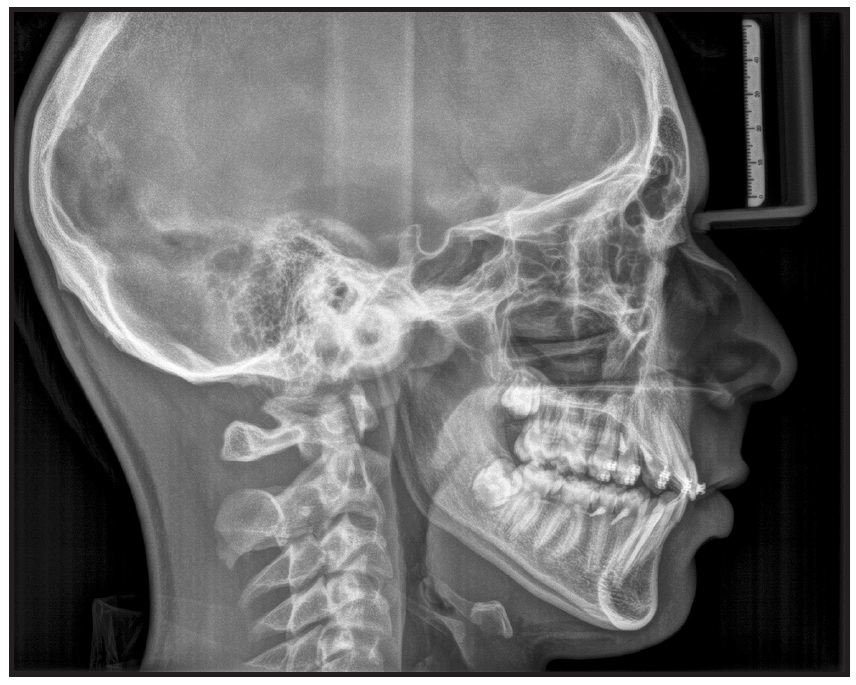
Fig. 5 Herbst appliance removed after 10 months of treatment.
The upper and lower arches exhibited an overcorrected Class I relationship. The upper first molars were bonded, and an .017" × .025" nickel titanium archwire was inserted (Fig. 6). Fixed multibracket appliances with .016" × .025" nickel titanium archwires were then placed in the lower arch, and the patient was given light Class II elastics to wear full time, starting at 30g per side and increasing over 11 months to 250g per side. To mesialize the upper posterior segments, elastic chains were connected from the first molars to the miniscrews. The lower archwires progressed to .017" × .025" nickel titanium, followed by final upper and lower .018" × .022" stainless steel wires.
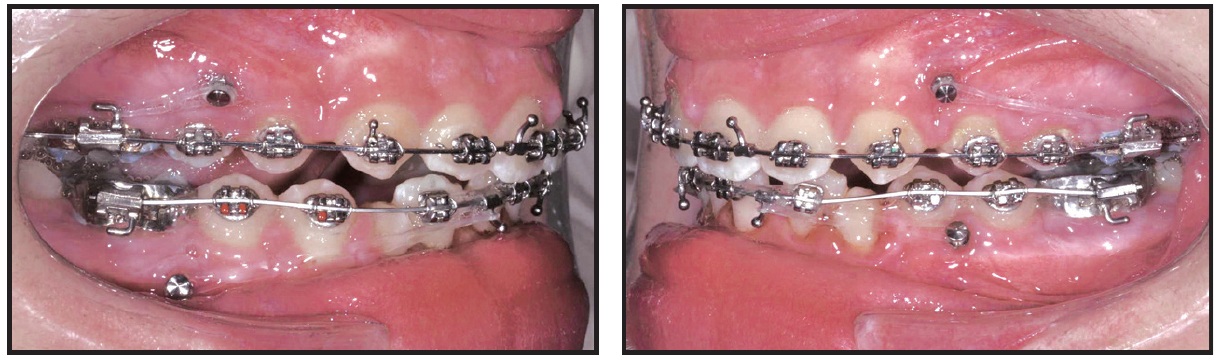
Fig. 6 Brackets bonded in lower arch, and full-time Class II elastic wear started; elastic chains attached between TADs and first molars to mesialize upper posterior segments.
Eleven months later, the fixed appliances were removed, and a positioner was delivered. After another six months, the positioner was replaced with two Essix‡ retainers.
Treatment Results
The active treatment time was 26 months (Fig. 7A).
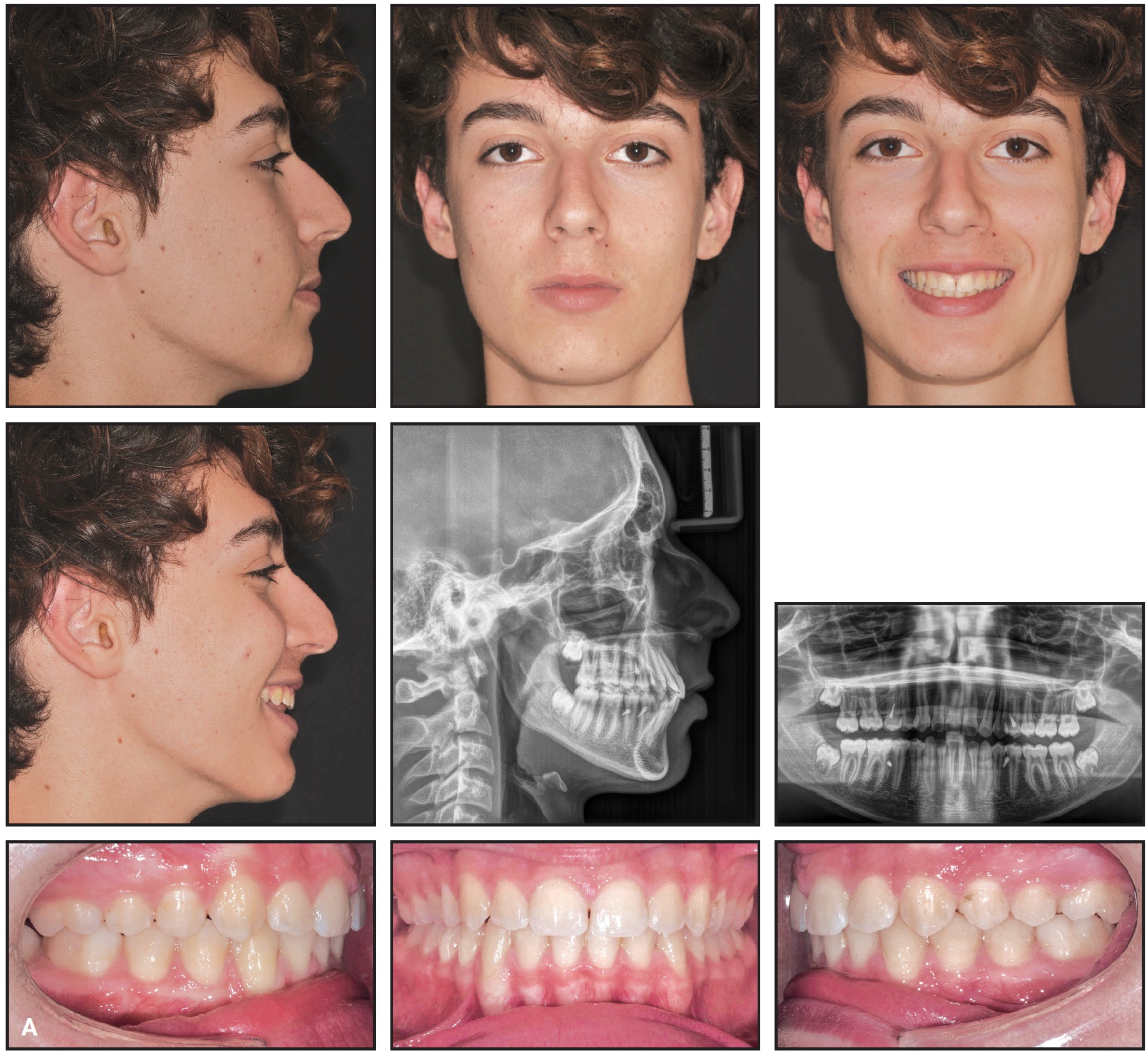
Fig. 7 A. Patient after 26 months of treatment (continued in next image).
The profile was improved substantially, resulting in harmony between the upper and lower lips, and bilateral Class I molar and canine relationships were achieved. A panoramic radiograph taken immediately after treatment showed acceptable root angulations, no evidence of root resorption, and stable bone levels. No muscle or joint problems had developed.
Because of mild upper incisor flaring, there was no worsening of the profile during the Herbst treatment (Table 1). The A point advanced between pretreatment (T0) and post-Herbst (T1) cephalograms and remained almost unchanged thereafter. The upper first molars were intruded and distalized, and vertical dentoalveolar growth was well controlled. The maxilla grew downward and forward, so that the posterior intrusion had only a dentoalveolar effect. By the end of treatment, the upper first molars had returned nearly to their pretreatment positions. Lower incisor inclination was well controlled between T0 and T1 and between T1 and the end of treatment (T2). Pogonion advanced 4.5mm, and substantial growth occurred at the ramus as the articular point moved upward and slightly forward.
The patient was satisfied with the overall esthetics and treatment outcome.
Discussion
The Herbst appliance is often utilized for treatment of a Class II malocclusion and a retrusive mandible because it works efficiently without relying on patient cooperation. Despite such advantages, however, it causes some side effects that can hinder the desired mandibular advancement. Although these effects can be partly reduced by using miniscrew anchorage and elastic power chains,14,23 there are still concerns about clockwise rotation of the maxillary arch and backward relapse of pogonion.7,26
The H4T method we have described, involving TADs in both arches, provided satisfactory control of our patient’s vertical dimension (−2.9° change in SN/GoGn between T0 and T2). This induced a counterclockwise rotation of the mandible and contributed to a considerable mandibular advancement, as measured in a 4.5mm forward movement of pogonion on the cranial base superimposition (Fig. 7B).
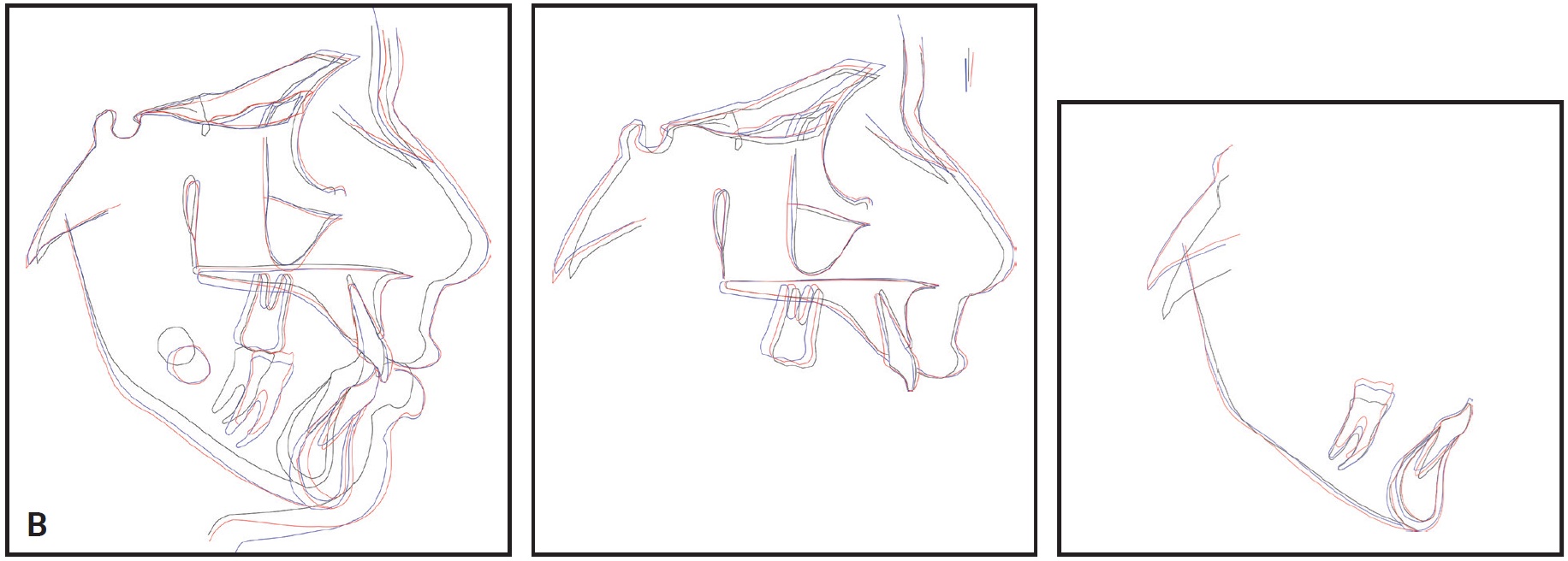
Fig. 7 (cont.) B. Superimposition of cephalometric tracings before treatment, after Herbst therapy, and after treatment.
The decision to utilize TADs in the upper arch was based on clinical evaluation of the patient’s excessive nasolabial angle. We believed the TADs could help prevent the usual palatal inclination of the upper incisors associated with the Herbst appliance. Buccal inclination of the lower incisors still occurred, but it resulted only in leveling of the lower arch. We employed Class II elastics to restrict the Herbst appliance’s propulsory effect on the mandible.
The concept of using four TADs to control vertical development and promote mandibular advancement can also be applied to mandibular propulsive systems such as the PowerScope,†† Forsus,‡‡ and other fixed functional appliances.
FOOTNOTES
- *Registered trademark of Dentaurum, Inc., Newtown, PA; www.dentaurum.com.
- **Trademark of Protec Dental Laboratories Ltd., Vancouver, BC, Canada; www.protecdental.com.
- ***Butterfly System, trademark of American Orthodontics, Sheboygan, WI; www.americanortho.com.
- †Micerium Anchorage System, Micerium S.p.A., Avegno, Italy; www.micerium.it.
- ‡Registered trademark of Denstply Sirona Orthodontics Inc., Sarasota, FL; www.essix.com.
REFERENCES
- 1. Alves, P. and Oliveira, A.: A comparison of the skeletal, dental, and soft tissue effects caused by Herbst and mandibular protraction appliances in the treatment of mandibular Class II malocclusions, World J. Orthod. 9:e1-19, 2008.
- 2. Baltromejus, S.; Ruf, S.; and Pancherz, H.: Effective temporomandibular joint growth and chin position changes: Activator versus Herbst treatment. A cephalometric roentgenographic study, Eur. J. Orthod. 24:627-637, 2002.
- 3. Barnett, G.; Higgins, D.; Major, P.; and Flores-Mir, C.: Immediate skeletal and dentoalveolar effects of the crown- or banded type Herbst appliance on Class II division 1 malocclusion, Angle Orthod. 78:361-369, 2008.
- 4. Baysal, A. and Uysal, T.: Soft tissue effects of Twin Block and Herbst appliances in patients with Class II division 1 mandibular retrognathy, Eur. J. Orthod. 35:71-81, 2013.
- 5. Bock, N. and Ruf, S.: Post-treatment occlusal changes in Class II division 2 subjects treated with the Herbst appliance, Eur. J. Orthod. 30:606-613, 2008.
- 6. Bock, N.; Reiser, B.; and Ruf, S.: Class II subdivision treatment with the Herbst appliance, Angle Orthod. 83:327-333, 2013.
- 7. Bock, N. and Ruf, S.: Dentoskeletal changes in adult Class II division 1 Herbst treatment—How much is left after the retention period? Eur. J. Orthod. 34:747-753, 2012.
- 8. Bock, N.C.; von Bremen, J.; and Ruf, S.: Occlusal stability of adult Class II Division 1 treatment with the Herbst appliance, Am. J. Orthod. 138:146-151, 2010.
- 9. Booij, J.; Goeke, J.; Bronkhorst, E.; Katsaros, C.; and Ruf, S.: Class II treatment by extraction of maxillary first molars or Herbst appliance: Dentoskeletal and soft tissue effects in comparison, J. Orofac. Orthop. 74:52-63, 2013.
- 10. Manni, A.; Mutinelli, S.; Cerruto, C.; Giraudo, P.; Romano, R.; and Cozzani, M.: Comparison of complications in the conventional telescopic Herbst rod and tube and Manni telescopic Herbst: A retrospective clinical study, Angle Orthod. 88:377-383, 2018.
- 11. O’Brien, K. et al.: Effectiveness of treatment for Class II malocclusion with the Herbst or twin-block appliances: A randomized, controlled trial, Am. J. Orthod. 124:128-137, 2003.
- 12. Pancherz, H.: The Herbst appliance—Its biologic effects and clinical use, Am. J. Orthod. 87:1-20, 1985.
- 13. Pancherz, H.: The mechanism of Class II correction in Herbst appliance treatment: A cephalometric investigation, Am. J. Orthod. 82:104-113, 1982.
- 14. Manni, A.; Mutinelli, S.; Pasini, M.; Mazzotta, L.; and Cozzani, M.: Herbst appliance anchored to miniscrews with 2 types of ligation: Effectiveness in skeletal Class II treatment, Am. J. Orthod. 149:871-880, 2016.
- 15. Aelbers, C.M. and Dermaut, L.R.: Orthopedics in orthodontics, Part I: Fiction or reality—A review of the literature, Am. J. Orthod. 110:513-519, 1996.
- 16. Cozza, P.; Baccetti, T.; Franchi, L.; De Toffol, L.; and McNamara, J.A.: Mandibular changes produced by functional appliances in Class II malocclusion: A systematic review, Am. J. Orthod. 129:599.e1-12, 2006.
- 17. Aidar, L.A.; Dominguez, G.C.; Abrahao, M.; Yamashita, H.K.; and Vigorito, J.W.: Effects of Herbst appliance treatment on temporomandibular joint disc position and morphology: A prospective magnetic resonance imaging study, Am. J. Orthod. 136:412-424, 2009.
- 18. Weschler, D. and Pancherz, H.: Efficiency of three mandibular anchorage forms in Herbst treatment: A cephalometric investigation, Angle Orthod. 75:23-27, 2005.
- 19. Pancherz, H. and Hansen, K.: Mandibular anchorage in Herbst treatment, Eur. J. Orthod. 10:149-164, 1988.
- 20. Franchi, L.; Baccetti, T.; and McNamara, J.A. Jr.: Treatment and posttreatment effects of acrylic splint Herbst appliance therapy, Am. J. Orthod. 115:429-438, 1999.
- 21. Flores-Mir, C.; Ayeh, A.; Goswani, A.; and Charkhandeh, S.: Skeletal and dental changes in Class II division 1 malocclusions treated with splint-type Herbst appliances: A systematic review, Angle Orthod. 77:376-381, 2007.
- 22. Manni, A.; Pasini, M.; and Cozzani, M.: Comparison between Herbst appliances with or without miniscrew anchorage, Dent. Res. J. (Isfahan) 9:S216-221, 2012.
- 23. Bremen, J.; Ludwig, B.; and Ruf, S.: Anchorage loss due to Herbst mechanics—Preventable through miniscrews? Eur. J. Orthod. 37:462-466, 2014.
- 24. Manni, A.; Lupini, D.; and Cozzani, M.: Bone anchored inter-maxillary elastics in an asymmetric Class II malocclusion: A case report, Int. Orthod. 15:263-277.
- 25. Manni, A.; Lupini, D.; and Cozzani, M.: Combining skeletal anchorage and intermaxillary elastics in Class II treatment, J. Clin. Orthod. 52:227-234, 2018.
- 26. Bock, N. and Pancherz, H.: Herbst treatment of Class II division 1 malocclusions in retrognathic and prognathic facial types, Angle Orthod. 76:930-941, 2006.
-
 DR. MANNI
DR. MANNI -
 DR. CERRUTO
DR. CERRUTO -
 DR. COZZANI
DR. COZZANI
Dr. Manni is in the private practice of orthodontics in Racale, Italy; e-mail: antoniomanni2003@libero.it. Dr. Cerruto is in the private practice of orthodontics in Siena, Italy. Dr. Cozzani is an instructor at the Istituto Giuseppe Cozzani, La Spezia, Italy.