CASE REPORT
Nonsurgical Management of Severe Reverse Overbite in a Young Adult
A forward functional shift of the mandible, anterior crossbite, and centric relation-centric occlusion (CR-CO) discrepancy are suggestive of a pseudo-Class III malocclusion, in which the individual reflexively adjusts the bite to accommodate the occlusion. Although such a patient’s proclined lower and retroclined upper incisors are generally associated with a mesial step of at least 3mm, the incisors will move into an end-to-end relationship when the jaws are guided into CR.1 The pseudo-Class III patient may appear to have a Class I molar relationship, a normal mandibular appearance, and a straight profile, disguising the skeletal discrepancy.2
Treatment objectives should focus on the main underlying cause of the pseudo-Class III: the inclination of the upper incisors. Various appliances have been proposed for this purpose, including fixed or removable inclined planes, removable plates with springs, functional appliances, chin cups, and conventional fixed appliances. In a prospective, longitudinal study by Hägg and colleagues of patients in the mixed dentition, the use of a simple 2 × 4 fixed appliance in the first phase of treatment resulted in a positive overjet that was maintained long term.3 No previous reports have documented treatment of a severe reverse overbite with a 2 × 4 appliance in a young adult, however, as described here.
Similar articles from the archive:
Diagnosis and Treatment Plan
A 25-year-old male presented to the Department of Orthodontics, KLE V.K. Institute of Dental Sciences, with the chief complaint of inability to chew with his front teeth. On clinical examination, he showed a slightly concave profile and a horizontal growth pattern, with no facial asymmetry (Fig. 1, Table 1). None of the patient’s direct family members exhibited skeletal Class III features.
Intraoral examination revealed a severe anterior reverse overbite of −16mm and overjet of −4mm, overerupted lower incisors with midline spacing, Grade 1 mobility of the lower central incisors, and a 5mm curve of Spee. Bolton analysis indicated a 3mm excess of lower anterior tooth material. The patient was diagnosed with a pseudo-Class III malocclusion due to a CR-CO discrepancy.
The treatment plan was to eliminate the functional mandibular shift, correct the anterior crossbite, establish positive overjet and overbite, and achieve Class I molar and canine relationships and a pleasant profile.
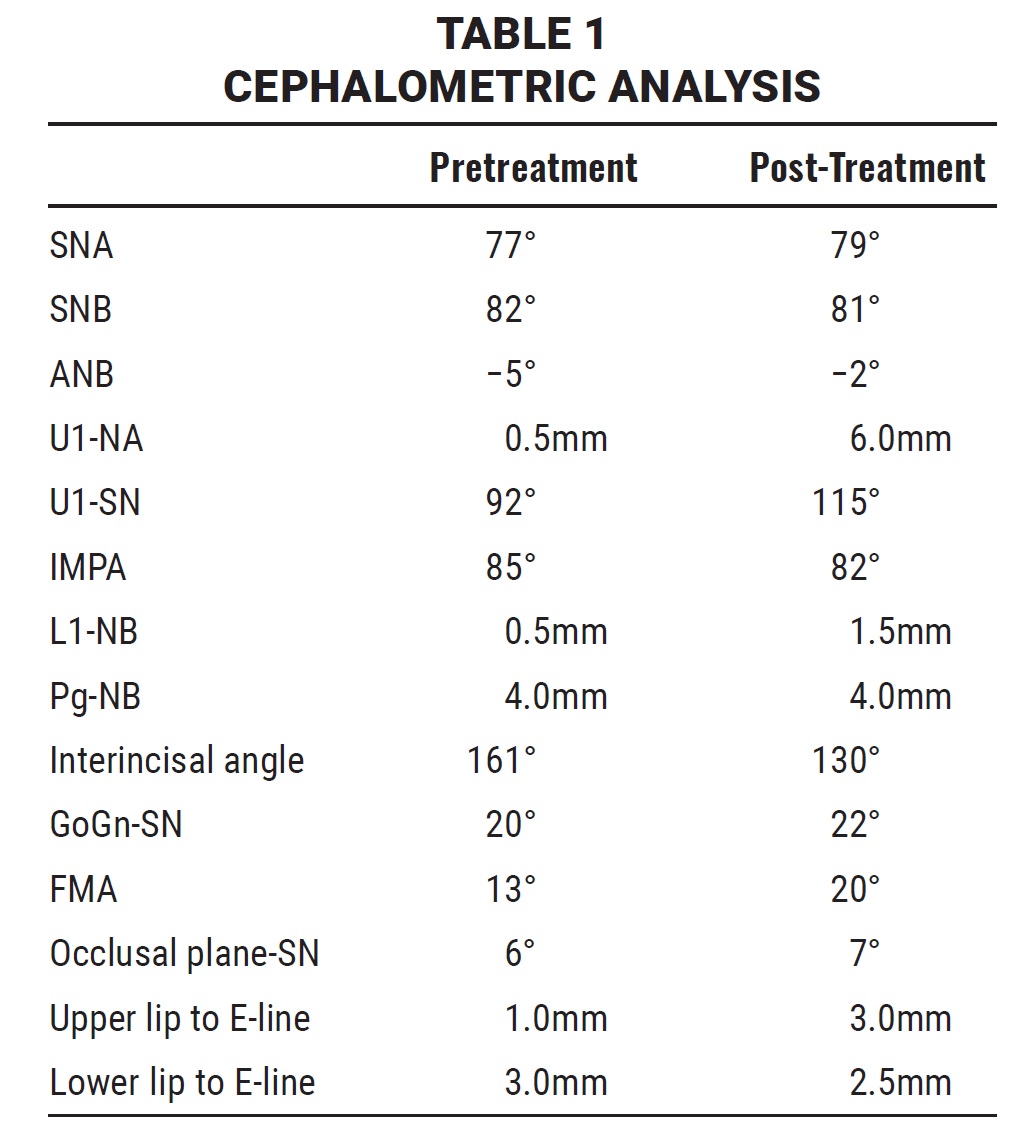
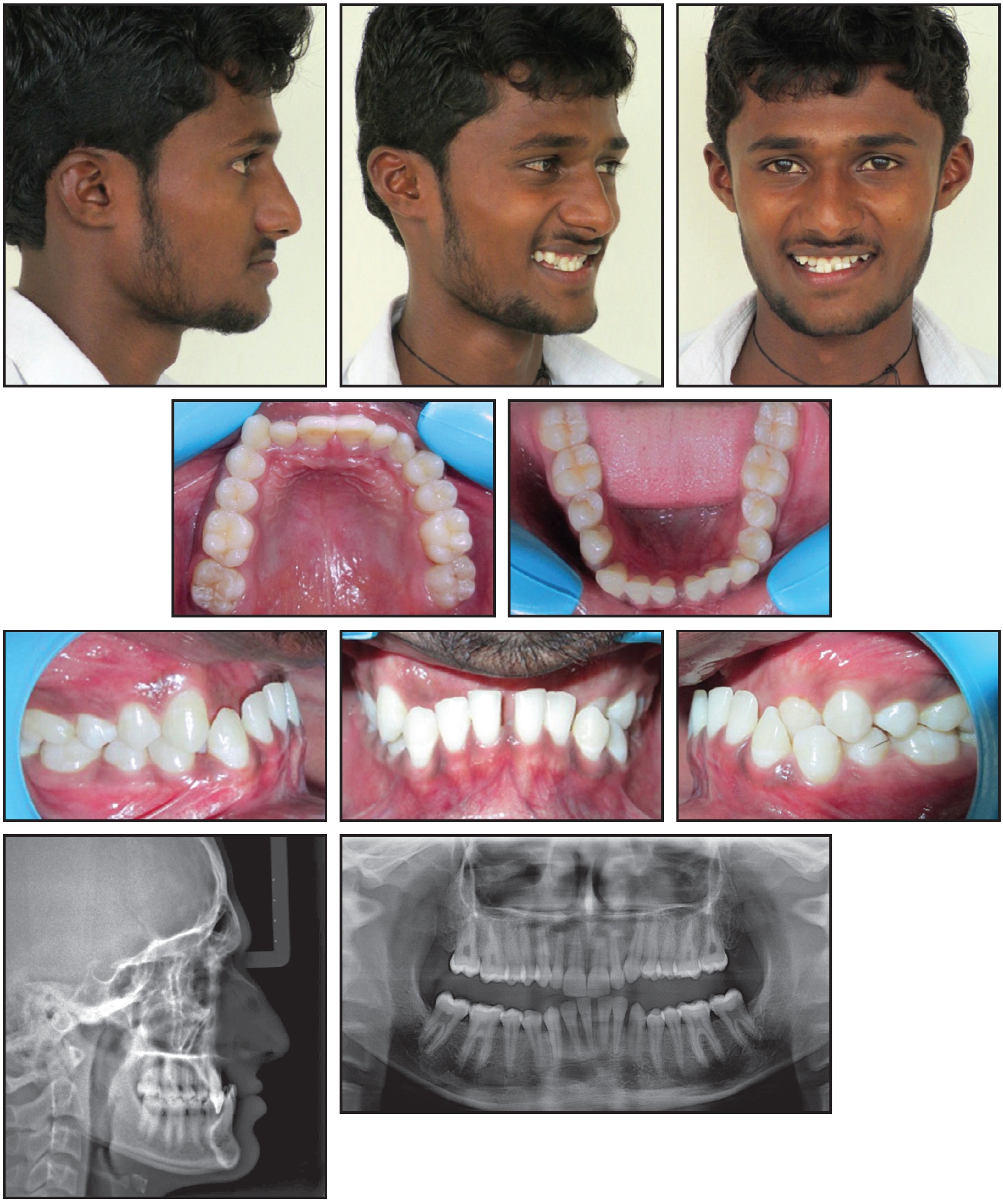
Fig. 1 25-year-old male patient with pseudo-Class III malocclusion before treatment.
Treatment Progress
The lower arch was bonded with an .022" × .028" MBT* appliance, and an .012" round nickel titanium archwire was placed. Three months later, the wire size was increased to .014" for two more months of leveling. Since growth appeared to be complete, a 2 × 4 appliance was then bonded in the upper arch for correction of the upper incisor inclination (Fig. 2). The patient was asked to wear a removable posterior bite plate (7mm thick in the premolar region) for one month while sleeping, followed by an additional six hours of wear every day for four months.
The posterior bite plate was trimmed occlusally at each monthly visit, and the patient was assessed for signs and symptoms of TMD. Positive overjet and overbite were achieved in nine months (Fig. 3). The upper canines and premolars were bonded, and reverse-curve .016" × .022" nickel titanium archwires were inserted for three months of leveling.
At that point, .019" × .025" stainless steel wires were placed in both arches and diagonal elastics were prescribed to correct the midline discrepancy (Fig. 4). Patient compliance with the elastics was excellent throughout treatment. Restorative composite build-ups were added to compensate for the Bolton discrepancy of the upper lateral incisors, and the upper left central incisor was recontoured. Fixed appliances were removed after 18 months of treatment because of the patient’s impending military review.
Treatment Results
Post-treatment results showed an improved profile and Class I molar and canine relationships, with optimal overjet and overbite (Fig. 5A). The anterior crossbite was corrected, and the overall facial balance was greatly improved. Extraoral photographs displayed a relaxed lip closure and an esthetic smile with a favorable smile arc, meeting the patient’s expectations. The panoramic radiograph demonstrated proper root parallelism with no apical resorption.
Maxillary and mandibular cephalometric superimpositions confirmed that the upper incisors were proclined labially and the lower posterior teeth were uprighted and moved distally (Fig. 5B, Table 1).

Fig. 2 After five months of leveling with lower .022" × .028" MBT* appliance and nickel titanium archwires, 2 × 4 appliance placed in upper arch.
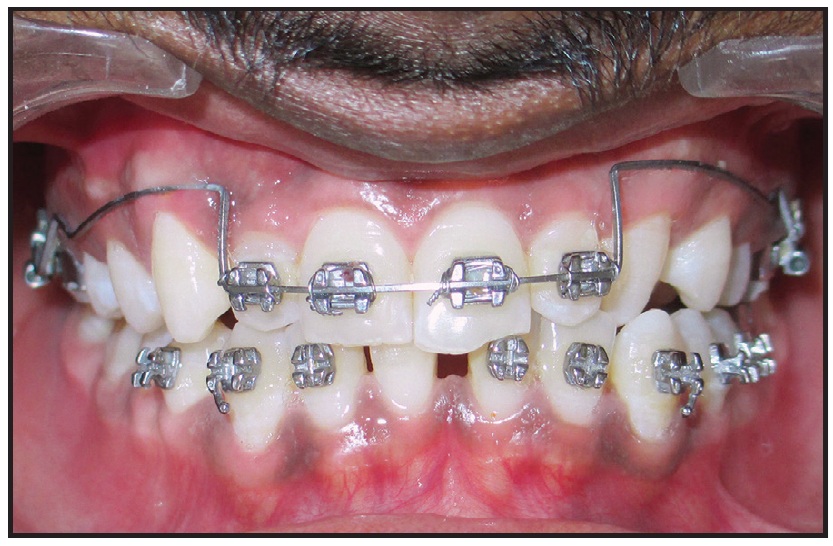
Fig. 3 Positive overjet and overbite achieved after nine months of treatment.

Fig. 4 After 16 months of treatment.
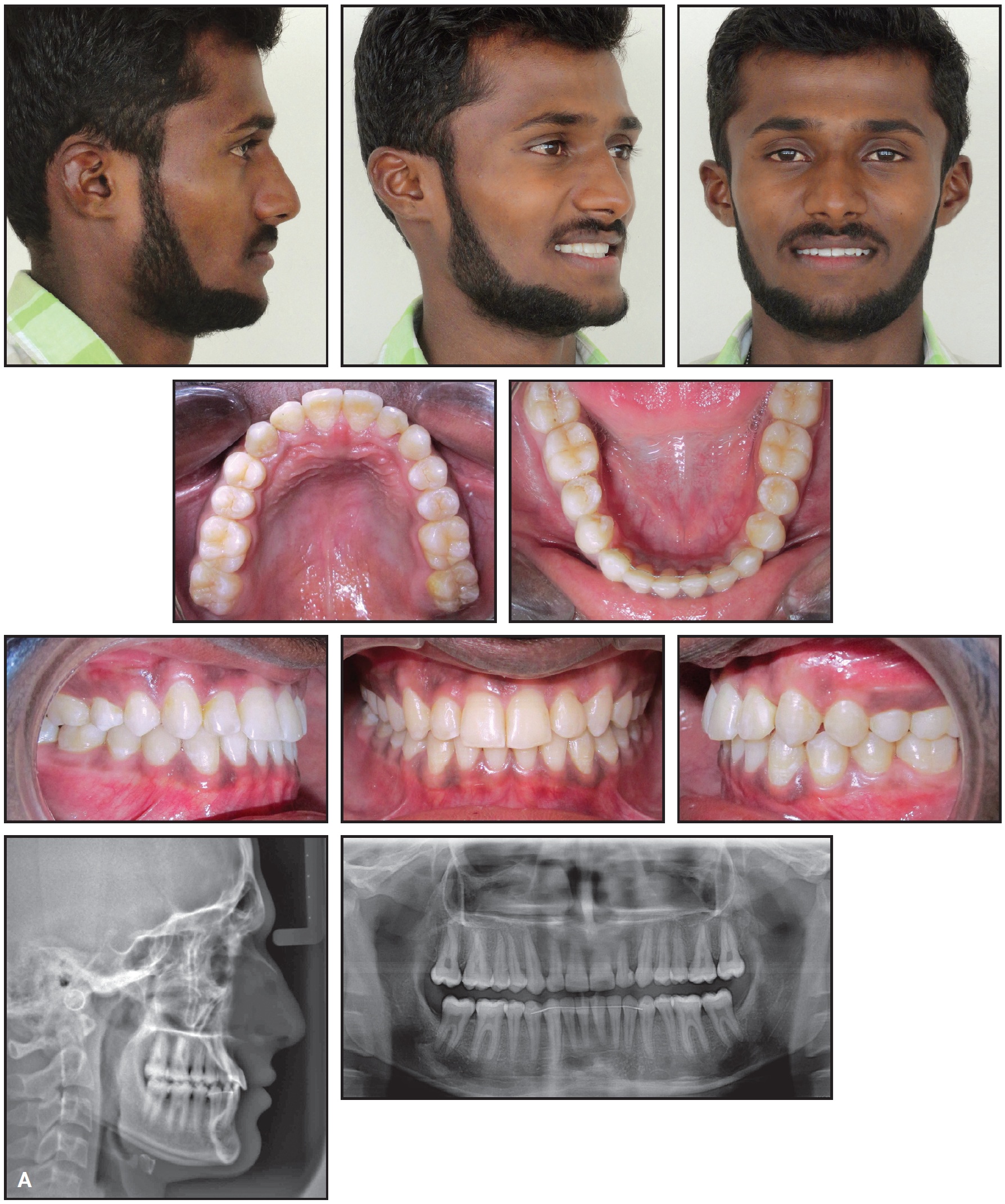
Fig. 5 A. Patient after 18 months of treatment.
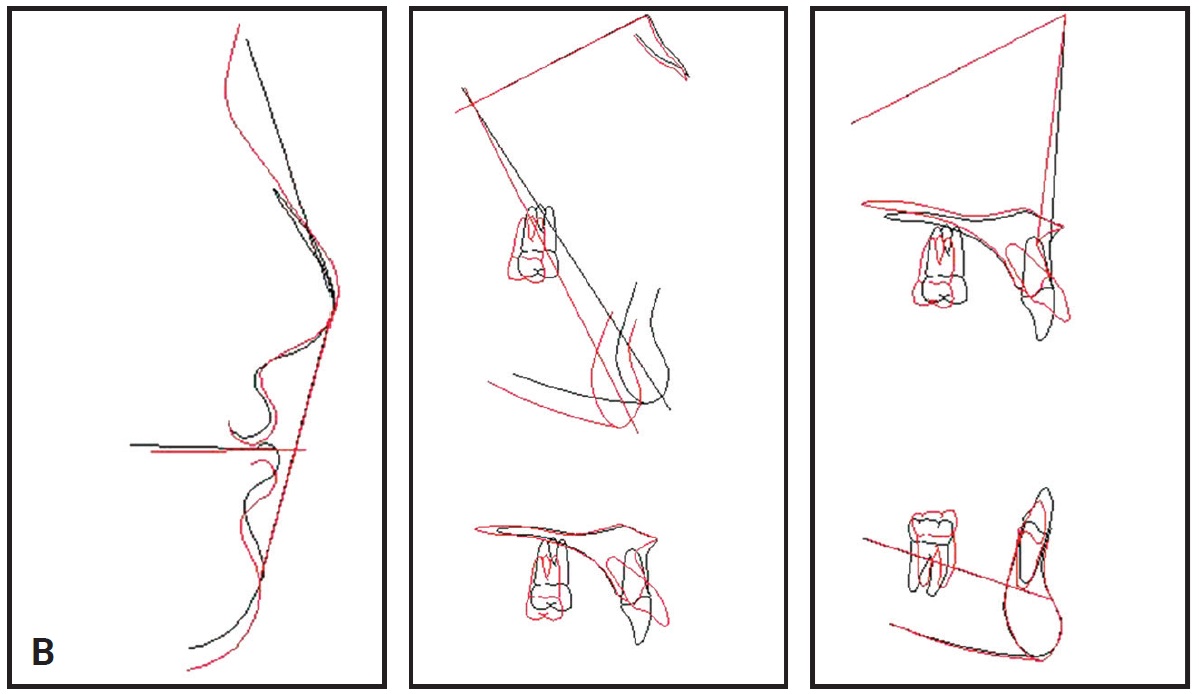
Fig. 5 (cont.) B. Superimposition of pre- and post-treatment cephalometric tracings.
Discussion
Class III malocclusion may result from a combination of etiologic factors, depending on the patient’s growth pattern and potential. The causes and expression of a Class III malocclusion must be identified and understood to enable formulation of an effective treatment plan—whether orthodontic, orthopedic, surgical, or a combination of these modalities.
Failure to correct a pseudo-Class III at an early age may lead to the establishment of a skeletal Class III malocclusion.4,5 In our case, however, the maxillary incisor inclination was well within the established limit (120°) for dentoalveolar compensation in Class III treatment. Satisfactory occlusal and esthetic results were attributable to significant dentoalveolar compensation and excellent patient compliance.
FOOTNOTES
- *Trademark of 3M Unitek, Monrovia, CA; www.3Munitek.com.
REFERENCES
- 1. Reyes, A.; Serret, L.; Peguero, M.; and Tanaka, O.: Diagnosis and treatment of pseudo-Class III malocclusion, Case Rep. Dent. 2014:652936, 2014.
- 2. Angle, E.H.: Classification of malocclusion, Dent. Cosmos 41:248-264, 1899.
- 3. Hägg, U.; Tse, A.; Bendeus, M.; and Rabie, A.B.: A follow-up study of early treatment of pseudo Class III malocclusion, Angle Orthod. 74:465-472, 2004.
- 4. Daher, W.; Caron, J.; and Wechsler, M.H.: Nonsurgical treatment of an adult with a Class III malocclusion, Am. J. Orthod. 132:243-251, 2007.
- 5. Janson, G.; de Souza, J.E.; de Andrade Alves, F.; Andrade, P. Jr.; Nakamura, A.; de Freitas, M.R.; and Henriques, J.F.: Extreme dentoalveolar compensation in the treatment of Class III malocclusion, Am. J. Orthod. 128:787-794, 2005.
-
 DR. TAKANE
DR. TAKANE -
 DR. KELUSKAR
DR. KELUSKAR -
 DR. JAISINGHANI
DR. JAISINGHANI -
 DR. MALAGAN
DR. MALAGAN -
 DR. JATTI
DR. JATTI
Dr. Takane is in the private practice of orthodontics at Smilekart Dental Clinic,Shop No. 2 Atria, Kabra Galaxy, Off Ghodbunder Road, Brahmand, Thane West 400607, India; e-mail: vanashree3087@gmail.com. Dr. Keluskar is Professor and Dean, Dr. Malagan is a Reader, and Dr. Jatti is Professor and Department Head, Department of Orthodontics, KLE V.K. Institute of Dental Sciences, JNMC Campus, Nehrunagar, Belgavi, Karnataka, India. Dr. Jaisinghani is an Associate Professor, Sinhgad Dental College and Hospital, Pune, India.